

Abstract
SARS-CoV-2 has spread rapidly worldwide, but the full impact of the COVID-19 pandemic on the field of hematopoietic cell transplantation (HCT) remains unknown. To understand this better, an 18-item online survey was disseminated by the Worldwide Network for Blood & Marrow Transplantation with questions exploring SARS-CoV-2 testing algorithms, mobilization, and cryopreservation strategies and COVID-19 infections in allogeneic related and autologous hematopoietic progenitor cell (HPC) donors. The aim of this survey was to assess the impact of the outbreak on policies relating to HPC mobilization, collection, and processing with respect to changes in daily routine. A total of 91 individual responses from distinct centers in 6 continents were available for analysis. In these centers, the majority (72%) of allogeneic related and autologous donors are routinely tested for SARS-CoV-2 before HPC collection, and 80% of centers implement cryopreservation of allogeneic HPC grafts before commencing conditioning regimens in patients. Five related and 14 autologous donors who tested positive for COVID-19 did not experience any unexpected adverse events or reactions during growth factor administration (eg, hyperinflammatory syndrome). These data are limited by the small number of survey respondents but nonetheless suggest that centers are following the recommendations of appropriate scientific organizations and provide some preliminary data to suggest areas of further study.
Key Words: COVID-19, G-CSF, Cryopreservation, Mobilization
INTRODUCTION
In late 2019, a novel coronavirus, later named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in China and then spread worldwide, causing the disease called coronavirus disease 2019 (COVID-19). On March 11, 2020, the World Health Organization (WHO) classified COVID-19 as a pandemic. Subsequently, many countries imposed major restrictions on travel and everyday life and were in a state of “lockdown.” At the time of this writing (October 30, 2020), more than 46 million global cases, 1,195,418 global deaths, and 565,797 new daily cases have been reported by the WHO and Johns Hopkins University [1,2]. COVID-19 continues to have a significant impact on all aspects of hematopoietic cell transplantation (HCT) in many parts of the world and will likely impact the future use of cellular therapies, including chimeric antigen receptor T (CAR T) cell therapy.
Early in the outbreak, scientific and not-for profit organizations, including the European Society for Blood and Marrow Transplantation (EBMT) [3], the American Society for Transplantation and Cellular Therapies (ASCT), the Center for International Blood and Marrow Transplant Research (CIBMTR) [4], and the World Marrow Donor Association (WMDA) [5], developed recommendations for HCT centers and hematopoietic progenitor cell (HPC) collection and processing facilities. These recommendations are updated regularly and include preventive measures for staff and outpatient visits [6,7]. In addition, the Worldwide Network for Blood & Marrow Transplantation (WBMT), a nonprofit organization in a official relationship with the WHO, has recommended deferring nonurgent HCT in areas with endemic or high‐frequency COVID‐19 infection [8]. More recently, a consensus decision was reached between the WBMT and CIBMTR's Health Services and International Studies (HSIS) committee and other HCT experts representing multiple continents [9]. Later, concerns about the use of granulocyte colony-stimulating factor (G-CSF) products in SARS-CoV-2-infected individuals and the potential for induction of adverse events, such as hyperinflammatory reactions, were raised.
To better understand the impact of the pandemic on transplantation centers, a survey was disseminated by the WBMT with questions exploring SARS-CoV-2 testing algorithms, mobilization and cryopreservation strategies, and COVID-19 infections in allogeneic related and autologous hematopoietic progenitor cell (HPC) donors. As accumulating evidence suggests that a subgroup of patients with severe COVID-19 may experience a cytokine storm syndrome, we were also interested to explore whether G-CSF administration as part of HPC mobilization would be able to cause a hyperinflammatory state, including secondary hemophagocytic lymphohistiocytosis, in cases of COVID-19 positivity.
METHODS
A link to a survey using the SurveyGizmo tool (SurveyGizmo, Boulder, CO) was disseminated by the WBMT to member societies the Australasian Bone Marrow Transplant Recipient Registry (ABMTRR), African Blood and Marrow Transplantation Society, Asia Pacific Blood and Marrow Transplantation Group (APBMT), ASTCT, CIBMTR, EBMT, Eastern Mediterranean Blood and Marrow Transplantation Group (EMBMT), and Latin America Blood and Marrow Transplantation Group (LABMT), who were asked to invite their members to participate. The decision to circulate the survey and how this was done was specific to each member organization. A reminder was requested to be sent out around 1 week after dissemination. The survey was available online for 3 weeks. Not all the organizations were able to disseminate the invitation to members in the timeframe of the study. In view of the nature of the participating organizations, some have overlapping membership. Only one completed survey per center (the most complete) was accepted after review by the WBMT office.
Survey
The 18-item survey (“SARS-CoV-2 in related donors and patients after G-CSF mobilization”) was developed by the standing Committee on Donor Issues of the WBMT and the WBMT Board and transferred to SurveyGizmo (Supplementary Table S1). The authors piloted the survey, assessed the design, and checked the feasibility and validity of the questions. The finalized online survey was made available online from May 18 to June 8, 2020.
We sought agreement to publish the compiled data and for descriptive data of the respective centers (ie, country, city, center name, society for outcome data reporting, center number, and contact person). The following points were addressed in patients with allogeneic related donors: SARS-CoV-2 testing policy, test results, severe events and adverse reaction to G-CSF administration, clinical outcome in those tested positive, and policies for collection and processing of allogeneic products. Patients undergoing autologous mobilization were assessed for SARS-CoV-2 testing and test results in those undergoing HPC mobilization, severe events and adverse reaction to G-CSF administration and clinical outcome in those testing positive, and possible changes in mobilization strategies during the COVID-19 pandemic in the autologous setting (Supplementary Table S1).
To explore whether G-CSF administration and concurrent COVID-19 infection resulted in a hyperinflammatory syndrome, we asked specific questions were asked about elevated levels of C-reactive protein (CRP), lactate dehydrogenase (LDH), D-dimer, and ferritin. We also collected data on the need for intensive care, mechanical ventilation, and dialysis.
RESULTS
A total of 153 individual responses was received. We accepted only one response per center and deleted duplicates and blank responses. After data cleaning, 91 responses remained for further analysis. The responding countries and number of centers are listed in Supplementary Table S2. Answers reflect the policies and possibilities (in terms of resources) of centers in different parts of the world at the time of the survey.
The majority of responding centers routinely report their HCT outcome data to the CIBMTR (n = 50; 55%) and EBMT (n = 26; 29%). In addition, 5% of centers (n = 4) report to the EMBMT, 3% (n = 3) report to the LABMT, 1% (n = 1) report to the APBMT, and 8% (n = 7) report to other organizations not specified.
Allogeneic Donors
SARS-CoV-2 Testing in Related Donors
The majority of responding centers (73%; 66 of 91) reported always testing related donors since the pandemic, whereas 17% (16 of 91) tested only on request of the transplantation/apheresis center, and 9 (10%) did not have the ability to test at all. Centers not having the ability to test at the time of the survey (late May to June 2020) were located in Brazil (n = 3), Thailand (n = 1), and the United States (n = 5). Testing on request was possible in centers located in Algeria (n = 1), Australia (n = 2), Brazil (n = 1), Canada (n = 2), China (n = 1), India (n = 2), Israel (n = 1), Saudi Arabia (n = 1), and the United States (n = 5).
Regarding the time point of SARS-CoV-2 testing, the following options were given in the survey, and participants could choose one or more applicable options: at medical checkup, at the start of mobilization (ie, 1 to 3 days before or at the day of the first G-CSF application), on the day of collection, and only in the event of symptoms. Twenty-four percent (16 of 66) reported testing allogeneic donors at medical checkup. However, 9 of these centers repeat the test when starting the mobilization regimen. Therefore, the majority (86%) of responding centers tested related donors at the start of mobilization. Seven centers (11%) also tested on the day of collection. Five percent of centers reported testing only in the event of symptoms or in donors at risk of SARS-CoV-2 infection. (Figure 1 A).
Figure 1.
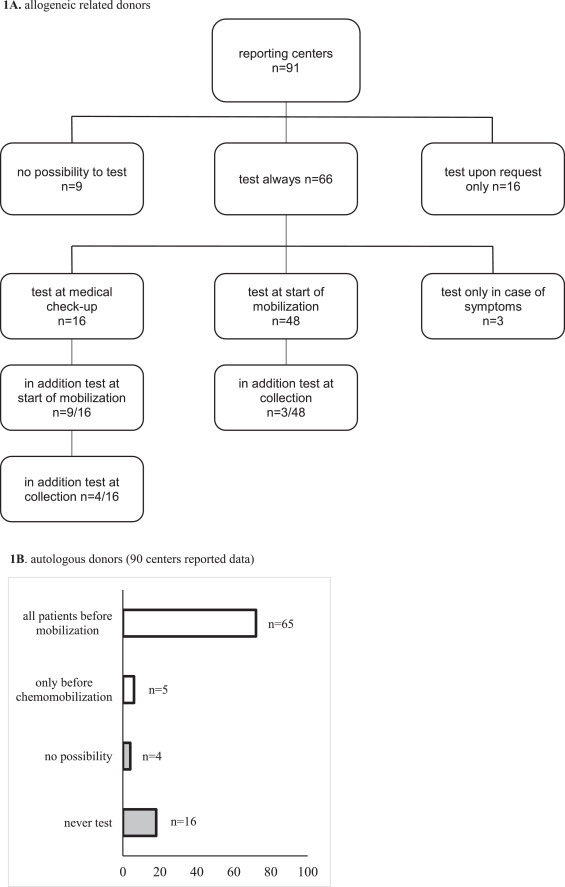
The algorithm for SARS-CoV-2 testing in allogeneic related (n = 91) (A) and autologous (n = 90) (B) HPC donors. 1A. allogeneic donors (91 centers reported data).
Related Donors Testing Positive for SARS-CoV-2 and Clinical Course
Sixty-six of the 91 responding centers answered this question. Four of 66 centers reported a total of 5 donors testing positive at medical checkup (n = 1), start of mobilization (n = 2), collection (n = 1), or at follow-up (n = 1 on day 18 after donation). The donors were reported from 2 different centers in Brazil (1 donor each), 1 center in Italy (2 donors), and 1 center in the United States (1 donor). No detailed information on the deferral period of the donors who tested positive at medical checkup was given. All but 1 center reported cryopreserving related and unrelated allogeneic HPCs, whereas the Italian center reported freezing only unrelated HPCs. For this reason, this center had to use the HPCs even though the donor had tested positive.
To understand the product release strategy of HPC grafts from COVID-19 positive tested donors, we contacted the reporting centers, but were not successful in gaining more information. In the 3 positive donors who received G-CSF concurrently during their COVID-19 infection, no adverse events after G-CSF mobilization or hyperinflammatory symptoms were noted. In 2 cases where CRP, LDH, and D-dimer levels were tested, values were within the normal ranges, but these tests were not done in the remaining 3 donors. Ferritin level was available in only 1 donor who tested positive on day 18 after HPC donation and was elevated. The clinical course was uneventful in 4 donors, whereas only 1 donor who experienced the infection on day 18 after HPC donation presented with fever for 3 days. None of these donors required hospital admission.
Further information on the outcome of 3 patients who received products from donors tested positive at medical checkup (n = 1), at the start of mobilization (n = 1), and during follow-up (n = 1 on day 18 after donation) was provided by the respective centers. In none of the 3 patients was transmission of SARS-CoV-2 detected. Data from the remaining 2 patients have not been reported.
Changes to Centers’ Policies for Handling Allogeneic HPC Grafts During the SARS-CoV-2 Pandemic
The majority of centers (75%; 68 of 91) changed their policies with regard to allogeneic HCT. Fifteen of these centers (22%) reported proceeding to HCT only for patients with high-risk disease while delaying HCT for those without urgent transplant indications, in accordance with recommendations of the EBMT and ASTCT. In addition, participating centers reported using peripheral blood stem cells more often than bone marrow during that time and in 5 of 68 centers (7%), a switch to haploidentical family donors instead of unrelated donors was considered.
Fifty percent of centers began cryopreserving allogeneic HPC products (peripheral blood stem cells and bone marrow) from related and unrelated donors before starting a conditioning regimen. Twenty-six percent cryopreserve products only from unrelated donors, whereas 4% do so only from related donors. Eighteen centers (20%) reported not freezing allogeneic products.
In 43% of centers, a negative SARS-CoV-2 test in the donor is required for further release of the stem cell product. Forty-three percent of centers wait for a negative medical history of the donor 1 to 2 weeks after donation, whereas 24% do not have any new requirements.
Autologous Donors
Ninety centers responded to survey items for autologous donors.
Centers Changing Their Mobilization Policy for Autologous HPC Grafts During the SARS-CoV-2 Pandemic
The majority of centers (73%; 66 of 90) changed their mobilization policy for autologous HPCs, whereas 7 centers (2 in Australia and 1 each in Brazil, India, Kuwait, Pakistan, and Thailand) reported stopping autologous HPC collection at the time the survey was conducted. The responses from 82 of the 90 centers (91%) were available for more detailed analysis: 19% answered that they used chemotherapy-based mobilization for all patients and 33% did so only for patients with standard protocols for their underlying disease (eg, diffuse large cell lymphoma, Hodgkin lymphoma), whereas the majority (48%) used steady-state G-CSF mobilization for all patients.
SARS-CoV-2 Testing in Patients Undergoing Autologous HPC Mobilization
At the time of the survey, the majority of centers (72%) tested all patients before HPC mobilization, whereas 6% tested only before chemotherapy-based mobilization, 18% never tested, and 4% reported being unable to test. The latter centers were in Brazil (n = 3) and Canada (n = 1) (Figure 1).
Patients Undergoing HPC Mobilization Who Tested Positive for SARS-CoV-2 and Clinical Course
Nine of the 90 centers (10%; Austria, n = 1; Brazil, n = 4; Kuwait, n = 1; Turkey, n = 1; United States, n = 2) reported a total of 14 patients testing positive for SARS-CoV-2 during the mobilization/collection period. Nine patients were reported from the 4 Brazilian centers, and the other centers each had only 1 patient detected with a COVID-19 infection.
In no case infection with SARS-CoV-19 was associated with additional adverse events to G-CSF mobilization and none of the patients presented with a hyperinflammatory state. Detailed laboratory parameters were made available for 12 patients. In the majority, elevated levels of CRP (n = 16), ferritin (n = 7), and D-dimer (n = 6) were observed. One patient was admitted to an intensive care unit, but mechanical ventilation or dialysis was not required.
Data on the duration of symptoms and admission were available for 9 patients. In 6 of these patients, the infection was clinically asymptomatic despite abnormal laboratory parameters. Three patients had clinical symptoms over 7 to 8 days leading to hospital admission for 10 days in 2 of them. Data on the duration of infection and need for hospitalization were not reported in 5 patients.
The clinical outcome was available for 13 patients. One patient died due to COVID-19 infection, while 12 recovered without complications.
Seven of the 9 centers reported not using HPC products collected from SARS-CoV-2- positive patients. One center reported testing the product before using it for HPC transplantation, whereas another center reported using the product.
DISCUSSION
This is the first survey not only to address changes in the daily practice of autologous and allogeneic HPC collection and processing units, and transplant centers during the pandemic and lock-down of the respective countries but also to analyze whether SARS-CoV-2 infections may have an influence on the tolerability of G-CSF administration for HPC mobilization either as single-agent therapy or in combination with chemotherapy.
Key Results
The majority of centers changed their policy and began to order products especially from unrelated donors in advance. This was not only due to the local COVID-19 situation, but also to the situation in the respective region of the collection centers, as travel restrictions made it impossible to foresee whether a product will arrive in time. Interestingly, countries not freezing allogeneic products at the time of the survey (ie, Algeria, Brazil, China, Jordan, Lebanon, Mexico, Oman, Pakistan, Paraguay, Saudi Arabia, and Hawaii) were mostly in the early stages of a marked increase of COVID-19 cases (Brazil, Mexico, Oman, Pakistan, and Saudi Arabia) or had only a very low daily infection rate (eg, Algeria, <100/day; Jordan and Hawaii, <20/day; Paraguay, <30/day; Lebanon, <50/day).
In accordance with published recommendations of scientific societies (eg, ASTCT, EBMT) for recipients and donors of HPCs [3,4,7], some centers reported scheduling patients with more urgent transplantation indications while postponing non-urgent transplantations.
Few COVID-19 cases have been reported in allogeneic related HPC donors. In these donors, no increase in severe events and adverse reactions due to growth factor mobilization was observed. Available data in 3 recipients of HPC grafts from SARS-CoV-2-positive donors demonstrated no viral transmission. Similar to other human coronaviruses (including SARS‐CoV and MERS‐CoV), transfusion transmission of SARS‐CoV‐2 has not yet been reported, suggesting that transfusion transmission of coronaviruses is rare if it occurs at all. However, it is acknowledged that SARS‐CoV‐2 has been identified only recently, and thus the possibility of virus transmission by transfusion cannot be excluded 10, 11, 12, 13.
More infections were observed in autologous cases, unfortunately also with 1 fatal outcome, but no increased severe events and adverse reactions due to G-CSF or hyperinflammation were reported in this group. Recent studies have identified cancer patients as a vulnerable population with a high risk of morbidity due to COVID-19 14, 15, 16, 17; however, published case fatality rates vary widely (62% vs 13%), depending also on patient age and comorbidities 14, 15, 16, 17, 18.
Limitations
This survey has several limitations. One limitation is that it mirrors strategies of responding centers only for the survey period from May to June 2020. However, we were able to include 91 responses and reach centers in 6 continents (Africa, Asia, Australia, Europe, North America, and South America). Moreover, the number of centers responding to our survey varied among countries. Therefore, our data reflect only components of the situation in different countries and cannot be generalized for whole countries or whole continents. The invitation and link to the survey was disseminated by WBMT to all the member societies, although the invitation was not disseminated by all member societies to their members, and thus European countries and centers are underrepresented in this survey.
The survey was sent out shortly after the peak of COVID-19 infections in Europe and Turkey, but at that time infections were dramatically increasing in North and South America, the Near East, and Africa. Contemporary infection rates in Canada had declined already and were in between 2 peaks in Australia, Europe and the Middle East (Figure 2 ). This implies that continents and the regional responses may have been affected by the pandemic to varying degrees. Depending on the location of centers and the COVID-19 situation in the respective region, recommendations of associated scientific organizations were followed [4,6, 7, 8, 9].
Figure 2.
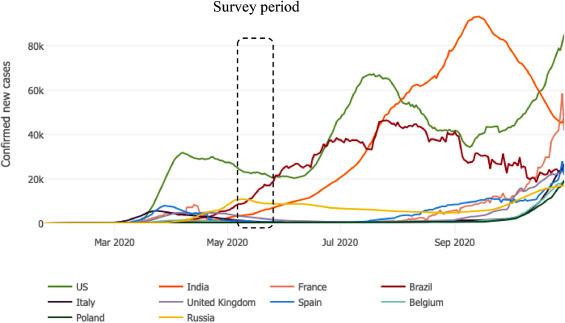
Outbreak evolution for the 10 most affected countries in the world (as of October 30, 2020), according to the Johns Hopkins University Coronavirus Resource Center. The dashed bar indicates the survey period (May 18 to June 8, 2020).
To prevent exposure to COVID-19 in patients and donors, especially in regions where testing is not possible, it is recommended that maximum emphasis be placed on personal protection by avoiding unnecessary travel to high‐risk areas and exercising good hygiene for donors and patients. Even though this virus has not been shown to be transmitted by transfusion of blood products, published recommendations for donor screening and detailed medical history (including travel history, exposure to COVID-19, etc) should be included in all centers’ procedures [4,6, 7, 8, 9].
ACKNOWLEDGMENTS
The authors thank Martine Schuit for translating the questionnaire into the SurveyGizmo tool and distributing the link. The authors are grateful to all centers who participated and thank all staff members at the various institutions for their support.
Financial disclosure: There are no financial dislosures to report in the context of the submitted manuscrip.
Conflict of interest statement: There are no conflicts of interest to report.
Authorship statement: N.W., B.S., M.A., M.K., A.S., D.W., J.S., S.G., Y.K., P.E., S.H., Y.A., J.S., W.S., D.N. and H.G. designed the survey and wrote the manuscript, and N.W. analyzed the data.
Footnotes
Financial disclosure: See Acknowledgments on page 270.e5.
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jtct.2020.11.019.
Appendix. Supplementary materials
REFERENCES
- 1.World Health Organization. Coronavirus disease (COVID-2019) situation reports. Available at: https://wwwwhoint/emergencies/diseases/novel-coronavirus-2019/situation-reports. Accessed November 6th, 2020
- 2.Johns Hopkins University & Medicine Coronavirus Resource Center. New cases of COVID-19 in world countries. Available at: https://coronavirus.jhu.edu/data/new-cases. Accessed November 8th, 2020.
- 3.European Society for Blood and Marrow Transplantation. Coronavirus disease COVID-19: EBMT recommendations. Available at: https://wwwebmtorg/ebmt/news/coronavirus-disease-covid-19-updated-ebmtrecommendations-8th-march-2020. Accessed March 8th, 2020.
- 4.American Society for Transplantation and Cellular Therapy. Interim guidelines for COVID-19 management in hematopoietic cell transplantation and cellular therapy patients. Available at: https://www.astct.org/communities/public-home?CommunityKey=d3949d84-3440-45f4-8142-90ea05adb0e5. Accessed March 9th, 2020. [DOI] [PMC free article] [PubMed]
- 5.World Marrow Donor Association. (WMDA) information on COVID-19. Available at: https://share.wmda.info/pages/viewpage.action?pageId=344866320. Accessed March 2020.
- 6.EBMT recommendation update version 9. Available at: https://www.ebmt.org/covid-19-and-bmt. Accessed November 18th, 2020.
- 7.Ljungman P, Mikulska M, de la Camara R. The challenge of COVID-19 and hematopoietic cell transplantation; EBMT recommendations for management of hematopoietic cell transplant recipients, their donors, and patients undergoing CAR T-cell therapy. Bone Marrow Transplant. 2020;55:2071–2076. doi: 10.1038/s41409-020-0919-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.WBMT press release: Coronavirus and Haematopoietic Stem Cell Transplantation. Available at: https://www.wbmt.org/wp-content/uploads/2020/03/WBMT_COVID-19-2.pdf. Accessed February 24th, 2020.
- 9.Algwaiz G, Aljurf M, Koh M. Real-world issues and potential solutions in hematopoietic cell transplantation during the COVID-19 pandemic: perspectives from the Worldwide Network for Blood and Marrow Transplantation and Center for International Blood and Marrow Transplant Research Health Services and International Studies Committee. Biol Blood Marrow Transplant. 2020;26:2181–2189. doi: 10.1016/j.bbmt.2020.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.World Health Organization. Maintaining a safe and adequate blood supply and the collection of COVID-19 convalescent plasma during the pandemic outbreak of coronavirus disease (COVID-19). Interim guidance. 10 July 2020. Available at: https://www.who.int/publications/i/item/maintaining-a-safe-and-adequate-blood-supply-during-the-pandemic-outbreak-of-coronavirus-disease-(covid-19). Accessed July 10th, 2020.
- 11.Katz LM. Is SARS-CoV-2 transfusion transmitted? Transfusion. 2020;60:1111–1114. doi: 10.1111/trf.15831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kiely P, Hoad VC, Seed CR, Gosbell IB. Severe acute respiratory syndrome coronavirus-2: implications for blood safety and sufficiency [e-pub ahead of print] Vox Sang. 2020 doi: 10.1111/vox.13009. Accessed Sep 23, 2020. Online ahead of print. PMID: 32965726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Leblanc JF, Germain M, Delage G, O'Brien S, Drews SJ, Lewin A. Risk of transmission of severe acute respiratory syndrome coronavirus-2 by transfusion: a literature review. Transfusion. 2020;60:3046–3054. doi: 10.1111/trf.16056. Epub 2020 Sep 1. PMID: 32798237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.He W, Chen L, Chen L. COVID-19 in persons with haematological cancers. Leukemia. 2020;34:1637–1645. doi: 10.1038/s41375-020-0836-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chari A, Samur MK, Martinez-Lopez J. Clinical features associated with COVID-19 outcome in MM: first results from International Myeloma Society Dataset. Blood. 2020 doi: 10.1182/blood.2020008150. Accessed November 6, 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lamure S, Duléry R, Di Blasi R. Determinants of outcome in Covid-19 hospitalized patients with lymphoma: a retrospective multicentric cohort study. EClinicalMedicine. 2020;27 doi: 10.1016/j.eclinm.2020.100549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Passamonti F, Cattaneo C, Arcaini L. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. 2020;7:e737–e745. doi: 10.1016/S2352-3026(20)30251-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hatzl S, Eisner F, Schilcher G. Response to "COVID-19 in persons with haematological cancers". Leukemia. 2020;34:2265–2270. doi: 10.1038/s41375-020-0914-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.