

Abstract
Objective
We aim to explore the differential presence of symptoms of anxiety, depression, and acute stress between men and women during the COVID‐19 outbreak, and to study the relationship between these symptoms and two environmental variables, coexistence, and violence.
Methods
We conducted a cross‐sectional study starting on March 29 to April 5, 2020, based on a national online survey using snowball sampling techniques. Symptoms of anxiety (Hamilton Anxiety Scale), depression (Beck Depression Inventory), and acute stress (Acute Stress Disorder Inventory) were assessed. Differences in the presence of symptoms and the relationship of coexistence and domestic violence were evaluated from a gender perspective.
Results
Men showed significant lower mean (SD) in anxiety, depression, and acute stress levels than women [HARS, 14.1 (9.8) versus. 18.4 (10.2), F = 56.2, p < .001; BDI 3.4 (3.9) versus 4.5 (4.3), F = 16.6, p < .001, and ASDI 3.6 (2.9) versus 4.7 (3.1), F = 39.0, p < .001, respectively), as well as a weaker depressive syndrome (28.1% males versus 39.9% females, χ2 = 25.5, p < .001). In addition, an interaction Gender × Coexistence was found in anxiety (F = 56.2, p < .001) and acute stress (F = 3.52, p = .06) and, according to depressive symptoms, an interaction Gender × Violence was found marginally significant (F = 3.3, p = .07).
Conclusions
Findings indicate that women present greater severity in symptoms of anxiety, depression, and acute stress. Moreover, loneliness and violence specifically worsen the emotional state in women. These results can undoubtedly guide better healthcare planning adopting a gender perspective.
Keywords: acute stress, anxiety, COVID‐19, depression, gender differences
Our results indicate that women present greater severity in symptoms of anxiety, depression, and acute stress Moreover, loneliness and violence specifically worsen the emotional state in women.
1. INTRODUCTION
The COVID‐19 outbreak appeared in December 2019 in China and rapidly spread worldwide, becoming an unprecedented traumatic event. This forced the World Health Organization to declare COVID‐19 outbreak a health emergency of international concern, and consequently, government entities in different countries, including Spain, took drastic measures to restrict the mobility of its inhabitants.
Previously declared epidemics had already proved their potential to generate psychological impact (Chan‐Yeung, 2004), but unfortunately none has had the magnitude of the current pandemic. The global situation of accumulating cases and deaths and the extensive media coverage added to the individual fear of contagion, alongside with the fear of forced social transformation in the future, are all elements that might contribute to the detriment in mental health (Aiello et al., 2020; Stella et al., 2020).
Although COVID‐19 has affected the same number of men and women, gender differences have been identified in terms of fatality rates ((CDC) C for DC and P, 2020) suffering men a worse prognosis and a higher risk of death (Spagnolo et al., 2020). On the other hand, COVID‐19 has also become a potent stressor with people experiencing fear and isolation over a long period of time, leading to an increased vulnerability to anxiety, depression, and acute stress that affect women more than men (Mauvais‐Jarvis et al., 2020). Proof of this is the higher prevalence and severity of symptoms of anxiety, depression, and acute stress observed in females during the initial phase of the pandemic (Liu et al.,).
According to the international psychiatric classifications, a traumatic event is defined as the exposure to death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence (APA, 2013). Hence, this pandemic could be considered a trauma. Research has pointed out that women are more likely than men to develop distress after being exposed to trauma (Tolin & Foa, 2006). However, this gender difference is not absolute, when examining specific very high‐risk events for the development of post‐traumatic stress disorder, the relative risk equalizes or even reverses (Kessler et al., 1995).
To the best of our knowledge, there are few published studies addressing the gendered impact of the COVID‐19 outbreak in a country like Spain, where mortality remains as one of the highest worldwide. With this purpose, we aimed to explore the differential presence of symptoms of anxiety, depression, and acute stress between men and women, and to study the relationship between these symptoms and two environmental variables, coexistence and violence.
2. METHODS
A total of 520 men and 1,115 women, aged from 18 to 84 (mean 40.4 ± 14.1 years), participated in this cross‐sectional study previously published by our group (García‐Fernández et al., 2020), based on a national online survey applying an exponential nondiscriminative snowball sampling. The questionnaire was published on the hospital website and distributed by social networks to different geographical regions with the aim of reaching a representative sample of the Spanish population.
Up to 2,710 participants completed the self‐reported questionnaire from March 29 to April 5, 2020, which covers the peak of the SARS‐CoV‐2 infection in Spain. Anyone with access to social networks who consented to participate and was over 18 completed the questionnaire. Of total respondents, healthcare workers and people with a current or past mental disorder were excluded for the present study as they have been considered especially vulnerable population groups for emotional reactions to COVID already predisposed to experience more stress and have been analyzed in a different study (PsyCOVID San Juan imas12).
Informed consent was provided, and confidentiality was assured. The study was approved by Hospital de San Juan's local ethics committee.
Sociodemographic information on age, gender, and occupation was required, as well as whether responders had lived alone or with other people and had experienced situations of violence, either emotional or physical abuse, during the pandemic period.
To assess symptoms of anxiety and depression, we included the Hamilton Anxiety Scale (HARS) (Hamilton, 1959; Lobo et al., 2002) and the Beck Depression Inventory (BDI) (Bech, 1988; Vazquez & Sanz, 1999), respectively. For reporting the presence of acute stress, we adapted ad hoc for this study the clinical criteria for the diagnosis of Acute Stress Disorder (Acute stress disorder inventory—ASDI) of the Diagnostic and Statistical Manual of Mental Disorders (DSM‐5) (APA, 2013). We developed a list of symptoms to be applied as self‐reported questionnaire with a dichotomous answer (yes/no). In addition, the score of total affirmative responses to each of the items was recorded.
Differences between males and females in clinical variables were tested using one‐way analysis of variance corrected for age and chi‐squared tests as appropriate. Then, the ANOVAs were repeated including the following sociodemographic variables: coexistence (living alone versus with other people), having experienced violence (yes versus no), economic losses (yes versus no), unemployment (yes versus no), COVID‐19 infection (confirmed/suspected/discarded), and having experienced the passing of a loved one (yes versus no). All these variables were asked referring to the pandemic period. The analyses presented have been corrected for age. Bonferroni corrections for multiple comparisons have been applied when appropriate. All statistical analyses were considered statistically significant when p < .05.
3. RESULTS
3.1. Relationship between gender and clinical variables
Regarding anxiety symptoms (F = 56.2, p < .001), males had significant lower HARS scores (M = 14.1, SD = 9.8) than females (M = 18.4, SD = 10.2). In addition, results showed that males had significant lower BDI scores than females (F = 16.6, p < .00; M = 3.4, SD = 3.9 and M = 4.5, SD = 4.3, respectively). In the same line, when a cutoff syndrome score of 4 (absent or minimal versus. mild/moderate/severe depression) is applied, a weaker depressive syndrome in males was observed (χ2 = 25.5, p < .00; 28.1% males versus. 39.9% females). Finally, in ASDI scores (F = 39.0, p < .001), males had significantly lower ASDI scores than females (M = 3.6, SD = 2.9 and M = 4.7, SD = 3.1, respectively).
3.2. Relationship between gender and environmental variables
A significant interaction Gender × Coexistence was found in anxiety (F = 56.2, p < .001). Specifically, while there were no differences in males living alone or living with other people, females living alone showed significantly higher scores than those who lived with other people. No other variables had a differential impact on anxiety depending on the gender of the respondent: violence (F = 0.27, p = .60), economic losses (F = 0.002, p=.97), unemployment (F = 0.42, p = .52), COVID‐19 infection (F = 0.54, p = .59), or death of a loved one (F = 0.20, p = .66).
According to depressive symptoms, the interaction Gender x Violence was marginally significant (F = 3.3, p = .07). There were no differences in BDI scores between males who had experienced violence and those who had not. However, females who had experienced domestic violence had significantly higher levels of depressive symptoms than those who had not. No other variables had a differential impact on depressive symptoms depending on the gender of the respondent: coexistence (F = 0.20, p = .66), economic losses (F = 0.10, p = .75), unemployment (F = 0.13, p = .71), COVID‐19 infection (F = 1.27, p = .28), or death of a loved one (F = 0.61, p = .44).
In the case of ASDI scores, the interaction Gender x Coexistence was marginally significant (F = 3.52, p = .06). The mean difference in ASDI scores between males and females who live alone (women measuring higher) is more than twice compared to the difference between those who do not live alone. No other variables showed an interaction effect with gender: violence (F = 0.96, p=.33), economic losses (F = 1.21, p=.27), unemployment (F = 0.16, p=.69), COVID‐19 infection (F = 1.70, p=.18), or death of a loved one (F = 0.22, p=.64). (Mean and SD of all these analyses are presented in Table 1).
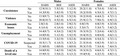
Table 1.
Mean and standard deviations of the psychological variables (HARS, BDI, and ASDI) as function of gender and the sociodemographic variables included in the analyses
| Males | Females | ||||||
|---|---|---|---|---|---|---|---|
| HARS | BDI | ASDI | HARS | BDI | ASDI | ||
| Coexistence | No | 12.9 (10.1) | 3.5(3.8) | 3.1(2.8) | 20.2(11.8) | 4.7(4.4) | 5.0(3.4) |
| Yes | 14.3 (9.8) | 3.4 (3.9) | 3.7 (2.9) | 18.2 (10.0) | 4.5 (4.3) | 4.7 (3.1) | |
| Violence | No | 13.9 (9.7) | 3.4 (3.9) | 3.5 (2.8) | 18.2 (10.0) | 4.4 (4.2) | 4.7 (3.1) |
| Yes | 20.0 (10.7) | 4.5 (2.8) | 6.5 (3.6) | 25.9 (12.7) | 7.9 (6.5) | 6.9 (3.2) | |
| Economic losses | No | 2.8 (3.4) | 2.8 (3.4) | 2.9 (2.5) | 4.0 (3.9) | 4.0 (3.9) | 4.3 (3.0) |
| Yes | 4.1 (4.4) | 4.1 (4.4) | 4.4 (3.1) | 5.3 (4.7) | 5.3 (4.7) | 5.4 (3.2) | |
| Unemployment | No | 14.4 (9.7) | 4.3 (4.2) | 3.8 (2.9) | 18.3 (10.2) | 5.2 (4.6) | 4.8 (3.2) |
| Yes | 14.0 (9.8) | 3.1 (3.8) | 3.5 (2.9) | 18.4 (10.2) | 4.0 (4.0) | 4.6 (3.1) | |
| COVID−19 | No | 13.5 (9.4) | 3.3 (3.9) | 3.5 (2.8) | 18.0 (10.0) | 4.5 (4.3) | 4.7 (3.1) |
| Suspected | 18.5 (11.7) | 4.1 (4.3) | 4.3 (3.2) | 21.5 (10.4) | 4.8 (3.9) | 5.3 (3.1) | |
| Yes | 21.0 (0.0) | 1.0 (0.0) | 1.0 (0.0) | 30.3 (15.0) | 7.3 (4.4) | 7.4 (4.5) | |
| Death of a loved one | No | 14.0 (9.8) | 3.4 (3.9) | 3.6 (2.8) | 18.3 (10.2) | 4.6 (4.3) | 4.7 (3.1) |
| Yes | 15.9 (9.3) | 3.5 (4.2) | 4.1 (3.2) | 19.4 (9.8) | 4.2 (3.5) | 4.8 (3.1) | |
4. DISCUSSION
The first aim of the present study was to explore the differential presence of symptoms between men and women during the peak of the COVID‐19 outbreak in Spain. Findings indicate, as has also been observed in Europe and China (Gebhard et al., 2020; Liu et al.,; Wang et al., 2020), that women present greater severity in symptoms of anxiety, depression, and acute stress, which denotes an increase in arousal response to stress in females (Bangasser & Wicks, 2017) supporting sex differences in stress response systems, also during COVID‐19. Hence, these results seem to point out that although the objective risk, due to morbidity and mortality ((CDC) C for DC and P, 2020) of the COVID‐19 pandemic, is significantly greater for men, the emotional response is higher in women, which evidences the existence of other factors, beyond verified data on severity, influencing the emotional response.
The study further demonstrates that women living alone show more severe levels of anxiety, a fact that has not been observed in men, supporting the existence of gender differences that remain in the response to COVID and that may have to do with the predominant role of women as family caregivers and the greater susceptibility to social isolation (Gebhard et al., 2020; Spagnolo et al., 2020). In the same line, having experienced situations of domestic violence during the period of the pandemic is associated, only in women, with greater depressive symptoms. These findings add valuable information and support the gender differences found in relation to the concerns during COVID‐19 of men and women, focused on the effects on the economy and society in men and on the family health and well‐being in women (Van der et al., 2020).
The main strength of the study includes data collection from a wide general population sample during a particularly difficult period of infection in Spain, but some limitations must be pointed out. First, response bias exist as a voluntary online self‐administered survey was applied, second, there is a difference in the number of men and women who have responded to the survey, and to end, an anxiety scale initially designed for the evaluation of people with mental disorders has been applied as well as a scale to measure acute stress based on the DSM 5 criteria still in the validation process.
To the best of our knowledge, this is the first time that symptoms of anxiety, depression, and acute stress after the outbreak of COVID‐19 are assessed in Spain in a great sample, incorporating both a broad representation of the general population and a gender perspective. The response to coronavirus appears to be different between men and women. Moreover, loneliness and violence specifically worsen the emotional state in women. These results emphasize the need to address the gender impact of outbreaks, as well as the benefit of paying special attention to women living alone and those who suffer domestic violence to ensure their emotional well‐being.
CONFLICT OF INTEREST
Dr. R. Rodriguez‐Jimenez has been a consultant for, spoken in activities of, or received grants from Instituto de Salud Carlos III, Fondo de Investigación Sanitaria (FIS), Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid Regional Government (S2010/ BMD‐2422 AGES; S2017/BMD‐3740), JanssenCilag, Lundbeck, Otsuka, Pfizer, Ferrer, Juste, Takeda, Exeltis, Angelini, and Casen‐Recordati. All other authors declare that they have no conflict of interest.
AUTHOR CONTRIBUTIONS
LGF and RRJ designed the study and wrote the protocol; LGF, PDLR, and MMG carried the study out; VRF and SPU undertook the statistical analysis; all authors contributed and have approved the final manuscript.
Peer Review
The peer review history for this article is available at https://publons.com/publon/10.1002/brb3.1934.
ACKNOWLEDGEMENTS
We thank all participants who have kindly responded to the survey.
García‐Fernández L, Romero‐Ferreiro V, Padilla S, David López‐Roldán P, Monzó‐García M, Rodriguez‐Jimenez R. Gender differences in emotional response to the COVID‐19 outbreak in Spain. Brain Behav.2021;11:e01934 10.1002/brb3.1934
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Aiello, L. M. , Quercia, D. , Zhou, K. , Constantinides, M. , Šćepanović, S. , & Joglekar, S. (2020). How Epidemic Psychology Works on Social Media: Evolution of responses to the. [Google Scholar]
- American Psychiatric Association (APA) (2013). Diagnostic and statistical manual of mental disorders (DSM‐5®). American Psychiatric Pub. [Google Scholar]
- Bangasser, D. A. , & Wicks, B. (2017). Sex‐specific mechanisms for responding to stress. Journal of Neuroscience Research 95(1–2), 75–82. 10.1002/jnr.23812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bech, P. Rating scales for mood disorders: Applicability, Consistency and construct validity. Acta Psychiatrica Scand. 1988;78(345 S):45–55. [DOI] [PubMed] [Google Scholar]
- CDC C for DC and P (2020). The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID‐19) in China. China CDC Weekly, 2(8), 113–122. [PMC free article] [PubMed] [Google Scholar]
- Chan‐Yeung, M. (2004). Severe acute respiratory syndrome (SARS) and healthcare workers. International Journal of Occupational and Environmental Health, 10, 421–427. [DOI] [PubMed] [Google Scholar]
- García‐Fernández, L. , Romero‐Ferreiro, V. , López‐Roldán, P. D. , Padilla, S. , Calero‐Sierra, I. , Monzó‐García, M. et al (2020). Mental health impact of COVID‐19 pandemic on Spanish healthcare workers. Psychol Med [internet]., May 27 [cited 2020 May 28];1–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32456735. http://www.ncbi.nlm.nih.gov/pubmed/32456735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gebhard, C. , Regitz‐Zagrosek, V. , Neuhauser, H. K. , Morgan, R. , & Klein, S. L. Impact of sex and gender on COVID‐19 outcomes in Europe. Biol Sex Differ 2020;11(1):29. doi:10.1186/s13293–020–00304–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton, M. (1959). The assessment of anxiety states by rating. British Journal of Medical Psychology, 32(1), 50–55. Available from https://onlinelibrary.wiley.com/doi/abs/10.1111/j.2044‐8341.1959.tb00467.x. [DOI] [PubMed] [Google Scholar]
- Kessler, R. C. , Sonnega, A. , Bromet, E. , Hughes, M. , & Nelson, C. B. (1995). Posttraumatic Stress Disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52(12), 1048–1060. [DOI] [PubMed] [Google Scholar]
- Liu, N. , Zhang, F. , Wei, C. , Jia, Y. , Shang, Z. , Sun, L. et al Prevalence and predictors of PTSS during COVID‐19 outbreak in China hardest‐hit areas: Gender differences matter. Elsevier [Internet]. [cited 2020 May 28]; Available from: https://www.sciencedirect.com/science/article/pii/S016517812030545. [DOI] [PMC free article] [PubMed]
- Lobo, A. , Chamorro, L. , Luque, A. , Dal‐Re, R. , Badia, X. , & Baró, E. (2002). Validation of the Spanish versions of the Montgomery‐Asberg Depression Rating Scale and the Hamilton Anxiety Rating Scale for the assessment of depression and anxiety. Medicina Clínica., 118, 493–499. 10.1016/S0025-7753(02)72429-9 [DOI] [PubMed] [Google Scholar]
- Mauvais‐Jarvis, F. , Bairey Merz, N. , Barnes, P. J. , Brinton, R. D. , Carrero, J. J. , DeMeo, D. L. et al (2020). Sex and gender: Modifiers of health, disease, and medicine. Lancet 396(10250):565–582. 10.1016/S0140-6736(20)31561-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spagnolo, P. A. , Manson, J. E. , & Joffe, H. (2020). Sex and Gender Differences in Health: What the COVID‐19 Pandemic Can Teach Us. Annals of Internal Medicine, 173(5), 385–386. 10.7326/M20-1941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stella, M. , Restocchi, V. , & De Deyne, S. (2020). #lockdown: Network‐Enhanced Emotional Profiling in the Time of COVID‐19. Big Data Cogn. Comput., 4(2), 14 10.3390/bdcc4020014 [DOI] [Google Scholar]
- Tolin, D. F. , & Foa, E. B. (2006). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132(6), 959–992. [DOI] [PubMed] [Google Scholar]
- Van der Vegt, I. , & Kleinberg, B. Women worry about family, men about the economy: Gender differences in emotional responses to COVID‐19. arXiv preprint arXiv:2004.08202, 2020.
- Vazquez, C. , & Sanz, J. (1999). Reliability and validity of the Spanish version of Beck’s Depression Inventory (1978) in patients with psychological disorders. Clínica Y Salud, 10(1), 59–81. [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , Ho, C. S. et al (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID‐19) epidemic among the general population in China. Int J Environ Res Public Health [internet]., [cited 2020 May 28];17(5):1729. Available from: www.mdpi.com/journal/ijerph. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.