

Abstract
Objective
To report the surgical survival of dams and piglets and follow‐up survival and future breeding potential of swine that underwent cesarean section for correction of dystocia.
Study design
Retrospective study.
Animals
One hundred ten client‐owned, female swine. All swine included in this study were breeding stock for market pigs to be used for exhibition purposes.
Methods
Medical records of swine that underwent cesarean section at The Ohio State University Hospital for Farm Animals for resolution of dystocia between January of 2013 and July of 2018 were reviewed. Signalment, history, number of piglets per litter, treatments, and surgical procedure were recorded. Follow‐up information (survival, complications, and additional pregnancies) was obtained via telephone interview.
Results
A fetus was not palpable in 77 of 110 (70%) cases at presentation. The median litter size was eight piglets (range, 1‐14), with medians of five (range, 0‐13) live and one dead (range, 0‐11) piglets per litter. Follow‐up was available for 52 dams, of which 39 (75%) survived. Complications were recorded in 20 of 52 (38.46%) cases and included incisional seroma formation, lethargy, and anorexia. Twenty‐three dams became pregnant and farrowed after the cesarean section, with no reported complication in 13 of these.
Conclusion
Cesarean section in swine is associated with a good prognosis for recovery from the procedure and a fair to guarded prognosis for future breeding.
Clinical significance
Cesarean section may be considered for resolution of dystocia in swine. However, owners should be advised that nearly half of sows require assistance in subsequent deliveries.
1. INTRODUCTION
Dystocia is considered rare in swine, with an estimated prevalence of less than 1%. 1 Normal labor in swine usually lasts between 1 and 5 hours, with 15 minutes between delivery of each piglet; a period of greater than 1 hour between piglets is considered indicative of dystocia. 1 The two most commonly reported causes of dystocia in swine include uterine inertia, or ineffective myometrial contractions, and fetomaternal mismatch. Constipation, obesity, and swelling due to iatrogenic trauma caused by intrapelvic manipulation may result in narrowing of the vaginal canal and are risk factors for dystocia. 1
Cesarean section in swine is typically performed in cases of pelvic obstruction due to fetomaternal mismatch. 1 , 2 The approach for cesarean section in swine is well described, 1 , 2 , 3 but little information is available regarding complications and prognosis. Published veterinary literature focuses on elective cesarean section for derivation of gnotobiotic research piglets. 4 In this population, cesarean section is performed prior to the onset of labor. 5 This is in contrast to pigs in commercial or market situations, in which cesarean section is performed as an emergent procedure for resolution of dystocia in client‐owned animals. The available literature regarding cesarean section in swine for the resolution of dystocia is limited, and, to the best of the authors' knowledge, there are no published reports in English. 6 Some texts describing the procedure state that poor outcomes for both gilts/sows and piglets should be expected due to exhaustion, shock, or severe stress, but this is not based on empirical studies>. 1 , 2
The objective of this study was to describe the signalment, clinical signs, and outcomes of swine that underwent cesarean section for correction of dystocia. We hypothesized that cesarean section in swine would have a satisfactory outcome for survival of the dam and for subsequent full‐term pregnancy.
2. MATERIALS AND METHODS
2.1. Case selection
Medical records of client‐owned market swine presenting for dystocia and requiring cesarean section for resolution at The Ohio State University Hospital for Farm Animals between January of 2013 and July of 2018 were included in this study.
2.2. Medical record information
Information collected from the medical records included signalment, parity, cause of dystocia, duration of labor, number of piglets in the litter, number of live and dead piglets from each litter, number of piglets born prior to presentation, dam sedation and epidural protocol, antibiotic and analgesic administration, anesthetic protocol, and surgical procedure. A dam was considered to be in dystocia when either of two scenarios were true: (1) the dam was in active labor for more than 2 hours without the birth of a piglet, or (2) there was ≥1 hour between the births of piglets within a litter.
2.3. Follow‐up information
Follow‐up information was obtained via a telephone interview 9 months or more after the procedure. Owners were asked whether the animal had survived for 9 months or longer after discharge from the hospital. When the dam was not alive, they were asked how long it had lived after the procedure. In addition, they were asked whether the dam experienced any complications after the procedure, whether the owners attempted to breed the dam again, and whether the breeding resulted in pregnancy. When the dam did successfully breed back, the owners were asked whether the pregnancy was carried to term and whether the farrowing was uneventful or whether the animal experienced another dystocia. Finally, owners were asked to rank their satisfaction with the procedure on a scale of 1 to 5, with 1 being completely unsatisfied and 5 being completely satisfied.
3. RESULTS
3.1. Case presentation
One hundred twenty swine underwent cesarean section during the study time frame, and 110 animals met the inclusion criteria. The median age of the swine was 12 months (range, 10‐60). Ninety‐eight of the 110 (89.09%) swine were first parity gilts, five (4.55%) were second parity gilts, one (0.91%) was third parity gilt, and six (5.45%) did not have a recorded parity. There were 76 (69.09%) mixed breed swine, 13 Hampshire (11.82%), six Berkshire (5.45%), five Yorkshire (4.54%), four Landrace (3.64%), two Poland China (1.82%), and one each of Duroc (0.91%), Hereford (0.91%), spotted swine(0.91%), and Tamworth (0.91%). All swine were carrying litters of piglets intended for exhibition. The cause of dystocia in the animals included unproductive labor with no reported palpable piglet in the vaginal canal (n = 77 [70%]) and unproductive labor with a piglet palpably in the vaginal canal (n = 33 [30%]). Duration of labor prior to presentation was reported in 78 of the 110 (70.91%) animals. Sixty‐four of the 78 (82.05%) dams had labor that lasted ≤12 hours (range, 2‐12), and 14 of the 78 (17.95%) dams had duration of labor >12 hours (range 13‐72 hours).
3.2. Surgery and anesthesia
A vaginal examination was performed in all swine. The decision to perform a cesarean section was made when a piglet was in the canal and could not be retrieved vaginally, severe vaginal swelling and trauma limited the ability to safely deliver piglets vaginally, or there was failure of the piglet to reach the vaginal canal due to presumed uterine inertia.
Twenty‐five (22.73%) animals were sedated with 0.05 mg/kg of acepromazine IM because of severe distress or fractious nature. Seventy‐five (68.18%) animals received perioperative antibiotics including 5 mg/kg ceftiofur crystalline free acid IM (n = 58), 22 000 IU/kg procaine penicillin G IM (n = 10), or 19.8 mg/kg oxytetracycline IM (n = 7). Ninety‐one (82.73%) animals received perioperative flunixin meglumine (2.2 mg/kg IM). A lumbosacral epidural at a dose of 1 mL/10 kg of 2% lidocaine was reported to have been given in 82 (74.55%) animals.
All swine were induced with mask anesthesia by using flow‐by 5% isoflurane in 4 L/minute of oxygen. After anesthetic induction had been achieved, isoflurane and oxygen were adjusted as required to maintain anesthesia with mask flow‐by. Heart rate, respiratory rate, and temperature were monitored throughout the procedure. Mean total anesthetic time was 93 ± 20 minutes.
After induction of general anesthesia, IV auricular catheter was placed in the uppermost ear to secure venous access in 95 (86.36%) swine. Fluids (Ringer's solution, lactated Ringer's solution, or 0.9% saline) were administered IV via the auricular catheter. According to the medical records, fluids contained various additives (calcium gluconate, potassium, and dextrose), depending on the status of the dam under anesthesia and clinician preference. Volume of fluids administered ranged from 3 to 5 L.
The animal was placed in either right or left lateral recumbency, and the uppermost pelvic limb of the animal was abducted and extended caudally and secured in place. A 30‐cm area bordered by the inguinal region caudally, the uppermost mammary chain ventrally, and just beyond the flank fold craniodorsally was clipped and aseptically prepared. A 10‐ to 20‐cm incision was made through the skin immediately dorsal and parallel to the attachment of the mammary chain beginning 10 cm cranial to the inguinal region (Figure 1). The incision was continued through the subcutaneous tissues, the muscular and aponeurotic portions of external abdominal oblique muscle, the internal abdominal oblique muscle, and the transversus abdominus muscle. Retroperitoneal fat was digitally separated, and the peritoneum was sharply incised.
FIGURE 1.
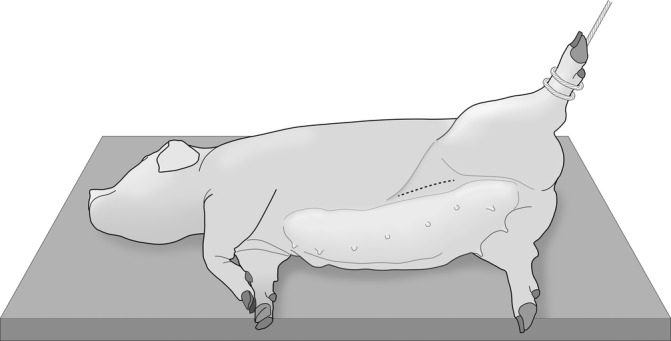
The positioning and surgical site for cesarean section in swine. The gilt or sow was positioned in lateral recumbency (right or left), and the uppermost limb was abducted and extended caudally. A 10‐ to 20‐cm incision was made just dorsal to the mammary chain, roughly 10 cm cranial to the inguinal region (dotted line)
An effort was made to expose both horns of the uterus through the incision. A 5‐ to 10‐cm hysterotomy incision was made in one of the horns of the uterus near the uterine body, and an attempt was made to remove all piglets through this hysterotomy. Occasionally, the uterus could not be completely exposed through the abdominal incision because of the large number or size of piglets. In this case, one or two additional hysterotomies were performed in the exposed uterine horn, and piglets were removed to facilitate exteriorization of the remaining uterus. After removal of all piglets, the entire uterus was again palpated to ensure that there were no piglets remaining in the uterus.
Hysterotomy incisions were closed with 2‐0 or 0 glycomer 631 or 2‐0, 0, 1, or 2 chromic gut by using either a Cushing or a Utrecht pattern, depending on surgeon preference. In 97 (88.18%) cases, hysterotomy incisions were closed with a single‐layer closure (Utrecht), and 13 (11.82%) cases were closed with a double‐layer closure (Cushing).
The serosal surface of the uterus was thoroughly lavaged with sterile saline to remove clotted blood and uterine fluid prior to replacing it in the abdomen. The abdomen was then lavaged with warmed, sterile saline, and blood clots were manually removed. The internal and external oblique muscles were apposed with 3 polyglactin 910 or 2 polydioxanone in a simple continuous or interrupted cruciate pattern. The subcutaneous tissues were apposed with 0 glycomer 631 in a simple continuous pattern. Skin was apposed with 0 glycomer 631 or 2 polydioxanone in a simple continuous Ford interlocking or interrupted cruciate pattern. After closure of the incision, animals were recovered from anesthesia, and auricular catheters were removed.
3.3. Surgical outcomes
The median litter size was eight piglets (range, 1‐14), with a median of five live (range, 0‐13) and one dead (range, 0‐11). The reported median number of piglets born prior to dystocia was one (range 0‐10).
One dam was hospitalized and died 2 days postoperatively of suspected septic shock. The diagnosis of septic shock was made based on tachycardia (>120 beats per minute [bpm], tachypnea (>50 bpm), dull mentation, hyperemic skin, congested mucous membranes, increased or decreased temperature (<101.6 °F, >103.6 °F), muscle tremors, and stiffness. 7 , 8 , 9 Two other dams were euthanized immediately after the procedure because of poor prognosis secondary to suspected sepsis and poor uterine health (dark uterine serosa, friable uterus, and absence of hemorrhage at the hysterotomy site) during surgery. One dam died of an unknown cause while under anesthesia. The remainder of the dams (106/110 [96.36%]) were discharged from the hospital after recovery from anesthesia.
3.4. Follow‐up
Information regarding the outcome of the dams that underwent cesarean section was available for 52 of the 106 (49.06%) dams that survived to discharge and was obtained via telephone interview with the owner 9 months to 5 years after the procedure. Thirty‐nine of 52 (75%) dams survived for 9 months or longer, seven (13.46%) dams were sent to slaughter, and six (11.54%) dams died after discharge within 48 hours of the procedure. Reasons for electing to send dams to slaughter included owner perception that the sow would require another cesarean section in the subsequent farrowing (n = 5 [71.42%]), it was the sow's second cesarean section (1 [14.29%]), and chronic anorexia and lethargy (1 [14.29%]).
Among the 52 dams with available follow‐up, postoperative complications were reported in 20 (38.46%) and included incisional site infection (n = 7 [35%]), postoperative anorexia (n = 4 [20%]), postoperative lethargy (n = 3 [15%]), metritis (n = 2 [10%]), delayed cycling compared to other sows in the herd that underwent normal parturition, (n = 1 [5%]), poor lactation (n = 1 [5%]), subcutaneous seroma formation (n = 1 [5%]), and chronic lethargy and anorexia (n = 1 [5%]).
Twenty‐seven dams were re‐bred by the owner, 23 (85.19%) of which carried a pregnancy to term. Among these 23, 13 (56.52%) had a normal, unassisted farrowing, seven (30.43%) farrowed with vaginal assistance provided by the owner, two (8.70%) required a second cesarean section, and one (4.35%) was euthanized during labor because of dystocia (Figure 2). Mean owner‐reported satisfaction with the procedure was 4 ± 1.
FIGURE 2.
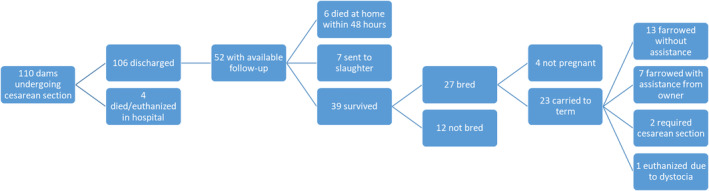
Flow chart summarizing outcomes of swine that underwent cesarean section for resolution of dystocia
4. DISCUSSION
In this study, swine that underwent cesarean section for resolution of dystocia had a good prognosis prognosis for survival of 6 months or longer and a fair to guarded prognosis for carrying at least one more pregnancy to term. Therefore, the authors' hypothesis that cesarean section would result in a satisfactory outcome for both survival and rebreeding was not supported, although results may have been hampered by lack of detail due to the reliance on owner observations for follow up information.
Large animal surgery and theriogenology resources cite duration of labor as a negative prognostic indicator for cesarean section in swine. 1 , 2 This retrospective study was dependent on owner‐reported data for duration of labor, and exact times for duration of labor were unknown for many of the cases included. This limitation prevents formulating conclusions regarding whether the duration of labor affected survival of the dams. Much of this information was based on rough estimates or time ranges because owners often were not present at the exact time the dam went into labor. Accurate determination of the duration of labor may have allowed detection of an impact on the dam survival as well as piglet survival. Follow‐up information regarding dam survival was available only for about half of the originally presenting animals. Within this group, all of the dams that spontaneously died after the procedure did so within 2 days of surgery. This finding provides evidence that positive outcome may be more likely when swine live beyond 2 days after surgery. Although postmortem data were not available, deaths occurring within 48 hours likely result from retained fetal membranes leading to septic metritis. 10 Other differentials could include hemorrhage, surgical site infection, and peritonitis. 11 Longer hospitalization with monitoring and additional treatment could result in an increased survival rate during this period, but may not always be a financially viable option for the owner.
Less than half of the swine with available follow‐up successfully carried at least one more pregnancy to term. The decision to send some of the animals to slaughter without an attempt to breed was based on owners' concerns regarding potential dystocia in the future if the swine were re‐bred. When an attempt was made to breed after surgery, sows had a good prognosis for achieving and maintaining pregnancy. However, just over half of these sows farrowed normally. The absence of veterinary assistance prevented definitive diagnosis of dystocia in seven of the sows requiring owner assistance during farrowing. Indeed, these sows may have received extra scrutiny by the owners because of their previous history.
The rate of stillborn piglets was higher in our population than in the report by Friendship et al, 5 in which the reported rate of stillborn piglets was only 0.2 per litter, with a mean litter size in swine cesarean section of 10 piglets. However, the animals included in Friendship et al 5 were in a laboratory setting in which cesarean sections were performed on sows at 113 days (mean gestation is 114‐115 days) of gestation 1 and prior to the onset of labor. Because the sows were not in labor, there was an absence of dystocia, likely contributing to the lower stillbirth rate. Jackson 12 examined stillbirth rates of sows in dystocia and found that several different factors have an influence on stillbirth rate including time in labor, with increased time in labor dramatically reducing piglet viability. Jackson 12 also found that increasing parity decreased stillbirth rate, and the stillbirth rate of first parity gilts was reported to be 21.8%. The relatively high number of dead piglets born to dams in the current study could be indicative of the number of gilts included in the study rather than the time in labor. In addition, because gilts produce smaller litters than multiparous sows, 13 this may also account for the smaller litter size in the study reported here.
Local or epidural anesthesia with combined mask inhalant anesthesia or injectable anesthesia is acceptable anesthetic protocol. 1 , 2 , 14 In swine cases of cesarean section for the relief of dystocia, sows may be in varying degrees of hypovolemia and shock. 15 Depth of anesthesia can be more easily and quickly altered with inhaled compared with injectable anesthesia; therefore, inhaled isoflurane was the anesthetic used to maintain general anesthesia throughout the procedure in all cases in this study. Orotracheal or nasotracheal intubation would have allowed for even more precise control of anesthesia as well as assisted ventilation and evaluation of end tidal CO2. In addition, bloodwork such as blood gas evaluation and electrolyte panels would have provided useful information for intraoperative anesthetic adjustment and fluid therapy. Because of the cost and additional personnel associated with such monitoring and economics of the market swine industry demanding that procedures associated with these animals must be profitable, additional anesthetic monitoring was not performed in any of the cases. Our results provide evidence that satisfactory dam and piglet survival outcomes can be achieved with isoflurane inhalant anesthesia during caesarean section.
Surgical approaches to cesarean section in swine include ventral midline, paramedian, ventrolateral, and paralumbar fossa. 2 , 11 The ventrolateral approach was selected in these cases. The ventrolateral approach offers benefits including ease of access to the uterine horns (unlike the flank approach) and the avoidance of the vasculature associated with the mammary chains (unlike ventral midline or paramedian approaches). 2 , 3 No major surgical complications were encountered with this approach, although surgical site infection or seroma was noted by the owners of some dams on follow‐up. These complications likely occurred because the incision is relatively ventral and prone to contamination or repeated abrasion. In addition, the incision is close to the mammary chain and may be exposed to contamination and tension secondary to nursing piglets.
Owners were generally highly satisfied with the procedure (mean score, 4/5), although this rating should be interpreted with caution. Survival of the sow or piglets or lower than expected cost could all improve satisfaction scores. In addition, the satisfaction scores may have been skewed by owners with higher satisfaction with the procedure being more willing to participate in a questionnaire regarding the procedure. If this was the case, the animals lost to follow‐up may have experienced more complications and a lower 6‐month survival than what we report here.
This study has several limitations. The retrospective nature of the study leaves many uncontrolled variables that likely affected the outcome in each individual case. In addition, follow‐up was variable in length and may have been affected by recall bias. Furthermore, follow‐up was not available for all cases, and response may be influenced by the outcome of the case.
In conclusion, cesarean section performed on swine under general anesthesia was associated with a good prognosis for dam survival in our clinical setting. Postoperative death of the dam was most likely to occur within the first 48 hours. The overall prognosis for a gilt or sow to become pregnant and successfully carry a litter to term after caesarean section was found to be fair to guarded. Owners should be counseled that a high number of sows becoming pregnant after a cesarean section may require assistance in subsequent deliveries.
CONFLICT OF INTEREST
The authors declare no conflicts of interest related to this report.
ACKNOWLEDGMENTS
Author Contributions: Lozier, JW, DVM, MS, DACVS‐LA: Contributions to conception and design of work, acquisition of data, interpretation of data, and manuscript preparation; VanHoy, GM, DVM, MS, DACVIM‐LA: Contributions to the conception and design of work, acquisition of data, and manuscript preparation; Jordan, BA, DVM: Acquisition of data and manuscript preparation; Muir, AJT, DVM: Acquisition of data and manuscript preparation; Lakritz, J, DVM, PhD, DACVIM, DACVCP: Conception and design of work and manuscript preparation; Hinds, CA, DVM, MS, DACVIM‐LA: Conception and design of work and manuscript preparation; Niehaus, AJ, DVM, MS, DACVS‐LA: Conception and design of work, interpretation of data, and manuscript preparation.
Lozier JW, VanHoy GM, Jordan BA, et al. Complications and outcomes of swine that underwent cesarean section for resolution of dystocia: 110 cases (2013‐2018). Veterinary Surgery. 2021;50:38–43. 10.1111/vsu.13530
REFERENCES
- 1. Cowart RP. Parturition and dystocia in swine In: Threlfall RR, Youngquist RS, eds. Current Therapy in Large Animal Theriogenology. 2nd ed. St Louis, MO: Saunders Elsevier; 2007:778‐784. [Google Scholar]
- 2. Callan RJ, Hackett RP, Fubini SL. Surgery of the swine reproductive system and urinary tract In: Fubini SL, Ducharme NG, eds. Farm Animal Surgery. 2nd ed. St Louis, MO: Elsevier; 2017:629‐630. [Google Scholar]
- 3. Mather EC. Lower flank incision for swine cesarean. Vet Med Small Anim Clin. 1966;61(9):890‐891. [PubMed] [Google Scholar]
- 4. Miniats OP, Jol D. Gnotobiotic pigs‐derivation and rearing. Can J Comp Med. 1978;42(4):428‐437. [PMC free article] [PubMed] [Google Scholar]
- 5. Friendship RM, Metzger KR, Robinson NP, Doig GS. Cesarean section in the sow: a retrospective analysis of litter size and stillbirth rate. Can Vet J. 1990;31(10):697‐699. [PMC free article] [PubMed] [Google Scholar]
- 6. Dimigen J. Cesarean secretion in market pigs. Dtsch Tierarztl Wochenschr. 1972;79(10):235‐237. [PubMed] [Google Scholar]
- 7. Robinson NA, Loynachan AT. Cardiovascular and hematopoietic systems In: Zimmerman JJ, Karriker LA, Ramirez A, Schwartz KJ, Stevenson GW, Zhang J, eds. Diseases of Swine. 11th ed. Hoboken, NJ: John Wiley & Sons; 2019:223‐233. [Google Scholar]
- 8. Sanford SE, Josephson GK, Rehmtulla AJ. Sudden death in sows. Can Vet J. 1994;35(6):388. [PMC free article] [PubMed] [Google Scholar]
- 9. Callan RJ. Examination of the surgical patient (pig) In: Fubini SL, Ducharme NG, eds. Farm Animal Surgery. 2nd ed. St Louis, MO: Elsevier; 2017:16‐22. [Google Scholar]
- 10. Fangman TJ, Shannon MC. Diseases of the puerperal period In: Youngquist RS, Threlfall WR, eds. Current Therapy in Large Animal Theriogenology. 2nd ed. St Louis, MO: Saunders Elsevier; 2007:790‐791. [Google Scholar]
- 11. Baird AN. Swine surgery In: Hendrickson DA, Baird AN, eds. Turner and McIlwraith's Techniques in Large Animal Surgery. 4th ed. Ames, IA: Wiley Blackwell; 2013:317‐319. [Google Scholar]
- 12. Jackson PG. The incidence of stillbirth in cases of dystocia in sows. Vet Rec. 1975;97(21):411‐412. [DOI] [PubMed] [Google Scholar]
- 13. Safranksy TJ, Cox NM. Clinical reproductive physiology and endocrinology of sows: mating management In: Threlfall RR, Youngquist RS, eds. Current Therapy in Large Animal Theriogenology. 2nd ed. St Louis, MO: Elsevier Saunders; 2007:738‐749. [Google Scholar]
- 14. Ko JCH, Thurmon JC, Benson JG, Tranquilli WJ. Olson WA. A new drug combination for use in porcine cesarean sections. Vet Clin North Am Food Anim Pract. 1993;88(5):466‐472. [Google Scholar]
- 15. Benson GJ. Anesthetic management of ruminants and swine with selected pathophysiologic alterations. Vet Clin North Am Food Anim Pract. 1986;2(3):677‐691. [DOI] [PubMed] [Google Scholar]