

Abstract
Aberrant pauses are characteristic of schizophrenia and are robustly associated with its negative symptoms. Here, we found that pause behavior was associated with negative symptoms in individuals at clinical high risk (CHR) for psychosis, and with measures of syntactic complexity—phrase length and usage of determiners that introduce clauses—that we previously showed in this same CHR cohort to help comprise a classifier that predicted psychosis. These findings suggest a common impairment in discourse planning and verbal self-monitoring that affects both speech and language, and which is detected in clinical ratings of negative symptoms.
Subject terms: Psychosis, Biomarkers
Everyday conversations are governed by a set of rules that are often implicit—taking turns, staying on topic, and using the appropriate volume and tone are required for accurate perception and understanding. One important aspect of communication is pausing. Pauses in speech serve both physiological and cognitive functions. While pausing to breathe is a physiological necessity, cognitive pausing allows speakers not only to plan what they are going to say, but allows their interlocutor a chance to respond1. Pauses also hold significant social communicative meaning. The placement and length of a pause can substantially affect the interpretation of an interaction, as longer pauses are often accompanied by negative social attributions2.
Abnormalities in speech, including aberrant pausing behavior, are characteristic of schizophrenia and have been examined in the context of negative symptoms. Speech features such as reductions in prosody have been associated with negative symptoms, showing that the most robust speech correlate of negative symptoms in schizophrenia is pause length3. While the analysis of linguistic features of spoken language (e.g., semantics and syntax) require transcription and natural language processing algorithms, acoustic qualities of spoken language can easily be recorded and quantified using open-source software which avoids introducing errors through automated transcription. Automated speech analyses have only begun to be applied in clinical high risk (CHR) individuals, with one prior study finding an association between abnormal turn-taking and positive symptom severity4. As negative symptoms are prevalent in CHR individuals, we tested the hypothesis that they may be associated with increased time spent pausing, as in schizophrenia. We also tested whether increased time spent pausing was associated with features of syntactic complexity—maximum phrase length and usage of determiner pronouns (that introduce dependent clauses), which themselves were associated with negative symptoms in this same cohort5. These syntactic features were identified using automated part-of-speech (POS) tagging6 and were input into a machine learning classifier that both predicted psychosis onset previously within this same cohort, and which were associated with negative symptoms in canonical correlation5.
CHR individuals had mean total negative symptom ratings of 13.4 (SD 7.8) and mean pause length of 1.0 (SD 0.4) seconds, with mean 48% (SD 16%) of pauses in narrative. Total negative symptom severity was significantly associated with both mean pause length (r = 0.64, p < 0.005) and percentage of pauses (r = 0.60, p < 0.005) (Fig. 1), which were themselves intercorrelated (r = 0.94, p < 0.005). The cohort was stratified by negative symptom severity into subgroups (“low”: 0–1 items >= 3, “medium”: 2–3 items >= 3; “high”: 4–6 items >= 3). These subgroups significantly differed in both mean pause length (F(2,30) = 6.81, p = 0.004) and pause percentage (F(2,30) = 6.34, p = 0.005), with the “high” subgroup” having significantly longer average pauses (mean 1.32 s (SD 0.44 s) than both the “low” (mean 0.90 s, (SD 0.23 s)) and “medium” (mean 0.84 s, (SD 0.27 s)) negative symptom subgroups. Additionally, the “high” negative symptoms subgroup had a significantly higher pause percentage (mean 59% (SD 15%) than the “low” (mean 40% (SD 15%) and “medium” (mean 42% (SD 10%) negative symptoms subgroups. The linguistic variable of maximum phrase length was negatively associated with both mean pause length (r = −0.57, p = 0.001) and percentage of pauses (r = −0.56, p = 0.001), and determiner pronoun usage was negatively associated with average pause length (r = −0.37, p = 0.03) but not percentage of pauses (p > 0.13). Of note, both maximum phrase length (r = −0.47, p = 0.006) and determiner pronoun use (r = −0.39, p = 0.03) were significantly negatively correlated with total negative symptoms. In this cohort, there were no associations of age or sex with negative symptoms, mean pause length or percentage of pauses (all p’s > 0.30). No group differences were found for pause variables by medication prescription or by total words spoken by the interviewer (all p’s > 0.12).
Fig. 1. Associations of negative symptom severity and pause behavior.
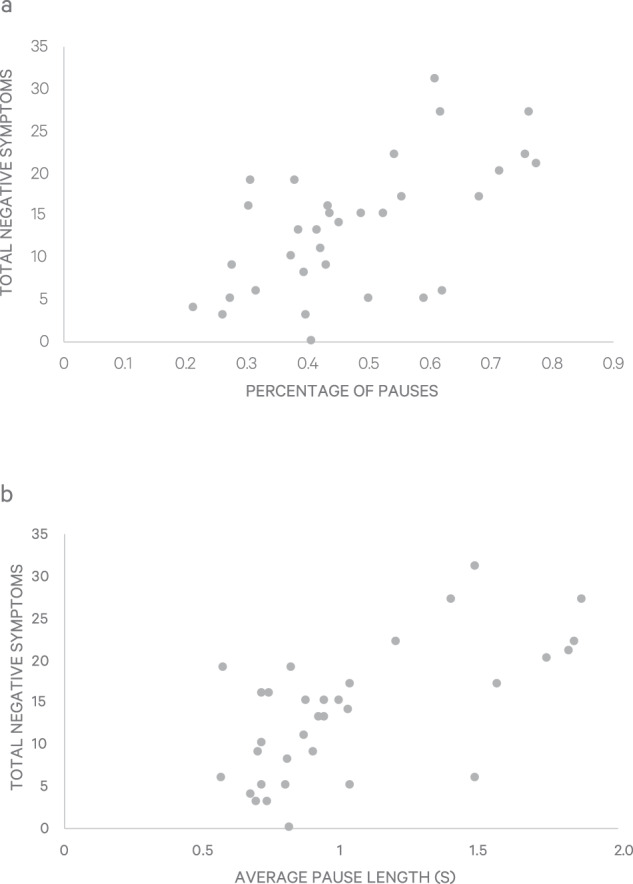
Panel 1a shows the association of negative symptom severity with mean pause length in seconds. Panel 1b shows the association of negative symptoms severity with percentage of pauses.
Overall, using open-source automated acoustic analysis, longer pause lengths and percentage of time spent in silences (e.g., long pauses) were found to be associated with both negative symptoms and shorter maximum phrase length in individuals at clinical risk for psychosis. These results are consistent with the prior study by Cohen et al.3, which identified pause length as the sole speech feature (among seven acoustic variables) that was consistently associated with negative symptom severity in schizophrenia across five studies with disparate methods for soliciting speech, including interviews, as in the current study, but also in social cognition tasks and monologues.
The association between negative symptoms and increased time spent pausing across stages of psychosis might be based in cognitive and linguistic mechanisms. A recent study by Cokal et al.7 identified that aberrant pauses in schizophrenia lie at the boundaries of large syntactic units as opposed to within clauses, indicating that word-finding (reflected by within-clause pausing) is not the problem, but instead a difficulty in the organization of thought in speech, which occurs at clausal boundaries. Therefore, it may be that longer pauses reflect impairment in discourse planning and verbal self-monitoring, similar to what has been found for measures of thought disorder8. This premise is supported by neuroimaging studies that show attenuation of activity during pauses in regions of the brain involved in the planning and monitoring of speech, specifically left superior temporal gyrus and insula9. Further, these pauses may be interpreted clinically as reflecting alogia and diminished emotional expression, as manipulation of pre-recorded patient speech to artificially inflate pause length, holding all other acoustic variables constant, leads to higher ratings of negative symptoms in patients with schizophrenia10.
There are a few limitations in this pilot study, namely modest sample size and lack of a comparison group. Future directions will include the study of pauses and other acoustic variables, as well as additional measures of syntactic complexity, in a large prospective psychosis risk cohort study with healthy and patient comparison participants fully characterized in respect to symptoms and cognition, with potential contributions of medications, motivational impairments, and social behavior considered. Finally, mechanistic studies of these putative biomarkers of negative symptoms can identify targets for engagement in preventive intervention strategies.
Methods
Participants and clinical characterization
Participants met criteria for the “Clinical High Risk” (CHR) syndrome of attenuated positive symptoms, as assessed with the Structured Interview for Psychosis-Risk Syndromes/Scale of Psychosis-Risk Symptoms11. Participants were 33 CHR individuals with mean(SD) age = 21(4) years, who were 1/3 female and ethnically diverse (36% Caucasian). 24% of participants were prescribed medications (9% antipsychotics, 21% antidepressants). Adult participants provided written informed consent; participants under 18 provided written assent, with written consent provided by a parent. This study was approved by the Institutional Review Boards at first the New York State Psychiatric Institute at Columbia University, and then at the Icahn School of Medicine at Mount Sinai. Negative and other symptoms were assessed by PhD raters using the Structured Interview for Psychosis-Risk Syndromes/Scale of Psychosis-Risk Syndromes (SIPS/SOPS)11, separate from narrative interviews.
Speech elicitation
Speech was elicited through open-ended narrative interviews12, in which participants were instructed to discuss their lives broadly; interviews were conducted using qualitative methods13 meant to maximize the amount of narrative speech by the person interviewed with interviewers interjecting only to encourage the participant to speak further. Interviewers were trained in qualitative interviewing by an expert in phenomenological research methods8. Over approximately one hour, participants were encouraged to describe their experience, its impact on them, and their expectations for the future.
Speech preprocessing and pause analysis
Interviewer speech was manually spliced and removed from transcripts to ensure pauses were only those that could be attributed to the participant. Pause analysis was conducted using PRAAT (www.fon.hum.uva.nl/praat). Based on the criterion set forth by Goldman-Eisler14, pauses were defined as any silence longer than 250 ms, as pauses shorter than 250 ms are considered to signify breathing and articulation, while pauses longer than 250 ms are assumed to reflect higher level cognitive processes. Mean pause length was calculated, as well as the percentage of time during the encounter spent in silences greater than 250 ms, defined as the percentage of pauses. These variable types (mean and percentage) were considered to be relatively insensitive to length of audio recordings, which were shorter among individuals with highest negative symptoms (see below); (F(2,30) = 3.80, p = 0.03).
Natural language processing analysis: preprocessing and part-of-speech tagging
Interviews were transcribed by an independent company. Transcripts were preprocessed using the Natural Language Toolkit (NLTK; http://www.nltk.org/). After discarding punctuation, each interview was automatically parsed into phrases. Words were then converted to the roots from which they are inflected, or lemmatized, using the NLTK WordNet lemmatizer. The resultant preprocessed data consisted of a list of lemmatized words, parsed into phrases, maintaining the original order, without punctuation and in lower case. Maximum phrase length and usage of determiner pronouns (which introduce clauses) were determined previously using part-of-speech (POS) tagging, as described in our prior study of linguistic predictors of psychosis onset and linguistic correlates of prodromal symptoms5.
Data analyses
Spearman correlation analyses were done for pause variables with demographics, negative symptoms and two linguistic features of syntactic complexity (maximum phrase length and use of determiner pronouns). Also, following Cohen et al.3, participants were stratified by negative symptom severity, here using the SIPS/SOPS, with an enumeration of negative symptoms rated as 3 or higher: low as 0–1 items >= 3, N = 9; medium as 2–3 items >= 3; N = 12, and high as 4–6 items >= 3, N = 12. ANOVA analyses were used to identify differences in pause variables between these subgroups. Alpha was set at 0.05 for hypothesized associations of pause variables with negative symptom severity, and with linguistic variables of syntactic complexity, maximum phrase length, and use of determiner pronouns. No adjustment was made for covariates in this small sample. All tests were two-sided.
Reporting summary
Further information on experimental design is available in the Nature Research Reporting Summary linked to this article.
Supplementary information
Acknowledgements
This research was supported by NIMH (R01MH107558; PI = Corcoran; R01MH115332).
Author contributions
Cansu Sarac and Zarina Bilgrami aggregated all data including pre-existing demographic, diagnostic, clinical and linguistic data, as well as the speech/acoustic data that Emma Stanislawski extracted from audiofiles and then analyzed. Emma Stanislawski wrote the first and subsequent drafts of the paper, with supervision from Cheryl Corcoran and input from all authors, including Sahil Garg and Guillermo Cecchi. Carla Agurto and Stephen Heisig computed the acoustic analysis variables and assisted with data analysis. Cheryl Corcoran is the principal investigator for the R01 that supports these data collection and analyses. All authors made substantial contributions to the manuscript, making critical revisions, conferring final approval, and assuming accountability.
Data availability
The data that support the findings of this study are available from the corresponding author upon request.
Code availability
All analyses were conducted in Praat and Python. The code is available from the corresponding author upon request.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information The online version of this article (10.1038/s41537-020-00132-1) contains supplementary material, which is available to authorised users.
References
- 1.Lundholm Fors, K. Production and Perception of Pauses in Speech (University of Gothenburg, 2015).
- 2.Roberts, F. & Francis, A. L. Identifying a temporal threshold of tolerance for silent gaps after requests. J. Acoust. Soc. Am. 10.1121/1.4802900 (2013). [DOI] [PubMed]
- 3.Cohen, A. S., Mitchell, K. R., Docherty, N. M. & Horan, W. P. Vocal expression in schizophrenia: Less than meets the ear. J. Abnorm. Psychol. 10.1037/abn0000136 (2016). [DOI] [PMC free article] [PubMed]
- 4.Sichlinger, L., Cibelli, E., Goldrick, M. & Mittal, V. A. Clinical correlates of aberrant conversational turn-taking in youth at clinical high-risk for psychosis. Schizophr. Res.10.1016/j.schres.2018.08.009 (2019). [DOI] [PMC free article] [PubMed]
- 5.Bedi G, et al. Automated analysis of free speech predicts psychosis onset in high-risk youths. NPJ Schizophr. 2015;1:115030. doi: 10.1038/npjschiz.2015.30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Santorini, B. Part-of-Speech Tagging Guidelines for the Penn Treebank Project (3rd Revision). Univ. Pennsylvania 3rd Revis. 2nd Print. 10.1017/CBO9781107415324.004 (1990).
- 7.Çokal, D. et al. Disturbing the rhythm of thought: speech pausing patterns in schizophrenia, with and without formal thought disorder. PLoS ONE.10.1371/journal.pone.0217404 (2019). [DOI] [PMC free article] [PubMed]
- 8.Barch, D. M. & Berenbaum, H. The effect of language production manipulations on negative thought disorder and discourse coherence disturbances in schizophrenia. Psychiatry Res. 10.1016/s0165-1781(97)00045-0 (1997). [DOI] [PubMed]
- 9.Matsumoto, K. et al. Frequency and neural correlates of pauses in patients with formal thought disorder. Front. Psychiatry.10.3389/fpsyt.2013.00127 (2013). [DOI] [PMC free article] [PubMed]
- 10.Alpert, M., Pouget, E. R. & Silva, R. Cues to the assessment of affects and moods: speech fluency and pausing. Psychopharmacol. Bulletin31, 412–141 (1995). [PubMed]
- 11.Miller, T. J. et al. Symptom assessment in schizophrenic prodromal states. Psychiatr. Q. 70, (1999). [DOI] [PubMed]
- 12.Ben-David S, et al. The subjective experience of youths at clinically high risk of psychosis: a qualitative study. Psychiatr. Serv. 2014;65:1499–1501. doi: 10.1176/appi.ps.201300527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davidson, L. Phenomenological research in schizophrenia: from philosophical anthropology to empirical science. J. Phenomenol. Psychol. 10.1163/156916294X00133 (1994).
- 14.Boomer, D. S. Psycholinguistics; Experiments in Spontaneous Speech (Frieda Goldman Eisler Academic Press, London & New York, 1968).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.
All analyses were conducted in Praat and Python. The code is available from the corresponding author upon request.