

Abstract
Background
Overactivity in the context of chronic pain (i.e. activity engagement that significantly exacerbates pain) is an important clinical issue that has gained empirical attention in the last decade. Current assessment concepts of overactivity tend to focus on frequency to quantify the severity of the pain behaviour. This study aimed to develop and validate a more comprehensive self‐assessment, the Overactivity in Persistent Pain Assessment (OPPA).
Methods
A sample of 333 individuals with chronic pain completed the OPPA. A subset of 202 individuals also completed a set of existing measures of pain‐related outcomes and activity patterns. The remaining 131 participants were provided with a second copy of the OPPA to fill in one week following their initial assessment.
Results
A principal component analysis confirmed that the OPPA items were best represented by a single construct. The OPPA was found to correlate with pain‐related measures in an expected way that is supported by both theory and qualitative data. When compared to existing overactivity measures, the OPPA was the only measure to contribute significantly to the regression models predicting higher levels of pain severity, more pain interference and lower levels of activity participation after controlling for age, gender and activity avoidance. In addition, the OPPA scale exhibited acceptable internal consistency and good test–retest reliability.
Conclusion
The results of this study reinforce the potentially important role of overactivity in the maintenance of pain‐related suffering and supports a corresponding assessment tool with preliminary psychometric evidence for clinical and research applications.
Significance
This study deconstructs the overactivity concept and develop a corresponding assessment based on five quantifiable severity features: severity of pain exacerbation, maladaptive coping strategies used, impact on occupational performance, recovery time and frequency. Results of the psychometric evaluation indicate that this comprehensive assessment of overactivity severity features may be necessary to understand the impact of overactivity on pain severity and physical functioning from both a clinical and research perspective.
1. INTRODUCTION
Exercise prescription and advice to remain active are widely accepted and utilized as treatment modalities for individuals with chronic pain (Booth et al., 2017). Recent studies, however, recognized that individuals with pain can do too much which can have a negative impact on their life (Andrews et al., 2015a, 2015b). Overactivity in the context of chronic pain refers to engagement in activity in a way that severely exacerbates pain intensity, resulting in a period of reduced functional capacity (Andrews et al., 2015a; Philips, 1988). Qualitative enquiries have revealed that habitual overactive individuals with chronic pain reported issues in a number of quality of life domains from poor sleep quality to reduced work capacity and negative emotions (Andrews et al., 2015b).
Several self‐report scales have been created to measure overactivity behaviour. The scales are usually part of an overall assessment of activity patterns including the Pain and Activity Relations Questionnaire (PARQ) (McCracken & Samuel, 2007), the Patterns of Activity Measure‐Pain (POAM‐P) (Cane et al., 2013) and, the Activity Patterns Scale (APS) (Esteve et al., 2016). Overactivity tends to be captured by means of frequency in which individuals with chronic pain engage in certain behaviours in these measures. For example, “I keep going until I can't stand the pain anymore” is rated using either a 5‐point or 6‐point Likert frequency scale (e.g. 0 = never; 4/5 = always).
Investigators have used the aforementioned measures to study the impact of overactivity behaviour on the quality of life of individuals with chronic pain. Higher scores on the PARQ confronting scale were associated with opioid use (Andrews et al., 2016b) and poor sleep quality (Andrews et al., 2016a), and higher levels of APS excessive persistence were positively linked to negative affect (Esteve et al., 2016). However, inconsistent associations between the scores of the overactivity scales and global measures of disability have been noted across studies; some revealed a positive (Cane et al., 2013), negative (Esteve et al., 2016; Luthi et al., 2018) or no association (Andrews et al., 2016a; Kindermans et al., 2011a, 2011b; McCracken & Samuel, 2007). In addition, the correlations between the POAM‐P overdoing scale and negative affect have also been incongruous across studies (Cane et al., 2013; Kindermans et al., 2011a, 2011b; Luthi et al., 2018). While these conflicting findings may be partially explained by differences in the study cohorts (Luthi et al., 2018) the assessment concept of overactivity could also possibly be a major contributing factor for these inconsistent results.
Current measures of overactivity in chronic pain focus on merely one aspect of the construct as an indicator of severity (i.e. the frequency of overactivity behaviour). This single facet may have neglected other quantifiable components of the construct which are inherent to the definition of overactivity, such as the magnitude of the pain exacerbation. In addition, both the PARQ confronting and POAM‐P overdoing scales incorporate items that are more reflective of task persistence (i.e. persisting with activities in spite of pain) than overactivity (i.e. persisting with activities to a point where pain is significantly exacerbated and alters functional capacity) (Andrews et al., 2015a; Kindermans et al., 2011b). While task persistence is a precursor to overactivity (Andrews et al., 2012), the behaviour is generally considered to be a different construct that is neither functional nor dysfunctional (Andrews et al., 2012; Kindermans et al., 2011b; Luthi et al., 2018).
The aim of this study was to develop a multifaceted self‐report severity measure specific to overactivity, the Overactivity in Persistent Pain Assessment (OPPA), and examine its psychometric properties in a cohort of individuals with chronic pain seeking treatment a tertiary multidisciplinary pain centre. We hypothesized that the OPPA would: (1) be psychometrically sound in terms of its structural validity, construct validity, test–retest reliability, and internal consistency and, (2) demonstrate stronger associations with pain‐related outcome measures when compared to the existing overactivity scales. A complete list of the strength and direction of hypothesized associations between the OPPA and other measures, based on theories (Birkholtz et al., 2004; Fordyce, 1976; Hanson & Gerber, 1990; Philips, 1988) and qualitative data (Andrews et al., 2015b), is displayed in Table 1. The APS (Esteve et al., 2016) was not included as a measure due to the APS being published after the current study was conceptualized.
TABLE 1.
Hypothesized associations between overactivity severity measured using the OPPA and pain measures
| Direction | Strength | Rationale | |
|---|---|---|---|
| Other overactivity measures | Positive | Moderate | Based on the assumption that other measures provide an incomplete assessment of the overactivity construct i.e. they should be related to the OPPA but not strongly |
| Activity avoidance | Positive | Small | Overactivity is theorized to result in increased activity avoidance overtime (Birkholtz et al., 2004; Philips, 1988) and some but not all overactive individuals report avoidance of non‐essential activities (Andrews et al., 2015b) |
| Activity pacing | No Association | No Association | Overactive individuals have described either infrequent use of activity pacing strategies or using pacing strategies regularly but ineffectively (Andrews et al., 2015b) |
| Depression | Positive | Moderate | Overactivity behaviour has been theorized to significantly worsen pain severity, mood, sleep quality and disrupt normal activity participation (Birkholtz et al., 2004; Fordyce, 1976; Hanson & Gerber, 1990; Philips, 1988). Qualitative data have supported these theoretical perspectives (Andrews et al., 2015b). |
| Anxiety | Positive | Moderate | |
| Stress | Positive | Moderate | |
| Pain severity | Positive | Moderate | |
| Pain interference | Positive | Moderate | |
| Activity participation | Negative | Moderate |
2. METHODS
Procedures used during the development and psychometric evaluation of the OPPA were informed by the COSMIN Study Design checklist for patient‐reported outcome measurement instruments (Mokkink et al., 2019; Mokkink et al., 2010).
2.1. Development of the Overactivity in Persistent Pain Assessment (OPPA)
Items of the OPPA were drafted by an occupational therapist with extensive experience in the study and treatment of overactivity in chronic pain (N.E.A). The overactivity concept was first deconstructed using the original descriptions and definitions of overactivity in the pain literature (Fordyce, 1976; Hanson & Gerber, 1990; Philips, 1988), the conceptual framework for functional capacity evaluation (Gibson & Strong, 2003), the operant behavioural model of chronic pain (Fordyce, 1976) and qualitative data (Andrews et al., 2015b). From this deconstruction, five quantifiable and progressive features were identified for inclusion in the OPPA. Figure 1 illustrates a graphical representation of these features which are described in more detail below.
FIGURE 1.

The deconstruction of the overactivity construct in a graphical form
Three quantifiable components were identified through examination of the original descriptions and definitions of overactivity (i.e. activity engagement that significantly exacerbates pain resulting in a period of reduced functional capacity). The first feature was the magnitude of the pain exacerbation that results from activity engagement labelled severity of pain exacerbation. The second and third features quantify the period of reduced functional capacity that results from the pain exacerbation. In accordance with the conceptual framework for functional capacity evaluation (Gibson & Strong, 2003), functional capacity was conceptualized as difficulties an individual has executing their normal daily activities otherwise known as occupational performance. The degree of difficulty experienced directly following a pain exacerbation was classed as the second feature which was labelled impact on occupational performance. The temporal nature of the functional capacity reduction can be quantified using time and this third feature was given the label recovery time. Drawing from the operant behavioural model, Fordyce (1976) originally proposed that overactivity is a learnt behaviour that is strengthened through negative reinforcement (i.e. a learned association between periods of rest and severe pain develops and rest is subsequently avoided). Qualitative findings have, however, suggested that the behaviour may be positively reinforced by events that occur during the recovery period such as presenting to an emergency department or taking more prescribed opioid medication (Andrews et al., 2015b). Hence, these maladaptive coping strategies may also be an indication of the severity of the pain behaviour denoting the fourth feature: maladaptive coping strategies used. The final feature draws from how overactivity is currently assessed aptly labelled frequency. Qualitative data have revealed some factors that may play a role in determining which individuals become habitually overactive in response to pain (e.g. personality traits) (Andrews et al., 2015b). While these factors are considered important when assessing the pain behaviour from a clinical perspective, it is unlikely that these factors are a direct indication of how severe the pain behaviour is and hence were not considered for inclusion as a single feature in the OPPA. In addition, long‐term consequences of habitual overactivity behaviour described by theorists and individuals with chronic pain (e.g. overall pain severity, disturbed sleep quality and difficulties maintaining employment (see: Hasenbring et al., 2020)) are considered possible outcomes that can be partially explained by the severity of overactivity behaviour and hence are not considered overactivity severity features.
Based on the conceptualization presented above, a single‐item format was further adopted to quantify each of the five features of overactivity in chronic pain in the OPPA. This was made by reference to two well‐validated and widely utilized health measures including the Owestry Disability Index (Fairbank & Pynsent, 2000) and EQ‐5D‐5L (Herdman et al., 2011). The use of the single‐item format was also considered to decrease the responders’ burden, and single‐item measures have been shown to have concurrent validity comparable to multi‐item measures (Bergkvist & Rossiter, 2007). The item responses were drawn from qualitative data (Andrews et al., 2015b) and clinical observations.
Following the draft version of the OPPA, the contents of the five OPPA items were presented at a continuing medical education session at a multidisciplinary pain centre located in a large tertiary hospital in Australia. There were 20 staff who attended the session and they were from occupational therapy, physiotherapy, psychology, psychiatry, medicine, or nursing. Staffs were invited to provide feedback on the clarity and content of draft items and rating responses. Meanwhile, the draft version was also administered to five individuals with chronic pain to assess responders’ comprehension and variation in responses. Feedback was obtained relating to the wording of questions/responses, the aptness of the rating responses, the order of the questions and the length of the questionnaire. Minor revisions were made to the wording of two questions and two rating responses, resulting in the final version of the items, rating responses and scoring procedure displayed in Table 2.
TABLE 2.
Final items and responses for the overactivity in persistent pain assessment (OPPA)
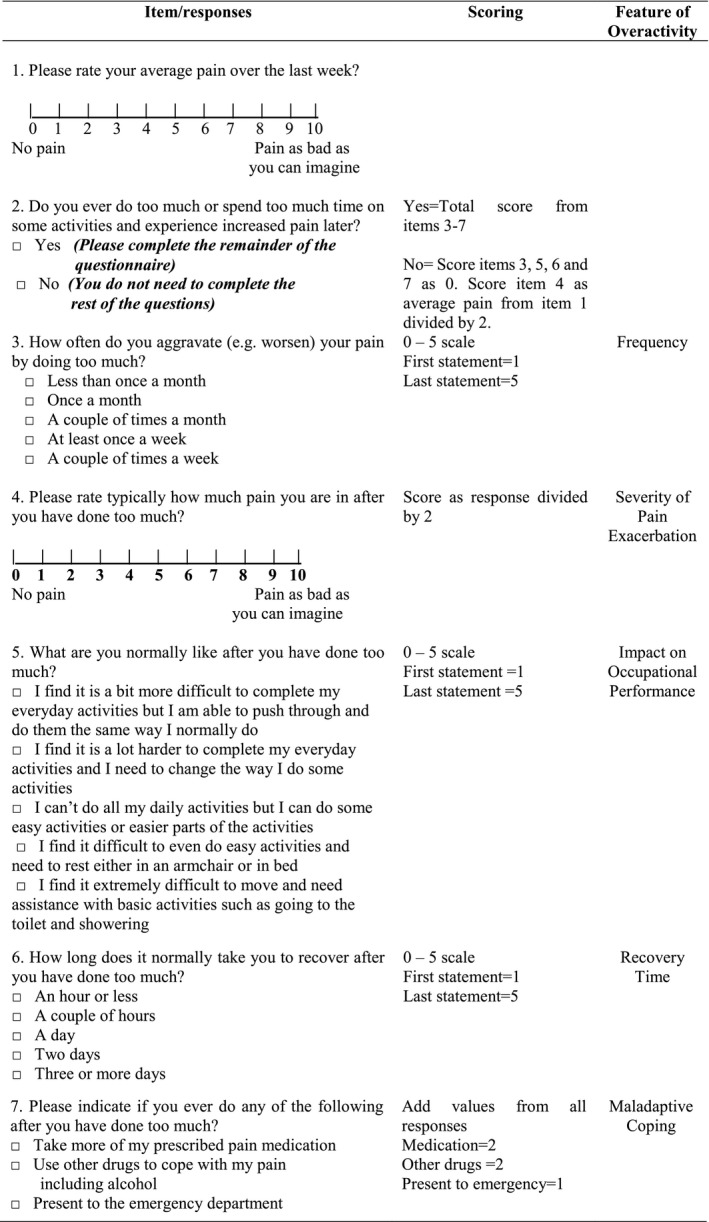
In the OPPA final version, each of the five overactivity features are transformed to a 0 – 5 rating scale based on specific algorithms (Table 2), with higher scores indicative of more severe overactivity behaviour in that feature. As individuals who are not overactive or deny being overactive would struggle to answer some questions pertaining to the severity of overactivity features, an initial question asks individuals to indicate if they ever do too much or spend too much time on some activities and experience increased pain later. If individuals answer no to this question, they are automatically given low scores for the remaining OPPA items as detailed below. This is equivalent to the scores of individuals who rate overactivity items consistently as zero (i.e. “I never engage in overactivity behaviour”) on existing continuous overactivity measures.
Three items of the OPPA (i.e. Frequency, Impact on Occupational Performance and Recovery Time) are scored using a Likert scale comprising of fived ranked statements. Individuals who have previously selected ‘no’ for the second question “Do you ever do too of much or spend too much time on some activities and experience increased pain later?” are given a score of zero for the above three items. This scoring indicates never being overactive, no recovery time and activity‐related pain exacerbations having no impact on occupational performance. The fourth question asks individuals to quantify the severity of their pain exacerbation using an 11‐point numerical rating scale. As individuals with chronic pain who are not overactive are unlikely to rate their pain as zero, methods were used to establish a more appropriate lower limit reference point for this item; those people who deny engaging in overactivity behaviour are instead scored based on their average pain score from the first question. This scoring is reflective of the pain intensity that is normal for that individual without exacerbating their pain from overactivity behaviour. Hence, pain exacerbation scores are considered on a scale where normal or average pain intensity is the lower limit reference point. All these 11‐point scores of pain exacerbation or average pain are subsequently transformed to the 0 – 5 rating scale for Severity of Pain Exacerbation by diving the responses by two.
The final item of the OPPA measures maladaptive coping during the reduced period of functional capacity based on weighted scores from three binary response items on taking extra prescribed medication, having more substance use and going to the emergency department. The first two responses are given a higher weighted score of 2 given the potential impact on life expectancy (Ye et al., 2018), compared to the last item with an unweighted score of 1. Thus, a combination of all three response options produces a score ranging from 0 to 5. Similarly, both individuals who deny engaging overactivity behaviour and those who do not engage in any of the three coping strategies to manage their activity‐related pain exacerbations are given a score of zero for this Maladaptive Coping item.
2.2. Participants and procedure
A total of 333 individuals with chronic pain who attended an outpatient clinic at a multidisciplinary pain centre (MPC) located in a large tertiary hospital in Australia were recruited for the psychometric evaluation. The inclusion criteria for this consecutive sample were (1) outpatient of the MPC, (2) persistent non‐cancer pain for at least 3 months, (3) generalized pain distribution impacting on the participant's gross movement (i.e., gross movement patterns increase the participants pain), (4) English literate, (5) 16 years and over, and 6) ability to provide informed consent.
Participants meeting the selection criteria were identified by administration staff at the MPC on presentation to their outpatient appointment. All eligible participants completed the OPPA and a demographic questionnaire at the time of their appointment. These data were used to establish the structural validity and internal consistency of the OPP based on a reflective model (Mokkink et al., 2019). Participants were then divided into one of two subgroups for testing different aspects of the psychometric properties of the OPPA, based on their appointment status at the MPC. Participants who attended a review or follow‐up appointment were invited to complete an additional set of written questionnaires in order to assess the construct validity of the OPPA (i.e. hypothesis testing) at the time of their appointment (subgroup 1). Patients who attended a new appointment in the MPC were provided with a second copy of the OPPA to complete one week following their appointment to assess the test–retest reliability and measurement error of the OPPA (subgroup 2). We chose new patients to specifically assess the test–retest reliability, because they were unlikely to receive any active treatment to address overactivity behaviour and were expected to remain relatively stable between both assessments. Participants attending a review appointment had previously received a wide variety of treatments from the centre, depending on their treatment plan, including medical procedures (e.g. injections/infusions), pain management programs and individual allied health treatment.
The additional set of questionnaires completed by subgroup 1 comprised of existing measures of overactivity/pain‐related activity patterns, pain severity, psychological functioning, pain interference and activity participation. Subgroup 2, who were provided with a second OPPA and a replied paid envelope, were sent a reminder via text message to complete the OPPA one week following their appointment. If the OPPA was not returned to the clinic three weeks following their appointment they received a second reminder via text message. The procedure and flow of participants through the different phases of this study are illustrated in Figure 2.
FIGURE 2.
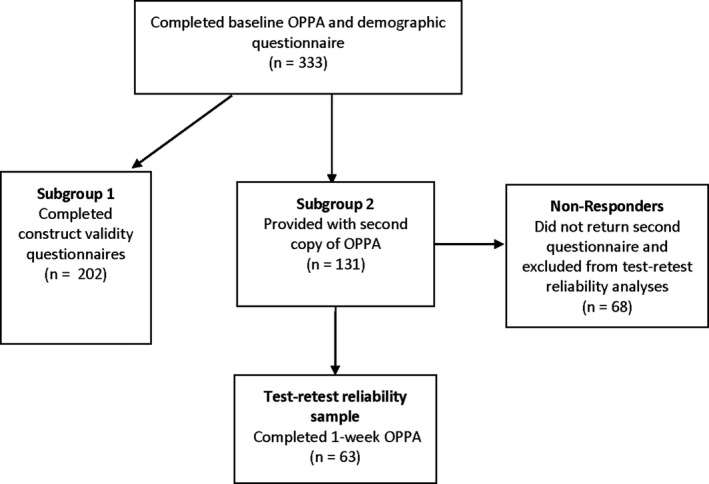
Flow of participants through the different phases of the study
All participants were provided with written and verbal information about the study, and written informed consent was required before participation. The Royal Brisbane and Women's Hospital's Human Research Ethics Committee (Number: HREC/17/QRBW/169 and HREC/17/QRBW/112) approved the protocol for this study.
2.3. Measures
2.3.1. Demographic questionnaire
Information on the participants’ age, gender, living environment, level of education, employment status, pain location and duration of pain was gathered.
2.3.2. Overactivity assessment in persistent pain (OPPA)
The version of the OPPA as displayed in Table 2 was administered.
2.3.3. Pain and activity relations questionnaire (PARQ)
The PARQ (McCracken & Samuel, 2007) is a 21‐item self‐report measure of activity patterns for pain populations. The measure consists of three scales: avoidance (8 items), confronting (7 items) and pacing (6 items). Sample items include: “I avoid important activities when I am in pain” (avoidance), “I alternate between doing nothing and pushing too hard” (confronting) and “I split tasks into parts and do them one step at a time” (pacing). Participants rate the frequency with which they engage in each behaviour on a 6‐point Likert scale (0 = never, to 5 = always). Validity and internal consistency of the PARQ have been found to be adequate based on initial psychometric testing by the developers (McCracken & Samuel, 2007). In addition, Andrews and colleagues provided support for the validity of the confronting subscale as a measure of habitual overactivity (Andrews et al., 2015a).
2.3.4. Patterns of activity measure‐pain (POAM‐P)
The POAM‐P (Cane et al., 2013) uses three scales (i.e. overdoing, avoidance and pacing) to assess the activity patterns of individuals with chronic pain. Each scale comprises of 10 items and participants rate items on a 5‐point frequency Likert scale (0 = not at all, to 4 = all the time). Sample items include: “I avoid activities that I know will make my pain worse” (avoidance), “When I do an activity I do the whole thing all at once” (overdoing), and “I do activities at a slow and steady pace” (pacing). The POAM‐P has adequate psychometric properties based on initial psychometric testing by the developers (Cane et al., 2013).
2.3.5. Depression anxiety stress scales 21 (DASS‐21)
The DASS‐21 (Lovibond & Lovibond, 1995) comprises of three scales that assess negative affective states: depression, anxiety and stress. Each scale includes seven items, with items measured on a 4‐point Likert scale (0 = did not apply to me at all, to 3 = applied to me very much or most of the time), based on participant's experience of the past week. Sample items include: “I found it hard to wind down” (stress), “I felt down‐hearted and blue” (depression) and “I felt I was close to panic” (anxiety). The DASS‐21 has been widely used in clinical and non‐clinical samples and there is sufficient high‐quality evidence for the criterion and construct validity of the measure (see review:Lee et al., 2019).
2.3.6. West Haven‐Yale Multidimensional Pain Inventory (WHYMPI)
The WHYMPI (Kerns et al., 1985) was developed to assess several dimensions of the chronic pain experience. It contains 52 items and 12 subscales. For the purpose of this study the following subscales were utilized: Interference, Pain Severity and the four activity participation subscales (i.e. Household Chores, Outdoor Work, Activities Away from Home and Social Activities). The activity participation subscales assess participants’ self‐reported participation in common daily activities. Participants indicate how often they complete activities on a 7‐point frequency Likert scale (0 = never to 6 = very often). Items from the four subscales are combined to create a General Activity Score. The 9‐item interference subscale measures perceived interference of pain in various areas of participants’ functioning such as ability to work and ability to participate in leisure activities. Three items assess pain severity. All pain severity and pain interference items are measured on a 7‐point Likert scale with higher scores indicating more severe pain or higher levels of pain interference. The WHYMPI has been used in diverse chronic pain conditions, and is reliable and valid (see review: Peipert et al., 2018). In addition, the WHYMPI is a recommended instrument for the assessment of individuals suffering from chronic pain based on an evidenced‐based consensus review (Dworkin et al., 2005).
2.4. Statistical analysis
All statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS) version 25.0 for windows. All data were initially assessed for missing data, linearity, constant variance and outliers. Additionally, floor and ceiling effects were examined for OPPA items and the total score. The percentage of participants who had at least one missing response was: 3% (PARQ), 10% (POAM‐P), 7% (DASS‐21) and 3% (WHYMPI). As per the scoring instruction of the WHYMPI and DASS‐21 (Kerns et al., 1985; Lovibond & Lovibond, 1995), missing items were replaced with the average score for that scale; if over 25% of items were missing, missing data resulting in the exclusion of that case from analysis. The numbers of excluded cases were: 3 (PARQ), 11 (POAM‐P), 1 (DASS‐21) and 5 (WHYMPI). A series of independent measures t‐tests and chi squared statistics were performed to examine the difference in the demographics and OPPA scores at the first assessment between non‐responders and responders who were included in the test–retest subgroup. As average pain intensity over the past week (i.e. question 1 of the OPPA) is used to establish a lower limit reference point for another item, we also tested whether there was a significant difference in responses to this item between those who denied overactivity behaviour and those who filled in the remainder of the OPPA.
To examine the structural validity of the OPPA, a principal component analysis (PCA) using direct oblimin rotation was conducted on the whole sample (n = 333) to explore if the items were best represented by one or more construct(s). The correlation between the items, the Bartlett Test of Sphericity and the Kaiser‐Meyer‐Olkin Measure of Sampling Adequacy were performed prior to the PCA to ensure the data suitability for the identity matrix, sampling adequacy. The eigenvalue‐one criterion was used to determinate the number of meaningful components. A cut‐off of 0.40 for the component loading was used to reduce items (Stevens, 1992).
Next, the construct validity of the OPPA was evaluated by correlating the OPPA scores to the scores of other overactivity measures, measures of activity avoidance, activity pacing, pain severity, pain‐related disability and psychological functioning. Cohen's conventions to interpret the effect size of correlations are reported as follows: no association r < 0.1, small association r = 0.1–0.29, moderate association r = 0.30–0.49, large association r > 0.5 (Cohen, 1988; Statistical Solutions, 2020). In addition, we were interested in whether the OPPA had superior ability to predict pain severity, pain‐related disability and psychological functioning, when compared with the other existing overactivity scales (i.e., the PARQ confronting subscale and the POAM‐P overdoing subscale). Thus, a series of hierarchical linear regression models were performed, where four predicted variables (i.e. DASS‐21 total score, WHYMPI Pain Severity, WHYMPI Interference, and WHYMPI General Activity) were treated as the dependent variable separately in each model. A total of four separate models were produced for each of the three independent variables relating to overactivity when they were entered in step 2, after controlling for age, gender, and PARQ Avoidance in step 1. Activity avoidance was controlled for in these models as it was hypothesized that activity avoidance would be associated with both overactivity severity and the dependent variables. Numerous treatment models target activity avoidance while largely neglecting the potential effects of overactivity (e.g. Darnall et al., 2018; Vlaeyen et al., 2002). As such, we were also interested in establishing the effect of overactivity severity on pain outcomes after controlling for activity avoidance. The total R 2 and R 2 change values were reported and compared across each model. Variance inflation factor (VIF) values were produced and residuals from regression models were checked for linearity, normality and equality of variance.
To examine the test–retest reliability of the OPPA, interclass correlation coefficients (ICC) with 95% confident intervals were calculated based on the 2‐way mixed‐effects model with absolute agreement (Koo & Li, 2016) at both item and total scale levels. A Bland‐Altman plot was produced for the OPPA total scores to evaluate measurement error and the level of agreement between the responses at the two time points. The average difference between the measurements and Limits of Agreement (mean difference ± 1.96SD) were calculated and plotted. The internal consistency was calculated for the total sample (n = 333) using Cronbach's alpha coefficient.
3. RESULTS
3.1. Demographics for study cohorts
The demographic information of the study cohorts are presented in Table 3. The demographics across the different subgroups were statistically comparable. Participants were predominately female, lived with a partner and were unemployed secondary to pain. Over half of the sample had lower back and lower limb pain with an average pain duration of 12 years. The average age for the entire cohort was 50.3 years. For the test–retest reliability testing, there were 68 (51.9%) participants who did not return the OPPA at the second assessment. These non‐responders were more likely to be younger (t(129) = −4.21, p < 0.001), live with children (χ2(1, N = 131) = 4.08, p = 0.04) and employed full‐time (χ2(5, N = 131) = 20.23, p = 0.001) compared to the responders in the test–retest reliability subgroup. The mean OPPA total baseline score was however comparable between these two subgroups (t(129) = 0.17, p = 0.86). Average pain intensity over the past week (i.e. item one of the OPPA) was also statistically comparable between those who denied overactivity tendencies and those who reported being overactive (t(200) = −1.13, p = 0.26).
TABLE 3.
Characteristics of the study populations
| Demographic variable | Total % (N = 333) | Construct validity sample % (N = 202) | Test–retest reliability responders % (N = 63) | Test–retest reliability non‐responders % (N = 68) |
|---|---|---|---|---|
| Gender | ||||
| Male | 38.7 (129) | 37.1 (75) | 39.7 (25) | 42.6 (29) |
| Female | 61.3 (204) | 62.9 (127) | 60.3 (38) | 57.4 (39) |
| Age (years) a | 50.3 (17–84) | 52.4 (19–78) | 52.67 (19–84) | 42.03 (17–76) |
| Pain Duration (years) a | 12.2 (0.6–50) | 12.7 (0.8–49) | 11.85 (0.6–50) | 11.1 (0.6–50) |
| Pain Location (incidence) | ||||
| Head/face | 15.6 (52) | 16.3 (33) | 14.3 (9) | 13.2 (9) |
| Upper limb | 34.7 (116) | 33.7 (68) | 34.9 (22) | 38.2 (26) |
| Neck | 35.3 (118) | 36.1 (73) | 34.9 (22) | 32.4 (22) |
| Upper back | 34.7 (116) | 27.2 (55) | 20.6 (13) | 32.4 (22) |
| Lower back | 69.5 (232) | 72.8 (147) | 63.5 (40) | 66.2 (45) |
| Chest | 9.6 (32) | 8.9 (18) | 6.3 (4) | 14.7 (10) |
| Abdomen/groin | 20.7 (69) | 17.8 (36) | 23.8 (15) | 26.5 (18) |
| Lower limb | 54.5 (182) | 54.0 (109) | 54.0 (34) | 58.8 (40) |
| Total body | 3.6 (12) | 3.5 (7) | 4.8 (3) | 2.9 (2) |
| Average pain intensity | 5.97 (0–10) | 5.96 (1–10) | 6.05 (2–10) | 5.95 (0–10) |
| Living situation | ||||
| With partner | 53.3 (178) | 55.0 (111) | 55.6 (35) | 47.1 (32) |
| With children | 24 (80) | 24.3 (49) | 15.9 (10) | 30.9 (21) |
| With other family | 12 (40) | 11.9 (24) | 9.5 (6) | 14.7 (10) |
| With friends/flatmate | 9 (30) | 7.9 (16) | 15.9 (10) | 5.9 (4) |
| Lives alone | 20.7 (69) | 20.8 (42) | 19 (12) | 20.6 (14) |
| Education level | ||||
| Primary school | 4.2 (14) | 3.0 (6) | 7.9 (5) | 4.4 (3) |
| Junior high school | 25.4 (85) | 27.7 (56) | 22.2 (14) | 22.1 (15) |
| Senior high school | 24.6 (82) | 22.3 (45) | 28.6 (18) | 27.9 (19) |
| Tertiary non‐university | 27.5 (92) | 27.7 (56) | 25.4 (16) | 29.4 (20) |
| Tertiary university | 18.0 (60) | 19.3 (39) | 14.3 (9) | 16.2 (11) |
| Employment status | ||||
| Employed full‐time | 14.4 (48) | 13.4 (27) | 7.9 (5) | 23.5 (16) |
| Employed part‐time | 11.4 (38) | 12.4 (25) | 12.7 (8) | 7.4 (5) |
| Retired | 18.3 (61) | 21.3 (43) | 23.8 (15) | 4.4 (3) |
| Home duties/carer | 5.1 (17) | 4.5 (9) | 6.3 (4) | 5.9 (4) |
| Unemployed due to pain | 44.3 (148) | 42.1 (85) | 36.5 (23) | 55.9 (38) |
| Unemployed other reasons | 6.6 (22) | 6.4 (13) | 11.1 (7) | 2.9 (2) |
| Denied overactivity tendencies | 9.3 (31) | 6.9 (14) | 15.9 (10) | 10.3 (7) |
Values = Mean (Range).
3.2. Structural validity: Principal component analysis
The screening statistics of data suitability indicated that the data were appropriate for principal component analysis. All but one inter‐item correlation was above 0.30. The Kaiser‐Meyer‐Olkin measure of Sampling Adequacy was 0.81, well above the commonly recommended value of 0.6, and the Bartlett's test of sphericity was significant (χ2 (10) = 499.67, p < 0.001).
The PCA revealed only one component with an eigenvalue greater than 1 (2.73) among the five OPPA items. This component explained 54.66% of the total variance. Item loadings for the component and communalities are displayed in Table 4. All of the five OPPA items met the component loading cut‐off of 0.40 and hence were retained.
TABLE 4.
Component loadings and communalities based on a principal component analysis (N = 333)
| Item | Component loading | Communalities |
|---|---|---|
| Frequency: How often do you aggravate (e.g. worsen) your pain by doing too much? | 0.84 | 0.71 |
| Severity of Pain Aggravation: Please rate typically how much pain you are in after you have done too much? | 0.61 | 0.37 |
| Impact on Occupational Performance: What are you normally like after you have done too much? | 0.83 | 0.69 |
| Recovery Time: How long does it normally take you to recover after you have done too much? | 0.82 | 0.67 |
| Maladaptive Coping: Please indicate if you ever do any of the following after you have done too much? | 0.54 | 0.29 |
3.3. Distribution of OPPA items and the total score
The floor and ceiling effects for the OPPA items and the total score are displayed in Table 5. Both OPPA Frequency and OPPA Maladaptive Coping had a skewed distribution. OPPA Frequency was negatively skewed with just over 50% of the sample selecting the highest response. Conversely, OPPA Maladaptive Coping was positively skewed; close to a third of the sample denied using any maladaptive coping strategies following an activity‐related pain exacerbation and scored zero for this item. Neither a ceiling nor floor effect was observed for the OPPA total score which resembled a normal distribution.
TABLE 5.
Means, standard deviation values and correlations between the OPPA scores and existing measures of overactivity
| n | Floor Effect a | Ceiling Effect b | Mean (SD) |
PARQ Confronting ρ (p) |
POAM‐P Overdoing ρ (p) |
|
|---|---|---|---|---|---|---|
| PARQ confronting | 199 | – | – | 3.34 (0.73) | ||
| POAM‐P overdoing | 191 | – | – | 24.08 (7.68) | 0.75 (<0.001) | |
| OPPA frequency | 202 | 6.9 | 53 | 4.03 (1.46) | 0.35 (<0.001) | 0.21 (0.004) |
| OPPA severity of pain aggravation | 202 | 0.5 | 12.9 | 3.99 (0.74) | 0.15 (0.03) | 0.10 (0.16) |
| OPPA impact on occupational performance | 202 | 6.9 | 4.5 | 2.88 (1.28) | 0.08 (0.26) | 0.13 (0.08) |
| OPPA recovery time | 202 | 6.9 | 15.8 | 3.26 (1.29) | 0.10 (0.16) | 0.01 (0.85) |
| OPPA maladaptive coping | 202 | 30.7 | 2.0 | 1.63 (1.29) | 0.00 (0.99) | 0.08 (0.30) |
| OPPA total | 202 | 0.0 | 0.0 | 15.80 (4.36) | 0.17 (0.02) | 0.15 (0.04) |
OPPA, overactivity in persistent pain assessment; PARQ, pain and activity relations questionnaire; POAM‐P, patterns of activity measure‐pain.
Percentage of sample that were given the lowest possible score.
Percentage of the sample that were given the highest possible score.
3.4. Hypotheses testing for construct validity: Correlation with similar or related measures
As scores for the individual OPPA items are ordinal in nature and some items were not normally distributed Spearman's rho coefficients are reported. Spearman's correlation coefficients between the OPPA items and scores of the two existing overactivity measures (i.e. PARQ Confronting and POAM‐P overdoing) are displayed in Table 5. A small significant positive correlation (ρ=0.21) was found between the OPPA Frequency item and the POAM‐P Overdoing scale. Higher scores on the OPPA Frequency item were also significantly moderately associated with higher levels of the PARQ Confronting scale (ρ=0.35). A small significant positive correlation was observed between the OPPA Severity of Pain Aggravation item and PARQ Confronting scale (ρ=0.15). No significant association between the two overactivity measures and the remaining three OPPA items were found. However, a small significant positive correlation between the OPPA total score and both the existing overactivity measures was revealed (ρ=0.15–0.17).
Spearman's correlation coefficients between the OPPA total score, measure of activity pacing, activity avoidance, psychological functioning, pain severity, pain interference and activity participation are displayed in Table 6. A small significant positive correlation was found between the OPPA and both measures of activity avoidance (i.e. PARQ‐Avoidance and POAM‐P‐Avoidance). No significant association was found between the OPPA and measures of activity pacing. Higher scores on the OPPA were significantly moderately associated with higher levels of stress and depression as measured by the DASS‐21. A small significant positive association between the OPPA and higher levels of anxiety was also found. Significant moderate associations were observed between the OPPA and higher levels of both pain severity and pain interference. In addition, small significant positive correlations were found between the OPPA and reduced participation in household chores, outdoor work, social activities and activities outside the home as measured by the WHYMPI.
TABLE 6.
Means, standard deviation values and correlations between the OPPA total score and measures of pacing, activity avoidance, negative affect, pain‐related disability and pain severity
| n | Mean (SD) |
OPPA total ρ (p) |
|
|---|---|---|---|
| PARQ avoidance | 199 | 3.04 (0.95) | 0.20 (0.005) |
| POAM‐P avoidance | 191 | 23.17 (7.79) | 0.21 (0.003) |
| PARQ pacing | 199 | 3.22 (0.98) | −0.08 (0.26) |
| POAM‐P pacing | 191 | 22.34 (0.73) | 0.03 (0.68) |
| DASS−21 depression | 201 | 16.49 (12.06) | 0.30 (<0.001) |
| DASS−21 anxiety | 201 | 13.23 (10.36) | 0.23 (0.001) |
| DASS−21 stress | 201 | 18.11 (10.86) | 0.35 (<0.001) |
| DASS−21 total | 201 | 47.83 (29.99) | 0.33 (<0.001) |
| WHYMPI pain severity | 197 | 4.23 (1.07) | 0.41 (<0.001) |
| WHYMPI interference | 197 | 4.15 (0.91) | 0.40 (<0.001) |
| WHYMPI household chores | 198 | 3.80 (1.35) | −0.20 (0.005) |
| WHYMPI outdoor work | 198 | 1.38 (1.40) | −0.18 (0.01) |
| WHYMPI activities away from home | 198 | 2.34 (1.10) | −0.26 (<0.001) |
| WHYMPI social activities | 198 | 2.14 (1.17) | −0.19 (0.007) |
| WHYMPI general activity | 198 | 2.41 (0.96) | −0.28 (<0.001) |
Abbreviations: DASS‐21, 21 item depression anxiety stress scales; OPPA, overactivity in persistent pain assessment; PARQ, pain and activity relations questionnaire; POAM‐P, patterns of activity measure‐pain; WHYMPI, west haven‐yale multidimensional pain inventory.
Table 7 displays the results of hierarchical linear regressions when comparing the contribution of the OPPA and the two existing overactivity scales in the prediction of pain severity, pain‐related disability and psychological functioning. All base models (i.e. step 1) were significant, where the age, gender and activity avoidance accounted for 10% of the variance in psychological functioning (F (3,195) = 7.12, p < 0.001); 16% of the variance in pain severity (F (3,190) = 11.79, p < 0.001); 5% of the variance in pain interference (F (3,190) = 3.12, p = 0.03) and 7% of the variance in activity participation (F (3,191) = 5.04, p = 0.002).
TABLE 7.
Summary of hierarchical regression analysis for psychology functioning, pain interference, activity participation and pain severity
| Dependent variable | Model/step | Variables | β | R 2 | R 2 change | F change |
|---|---|---|---|---|---|---|
| DASS−21 total | All models: Step 1 | PARQ avoidance | 0.26** | 0.10 | 0.10 | 7.12** |
| Gender | 0.06 | |||||
| Age | −0.16* | |||||
| Model 1: Step 2 | OPPA Total | 0.23** | 0.15 | 0.05 | 11.43** | |
| PARQ Avoidance | 0.22** | |||||
| Gender | 0.14 | |||||
| Age | −0.13 | |||||
| Model 2: Step 2 | PARQ Confronting | 0.18** | 0.13 | 0.03 | 6.99** | |
| PARQ Avoidance | 0.27** | |||||
| Gender | 0.02 | |||||
| Age | −0.15* | |||||
| Model 3: Step 2 | POAM‐P Overdoing | 0.27** | 0.18 | 0.07 | 16.02** | |
| PARQ Avoidance | 0.28** | |||||
| Gender | 0.05 | |||||
| Age | −0.15* | |||||
| WHYMPI Pain Severity | All Models: Step 1 | PARQ Avoidance | 0.39** | 0.16 | 0.16 | 11.77** |
| Gender | −0.06 | |||||
| Age | −0.05 | |||||
| Model 1: Step 2 | OPPA Total | 0.40** | 0.30 | 0.15 | 39.75** | |
| PARQ Avoidance | 0.32** | |||||
| Gender | −0.12 | |||||
| Age | 0.01 | |||||
| Model 2: Step 2 | PARQ Confronting | 0.08 | 0.16 | 0.01 | 1.39 | |
| PARQ Avoidance | 0.40** | |||||
| Gender | −0.07 | |||||
| Age | −0.05 | |||||
| Model 3: Step 2 | POAM‐P Overdoing | 0.09 | 0.16 | 0.01 | 1.81 | |
| PARQ Avoidance | 0.39** | |||||
| Gender | −0.06 | |||||
| Age | −0.03 | |||||
| WHYMPI Interference | All models: Step 1 | PARQ Avoidance | 0.21** | 0.05 | 0.05 | 3.12* |
| Gender | 0.01 | |||||
| Age | −0.04 | |||||
| Model 1: Step 2 | OPPA Total | 0.30** | 0.13 | 0.08 | 18.03** | |
| PARQ Avoidance | 0.16* | |||||
| Gender | −0.04 | |||||
| Age | −0.01 | |||||
| Model 2: Step 2 | PARQ Confronting | 0.12 | 0.06 | 0.01 | 2.55 | |
| PARQ Avoidance | 0.22** | |||||
| Gender | −0.02 | |||||
| Age | −0.04 | |||||
| Model 3: Step 3 | POAM‐P overdoing | 0.08 | 0.06 | 0.01 | 1.31 | |
| PARQ avoidance | 0.23** | |||||
| Gender | −0.01 | |||||
| Age | −0.02 | |||||
| WHYMPI general activity | All models: Step 1 | PARQ avoidance | −0.25** | 0.07 | 0.07 | 5.04** |
| Gender | −0.10 | |||||
| Age | −0.03 | |||||
| Model 1: Step 2 | OPPA Total | −0.17* | 0.10 | 0.03 | 5.26* | |
| PARQ Avoidance | −0.22** | |||||
| Gender | −0.08 | |||||
| Age | −0.05 | |||||
| Model 2: Step 2 | PARQ confronting | 0.12 | 0.09 | 0.01 | 2.80 | |
| PARQ avoidance | −0.24** | |||||
| Gender | −0.12 | |||||
| Age | −0.03 | |||||
| Model 3: Step 2 | POAM‐P overdoing | 0.09 | 0.07 | 0.01 | 1.56 | |
| PARQ avoidance | −0.23** | |||||
| Gender | −0.10 | |||||
| Age | −0.03 |
Abbreviations: DASS‐21, 21 item depression anxiety stress scales; OPPA, overactivity in persistent pain assessment; PARQ, pain and activity relations questionnaire; POAM‐P, patterns of activity measure‐pain; WHYMPI, west haven‐yale multidimensional pain inventory.
p < 0.05.
p < 0.01.
The addition of the OPPA total scale in the model at step 2 accounted for a significant amount of the variance for all predicted variables. Introducing OPPA overactivity explained an additional 5% of the variation in psychological functioning (FΔ(4,194) = 11.43, p = .001); 15% of the variation in pain severity (FΔ(4,189) = 39.75, p < .001); 8% of the variation in pain interference (FΔ(4,189) = 18.03, p < 0.001) and 3% of the variance in activity participation (FΔ(3,190) = 5.26, p = 0.02). Higher levels of overactivity severity as measured by the OPPA total scale were significantly associated with poorer psychological functioning (B = 1.59; p = 0.001; 95% CI, 0.66–2.52), more severe pain (B = 0.10; p < 0.001; 95% CI, 0.07–0.13), more pain interference (B = 0.06; p < .001; 95% CI, 0.03–0.09), and lower levels of activity participation (B = −0.04; p = 0.02; 95% CI, −0.07 to 0.01).
Conversely, the PARQ Confronting and POAM‐P Overdoing scales were found not to be significant predictors of pain severity, pain interference or activity participation when they were added to the models at step 2. However, the addition of either PARQ or POAM‐P Overactivity scale to the base models of psychological function was found to significantly improve the explained variance. Furthermore, the POAM‐P Overdoing scale appeared to be the strongest predictor, compared to the OPPA and PARQ scales, which accounted for an additional 7% of the variation in psychological functioning (FΔ(4,183) = 16.03, p < 0.001). Residual and scatter plots indicated that the assumptions of normality, linearity and homoscedasticity were satisfied for all models. All VIF values were <2 indicated that multicollinearity was not present in the models.
3.5. Test–retest reliability, measurement error and internal consistency
At the item level, the single‐measure ICC values were as follows: Frequency (ICC = 0.74, 95%CI = 0.60–0.83, F(62,62) = 6.52, p < 0.001); Severity of Pain Exacerbation (ICC = 0.53, 95%CI = 0.34–0.70, F(62,62) = 3.25, p < 0.001); Impact on Functional Performance (ICC = 0.73, 95% CI = 0.59–0.83, F(62,62) = 6.39, p < 0.001); Recovery Time (ICC = 0.74, 95%CI = 0.60‐0.83, F(62, 62) = 6.63, p < 0.001); and Maladaptive Coping (ICC = 0.84, 95%CI = 0.76‐0.90, F(62,62) = 11.69, p < 0.001). At the total scale level, the single‐measure ICC value was 0.83 with a 95% confidence interval from 0.75 to 0.90 (F(62,62) = 11.35, p < 0.001).
The Bland‐Altman plot, displayed in Figure 3, illustrates the level of agreement between baseline and 1‐week OPPA scores. The overall bias was low (−0.34 units) which was not significantly different from zero (t(62) = 0.39, p = 0.39). There was a higher level of bias (values exceeding the Limits of Agreement) that occurred between 5 and 11 units as represented by 5 (7.9%) participants. Conbach's alpha showed the OPPA scale to have acceptable internal consistency (α = 0.78).
FIGURE 3.
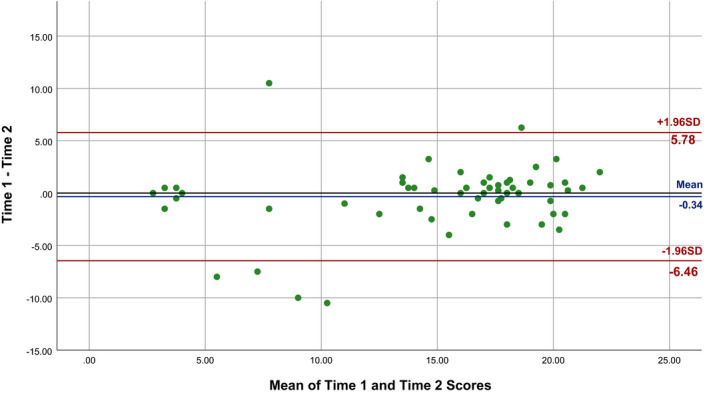
Bland‐Altman plot illustrating the level of agreement between baseline and 1‐week OPPA scores
4. DISCUSSION
This study is the first to develop a multifaceted self‐report measure (i.e. the OPPA) to capture not only the frequency of overactivity behaviour but also four other severity features for a more thorough assessment of overactivity severity in the context of chronic pain. A psychometric evaluation, informed by the COSMIN checklist (Mokkink et al., 2019; Mokkink et al., 2010), was undertaken examining the structural validity, construct validity, internal consistency, measurement error and test–retest reliability of the newly developed measure. Overall, a PCA confirmed that the five OPPA items were best represented by a single construct (labelled overactivity severity) providing support for the measure's structural validity. For construct validity, the OPPA was associated with pain‐related activity patterns and outcomes in the predictable ways that are supported by both theory and qualitative data. In addition, the OPPA exhibited acceptable internal consistency, good test–retest reliability and low levels of measurement error. These findings provide preliminary psychometric evidence supporting the use of the OPPA in clinical and research settings.
The OPPA total score and OPPA Frequency item were significantly associated with existing overactivity measures (i.e. the PARQ confronting scale and the POAM‐P overdoing scale). However, these associations were weaker than expected. There are a number of important differences between the OPPA and existing overactivity measures that may explain the weak associations observed. Both the PARQ and POAM‐P measure the frequency in which individuals with chronic pain engage in certain behaviours. While some items are reflective of overactivity behaviour (e.g. “I keep doing what I’m doing until my pain is so bad that I have to stop”) others may be more indicative of task persistence. Task persistence refers to persisting with activity in spite of pain and is generally considered to be a different construct (Andrews et al., 2012; Kindermans et al., 2011b; Luthi et al., 2018). Kindermans and colleagues (2011b) conducted a factor analysis on multiple questionnaires including the PARQ and POAM‐P to identify underlying dimensions of persistence. They found that the majority of items from the PARQ and POAM‐P loaded on a factor that was more aligned with persisting with activities for the purpose of finishing tasks (i.e. tasks persistence) as opposed to engaging in activities to the point of a severe pain aggravation (i.e. overactivity). The method for measuring frequency also differs between questionnaires; the OPPA uses unambiguous responses (e.g. “A couple of times a week”) as opposed to the more obscure markers used by the PARQ and POAM‐P which are more open to interpretation (e.g. “Always”). Thus, both the PARQ and POAM‐P may measure a general tendency towards persisting with activities in spite of pain as opposed to the severity of overactivity behaviour.
As hypothesized, we found that the OPPA was not associated with activity pacing but was associated, to a small extent, with higher levels of activity avoidance. Similar to existing overactivity measures, activity pacing self‐report measures tend to use a frequency scale to quantify pacing behaviour (Nielson et al., 2014). While these measures provide some indication of how often an individual with pain uses certain pacing strategies, they may provide little insight into the effective use of pacing strategies from a clinical perspective (Andrews & Deen, 2016; Murphy & Clauw, 2010; Nielson et al., 2014). Individuals with chronic pain who have been identified as being habitually overactive have described either infrequent use of activity pacing strategies or using pacing strategies regularly but ineffectively (Andrews et al., 2015b). This may explain the insignificant association between the overactivity severity and activity pacing measures found in the current investigation. On the other hand, the small positive association between the overactivity severity and activity avoidance is supported by qualitative findings (Andrews et al., 2015b) and theorists who have long alluded to an association between overactivity and increased levels of activity avoidance overtime based on clinical insight (Birkholtz et al., 2004; Philips, 1988). Individuals with pain have described how severe pain aggravations can contribute to increased pain catastrophizing and the avoidance of non‐essential activities in qualitative investigation (Andrews et al., 2015b). While the results of this study are supported by theory, they are in contrast with previous investigations that revealed either no association between activity avoidance and overactivity (Kindermans et al., 2011a; McCracken & Samuel, 2007) or significant negative associations (Cane et al., 2013; Kindermans et al., 2011b; Luthi et al., 2018). The inconsistencies observed may be due to the PARQ and POAM‐P scales being more reflective of a general tendency towards persisting with activities in spite of pain which is theoretically the opposite of activity avoidance (Leeuw et al., 2007; Vlaeyen & Linton, 2000).
In this study, significant moderate correlations between the OPPA and certain pain‐related outcomes (including higher pain severity, more pain interference, and higher levels of depression and stress) were found. In addition, small significant associations were found between the OPPA and reduced activity participation. These findings are in line with the viewpoint of Fordyce (1976) who was the first to suggest that overactivity behaviour could significantly worsen pain conditions. Other theorists have also described how the behaviour could intensify pain and the impact of pain on an individual's life (Birkholtz et al., 2004; Philips, 1988). These notions were further strengthened by qualitative data with vivid descriptions of the impact of overactivity behaviour on mood, sleep and social activity engagement from the perspective of those people with chronic pain (Andrews et al., 2015b). Quantitative data have also provided support for these associations through cross‐sectional and observational study designs (Andrews et al., 2014, 2016a, 2018; Cane et al., 2013; Esteve et al., 2016).
The results of our hierarchical regression analyses also demonstrated that the OPPA was the only overactivity measure to significantly improve the prediction of pain severity, pain interference and activity participation. The correlations between the OPPA items and existing overactivity scales revealed how the OPPA might be distinct from these measures and why the OPPA may be more strongly associated with long‐term pain outcomes. Neither the confronting scale of the PARQ nor the overdoing scale of the POAM‐P were not associated with the OPPA items Impact of Occupational Performance and Recovery Time. This suggests that the period of reduced functional capacity, which is inherent to definition of overactivity, may not be adequately measured or quantified by both the PARQ and POAM‐P. The findings of the current study indicate that a more comprehensive assessment of overactivity features may be useful to understand the impact of overactivity on overall perceptions of pain severity, physical functioning and pain interference.
Conversely, all the overactivity measures (including the OPPA) improved the prediction of psychological functioning after they were added in the regression models. There are a number of possible explanations for this finding. First, it is possible that the relationship between overactivity and psychological functioning is bidirectional and frequency of overactivity behaviour may be the most important aspect to consider when assessing this relationship. This theory is in line with Keefe and Lefebvre's (Keefe & Lefebvre, 1999) comprehensive model of pain behaviour, based on system theory, which purports that pain behaviours can influence and be influenced by an array of psychological factors. Individuals who have been identified as being habitually overactive have identified a number of psychological factors that they perceive contribute to their behaviour, such as psychological inflexibility and a reluctance to rely on others for support (Andrews et al., 2015b), which have been linked to poorer psychological health (Callaghan & Morrissey, 1993; Kashdan & Rottenberg, 2010). Second, the association between psychological functioning and overactivity may be explained partially owing to response bias. Individuals with chronic pain who have been identified as depressed or self‐report high levels of distress are more likely to endorse socially undesirable statements on self‐report questionnaires (Deshields et al., 1995; Haythornthwaite et al., 1991; Logan et al., 2008). In the current study, the overdoing scale of the POAM‐P was the strongest predictor of psychological functioning out of all the overactivity measures. This scale tends to use more emotive and socially undesirable language. For example, ‘my pain is so bad’ and ‘I can't stand the pain anymore’ are phrases found in POAM‐P items in contrast with ‘increased pain’ used in the OPPA. Individuals experiencing higher levels of distress may be more likely to rate items with emotive language higher. Further research is needed to elucidate the relationship between overactivity and psychological variables.
The current investigation provides initial support for the reliability of the OPPA. The OPPA reached an acceptable level of internal consistency. A good degree of reliability (Koo & Li, 2016) was also found between baseline and 1‐week OPPA total scores in the cohort of new clinic patients. At the item level, a moderate to good degree of reliability was found between baseline and 1‐week OPPA scores for all items except Severity of Pain Exacerbation which was poor to moderate (Koo & Li, 2016). One interpretation is that this item is scored differently to other items; those who deny overactivity behaviour are scored according to their average pain intensity over the past week which may have resulted in more test–retest variability. Thus, changes observed for the Severity of Pain Exacerbation score overtime, without corresponding changes to other items of the OPPA, should be interpreted with caution.
A Bland and Altman plot revealed a high level of agreement with baseline and 1‐week total OPPA scores. However, there was a higher level of measurement error that occurred between 5 and 11 units as represented by merely five participants. On closer inspection of the data, these outliers occurred secondary to participants changing their response to the second question (i.e. a shift between denying overactivity behaviour and reporting low levels of the behaviour). It is possible that participants changed their response after becoming more aware of their behaviour from either filling in the questionnaire or attending their initial appointment with medical staff as opposed to a shift in their overactivity behaviour. Therefore, the clinical significance of changes to this question in the OPPA should be interpreted with caution.
Finally, a ceiling effect was found for the OPPA Frequency item where 53% of participants chose the highest possible response. This may indicate that there is not enough variability in the responses for this item. Granted, the distribution for this item may change when other chronic pain samples are studied. For example, individuals who are managing their pain independently in the community may report engaging in overactivity behaviour at lower frequencies reducing the ceiling effect that was observed. As such, possible ceiling and floor effects for the OPPA items require further investigation.
The results of this study should be interpreted with several caveats in mind. The OPPA was validated and developed with the input from clinicians and individuals with chronic pain who were sourced from merely one tertiary multidisciplinary pain centre. This pain centre has been the recruitment source for the majority of research undertaken on overactivity in the context of chronic pain. Thus, the external validity of findings could be limited. In additional, the hypothesis testing was conducted on a subgroup of patients receiving active treatment. Results may differ if other chronic pain cohorts were used. The excessive persistence scale from the APS was not included as an overactivity outcome measure as the APS was published after the current study was conceptualized (Esteve et al., 2016). In addition, due to the cross‐sectional nature of this study, it is not possible to draw conclusions regarding causal relationships between overactivity and the key outcomes in chronic pain based on the findings presented. Finally, more than half of participants who did not return the OPPA at the second assessment point were excluded from the test–retest reliability analysis. These non‐responders were more likely to be younger individuals who lived with children and were employed full‐time. Researchers should consider strategies that may encourage and facilitate research participation for this cohort such as online questionnaires and participant incentives.
Despite these limitations, the current study provides preliminary evidence for the psychometric properties of the OPPA. It is recommended that the OPPA may be used as a tool to provide insight into the severity of overactivity behaviour in clinical and research settings. To make the OPPA clinically useful to evaluate the effectiveness of interventions targeting overactivity behaviour, further psychometric evaluation (e.g., responsiveness) of the OPPA is warranted.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
AUTHORS' CONTRIBUTIONS
N.E.A contributed substantially to the design, acquisition of the data, analysis, interpretation of the data, drafting the main manuscript text and preparing the tables and figures. C.W.C, D.I., and M.V. contributed substantially to the design, interpretation of the data and revised the text critically. All authors gave final approval of the version to be published.
ACKNOWLEDGEMENTS
The authors thank the administration staff of the Tess Cramond Pain and Research Centre for their valuable contribution to data collection including Luke Concannon, Sylvia Green, Timothy Brett and Thomas Whelan.
Andrews NE, Chien C‐W, Ireland D, Varnfield M. Overactivity assessment in chronic pain: The development and psychometric evaluation of a multifaceted self‐report assessment. Eur. J. Pain. 2021;25:225–242. 10.1002/ejp.1664
Funding information
N.E. Andrews was supported by a Patricia Dukes Fellowship administered by the Royal Brisbane and Women's Hospital Foundation.
REFERENCES
- Andrews, N. , & Deen, M. (2016). Defining activity pcing: Is it time to jump off the merry‐go‐round? Journal of Pain, 17, 1359–1362. [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , & Meredith, P. J. (2012). Activity pacing, avoidance, endurance, and associations with patient functioning in chronic pain: A systematic review and meta‐analysis. Archives of Physical Medicine and Rehabilitation, 93, 2109–2121. e2107. 10.1016/j.apmr.2012.05.029 [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , & Meredith, P. J. (2015a). Overactivity in chronic pain: Is it a valid construct? Pain, 156, 1991–2000. 10.1097/j.pain.0000000000000259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , & Meredith, P. J. (2016a). The relationship between approach to activity engagement, specific aspects of physical function, and pain duration in chronic pain. Clinical Journal of Pain, 32, 20–31. 10.1097/AJP.0000000000000226 [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , Meredith, P. J. , & Branjerdporn, G. S. (2018). Approach to activity engagement and differences in activity participation in chronic pain: A five‐day observational study. Australian Occupational Therapy Journal, 65, 575–585. 10.1111/1440-1630.12516 [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , Meredith, P. J. , & D'Arrigo, R. G. (2014). Association between physical activity and sleep in adults with chronic pain: A momentary, within‐person perspective. Physical Therapy, 94, 499–510. 10.2522/ptj.20130302 [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , Meredith, P. J. , & Fleming, J. A. (2016b). The relationship between overactivity and opioid use in chronic pain: A 5‐day observational study. Pain, 157, 466–474. 10.1097/j.pain.0000000000000384 [DOI] [PubMed] [Google Scholar]
- Andrews, N. E. , Strong, J. , Meredith, P. J. , Gordon, K. , & Bagraith, K. S. (2015b). "It's very hard to change yourself": An exploration of overactivity in people with chronic pain using interpretative phenomenological analysis. Pain, 156, 1215–1231. [DOI] [PubMed] [Google Scholar]
- Bergkvist, L. , & Rossiter, J. R. (2007). The predictive validity of multiple‐item versus single‐item measures of the same constructs. Journal of Marketing Research, 44, 175–184. 10.1509/jmkr.44.2.175 [DOI] [Google Scholar]
- Birkholtz, M. , Aylwin, L. , & Harman, R. M. (2004). Activity pacing in chronic pain management: One aim, but which method? Part one: Introduction and literature review. British Journal of Occupational Therapy, 67, 447–452. 10.1177/030802260406701005 [DOI] [Google Scholar]
- Booth, J. , Moseley, G. L. , Schiltenwolf, M. , Cashin, A. , Davies, M. , & Hübscher, M. (2017). Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskeletal Care, 15, 413–421. 10.1002/msc.1191 [DOI] [PubMed] [Google Scholar]
- Callaghan, P. , & Morrissey, J. (1993). Social support and health: A review. Journal of Advanced Nursing, 18, 203–210. 10.1046/j.1365-2648.1993.18020203.x [DOI] [PubMed] [Google Scholar]
- Cane, D. , Nielson, W. R. , McCarthy, M. , & Mazmanian, D. (2013). Pain‐related activity patterns: Measurement, interrelationships, and associations with psychosocial functioning. Clinical Journal of Pain, 29, 435–442. 10.1097/AJP.0b013e31825e452f [DOI] [PubMed] [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences, L. Erlbaum Associates. [Google Scholar]
- Darnall, B. D. , Ziadni, M. S. , Roy, A. , Kao, M. C. , Sturgeon, J. A. , Cook, K. F. , & Mackey, S. C. (2018). Comparative efficacy and mchanisms of a single‐session pain psychology class in chronic low back pain: Study protocol for a randomized controlled trial. Trials, 19, 165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deshields, T. L. , Tait, R. C. , Gfeller, J. D. , & Chibnall, J. T. (1995). Relationship between social desirability and self‐report in chronic pain patients. Clinical Journal of Pain, 11, 189–193. 10.1097/00002508-199509000-00005 [DOI] [PubMed] [Google Scholar]
- Dworkin, R. H. , Turk, D. C. , Farrar, J. T. , Haythornthwaite, J. A. , Jensen, M. P. , Katz, N. P. , Kerns, R. D. , Stucki, G. , Allen, R. R. , Bellamy, N. , Carr, D. B. , Chandler, J. , Cowan, P. , Dionne, R. , Galer, B. S. , Hertz, S. , Jadad, A. R. , Kramer, L. D. , Manning, D. C. , … Witter, J. (2005). Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain, 113, 9–19. 10.1016/j.pain.2004.09.012 [DOI] [PubMed] [Google Scholar]
- Esteve, R. , Ramírez‐Maestre, C. , Peters, M. L. , Serrano‐Ibáñez, E. R. , Ruíz‐Párraga, G. T. , & López‐Martínez, A. E. (2016). Development and initial validation of the activity patterns scale in patients with chronic pain. Journal of Pain, 17, 451–461. 10.1016/j.jpain.2015.12.009 [DOI] [PubMed] [Google Scholar]
- Fairbank, J. C. , & Pynsent, P. B. (2000). The oswestry disability index. Spine, 25, 2940–2952. 10.1097/00007632-200011150-00017 [DOI] [PubMed] [Google Scholar]
- Fordyce, W. (1976). Behavioral methods for chronic pain and Illness. The C.V. Mosby Company. [Google Scholar]
- Gibson, L. , & Strong, J. (2003). A conceptual framework of functional capacity evaluation for occupational therapy in work rehabilitation. Australian Occupational Therapy Journal, 50, 64–71. 10.1046/j.1440-1630.2003.00323.x [DOI] [Google Scholar]
- Hanson, R. W. , & Gerber, K. E. (1990). Coping with chronic pain: A guide to patient self‐management. Guilford Press. [Google Scholar]
- Hasenbring, M. I. , Andrews, N. E. , & Ebenbichler, G. (2020). Overactivity in chronic pain, the role of pain‐related endurance and neuromuscular activity: An interdisciplinary, narrative review. Clinical Journal of Pain, 36, 162–171. 10.1097/AJP.0000000000000785 [DOI] [PubMed] [Google Scholar]
- Haythornthwaite, J. A. , Sieber, W. J. , & Kerns, R. D. (1991). Depression and the chronic pain experience. Pain, 46, 177–184. 10.1016/0304-3959(91)90073-7 [DOI] [PubMed] [Google Scholar]
- Herdman, M. , Gudex, C. , Lloyd, A. , Janssen, M. F. , Kind, P. , Parkin, D. , Bonsel, G. , & Badia, X. (2011). Development and preliminary testing of the new five‐level version of EQ‐5D (EQ‐5D‐5L). Quality of Life Research, 20, 1727–1736. 10.1007/s11136-011-9903-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashdan, T. B. , & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30, 865–878. 10.1016/j.cpr.2010.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keefe, F. J. , & Lefebvre, J. (1999). Behavioral therapy In Melzack R. & Wall P. (Eds.), Textbook of pain (pp. 1445–1461). Churchill Livingstone. [Google Scholar]
- Kerns, R. D. , Turk, D. C. , & Rudy, T. E. (1985). The west haven‐yale multidimensional pain inventory (WHYMPI). Pain, 23, 345–356. 10.1016/0304-3959(85)90004-1 [DOI] [PubMed] [Google Scholar]
- Kindermans, H. P. , Huijnen, I. P. , Goossens, M. E. , Roelofs, J. , Verbunt, J. A. , & Vlaeyen, J. W. (2011a). "Being" in pain: The role of self‐discrepancies in the emotional experience and activity patterns of patients with chronic low back pain. Pain, 152, 403–409. 10.1016/j.pain.2010.11.009 [DOI] [PubMed] [Google Scholar]
- Kindermans, H. P. , Roelofs, J. , Goossens, M. E. , Huijnen, I. P. , Verbunt, J. A. , & Vlaeyen, J. W. (2011b). Activity patterns in chronic pain: Underlying dimensions and associations with disability and depressed mood. Journal of Pain, 12, 1049–1058. 10.1016/j.jpain.2011.04.009 [DOI] [PubMed] [Google Scholar]
- Koo, T. K. , & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15, 155–163. 10.1016/j.jcm.2016.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, J. , Lee, E.‐H. , & Moon, S. H. (2019). Systematic review of the measurement properties of the Depression Anxiety Stress Scales‐21 by applying updated COSMIN methodology. Quality of Life Research, 28, 2325–2339. 10.1007/s11136-019-02177-x [DOI] [PubMed] [Google Scholar]
- Leeuw, M. , Goossens, M. E. , Linton, S. J. , Crombez, G. , Boersma, K. , & Vlaeyen, J. W. (2007). The fear‐avoidance model of musculoskeletal pain: Current state of scientific evidence. Journal of Behavioral Medicine, 30, 77–94. 10.1007/s10865-006-9085-0 [DOI] [PubMed] [Google Scholar]
- Logan, D. E. , Claar, R. L. , & Scharff, L. (2008). Social desirability response bias and self‐report of psychological distress in pediatric chronic pain patients. Pain, 136, 366–372. 10.1016/j.pain.2007.07.015 [DOI] [PubMed] [Google Scholar]
- Lovibond, S. H. , & Lovibond, P. F. (1995). Manual for the depression anxiety stress scales. (2nd ed.). Psychology Foundation. [Google Scholar]
- Luthi, F. , Vuistiner, P. , Favre, C. , Hilfiker, R. , & Léger, B. (2018). Avoidance, pacing, or persistence in multidisciplinary functional rehabilitation for chronic musculoskeletal pain: An observational study with cross‐sectional and longitudinal analyses. PLoS One, 13, e0203329–e0203329. 10.1371/journal.pone.0203329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCracken, L. M. , & Samuel, V. M. (2007). The role of avoidance, pacing, and other activity patterns in chronic pain. Pain, 130, 119–125. 10.1016/j.pain.2006.11.016 [DOI] [PubMed] [Google Scholar]
- Mokkink, L. B. , Prinsen, C. A. C. , Patrick, D. L. , Alonso, J. , Bouter, L. M. , De Vet, H. C. W. , & Terwee C. B. (2019). COSMIN Study Design checklist for Patient‐reported outcome measurement instructments. Retrieved from: https://www.cosmin.nl/wp‐content/uploads/COSMIN‐study‐designing‐checklist_final.pdf.
- Mokkink, L. B. , Terwee, C. B. , Patrick, D. L. , Alonso, J. , Stratford, P. W. , Knol, D. L. , Bouter, L. M. , & de Vet, H. C. W. (2010). The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Quality of Life Research, 19, 539–549. 10.1007/s11136-010-9606-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy, S. L. , & Clauw, D. J. (2010). Activity pacing: What are we measuring and how does that relate to intervention? Pain, 149, 582–583. 10.1016/j.pain.2010.03.031 [DOI] [PubMed] [Google Scholar]
- Nielson, W. R. , Jensen, M. P. , Karsdorp, P. A. , & Vlaeyen, J. W. S. (2014). A content analysis of activity pacing in chronic pain: What are we measuring and why? Clinical Journal of Pain, 30, 639–645. 10.1097/AJP.0000000000000024 [DOI] [PubMed] [Google Scholar]
- Peipert, A. , Engel, E. , & Ehrlich‐Jones, L. (2018). Measurement characteristics and clinical utility of the West Haven‐Yale Multidimensional Pain Inventory in a chronic pain population. Archives of Physical Medicine and Rehabilitation, 99, 417–418. 10.1016/j.apmr.2017.08.481 [DOI] [Google Scholar]
- Philips, C. (1988). The psychological management of chronic pain. Springer. [Google Scholar]
- Solutions, S. (2020). Correlation (Pearson, Kendall, Spearman). Retreived from: https://www.statisticssolutions.com/correlation‐pearson‐kendall‐spearman/.
- Stevens, J. P. (1992). Applied multivariate statistics for the social sciences. (2nd ed.). Erlbaum. [Google Scholar]
- Vlaeyen, J. W. , de Jong, J. , Geilen, M. , Heuts, P. H. , & van Breukelen, G. (2002). The treatment of fear of movement/(re)injury in chronic low back pain: Further evidence on the effectiveness of exposure in vivo. Clinical Journal of Pain, 18, 251–261. 10.1097/00002508-200207000-00006 [DOI] [PubMed] [Google Scholar]
- Vlaeyen, J. W. , & Linton, S. J. (2000). Fear‐avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain, 85, 317–332. 10.1016/S0304-3959(99)00242-0 [DOI] [PubMed] [Google Scholar]
- Ye, X. , Sutherland, J. , Henry, B. , Tyndall, M. , & Kendall, P. R. W. (2018). At‐a‐glance ‐ Impact of drug overdose‐related deaths on life expectancy at birth in British Columbia. Health Promotion Chronic Disease Prevention in Canada: Research Policy and Practice, 38, 248–251. [DOI] [PMC free article] [PubMed] [Google Scholar]