

Abstract
Venous congestion has emerged as an important cause of renal dysfunction in patients with cardiorenal syndrome. However, only limited progress has been made in differentiating this haemodynamic phenotype of renal dysfunction, because of a significant overlap with pre‐existing renal impairment due to long‐term hypertension, diabetes, and renovascular disease. We propose congestive nephropathy (CN) as this neglected clinical entity. CN is a potentially reversible subtype of renal dysfunction associated with declining renal venous outflow and progressively increasing renal interstitial pressure. Venous congestion may lead to a vicious cycle of hormonal activation, increased intra‐abdominal pressure, excessive renal tubular sodium reabsorption, and volume overload, leading to further right ventricular (RV) stress. Ultimately, renal replacement therapy may be required to relieve diuretic‐resistant congestion. Effective decongestion could preserve or improve renal function. Congestive acute kidney injury may not be associated with cellular damage, and complete renal function restoration may be a confirmatory diagnostic criterion. In contrast, a persistently low renal perfusion pressure might induce renal dysfunction and histopathological lesions with time. Thus, urinary markers may differ. CN is mostly seen in biventricular heart failure but may also occur secondary to pulmonary arterial hypertension and elevated intra‐abdominal pressure. An increase in central venous pressure to >6 mmHg is associated with a steep decrease in glomerular filtration rate. However, the central venous pressure range that can provide an optimal balance of RV and renal function remains to be determined. We propose criteria to identify cardiorenal syndrome subgroups likely to benefit from decongestive or pulmonary hypertension‐specific therapies and suggest areas for future research.
Keywords: Cardiorenal syndromes, Heart failure, Intra‐abdominal hypertension, Pulmonary hypertension, Venous congestion
Introduction
Renal dysfunction in heart failure (HF) has traditionally been considered to result from decreased renal perfusion and associated neural and hormonal changes. Recently, persistent venous congestion was identified as a major contributor. 1 , 2 High central venous pressure (CVP) initiates a vicious cycle of hormonal and endothelial activation, hepatic dysfunction, ascites, increased intra‐abdominal pressure (IAP), intestinal mucosal ischaemia (with translocation of bacterial toxins), inflammation, oxidative stress, excessive renal tubular sodium reabsorption, and volume overload, leading to further right ventricular (RV) stress. 3 , 4 Ultimately, renal replacement therapy may be required to relieve congestion. 5 This sequence of events appears to be crucial in the pathophysiology of RV failure in patients with pulmonary arterial hypertension 6 and, more commonly, those with biventricular HF. 7 , 8
Despite evidence that unresolved congestion leads to adverse renal and overall outcomes in HF 1 , 9 —whereas effective decongestion preserves or even improves renal function 10 , 11 and improves survival 12 —this haemodynamic phenotype of renal dysfunction is still not clearly defined. This is partly because patients with concomitant HF and chronic kidney disease (CKD) are commonly diagnosed with cardiorenal syndrome (CRS), a heterogeneous and controversial clinical entity encompassing a spectrum of disorders mediated by multiple haemodynamic and non‐haemodynamic factors. 13 Many patients with CRS have hypertension and/or diabetes, 14 so albuminuria and renal dysfunction 15 , 16 , 17 generally lead to diagnosis of hypertensive nephrosclerosis or diabetic nephropathy without a corroborating kidney biopsy. 18 , 19 In patients with CRS, undetected congestion caused by HF and pulmonary hypertension (PH) may converge with other pathophysiological mechanisms to aggravate renal dysfunction. Early identification of patient subgroups having cardiac plus renal dysfunction, and phenotyping of underlying kidney disease mechanisms, may enable tailoring of therapy.
We propose the term congestive nephropathy (CN) to describe the neglected clinical entity of renal dysfunction that is associated with venous congestion as well as decreased renal perfusion. 20 Similar to obstructive nephropathy, 21 CN appears to be reversible in early stages. Whether long‐term congestion will result in tubular atrophy and renal fibrosis remains unknown. This review aims to (i) summarize current understanding of CN and its impact on the development of CKD, (ii) suggest criteria to characterize patient subgroups likely to benefit from decongestion, and (iii) identify areas for future research.
Clinical scenarios associated with congestive nephropathy
HF is likely the most common condition associated with CN; others include PH of any origin, isolated tricuspid regurgitation, 22 and congenital heart disease. 23 , 24 CN should also be suspected in patients who show improved renal function after decongestion by diuretics, HF‐specific and PH‐specific therapy, or mechanical means (e.g. paracentesis of ascites).
Various factors associated with renal dysfunction are encountered frequently in patients with pulmonary arterial hypertension and HF (Figure 1 ).
Figure 1.
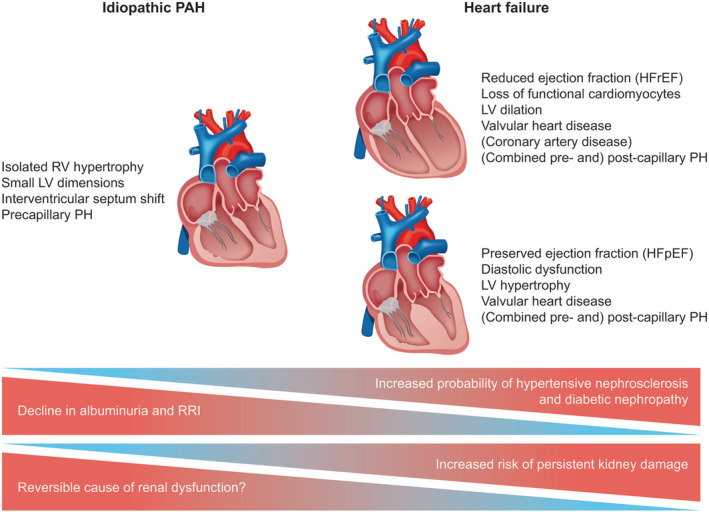
Congestive nephropathy in pulmonary arterial hypertension and heart failure. Various factors and co‐morbidities related to renal dysfunction appear frequently in patients with PAH and HF. HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LV, left ventricular; PAH, pulmonary arterial hypertension; PH, pulmonary hypertension; RRI, renal resistance index; RV, right ventricular.
Heart failure
One seminal study on acute decompensated HF found that high CVP on admission (or insufficient reduction after hospitalization) is a stronger predictor of renal dysfunction than cardiac index. 1 Another study by the same group, however, found no association between CVP and serum creatinine during treatment of HF. 25 Registry data show no association between ejection fraction in HF and renal dysfunction. 26 , 27 The ESCAPE trial revealed that improvement in cardiac index is not associated with renal outcomes, 28 and observational studies show that increased CVP is associated with decreased kidney function and increased mortality. 1 , 2 Importantly, RV diastolic pressure and pulmonary arterial diastolic pressure are comparably increased in HF patients with reduced or preserved ejection fraction. 29 In the presence of PH with RV dysfunction and relatively preserved cardiac index, CVP elevation is associated with a reduced glomerular filtration rate (GFR). 20 Overall, however, patients with congestion plus hypoperfusion have worse GFR and renal outcome and higher mortality than patients with isolated congestion or hypoperfusion. 20 , 26 , 27 , 30 , 31 , 32
Pulmonary hypertension due to left heart disease
PH is the most common precursor of RV failure, 33 being reported in 40–75% of patients with reduced ejection fraction and 36–83% of patients with preserved ejection fraction 34 ; the actual prevalence is probably higher because PH may manifest only upon stress (e.g. during exercise or fluid challenge) 35 Importantly, impaired renal venous flow (indicative of renal venous congestion) and reduced GFR have been described in HF without echocardiographic evidence of PH or RV dysfunction, suggesting that congestion may be present even without clinically detectable RV failure. 36
Chronic kidney disease and heart failure
The effect of severity and duration of venous congestion and volume overload on CKD remains largely unexplored. Studies have shown that a high HF hospitalization rate (reflecting persistent congestion) is associated with long‐term decline in GFR, 37 , 38 and that decongestive therapies improve overall outcome. 9 Furthermore, volume overload is reported to be associated with renal disease progression. 39 , 40 Whether the risk of CKD can be mitigated by relieving congestion (without precipitating low cardiac output) and achieving euvolaemia (using combination diuretic therapy to overcome diuretic resistance) needs to be determined, as also the CVP range that provides the optimum balance of RV and renal function in patients with HF.
Chronic kidney disease and pulmonary hypertension
CKD, per se, can cause cardiac dysfunction and failure. 13 PH often coexists with CKD; the prevalence increases with increasing CKD stage, suggesting an interdependent relationship. 3 , 36 , 41 , 42 , 43 In a recent study on patients with CKD undergoing right heart catheterization (n = 1873), 68% had PH, with post‐capillary PH being the predominant phenotype. Among those with post‐capillary PH, 64% had HF (33% with reduced ejection fraction and 31% with preserved ejection fraction), suggesting HF as the most prevalent cause of PH. 44 Interestingly, pre‐capillary PH was found in 16% of patients, 44 indicating that CKD itself may cause pulmonary vascular remodelling in predisposed patients. 45 CKD‐induced PH may result from volume overload, endothelial dysfunction, decreased bioavailability of nitric oxide, and increased endothelin‐1 levels. 3 In patients on dialysis, blood exposure to dialysis membrane and shunting via arteriovenous fistulae may also contribute. 3 Acute worsening of renal function in pulmonary arterial hypertension has been found to be strongly associated with RV failure and mortality. 46 , 47 , 48 , 49
Congenital heart disease, cardiac surgery, and isolated tricuspid regurgitation
In patients with Fontan circulation, renal function is inversely related to CVP 23 , 50 ; these patients have high baseline albuminuria and tubular damage biomarker levels, with the latter linked to adverse outcomes. 23 , 51 Interestingly, however, renal dysfunction tends to be delayed, 52 probably owing to renal compensatory mechanisms during adolescence. Meanwhile, in children undergoing surgery for congenital heart disease, CVP rather than cardiac output is associated with worsening of postoperative renal function. 24 Venous congestion and decreased renal perfusion pressure are also associated with increased risk of acute kidney injury in adults undergoing cardiac surgery 53 , 54 and heart transplantation 55 ; congestion in this setting may be a sign of underlying right HF.
Impaired renal function is a predictor of mortality in adults with isolated tricuspid regurgitation. 22 In retrospective studies, high preoperative serum creatinine was strongly associated with mortality in adult patients with tricuspid regurgitation receiving surgical and medical management. 56 , 57
Increased intra‐abdominal pressure
The splanchnic veins contain anywhere between 20% and 50% of the total blood volume. 58 As a result of sympathetic nerve overactivity in HF, vasoconstriction in this compartment forces movement of venous blood to the circulating compartment, which contributes to HF decompensation; this may be particularly important in acute HF. 58 , 59 , 60 As an additional component, high IAP compresses intra‐abdominal and intrathoracic blood vessels, compromising microvascular blood flow. 61 Diminished venous drainage results in renal, intestinal, and mesenteric venous congestion, oedema, and ischaemia. 62
In healthy volunteers, increased IAP by means of external abdominal compression results in increased renal venous pressure and CVP, and decreased renal blood flow, GFR, tubular function, and urine output. 63 CRS is commonly associated with increased IAP, especially when ascites is present. The impact of increased IAP on renal dysfunction in acute HF has been described in small studies. 64 , 65 , 66 In a seminal study involving patients with acute HF with reduced ejection fraction, an elevated IAP (≥8 mmHg) at admission was present in 60% of the study population (n = 40) and was associated with renal dysfunction. 65 Furthermore, a strong correlation (r = 0.77; P < 0.001) was observed between reduction in IAP at baseline and improvement in renal function, independent of haemodynamic changes. 65 Another study reported a similar association between increased IAP (≥12 mmHg) and renal dysfunction in patients with acute HF with mid‐range ejection fraction and preserved ejection fraction. 66 Furthermore, in that study, a persistent increase in IAP at 72 h was associated with a longer length of hospital stay and 1 year mortality. 66
Microcirculatory disturbance occurs when IAP reaches 10–15 mmHg. 61 In animal models, renal dysfunction commences at IAP of 10 mmHg, 67 , 68 and anuria occurs at IAP of 30 mmHg. 69 , 70 Such changes are not seen in animals with isolated elevation of intrarenal parenchymal pressure due to renal compression. 71 In models of abdominal compartment syndrome, reversal of reduced cardiac output by volume expansion does not improve renal function, suggesting that high renal venous pressure is principally responsible for renal dysfunction in the setting of increased IAP. 72
Congestive nephropathy
Pathophysiology
Table 1 provides an overview of key studies of the pathophysiology of renal venous congestion. Much of the evidence comes from animal experiments and cannot be entirely extrapolated to humans. Animal models show an association between increased renal venous pressure and reduced renal blood flow, 76 with congestion being a more important determinant of renal dysfunction than perfusion. 77
Table 1.
Studies examining renal function and glomerular haemodynamics related to venous congestion or elevation of intra‐abdominal and renal parenchymal pressure
| Study | Design | Cohort | Methods | Findings |
|---|---|---|---|---|
| Bradley et al., 1947 63 | Prospective interventional single centre | 17 healthy individuals; mean GFR 115 ± 19 mL/min | External abdominal compression at 80 mmHg (resulting in intra‐abdominal pressure approx. 20 mmHg), invasively measured renal venous pressure in 9 individuals | Abdominal compression is associated with renal venous pressure elevation and reduction of GFR and tubular activities (maximal glucose reabsorption and maximal diodrast excretion) |
| Damman et al., 2009 2 | Retrospective observational single centre | 2557 patients with broad spectrum of cardiovascular disease undergoing right heart catheterization; mean estimated GFR 65 ± 24 mL/min/1.73 m2 | Association of renal function with invasive haemodynamics; median 10.7 year follow‐up evaluating all‐cause mortality | Estimated GFR increases slightly as central venous pressure increases from 1 to 6 mmHg, whereas it falls sharply when central venous pressure rises above 6 mmHg; central venous pressure is an independent determinant of mortality |
| Iida et al., 2016 73 | Prospective observational single centre | 217 stable patients with HF (30% with preserved ejection fraction) and 38 healthy individuals; mean estimated GFR 64 ± 26 mL/min/1.73 m2 | Characterization of Doppler‐derived intrarenal venous flow patterns according to invasive haemodynamics, echocardiography, and renal function; 1 year follow‐up evaluating cardiovascular mortality and HF‐related hospitalization | Intrarenal venous flow patterns are associated with central venous pressure rather than cardiac index; discontinuous intrarenal venous flow patterns are independently associated with adverse outcomes |
| Husain‐Syed et al., 2019 74 | Prospective observational single centre | 205 patients with suspected or prediagnosed PH undergoing right heart catheterization; PH excluded in 40 patients; 165 patients diagnosed with PH group 1–5 | Characterization of Doppler‐derived intrarenal venous flow patterns and renal venous stasis index according to invasive haemodynamics, echocardiography, renal function, volume status, and intra‐abdominal pressure; median 1 year follow‐up evaluating composite endpoint of PH progression | Estimated GFR increases from renal venous stasis index = 0 to first tertile, but then decreases from second tertile of renal venous stasis index onwards; similar trend observed across intrarenal venous flow patterns |
| Experimental | ||||
| Winton 1931 76 | Prospective interventional | One dog model with isolated perfused kidneys | Ligature of renal veins (renal venous pressure of >20 mmHg) | Significant association between increased renal venous pressure, reduced renal blood flow, and reduced urine output; pressure in the vein is transmitted to the fluid in the distal portions of the tubules |
| Blake et al., 1949 84 | Prospective interventional | 22 intubated and anaesthetized dogs | Clamping of left renal vein (stepwise increase of renal vein pressure <600 mm saline), followed by reperfusion | Renal venous pressure elevation <350 mm saline leads to a significant decrease in free water and sodium excretion due to increased renal tubular reabsorption; further elevation (<600 mm saline) leads to reductions in renal blood flow and GFR |
| Hall et al., 1951 82 | Prospective interventional | 15 intubated and anaesthetized dogs | Ligature of left renal veins to allow comparison of congestive left kidneys with non‐congestive right kidneys (renal venous pressure of baseline, 10, 20, and 30 cm H2O) | Significant decrease in creatinine clearance and sodium and potassium excretion secondary to renal venous pressure elevation |
| Haddy et al., 1958 79 | Prospective interventional | 98 intubated and anaesthetized dogs | Compression of renal vein; cannulation of renal hilar lymph vessel [renal venous pressure of approx. 7 (baseline) and stepwise increase >25 mmHg] | Significant increase in renal lymph flow rate and renal vascular resistance secondary to venous pressure elevation |
| Lebrie et al., 1960 80 | Prospective interventional | Intubated and anaesthetized dogs | Partial occlusion of inferior vena cava above renal veins with balloon catheter [renal venous pressure of approx. 4 (baseline) and stepwise increase >25 cm H2O]; cannulation of renal capsular lymph vessels | Significant increase in renal lymph flow and decrease in urine output and sodium excretion secondary to venous pressure elevation |
| Burnett et al., 1980 85 | Prospective interventional | Ten intubated and anaesthetized dogs | Clamping of left renal vein [renal vein pressure of approx. 5 (baseline), 10, 20, 30, and 40 mmHg]; measurement of renal interstitial pressure | Renal venous pressure elevation in the presence of volume expansion leads to a gradual increase in renal interstitial pressure and gradual decreases in renal blood flow, GFR, and sodium excretion |
| Burnett et al., 1982 86 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats | Micropuncture tubular segmental analysis during left renal vein clamping in presence and absence of volume expansion (no data on renal venous pressure) | Significant increase as with decrease in fractional sodium excretion in euvolaemia vs. volume expansion; decreased proximal tubule sodium reabsorption in both volume states |
| Firth et al., 1988 75 | Prospective interventional | One rat model with isolated perfused kidneys | Ligation of renal vein (venous pressure of 0, 6.25, 12.5, 18.75, and 25 mmHg) | GFR increases slightly as venous pressure increases from 0 to 6.25 mmHg, but GFR and sodium excretion fall sharply when venous pressure rises above 6.25 mmHg, with these changes being reversible when venous pressure returns to baseline |
| Rohn et al., 1996 81 | Prospective interventional | Intubated and anaesthetized dogs | Partial occlusion of inferior vena cava above renal veins with balloon catheter [renal venous pressure 3.5 (baseline) and stepwise increase >27.2 cm H2O]; cannulation of renal lymph vessels | Significant increase in renal lymph flow and renal interstitial pressure secondary to renal venous pressure elevation, but increase >27.2 cm H2O leads to impaired lymphatic outflow |
| Doty et al., 1999 83 | Prospective interventional | Eight swine | Renal vein constriction (renal venous pressure of baseline and 30 mmHg) | Venous pressure elevation leads to significant decreases in renal blood flow and GFR and increases in plasma aldosterone and plasma renin activity, with these changes being reversible when renal venous pressure returns towards baseline |
| Doty et al., 2000 71 | Prospective interventional | Yorkshire swine (n = 6) vs. sham‐operated swine (n = 6) | Renal parenchymal compression (30 mmHg for 2 h) | Renal blood flow, GFR, plasma aldosterone or plasma renin activity are not affected by isolated elevation of renal parenchymal pressure |
| Li et al., 2012 77 | Prospective interventional | Intubated and anaesthetized mice vs. sham‐operated mice (C57BL/6) | Clamping of renal artery, vein, or both (whole pedicle) for 30–45 min followed by reperfusion | Renal vein clamping for 30 min induces a more pronounced decrease in renal blood flow and higher serum creatinine elevation than renal artery or pedicle clamping; at 24 h, renal vein clamping is associated with significantly increased pro‐inflammatory mediators (interleukin‐6, keratinocyte‐derived chemokine, granular‐colony stimulating factor, and monocyte chemoattractant protein‐1) compared with sham surgery |
| Shimada et al., 2018 78 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats vs. sham‐operated rats | Ligature by suture of inferior vena cava between renal veins to allow comparison of congestive left kidneys with non‐congestive right kidneys; measurement of cortical renal interstitial hydrostatic pressure | Significant increase in renal interstitial hydrostatic pressure secondary to venous pressure elevation compared with sham surgery |
| Huang et al., 2018 87 | Prospective interventional | 83 intubated and anaesthetized Lewis rats | Surgical left renal vein constriction [renal venous pressure of approx. 1 (baseline), 10, and 20 mmHg] | Elevation of renal venous pressure decreases ipsilateral renal blood flow and GFR, with the reduction being abolished by high salt diet but not renal denervation; the authors postulate that acute renal venous pressure elevation induces renal vasoconstriction and decreased GFR likely via the renin–angiotensin system rather than via the renal nerves |
GFR, glomerular filtration rate; HF, heart failure; PH, pulmonary hypertension.
Elevation of CVP is directly transmitted to the renal veins because venous vascular resistance is negligible. As the encapsulated kidney has little room to expand, renal interstitial hydrostatic pressure increases (Figure 2 ). 78 This increase may initially be prevented by a compensatory increase in renal lymphatic flow, 79 , 80 , 81 but continuing elevation of CVP will progressively reduce venous and lymphatic outflow and also late‐stage arterial inflow. 81 , 83
Figure 2.
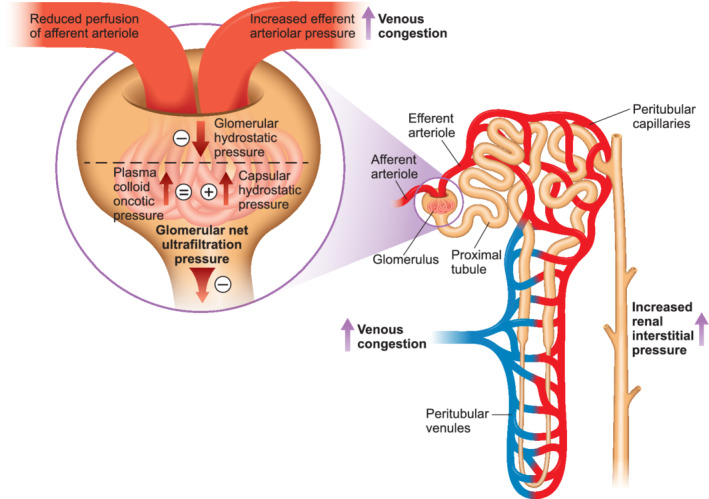
Venous congestion and glomerular haemodynamics. Renal venous congestion caused by intravascular congestion or an increase in intra‐abdominal pressure can lead to a build‐up of renal interstitial hydrostatic pressure through peritubular capillary congestion and development of interstitial oedema. This presumably leads to increased efferent arteriolar pressure, which may initially result in glomerular hyperfiltration; however, further increases in renal venous pressure with decreases in renal perfusion pressure ultimately reduce glomerular filtration rate.
As the post‐glomerular vascular and tubular network is a low‐pressure system, 88 , 89 , 90 increases in renal interstitial pressure cause compression or occlusion of vessels and tubules, resulting in reduced tubular secretion and reabsorption. 63 , 82 , 84 , 85 The renin–angiotensin–aldosterone system and the sympathetic nervous system are activated, leading to sodium and urea retention, interstitial oedema, endothelial dysfunction, reduced nitric oxide availability, increased production of inflammatory cytokines and reactive oxygen species, and reduced GFR. 71 , 75 , 77 , 83 , 85 , 86 , 91 The inflammatory response is also enhanced, 92 and the resulting increase in arterial stiffness and myocardial cell dysfunction further worsens renal dysfunction. Increased endothelial permeability results in fluid extravasation (e.g. into lung alveoli) and absorption of pro‐inflammatory endotoxin from the bowel. 92 Circulating lipopolysaccharide levels may amplify the systemic inflammation and induce acute kidney injury in this setting. 92
In animals 75 and humans, 2 a curvilinear relationship exists between CVP and GFR: as CVP increases, GFR first increases slightly then falls sharply. The early increase in GFR is presumably due to increased glomerular hydrostatic pressure consequent to elevated proximal peritubular capillary pressure, which results in increased efferent arteriolar pressure. 2 , 75 , 83 This phenomenon is comparable with the autoregulatory mechanism of the glomerulus, where efferent arteriole vasoconstriction leads to increased glomerular hydrostatic pressure and GFR. Increased renal venous pressure (e.g. during hydration) may initially lead to an increase in GFR by inducing glomerular hyperfiltration, as long as proximal tubular pressure remains below glomerular net ultrafiltration pressure (normally ~20 mmHg). 73 , 74 , 75 This assumption is supported by intrarenal Doppler ultrasonography studies showing increased GFR in the early stage of renal venous congestion. 74 Later, glomerular filtration progressively decreases and comes to a standstill during systole. In consequence, renal venous pressure dips only occur during RV diastolic filling. 73 , 74 Sodium and fluid retention also aggravate HF, further decreasing mean circulatory filling pressure and elevating renal venous pressure. Concomitant renovascular disease or treatment with renin–angiotensin–aldosterone system inhibitors and nonsteroidal anti‐inflammatory drugs may further interfere with maintenance of GFR. Of note, rat models suggest that hormonal factors may also be involved in the decrease of GFR, implicating pathways other than a simple reduction of the renal arteriovenous pressure gradient. 87
Proteinuria
In CN due to isolated RV failure (e.g. due to pulmonary arterial hypertension), a gradual increase in albuminuria is seen with increasing severity of congestion, although the increase probably remains within the physiological range. 74 , 93 Tubular dysfunction, chronic tubulointerstitial damage, 94 and increased levels of atrial natriuretic peptides, 95 which directly reduce proximal tubular reabsorption, may increase proteinuria. In contrast to patients with isolated RV failure, patients with HF commonly exhibit high levels of albuminuria (probably due to the presence of hypertensive nephrosclerosis, diabetic nephropathy, or renovascular disease). 96 A rapid increase in renal venous pressure may transiently increase proteinuria by causing acute glomerular and tubular dysfunction. Such functional albuminuria is probably common in HF and may be the consequence of congestion. 97 Table 2 provides an overview of studies reporting proteinuria related to venous congestion or IAP elevation.
Table 2.
Studies reporting proteinuria related to venous congestion or elevation of intra‐abdominal pressure
| Study | Design | Cohort | Methods | Findings |
|---|---|---|---|---|
| Bradley et al., 1947 63 | Prospective interventional single centre | 17 healthy individuals; mean GFR 115 ± 19 mL/min | External abdominal compression at 80 mmHg (resulting in intra‐abdominal pressure approx. 20 mmHg), invasively measured renal venous pressure in 9 individuals | Transient proteinuria and renal venous pressure elevation (from mean 5.8 to 18.3 mmHg) during abdominal compression |
| Vesely et al., 2001 95 | Prospective interventional single centre | 24 patients with HF with reduced ejection fraction and New York Heart Association functional class III; patients with serum creatinine levels >1.5 mg/dL were excluded | Infusion of long‐acting natriuretic peptide, vessel dilator, and kaliuretic peptide for a duration of 60 min | 2‐fold to 7‐fold increase in albuminuria, 2‐fold to 5‐fold increase in proteinuria, and 25‐fold to 40‐fold increase in urinary β2‐microglobulin (marker of proximal tubular reabsorption); authors postulate that part of the mechanism of the observed enhanced protein excretion is the inhibition of proximal tubular reabsorption of protein |
| Koyama et al., 2013 97 | Prospective observational single centre | 115 patients admitted for acute HF (preserved and reduced left ventricular ejection fraction); mean baseline estimated GFR 48 ± 23 mL/min/1.73 m2 | Spot urinary albumin‐to‐creatinine ratio measured on Days 1 and 7 of hospitalization | Increased albuminuria at admission with significant decrease within 7 days of treatment of cardiac decompensation; these changes were paralleled by decreases in N‐terminal pro‐b‐type natriuretic peptide levels, but not with baseline nor with changes in renal function |
| Navaneethan et al., 2016 98 | Prospective observational multi‐centre | 2959 patients with non‐dialysis‐dependent chronic kidney disease (estimated GFR: 20–70 mL/min/1.73 m2) and preserved left ventricular ejection fraction; PH present in 21%; patients with New York Heart Association functional class III/IV HF were excluded | Median 4.1 year follow‐up evaluating cardiovascular and renal outcomes, and all‐cause mortality | 24 h proteinuria comparable between those with and without PH (mean, 200 vs. 200 mg; P = 0.10), the overall higher‐than‐normal values likely reflecting the high prevalence of concomitant cardiovascular disease and diabetes in both cohorts |
| Jotwani et al., 2018 100 | Prospective observational dual centre | Random sample of 776 participants including cardiovascular disease and HF cases | Median 12.4 year follow‐up evaluating incident cardiovascular disease, HF, and all‐cause mortality | Higher urinary alpha‐1 microglobulin and urinary neutrophil gelatinase‐associated lipocalin levels are associated with elevated risk of incident cardiovascular disease and all‐cause mortality; no significant association with HF |
| Husain‐Syed et al., 2019 74 | Prospective observational single centre | 205 patients with suspected or prediagnosed PH undergoing right heart catheterization; PH excluded in 40 patients; 165 patients diagnosed with PH group 1–5 | Evaluation of baseline morning spot urinary protein‐to‐creatinine, albumin‐to‐creatinine, and α1‐microglobulin‐to‐creatinine ratios; median 1 year follow‐up evaluating composite endpoint of PH progression | Gradual increase in proteinuria, albuminuria, and α1‐microglobulin excretion with increasing severity of congestion, although the increase remains within the physiological range |
| Nickel et al., 2019 93 | Prospective observational dual‐centre | 283 patients with pulmonary arterial hypertension, 18 unaffected carriers of mutations in the gene encoding bone morphogenetic protein receptor type 2, 68 healthy controls (2 independent cohorts); patients with diabetes mellitus and estimated GFR < 60 mL/min/1.73 m2 were excluded | Morning spot urinary albumin‐to‐creatinine ratio | Gradual increase in albuminuria with increasing severity of congestion, although the increase remains within the physiological range (below the threshold of microalbuminuria) and is statistically non‐significant in this study; urinary albumin‐to‐creatinine ratio > 10 μg/mg significantly associated with higher odds of death or lung transplantation |
| Garimella et al., 2019 99 | Prospective multi‐centre open‐label clinical trial | Patients with high systolic blood pressure and high risk for cardiovascular events; 2337 selected non‐diabetic patients with estimated GFRs < 60 mL/min/1.73 m2; patients with HF were excluded | Median 3.8 year follow‐up evaluating a composite cardiovascular outcome | Lower urinary uromodulin excretion (which is associated with higher odds of tubular atrophy and fibrosis 151 ) and higher urinary alpha‐1 microglobulin levels are associated with elevated risk of HF |
| Experimental | ||||
| Winton 1931 76 | Prospective interventional | One dog model with isolated perfused kidneys | Ligature of renal veins (renal venous pressure of >20 mmHg) | Gradual increase in proteinuria during renal venous pressure elevation; proteinuria normalizes when renal venous pressure returns to baseline |
| Doty et al., 1999 83 | Prospective interventional | Eight swine | Renal vein constriction (renal venous pressure of baseline and 30 mmHg) | Renal venous pressure elevation leads to significantly increased proteinuria, with the finding being reversible when venous pressure returns towards baseline |
| Shimada et al., 2018 78 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats vs. sham‐operated rats | Ligature by suture of inferior vena cava between renal veins to allow comparison of congestive left kidneys with non‐congestive right kidneys | 3 days after surgery, significantly increased urinary albumin‐to‐creatinine ratio in the congestive left kidneys, potentially associated with observed podocyte injury and slit diaphragm disruption |
| Cops et al., 2018 101 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats (n = 7) vs. sham‐operated rats (n = 6) | Permanent surgical constriction (20 gauge) of thoracic inferior vena cava (increasing central venous pressure to a mean of 17 mmHg) | 12 weeks after surgery, plasma creatinine, plasma cystatin C, urinary albumin, glomerular surface area, and width of Bowman capsule increased significantly in the inferior vena cava group compared with the sham group; no difference in the acute tubular damage biomarker kidney injury molecule‐1 |
GFR, glomerular filtration rate; HF, heart failure; PH, pulmonary hypertension.
Histopathological findings
Studies in rodent models investigating the effects of congestion on renal histopathology report predominant congestion in peritubular capillaries, which, in the normal state, are almost invisible. These studies also report pericyte detachment, potentially resulting in dysregulated cortex and medullary circulation, hypoxia, and tubular injury, while chronic renal congestion may lead to tubular atrophy and fibrosis. 78 , 102 Renal histopathological findings from rodent models and a case report of a patient with idiopathic pulmonary arterial hypertension are described in Table 3 . Histopathological studies in humans with isolated CN are scarce because decreased GFR is usually attributed to nephrosclerosis and diabetic nephropathy. 107 , 108 Kidney biopsy is also often avoided because of an unproven increased risk of biopsy‐associated haemorrhage.
Table 3.
Studies reporting renal histopathological findings related to venous congestion, elevation of intra‐abdominal pressure or obstructive nephropathy
| Study | Design | Cohort | Methods | Findings |
|---|---|---|---|---|
| Faustinella et al., 1997 103 | Single‐centre case vignette | 34‐year‐old woman with idiopathic pulmonary hypertension; systolic pulmonary arterial pressure > 74 mmHg, 24 h proteinuria 5 g, and creatinine clearance 70 mL/min | Diagnostic kidney biopsy including immunohistologic and ultrastructural evaluation | Glomerulomegaly, mesangial hypercellularity and sclerosis, focal tubular atrophy, and interstitial fibrosis and inflammation; the authors postulate that elevation of central venous pressure, with passive congestion and glomerular capillary hypertension, is primarily responsible for the observed changes |
| Experimental | ||||
| Schachtrupp et al., 2002 67 | Prospective interventional | Intubated and anaesthetized domestic pigs | CO2 pneumoperitoneum (intra‐abdominal pressure of 15 mmHg for 24 h) | Low‐grade proximal tubular epithelial necrosis was observed |
| Sato et al., 2003 104 | Prospective interventional | Mice vs. sham‐operated mice (wild‐type and Smad3‐null) | Double‐ligation of right proximal ureter a | Wild‐type mice showed tubulointerstitial fibrosis associated with epithelial–mesenchymal transition of the renal tubules and collagen accumulation; this was prevented by lack of Smad3 |
| Li et al., 2012 77 | Prospective interventional | Intubated and anaesthetized mice vs. sham‐operated mice (C57BL/6) | Clamping of renal artery, vein, or both (whole pedicle) for 30 min followed by reperfusion | At 24 h after renal vascular clamping, both kidney function and histologic injury are the most severe in the renal vein clamping group |
| Chang et al., 2013 105 | Prospective interventional | Mice (ICR) | Intraperitoneal injection of albumin and normal saline (intra‐abdominal pressure of 0, 5, 10, or 20 cm H2O) | Increasing degrees of diffuse interstitial oedema, renal tubular lumen collapse, and interstitial inflammation were observed with increasing intra‐abdominal pressure |
| Shimada et al., 2018 78 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats vs. sham‐operated rats | Ligature by suture of inferior vena cava between renal veins to allow comparison of congestive left kidneys with non‐congestive right kidneys | 3 days after surgery, congestive left kidneys showed lesions in peritubular capillaries with pericyte detachment, up‐regulated pathways involved in extracellular matrix expansion and induction of expression of tubular injury markers (kidney injury molecule‐1) in stressed tubules; renal decapsulation ameliorated the tubular injury and profibrotic effects in the cortical region only |
| Owji et al., 2018 102 | Prospective interventional | 28 intubated and anaesthetized Sprague–Dawley rats | Bilateral clamping of the renal artery, vein, or both (whole pedicle) for 30 min followed by 2 h reperfusion; n = 7 in each group | At ~2 h after renal vascular clamping, both kidney dysfunction and histologic tubular injury were the most severe in the renal vein clamping group, with distinctive haemorrhagic congestion of peritubular capillaries in the cortex and medulla |
| Cops et al., 2018 101 | Prospective interventional | Intubated and anaesthetized Sprague–Dawley rats (n = 7) vs. sham‐operated rats (n = 6) | Permanent surgical constriction (20 gauge) of thoracic inferior vena cava (increasing central venous pressure to a mean of 17 mmHg) | 12 weeks after surgery, glomerular surface area and width of Bowman capsule increased significantly in the inferior vena cava group compared with the sham group; no difference in the acute tubular damage biomarker kidney injury molecule‐1 |
Experimental ureteral obstruction provides a model of obstructive nephropathy resulting in tubular injury and renal fibrosis. 106
Is congestive nephropathy a reversible condition?
In animal models, congestion‐induced renal dysfunction resolves completely when venous pressure is restored to basal levels with the extent of resolution depending on the duration and severity of congestion. 75 , 84 Improvement in renal function has been reported in a patient with HF after decongestion by peritoneal dialysis. 109 A recent post hoc analysis showed that sildenafil treatment in patients with pulmonary arterial hypertension improved renal function and reduced PH‐related morbidity. 110 Whether renal function improved owing to the effect of sildenafil on the pulmonary vasculature and right ventricle (and the resultant reduction in venous congestion) or owing to its direct vasodilatory and remodelling effect in the renal vasculature, or both, remains unknown.
Decongestion may not be effective in patients with pre‐existing CKD or long‐standing renal hypoperfusion or venous congestion, owing to the presence of irreversible tubulointerstitial damage. In studies on patients with end‐stage HF (43–49% of whom had ischaemic cardiomyopathy), the majority had improved renal function after implantation of a ventricular assist device (VAD), but the likelihood of improvement was lower in those with more severe preimplant renal dysfunction and diabetes. 111 , 112 , 113 Renal function improvement was probably owing to decreased venous congestion, increased systemic perfusion, and decreased hormonal activation. 114 , 115 In VAD recipients with improved renal function, renal Doppler ultrasonography showed decreased mean peak systolic velocity and increased mean end‐diastolic velocity, which together lowered the renal resistance index. The likely explanation is that reduction of venous congestion‐induced elevated renal interstitial pressure led to an increase in the cross‐sectional area of interstitial vessels and improved diastolic flow. 116 Renal function did not improve in some cases probably owing to underlying CKD (secondary to longstanding hypertension, diabetes, or renovascular disease), ongoing volume overload, or persistent low cardiac output despite VAD implantation.
In patients with acute HF, lowering of increased IAP by decongestive therapy can improve renal function, presumably by alleviating abdominal congestion. 65 In acute HF with ascites, paracentesis reduces IAP and volume overload and thereby improves renal function. 64 Paracentesis of ascites also improves renal function in patients with pulmonary arterial hypertension 117 and hepatorenal syndrome. 118 In patients with HF and refractory ascites, peritoneal dialysis is an alternative to repeated paracentesis. However, evidence on the benefits of peritoneal dialysis in this setting comes mostly from observational single‐centre studies. 119 Of note, peritoneal dialysis may temporarily increase IAP by generating an ‘artificial ascites’ through dialysate dwelling within the peritoneal cavity. However, the mean IAP with the classical intraperitoneal volume of 2 L in adult patients undergoing peritoneal dialysis is within the high‐normal range (9 ± 2 mmHg). 120 Factors associated with increased IAP include dialysate volume (IAP increases by 1.0 ± 0.3 mmHg for each 500 mL of infused volume) and body mass index. 121 There are no studies on IAP in CRS patients on peritoneal dialysis.
Diagnostic markers for congestive nephropathy
CN is a potentially reversible subtype of renal dysfunction, characterized by RV failure or volume overload. Decongestion may help to reverse renal dysfunction by improving RV function, lowering CVP/renal venous pressure, or lowering IAP/renal interstitial pressure. Notably, clinico‐biological presentation of CN may change with the severity of RV failure and/or volume overload, and with the duration of abnormal renal haemodynamics. Congestive acute kidney injury may not be associated with cellular damage, and complete renal function restoration may be a confirmatory diagnostic criterion. In contrast, a persistently low renal perfusion pressure might induce renal dysfunction and histopathological lesions with time. Thus, urinary markers may differ.
Diagnosis of CN is challenging because there is no gold standard to assess renal venous congestion. Many patients with CN have normal left ventricular ejection fraction, and the symptoms and signs of volume retention may quickly resolve with diuretic therapy. Moreover, the signs and symptoms of right HF are often nonspecific. Regardless, the diagnosis of acute kidney injury, volume overload, cardiac dysfunction, and any evidence of CKD must be pursued to establish potential reversibility of renal dysfunction by decongestion.
Clinical evaluation
Initial assessment would include the evaluation of symptoms, signs, and history; this is in accordance with the clinical practice guidelines of the European Society of Cardiology for HF 122 and PH. 6 Cardinal clinical symptoms/signs include recurrent short‐term weight gain due to volume overload; jugular venous distension; diuretic resistance (i.e. poor response to high doses of diuretics or need for combination of diuretics for sequential nephron segment blockade to achieve effective decongestion); previous unscheduled hospitalization for volume overload; and clinical/ultrasonographic signs of volume overload (bilateral ankle oedema, anasarca, pleural effusion, and/or ascites). If initial evaluation suggests HF/PH, advanced workup is necessary to demonstrate functional or structural alterations of the heart and the kidney as the underlying cause. CN may be suspected when high levels of natriuretic peptides 6 , 122 occur in combination with imaging signs of right HF and evidence of renal dysfunction. 123 , 124 , 125 Because this may refer to a large proportion of patients with HF, further diagnostic testing would be required to rule out other intrinsic causes of renal dysfunction.
Imaging: assessment of renal venous congestion
There is no method to measure renal venous congestion directly in the clinical setting. A wireless implantable haemodynamic monitoring system is available that measures pulmonary arterial pressure continuously; these data can be used by clinicians to assess congestion. The device has been shown to reduce HF‐related hospitalizations in outpatients with HF 8 ; however, availability and cost, and the invasive procedure for implantation, are major limitations. Currently, assessment of congestion is based on the CVP (inferior vena cava size and collapse), right atrial and RV size, and tricuspid annular plane systolic excursion (as a surrogate for RV systolic function), as well as parameters of RV–pulmonary circulation coupling. 123 , 126 , 127 In the non‐acute setting, congestion is usually assessed by observing whether renal function improves with decongestion.
Intrarenal Doppler ultrasonography can be useful for evaluating renal congestion as it can identify intrarenal venous flow patterns that predict diuretic response and adverse outcomes in HF, PH, and cardiac surgery. 36 , 53 , 73 , 74 Doppler intrarenal venous flow has shown stronger independent associations with adverse outcomes than invasive haemodynamic measurements, 73 , 74 suggesting that intrarenal venous flow may be an integrative marker of renal congestion. However, classification of discontinuous intrarenal venous flow patterns into different categories may miss important changes within those categories; a continuous measure may provide a more objective assessment of renal congestion. 74 Intrarenal Doppler ultrasonography may be useful for guiding HF‐specific and PH‐specific therapy, evaluating treatment response, and identifying patients at risk for adverse outcomes, but there are few studies examining dynamic changes in intrarenal venous flow. 36 So far, there have only been a few single‐centre reports on the use of Doppler ultrasonography to investigate renal congestion. No study has examined the correlation of invasively measured renal venous pressure with alterations in Doppler‐measured intrarenal venous flow. Of note, renal venous congestion does not necessarily indicate right HF, because tricuspid insufficiency with intact RV function may also induce congestion. Moreover, discontinuous intrarenal venous flow patterns have been described in obstructive nephropathy 128 where they are at least partly explained by increased renal interstitial pressure consequent to ureteral obstruction. Also, it remains unknown whether volume overload in absence of cardiac dysfunction (e.g. due to acute kidney injury) may also cause renal venous congestion. In our opinion, any Doppler‐derived discontinuous intrarenal venous flow is indicative of CN and calls for cardiac evaluation. It should be noted that ultrasound is relatively insensitive for detecting fibrotic changes. In a preclinical model, kidney elasticity estimation by ultrasound surface wave elastography (reflecting the combination of venous congestion, renal fibrosis, and altered renal compliance) correlated well with transcatheter measurement of kidney intracapsular pressure and IAP, 129 but this has not yet been confirmed in human studies. The use of other imaging techniques (e.g. magnetic resonance imaging) to assess renal venous congestion has not been described.
Other potentially useful diagnostic tests may include assessments of congestive hepatopathy secondary to HF (e.g. with Doppler‐derived portal venous flow alterations or liver stiffness measurement with transient elastography), but there are still limited data on their correlation with indices of RV failure and Doppler‐derived intrarenal venous flow. 53 , 130
Assessment of volume status
Among patients hospitalized for acute HF and deteriorating renal function, outcome is worse in those with residual congestion at discharge than in those without congestion. 9 What remains unknown is how underlying intrinsic renal insufficiency can be distinguished from the dynamic changes in GFR that commonly occur in the course of HF and during its management with diuretics and HF medications. Overall, it may be difficult to classify the patient with right HF to a CKD stage because serum creatinine elevation may also be due to congestion‐induced renal dysfunction or hypovolaemia resulting from excessive diuretic use. In both scenarios, achieving optimal volume status would allow more accurate estimation of baseline renal function and CKD stage. However, determining and maintaining the ideal volume status in patients with right HF is one of the most challenging problems in nephrology. A combination of different tools may be necessary to assess volume status, and monitoring of renal function during therapy would be needed to confirm the initial assessment. Of note, while ultrasonographically measured inferior vena cava diameter is used for assessment of intravascular volume, the diameter is also influenced by RV function and is thus a reflection of preload rather than tissue hydration. 131 Elevated levels of natriuretic peptides are indicators of intravascular and intracardiac congestion (e.g. atrial fibrillation), 58 but they are also influenced by medication; moreover, accumulation can occur in patients with renal dysfunction. 122 Therefore, natriuretic peptide levels must always be interpreted in the context of clinical findings. Carbohydrate antigen (CA)‐125 has potential value in HF as it is released by epithelial serous cells (pericardium, pleura, and/or peritoneum) in response to mechanical (hydrostatic pressure) or cytokine stimuli. 132 Furthermore, CA‐125 production is not influenced by age or renal function, which circumvents some of the limitations of natriuretic peptides. 133 Elevated levels of CA‐125 are found in two‐thirds of acute decompensated HF cases, 132 , 133 correlate with the severity of acute HF, 132 , 133 , 134 and relate to increased morbidity and mortality rates. 132 The CHANCE‐HF study examined the use of CA‐125‐guided therapy vs. standard of care in patients with acute HF and found a lower rate of rehospitalization for acute decompensated HF in the CA‐125‐guided group. Notably, patients allocated to the CA‐125 group were more frequently visited than patients in the standard of care group and received ambulatory administration of intravenous furosemide based on their CA‐125 levels. 135 Bioimpedance analysis is a non‐invasive technique to aid the clinical assessment of body mass and cellular water composition by bioelectrical impedance measurements, resistance, and reactance. 136 In patients with acute HF, bioimpedance analysis is a good predictor of length of hospital stay and correlates well with levels of natriuretic peptides and E/e′ ratio. 137 , 138 Furthermore, serial evaluation of bioimpedance analysis seems to be useful in monitoring volume status variations and the efficacy of decongestive therapy in HF. 139 , 140
Clinical chemistry: assessment of renal function
Equations using serum creatinine to calculate estimated GFR may overestimate renal function in patients with CN because of the high prevalence of non‐GFR determinants such as cardiac cachexia (with reduced creatinine generation) and low creatinine level due to serum dilution in patients with CRS. 141 Creatinine clearance may also be unreliable because incorrect collection/sampling may influence the GFR value. GFR equations based on cystatin C, which unlike serum creatinine is independent of muscle mass, may be superior for estimation of renal function. 141 However, diagnosis of CN does not necessarily require evidence of reduced renal function. Renal venous congestion precedes renal function decline as measured by established biomarkers such as serum creatinine and cystatin C 74 ; experimental studies suggest that early congestion is accompanied by a dramatic increase in lymphatic flow, which prevents any increase in renal interstitial pressure until full saturation. 79 , 80 This may particularly be the case in patients without intrinsic kidney damage (e.g. due to long‐standing hypertension and diabetes). Finally, different trajectories of changes in serum creatinine in acute HF have been described, 142 and further research is needed to evaluate their prognosis in terms of long‐term renal outcome and overall mortality.
Assessment of hormonal activation and biomarkers
There is no single laboratory marker of hormonal activation that has high discriminative power for CN; a combination of different markers may improve diagnostic accuracy. Increased blood urea nitrogen‐to‐creatinine ratio and dilutional hyponatraemia have been proposed as surrogate markers of hormonal activation as they reflect the disproportionate tubular reabsorption of urea and free water. 143 Persistent hypokalaemia (despite potassium substitution) and inverse urine sodium‐to‐potassium ratio indicate diuretic resistance due to hyperaldosteronism secondary to right HF. Hormone levels (e.g. renin, angiotensin II, and aldosterone) could support a diagnosis of CN, but antihypertensive medications may influence these parameters. In patients with HF, persistently low fractional excretion of sodium in urine despite use of potassium‐wasting diuretics suggests diuretic resistance and sodium retention, probably attributable to activationvof sodium chloride transport along the distal nephron. 144
Several novel tubular damage biomarkers have been identified, but their value in acutely decompensated HF may be limited to distinguishing serum creatinine elevation due to kidney damage from functional serum creatinine fluctuations. 145 Research on biomarkers in HF (e.g. soluble ST2, galectin‐3, copeptin, and adrenomedullin) has not yet found any that can be recommended for clinical practice. 122 However, galectin‐3 may be of interest in CN as it is associated with the development and progression of CKD and predicts development of HF. 146 , 147
Directions for future research
Experimental
Future animal models should clarify the impact of long‐standing venous congestion on renal pathology and renal function. Detailed immunohistologic and ultrastructural studies are needed. Only one study has examined the effects of congestion on the kidney, and that was in a rat model of abdominal venous congestion for up to 12 weeks, 101 which was too short for detailed analysis. In animal models, ligation of the inferior vena cava between the renal veins can generate collateral circulation, which would lower inferior vena cava pressure and relieve renal venous congestion; thus, alternative models need to be developed to study long‐term effects. 148 , 149
Clinical
In patients with CRS and persistent and/or progressive renal dysfunction despite adequate decongestion, we believe renal biopsy might be considered as it may help to identify patient subsets likely to have improvement in residual renal function after restoration of cardiac function by segregating those with reversible from those with irreversible tubulointerstitial damage. Further studies are needed to determine if CVP is a suitable metric to capture CN. Research is also needed to validate the role of intrarenal Doppler ultrasonography in the management of HF and PH and evaluation of volume status. Intrarenal Doppler ultrasonography performed at baseline and throughout therapy could help establish specific Doppler‐derived renal congestion targets indicative of optimal volume and RV status in individual patients, similar to the strategies used to guide medication adjustment in studies of pulmonary artery sensors. 150 Intrarenal Doppler ultrasonography studies should include patients requiring renal replacement therapy for diuretic‐resistant volume overload and acute kidney injury to evaluate the severity of renal congestion and to identify when, during renal replacement therapy, improvement in residual renal function will permit discontinuation of renal replacement therapy.
Conclusions
Prognosis varies widely among patients with concomitant cardiac and renal dysfunction, so it is important to identify high‐risk patients who might benefit from intensive monitoring and therapy. The adverse impact of congestion on renal function has long been recognized, but it is still not given due consideration in clinical practice. Early decongestion can improve renal function and outcome. Clear definition of this haemodynamic phenotype of renal dysfunction will help physicians identify patients likely to benefit from specific management strategies. We suggest the term CN for a potentially reversible subtype of renal dysfunction associated with declining renal venous outflow and progressively increasing renal interstitial pressure. Discontinuous venous flow patterns on intrarenal Doppler ultrasonography may indicate CN and the need for detailed cardiac evaluation. Further research is needed to validate the role of intrarenal Doppler ultrasonography in the management of HF and PH, to address the challenge of evaluating and optimizing volume status, and to identify the CVP value that provides the best balance of RV and renal function.
Conflict of interest
Dr. Gall discloses personal fees and non‐financial support from Actelion, AstraZeneca, Bayer, BMS, GlaxoSmithKline, Janssen Cilag, Lilly, MSD, Novartis, Pfizer, and United Therapeutics/OMT outside the submitted work. Dr. Seeger discloses personal fees for consulting from Bayer Pharma AG, from Liquidia Technologies, Inc, and from United Therapeutics Corporation outside the submitted work. Dr. Ghofrani discloses grants from German Research Foundation (DFG) during the conduct of the study and personal fees from Actelion, Bayer, GSK, Novartis, Pfizer, Bellerophon Pulse Technologies, and MSD Merck Sharpe & Dohme outside the submitted work. None of the other authors declare any competing interests.
Funding
The authors received no specific funding for this work.
Acknowledgements
Editorial assistance was provided by Claire Mulligan, PhD (Beacon Medical Communications Ltd, Brighton, UK), funded by the University of Giessen. Open access funding enabled and organized by Projekt DEAL.
Husain‐Syed, F. , Gröne, H.‐J. , Assmus, B. , Bauer, P. , Gall, H. , Seeger, W. , Ghofrani, A. , Ronco, C. , and Birk, H.‐W. (2021) Congestive nephropathy: a neglected entity? Proposal for diagnostic criteria and future perspectives. ESC Heart Failure, 8: 183–203. 10.1002/ehf2.13118.
Claudio Ronco and Horst‐Walter Birk are joint last authors.
References
- 1. Mullens W, Abrahams Z, Francis GS, Sokos G, Taylor DO, Starling RC, Young JB, Tang WHW. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol 2009; 53: 589–596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009; 53: 582–588. [DOI] [PubMed] [Google Scholar]
- 3. Husain‐Syed F, McCullough PA, Birk HW, Renker M, Brocca A, Seeger W, Ronco C. Cardio‐pulmonary‐renal interactions: a multidisciplinary approach. J Am Coll Cardiol 2015; 65: 2433–2448. [DOI] [PubMed] [Google Scholar]
- 4. Verbrugge FH, Dupont M, Steels P, Grieten L, Malbrain M, Tang WH, Mullens W. Abdominal contributions to cardiorenal dysfunction in congestive heart failure. J Am Coll Cardiol 2013; 62: 485–495. [DOI] [PubMed] [Google Scholar]
- 5. Costanzo MR, Ronco C, Abraham WT, Agostoni P, Barasch J, Fonarow GC, Gottlieb SS, Jaski BE, Kazory A, Levin AP, Levin HR, Marenzi G, Mullens W, Negoianu D, Redfield MM, Tang WHW, Testani JM, Voors AA. Extracorporeal ultrafiltration for fluid overload in heart failure: current status and prospects for further research. J Am Coll Cardiol 2017; 69: 2428–2445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, ESC Scientific Document Group . 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016; 37: 67–119. [DOI] [PubMed] [Google Scholar]
- 7. Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133. [DOI] [PubMed] [Google Scholar]
- 8. Abraham WT, Adamson PB, Bourge RC, Aaron MF, Costanzo MR, Stevenson LW, Strickland W, Neelagaru S, Raval N, Krueger S, Weiner S, Shavelle D, Jeffries B, Yadav JS, Group CTS . Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011; 377: 658–666. [DOI] [PubMed] [Google Scholar]
- 9. Metra M, Davison B, Bettari L, Sun H, Edwards C, Lazzarini V, Piovanelli B, Carubelli V, Bugatti S, Lombardi C, Cotter G, Dei Cas L. Is worsening renal function an ominous prognostic sign in patients with acute heart failure? The role of congestion and its interaction with renal function. Circ Heart Fail 2012; 5: 54–62. [DOI] [PubMed] [Google Scholar]
- 10. Bart BA, Goldsmith SR, Lee KL, Givertz MM, O'Connor CM, Bull DA, Redfield MM, Deswal A, Rouleau JL, LeWinter MM, Ofili EO, Stevenson LW, Semigran MJ, Felker GM, Chen HH, Hernandez AF, Anstrom KJ, McNulty SE, Velazquez EJ, Ibarra JC, Mascette AM, Braunwald E, Heart Failure Clinical Research N . Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med 2012; 367: 2296–2304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Costanzo MR, Stevenson LW, Adamson PB, Desai AS, Heywood JT, Bourge RC, Bauman J, Abraham WT. Interventions linked to decreased heart failure hospitalizations during ambulatory pulmonary artery pressure monitoring. J Am Coll Cardiol HF 2016; 4: 333–344. [DOI] [PubMed] [Google Scholar]
- 12. Testani JM, Chen J, McCauley BD, Kimmel SE, Shannon RP. Potential effects of aggressive decongestion during the treatment of decompensated heart failure on renal function and survival. Circulation 2010; 122: 265–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol 2008; 52: 1527–1539. [DOI] [PubMed] [Google Scholar]
- 14. Ronco C, Cicoira M, McCullough PA. Cardiorenal syndrome type 1: pathophysiological crosstalk leading to combined heart and kidney dysfunction in the setting of acutely decompensated heart failure. J Am Coll Cardiol 2012; 60: 1031–1042. [DOI] [PubMed] [Google Scholar]
- 15. Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, Jafar T, Jassal SK, Landman GW, Muntner P, Roderick P, Sairenchi T, Schottker B, Shankar A, Shlipak M, Tonelli M, Townend J, van Zuilen A, Yamagishi K, Yamashita K, Gansevoort R, Sarnak M, Warnock DG, Woodward M, Arnlov J, CKD Prognosis Consortium . Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta‐analysis of individual participant data. Lancet Diabetes Endocrinol 2015; 3: 514–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR, UKPDS Study Group . Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006; 55: 1832–1839. [DOI] [PubMed] [Google Scholar]
- 17. Mahmoodi BK, Matsushita K, Woodward M, Blankestijn PJ, Cirillo M, Ohkubo T, Rossing P, Sarnak MJ, Stengel B, Yamagishi K, Yamashita K, Zhang L, Coresh J, de Jong PE, Astor BC, Chronic Kidney Disease Prognosis Consortium . Associations of kidney disease measures with mortality and end‐stage renal disease in individuals with and without hypertension: a meta‐analysis. Lancet 2012; 380: 1649–1661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Dhaun N, Bellamy CO, Cattran DC, Kluth DC. Utility of renal biopsy in the clinical management of renal disease. Kidney Int 2014; 85: 1039–1048. [DOI] [PubMed] [Google Scholar]
- 19. Meyrier A. Nephrosclerosis: a term in quest of a disease. Nephron 2015; 129: 276–282. [DOI] [PubMed] [Google Scholar]
- 20. Damman K, Navis G, Smilde TD, Voors AA, van der Bij W, van Veldhuisen DJ, Hillege HL. Decreased cardiac output, venous congestion and the association with renal impairment in patients with cardiac dysfunction. Eur J Heart Fail 2007; 9: 872–878. [DOI] [PubMed] [Google Scholar]
- 21. Klahr S. Obstructive nephropathy. Intern Med 2000; 39: 355–361. [DOI] [PubMed] [Google Scholar]
- 22. Fender EA, Zack CJ, Nishimura RA. Isolated tricuspid regurgitation: outcomes and therapeutic interventions. Heart 2018; 104: 798–806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Opotowsky AR, Baraona FR, Mc Causland FR, Loukas B, Landzberg E, Landzberg MJ, Sabbisetti V, Waikar SS. Estimated glomerular filtration rate and urine biomarkers in patients with single‐ventricle Fontan circulation. Heart 2017; 103: 434–442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Saiki H, Kuwata S, Kurishima C, Iwamoto Y, Ishido H, Masutani S, Senzaki H. Prevalence, implication, and determinants of worsening renal function after surgery for congenital heart disease. Heart Vessels 2016; 31: 1313–1318. [DOI] [PubMed] [Google Scholar]
- 25. Dupont M, Mullens W, Finucan M, Taylor DO, Starling RC, Tang WH. Determinants of dynamic changes in serum creatinine in acute decompensated heart failure: the importance of blood pressure reduction during treatment. Eur J Heart Fail 2013; 15: 433–440. [DOI] [PubMed] [Google Scholar]
- 26. Van Aelst LNL, Arrigo M, Placido R, Akiyama E, Girerd N, Zannad F, Manivet P, Rossignol P, Badoz M, Sadoune M, Launay JM, Gayat E, Lam CSP, Cohen‐Solal A, Mebazaa A, Seronde MF. Acutely decompensated heart failure with preserved and reduced ejection fraction present with comparable haemodynamic congestion. Eur J Heart Fail 2018; 20: 738–747. [DOI] [PubMed] [Google Scholar]
- 27. Chioncel O, Mebazaa A, Maggioni AP, Harjola VP, Rosano G, Laroche C, Piepoli MF, Crespo‐Leiro MG, Lainscak M, Ponikowski P, Filippatos G, Ruschitzka F, Seferovic P, Coats AJS, Lund LH, ESC‐EORP‐HFA Heart Failure Long‐Term Registry Investigators . Acute heart failure congestion and perfusion status—impact of the clinical classification on in‐hospital and long‐term outcomes; insights from the ESC‐EORP‐HFA Heart Failure Long‐Term Registry. Eur J Heart Fail 2019; 21: 1338–1352. [DOI] [PubMed] [Google Scholar]
- 28. Binanay C, Califf RM, Hasselblad V, O'Connor CM, Shah MR, Sopko G, Stevenson LW, Francis GS, Leier CV, Miller LW, Investigators E , Coordinators ES . Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA 2005; 294: 1625–1633. [DOI] [PubMed] [Google Scholar]
- 29. Zile MR, Bennett TD, St John Sutton M, Cho YK, Adamson PB, Aaron MF, Aranda JM Jr, Abraham WT, Smart FW, Stevenson LW, Kueffer FJ, Bourge RC. Transition from chronic compensated to acute decompensated heart failure: pathophysiological insights obtained from continuous monitoring of intracardiac pressures. Circulation 2008; 118: 1433–1441. [DOI] [PubMed] [Google Scholar]
- 30. Ishihara S, Gayat E, Sato N, Arrigo M, Laribi S, Legrand M, Placido R, Manivet P, Cohen‐Solal A, Abraham WT, Jessup M, Mebazaa A. Similar hemodynamic decongestion with vasodilators and inotropes: systematic review, meta‐analysis, and meta‐regression of 35 studies on acute heart failure. Clin Res Cardiol 2016; 105: 971–980. [DOI] [PubMed] [Google Scholar]
- 31. Ghio S, Guazzi M, Scardovi AB, Klersy C, Clemenza F, Carluccio E, Temporelli PL, Rossi A, Faggiano P, Traversi E, Vriz O, Dini FL, all investigators . Different correlates but similar prognostic implications for right ventricular dysfunction in heart failure patients with reduced or preserved ejection fraction. Eur J Heart Fail 2017; 19: 873–879. [DOI] [PubMed] [Google Scholar]
- 32. Stevenson LW. Tailored therapy to hemodynamic goals for advanced heart failure. Eur J Heart Fail 1999; 1: 251–257. [DOI] [PubMed] [Google Scholar]
- 33. Mehra MR, Park MH, Landzberg MJ, Lala A, Waxman AB, International Right Heart Failure Foundation Scientific Working Group . Right heart failure: toward a common language. J Heart Lung Transplant 2014; 33: 123–126. [DOI] [PubMed] [Google Scholar]
- 34. Rosenkranz S, Gibbs JS, Wachter R, De Marco T, Vonk‐Noordegraaf A, Vachiery JL. Left ventricular heart failure and pulmonary hypertension. Eur Heart J 2016; 37: 942–954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Guazzi M, Naeije R. Pulmonary hypertension in heart failure: pathophysiology, pathobiology, and emerging clinical perspectives. J Am Coll Cardiol 2017; 69: 1718–1734. [DOI] [PubMed] [Google Scholar]
- 36. Nijst P, Martens P, Dupont M, Tang WHW, Mullens W. Intrarenal flow alterations during transition from euvolemia to intravascular volume expansion in heart failure patients. J Am Coll Cardiol HF 2017; 5: 672–681. [DOI] [PubMed] [Google Scholar]
- 37. Damman K, Masson S, Lucci D, Gorini M, Urso R, Maggioni AP, Tavazzi L, Tarantini L, Tognoni G, Voors A, Latini R. Progression of renal impairment and chronic kidney disease in chronic heart failure: an analysis from GISSI‐HF. J Card Fail 2017; 23: 2–9. [DOI] [PubMed] [Google Scholar]
- 38. Damman K, Jaarsma T, Voors AA, Navis G, Hillege HL, van Veldhuisen DJ, COACH investigators . Both in‐ and out‐hospital worsening of renal function predict outcome in patients with heart failure: results from the Coordinating Study Evaluating Outcome of Advising and Counseling in Heart Failure (COACH). Eur J Heart Fail 2009; 11: 847–854. [DOI] [PubMed] [Google Scholar]
- 39. Tsai YC, Tsai JC, Chen SC, Chiu YW, Hwang SJ, Hung CC, Chen TH, Kuo MC, Chen HC. Association of fluid overload with kidney disease progression in advanced CKD: a prospective cohort study. Am J Kidney Dis 2014; 63: 68–75. [DOI] [PubMed] [Google Scholar]
- 40. Hung SC, Lai YS, Kuo KL, Tarng DC. Volume overload and adverse outcomes in chronic kidney disease: clinical observational and animal studies. J Am Heart Assoc 2015; 4: e001918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Navaneethan SD, Wehbe E, Heresi GA, Gaur V, Minai OA, Arrigain S, Nally JV Jr, Schold JD, Rahman M, Dweik RA. Presence and outcomes of kidney disease in patients with pulmonary hypertension. Clin J Am Soc Nephrol 2014; 9: 855–863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Li Z, Liang X, Liu S, Ye Z, Chen Y, Wang W, Li R, Xu L, Feng Z, Shi W. Pulmonary hypertension: epidemiology in different CKD stages and its association with cardiovascular morbidity. PLoS ONE 2014; 9: e114392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Mavrakanas TA, Khattak A, Singh K, Charytan DM. Echocardiographic parameters and renal outcomes in patients with preserved renal function, and mild–moderate CKD. BMC Nephrol 2018; 19: 176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. O'Leary JM, Assad TR, Xu M, Birdwell KA, Farber‐Eger E, Wells QS, Hemnes AR, Brittain EL. Pulmonary hypertension in patients with chronic kidney disease: invasive hemodynamic etiology and outcomes. Pulm Circ 2017; 7: 674–683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Pabst S, Hammerstingl C, Hundt F, Gerhardt T, Grohe C, Nickenig G, Woitas R, Skowasch D. Pulmonary hypertension in patients with chronic kidney disease on dialysis and without dialysis: results of the PEPPER‐study. PLoS ONE 2012; 7: e35310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Haddad F, Peterson T, Fuh E, Kudelko KT, de Jesus Perez V, Skhiri M, Vagelos R, Schnittger I, Denault AY, Rosenthal DN, Doyle RL, Zamanian RT. Characteristics and outcome after hospitalization for acute right heart failure in patients with pulmonary arterial hypertension. Circ Heart Fail 2011; 4: 692–699. [DOI] [PubMed] [Google Scholar]
- 47. Sztrymf B, Souza R, Bertoletti L, Jais X, Sitbon O, Price LC, Simonneau G, Humbert M. Prognostic factors of acute heart failure in patients with pulmonary arterial hypertension. Eur Respir J 2010; 35: 1286–1293. [DOI] [PubMed] [Google Scholar]
- 48. Sztrymf B, Prat D, Jacobs FM, Brivet FG, O'Callaghan DS, Price LC, Jais X, Sitbon O, Simonneau G, Humbert M. Renal replacement therapy in patients with severe precapillary pulmonary hypertension with acute right heart failure. Respiration 2013; 85: 464–470. [DOI] [PubMed] [Google Scholar]
- 49. Shah SJ, Thenappan T, Rich S, Tian L, Archer SL, Gomberg‐Maitland M. Association of serum creatinine with abnormal hemodynamics and mortality in pulmonary arterial hypertension. Circulation 2008; 117: 2475–2483. [DOI] [PubMed] [Google Scholar]
- 50. Broda CR, Sriraman H, Wadhwa D, Wang Y, Tunuguntla H, Akcan‐Arikan A, Ermis PR, Price JF. Renal dysfunction is associated with higher central venous pressures in patients with Fontan circulation. Congenit Heart Dis 2018; 13: 602–607. [DOI] [PubMed] [Google Scholar]
- 51. Anne P, Du W, Mattoo TK, Zilberman MV. Nephropathy in patients after Fontan palliation. Int J Cardiol 2009; 132: 244–247. [DOI] [PubMed] [Google Scholar]
- 52. Rychik J. The relentless effects of the Fontan paradox. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2016; 19: 37–43. [DOI] [PubMed] [Google Scholar]
- 53. Beaubien‐Souligny W, Benkreira A, Robillard P, Bouabdallaoui N, Chasse M, Desjardins G, Lamarche Y, White M, Bouchard J, Denault A. Alterations in portal vein flow and intrarenal venous flow are associated with acute kidney injury after cardiac surgery: a prospective observational cohort study. J Am Heart Assoc 2018; 7: e009961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Saito S, Uchino S, Takinami M, Uezono S, Bellomo R. Postoperative blood pressure deficit and acute kidney injury progression in vasopressor‐dependent cardiovascular surgery patients. Crit Care 2016; 20: 74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Guven G, Brankovic M, Constantinescu AA, Brugts JJ, Hesselink DA, Akin S, Struijs A, Birim O, Ince C, Manintveld OC, Caliskan K. Preoperative right heart hemodynamics predict postoperative acute kidney injury after heart transplantation. Intensive Care Med 2018; 44: 588–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Lee JW, Song JM, Park JP, Lee JW, Kang DH, Song JK. Long‐term prognosis of isolated significant tricuspid regurgitation. Circ J 2010; 74: 375–380. [DOI] [PubMed] [Google Scholar]
- 57. Topilsky Y, Khanna AD, Oh JK, Nishimura RA, Enriquez‐Sarano M, Jeon YB, Sundt TM, Schaff HV, Park SJ. Preoperative factors associated with adverse outcome after tricuspid valve replacement. Circulation 2011; 123: 1929–1939. [DOI] [PubMed] [Google Scholar]
- 58. Boorsma EM, Ter Maaten JM, Damman K, Dinh W, Gustafsson F, Goldsmith S, Burkhoff D, Zannad F, Udelson JE, Voors AA. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nat Rev Cardiol 2020; 17: 641–655. [DOI] [PubMed] [Google Scholar]
- 59. Fallick C, Sobotka PA, Dunlap ME. Sympathetically mediated changes in capacitance: redistribution of the venous reservoir as a cause of decompensation. Circ Heart Fail 2011; 4: 669–675. [DOI] [PubMed] [Google Scholar]
- 60. Fudim M, Jones WS, Boortz‐Marx RL, Ganesh A, Green CL, Hernandez AF, Patel MR. Splanchnic nerve block for acute heart failure. Circulation 2018; 138: 951–953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Malbrain ML, Cheatham ML, Kirkpatrick A, Sugrue M, Parr M, De Waele J, Balogh Z, Leppaniemi A, Olvera C, Ivatury R, D'Amours S, Wendon J, Hillman K, Johansson K, Kolkman K, Wilmer A. Results from the international conference of experts on intra‐abdominal hypertension and abdominal compartment syndrome. I. Definitions. Intensive Care Med 2006; 32: 1722–1732. [DOI] [PubMed] [Google Scholar]
- 62. Caldwell CB, Ricotta JJ. Changes in visceral blood flow with elevated intraabdominal pressure. J Surg Res 1987; 43: 14–20. [DOI] [PubMed] [Google Scholar]
- 63. Bradley SE, Bradley GP. The effect of increased intra‐abdominal pressure on renal function in man. J Clin Invest 1947; 26: 1010–1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Mullens W, Abrahams Z, Francis GS, Taylor DO, Starling RC, Tang WH. Prompt reduction in intra‐abdominal pressure following large‐volume mechanical fluid removal improves renal insufficiency in refractory decompensated heart failure. J Card Fail 2008; 14: 508–514. [DOI] [PubMed] [Google Scholar]
- 65. Mullens W, Abrahams Z, Skouri HN, Francis GS, Taylor DO, Starling RC, Paganini E, Tang WH. Elevated intra‐abdominal pressure in acute decompensated heart failure: a potential contributor to worsening renal function? J Am Coll Cardiol 2008; 51: 300–306. [DOI] [PubMed] [Google Scholar]
- 66. Rubio‐Gracia J, Gimenez‐Lopez I, Sanchez‐Marteles M, Josa‐Laorden C, Perez‐Calvo JI. Intra‐abdominal pressure and its relationship with markers of congestion in patients admitted for acute decompensated heart failure. Heart Vessels 2020; 35: 1545–1556. [DOI] [PubMed] [Google Scholar]
- 67. Schachtrupp A, Toens C, Hoer J, Klosterhalfen B, Lawong AG, Schumpelick V. A 24‐h pneumoperitoneum leads to multiple organ impairment in a porcine model. J Surg Res 2002; 106: 37–45. [DOI] [PubMed] [Google Scholar]
- 68. Winton FR. Arterial, venous, intrarenal, and extrarenal pressure effects on renal blood flow. Circ Res 1964; 15: 103–109. [PubMed] [Google Scholar]
- 69. Thorington JM, Schmidt CF. A study of urinary output and blood pressure changes resulting in experimental ascites. Am J Med Sci 1923; 165: 880–886. [Google Scholar]
- 70. Toens C, Schachtrupp A, Hoer J, Junge K, Klosterhalfen B, Schumpelick V. A porcine model of the abdominal compartment syndrome. Shock 2002; 18: 316–321. [DOI] [PubMed] [Google Scholar]
- 71. Doty JM, Saggi BH, Blocher CR, Fakhry I, Gehr T, Sica D, Sugerman HJ. Effects of increased renal parenchymal pressure on renal function. J Trauma 2000; 48: 874–877. [DOI] [PubMed] [Google Scholar]
- 72. Harman PK, Kron IL, McLachlan HD, Freedlender AE, Nolan SP. Elevated intra‐abdominal pressure and renal function. Ann Surg 1982; 196: 594–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Iida N, Seo Y, Sai S, Machino‐Ohtsuka T, Yamamoto M, Ishizu T, Kawakami Y, Aonuma K. Clinical implications of intrarenal hemodynamic evaluation by Doppler ultrasonography in heart failure. J Am Coll Cardiol HF 2016; 4: 674–682. [DOI] [PubMed] [Google Scholar]
- 74. Husain‐Syed F, Birk HW, Ronco C, Schormann T, Tello K, Richter MJ, Wilhelm J, Sommer N, Steyerberg E, Bauer P, Walmrath HD, Seeger W, McCullough PA, Gall H, Ghofrani HA. Doppler‐derived renal venous stasis index in the prognosis of right heart failure. J Am Heart Assoc 2019; 8: e013584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Firth JD, Raine AE, Ledingham JG. Raised venous pressure: a direct cause of renal sodium retention in oedema? Lancet 1988; 1: 1033–1035. [DOI] [PubMed] [Google Scholar]
- 76. Winton FR. The influence of venous pressure on the isolated mammalian kidney. J Physiol 1931; 72: 49–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Li X, Liu M, Bedja D, Thoburn C, Gabrielson K, Racusen L, Rabb H. Acute renal venous obstruction is more detrimental to the kidney than arterial occlusion: implication for murine models of acute kidney injury. Am J Physiol Renal Physiol 2012; 302: F519–F525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Shimada S, Hirose T, Takahashi C, Sato E, Kinugasa S, Ohsaki Y, Kisu K, Sato H, Ito S, Mori T. Pathophysiological and molecular mechanisms involved in renal congestion in a novel rat model. Sci Rep 2018; 8: 16808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Haddy FJ, Scott J, Fleishman M, Emanuel D. Effect of change in renal venous pressure upon renal vascular resistance, urine and lymph flow rates. Am J Physiol 1958; 195: 97–110. [DOI] [PubMed] [Google Scholar]
- 80. Lebrie SJ, Mayerson HS. Influence of elevated venous pressure on flow and composition of renal lymph. Am J Physiol 1960; 198: 1037–1040. [DOI] [PubMed] [Google Scholar]
- 81. Rohn DA, Stewart RH, Elk JR, Laine GA, Drake RE. Renal lymphatic function following venous pressure elevation. Lymphology 1996; 29: 67–75. [PubMed] [Google Scholar]
- 82. Hall PW 3rd, Selkurt EE. Effects of partial graded venous obstruction on electrolyte clearance by the dog's kidney. Am J Physiol 1951; 164: 143–154. [DOI] [PubMed] [Google Scholar]
- 83. Doty JM, Saggi BH, Sugerman HJ, Blocher CR, Pin R, Fakhry I, Gehr TW, Sica DA. Effect of increased renal venous pressure on renal function. J Trauma 1999; 47: 1000–1003. [DOI] [PubMed] [Google Scholar]
- 84. Blake WD, Wégria R, Keating RP, Ward HP. Effect of increased renal venous pressure on renal function. Am J Physiol 1949; 157: 1–13. [DOI] [PubMed] [Google Scholar]
- 85. Burnett JC Jr, Knox FG. Renal interstitial pressure and sodium excretion during renal vein constriction. Am J Physiol 1980; 238: F279–F282. [DOI] [PubMed] [Google Scholar]
- 86. Burnett JC Jr, Haas JA, Knox FG. Segmental analysis of sodium reabsorption during renal vein constriction. Am J Physiol 1982; 243: F19–F22. [DOI] [PubMed] [Google Scholar]
- 87. Huang X, Hamza SM, Zhuang W, Cupples WA, Braam B. Sodium intake but not renal nerves attenuates renal venous pressure‐induced changes in renal hemodynamics in rats. Am J Physiol Renal Physiol 2018; 315: F644–F652. [DOI] [PubMed] [Google Scholar]
- 88. Gottschalk CW. 23—a review of intrarenal hemodynamics and hydrodynamics In Boyarsky S., Tanagho E. A., Gottschalk C. W., Zimskind P. D., eds. Urodynamics: Hydrodynamics of the Ureter and Renal Pelvis. New York: Academic Press; 1971. p 299–308. [Google Scholar]
- 89. Neal CR, Arkill KP, Bell JS, Betteridge KB, Bates DO, Winlove CP, Salmon AHJ, Harper SJ. Novel hemodynamic structures in the human glomerulus. Am J Physiol Renal Physiol 2018; 315: F1370–F1384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Oken DE. An analysis of glomerular dynamics in rat, dog, and man. Kidney Int 1982; 22: 136–145. [DOI] [PubMed] [Google Scholar]
- 91. Mohmand H, Goldfarb S. Renal dysfunction associated with intra‐abdominal hypertension and the abdominal compartment syndrome. J Am Soc Nephrol 2011; 22: 615–621. [DOI] [PubMed] [Google Scholar]
- 92. Colombo PC, Ganda A, Lin J, Onat D, Harxhi A, Iyasere JE, Uriel N, Cotter G. Inflammatory activation: cardiac, renal, and cardio‐renal interactions in patients with the cardiorenal syndrome. Heart Fail Rev 2012; 17: 177–190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Nickel N, Perez VAJ, Fessel JP, Cogan J, Hamid R, West JD, de Caestecker M, Yang H, Zamanian RT, Austin E. Low‐grade albuminuria in pulmonary arterial hypertension. Pulm Circ 2019; 9: 2045894018824564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Wagner MC, Campos‐Bilderback SB, Chowdhury M, Flores B, Lai X, Myslinski J, Pandit S, Sandoval RM, Wean SE, Wei Y, Satlin LM, Wiggins RC, Witzmann FA, Molitoris BA. Proximal tubules have the capacity to regulate uptake of albumin. J Am Soc Nephrol 2016; 27: 482–494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Vesely DL, Perez‐Lamboy GI, Schocken DD. Long‐acting natriuretic peptide, vessel dilator, and kaliuretic peptide enhance urinary excretion rate of albumin, total protein, and beta(2)‐microglobulin in patients with congestive heart failure. J Card Fail 2001; 7: 55–63. [DOI] [PubMed] [Google Scholar]
- 96. Jackson CE, Solomon SD, Gerstein HC, Zetterstrand S, Olofsson B, Michelson EL, Granger CB, Swedberg K, Pfeffer MA, Yusuf S, McMurray JJ, CHARM Investigators and Committees . Albuminuria in chronic heart failure: prevalence and prognostic importance. Lancet 2009; 374: 543–550. [DOI] [PubMed] [Google Scholar]
- 97. Koyama S, Sato Y, Tanada Y, Fujiwara H, Takatsu Y. Early evolution and correlates of urine albumin excretion in patients presenting with acutely decompensated heart failure. Circ Heart Fail 2013; 6: 227–232. [DOI] [PubMed] [Google Scholar]
- 98. Navaneethan SD, Roy J, Tao K, Brecklin CS, Chen J, Deo R, Flack JM, Ojo AO, Plappert TJ, Raj DS, Saydain G, Sondheimer JH, Sood R, Steigerwalt SP, Townsend RR, Dweik RA, Rahman M, Chronic Renal Insufficiency Cohort Investigators . Prevalence, predictors, and outcomes of pulmonary hypertension in CKD. J Am Soc Nephrol 2016; 27: 877–886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Garimella PS, Lee AK, Ambrosius WT, Bhatt U, Cheung AK, Chonchol M, Craven T, Hawfield AT, Jotwani V, Killeen A, Punzi H, Sarnak MJ, Wall BM, Ix JH, Shlipak MG. Markers of kidney tubule function and risk of cardiovascular disease events and mortality in the SPRINT trial. Eur Heart J 2019; 40: 3486–3493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Jotwani V, Katz R, Ix JH, Gutierrez OM, Bennett M, Parikh CR, Cummings SR, Sarnak MJ, Shlipak MG. Urinary biomarkers of kidney tubular damage and risk of cardiovascular disease and mortality in elders. Am J Kidney Dis 2018; 72: 205–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Cops J, Mullens W, Verbrugge FH, Swennen Q, Reynders C, Penders J, Rigo JM, Hansen D. Selective abdominal venous congestion to investigate cardiorenal interactions in a rat model. PLoS ONE 2018; 13: e0197687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Owji SM, Nikeghbal E, Moosavi SM. Comparison of ischaemia–reperfusion‐induced acute kidney injury by clamping renal arteries, veins or pedicles in anaesthetized rats. Exp Physiol 2018; 103: 1390–1402. [DOI] [PubMed] [Google Scholar]
- 103. Faustinella F, Uzoh C, Sheikh‐Hamad D, Truong LD, Olivero JJ. Glomerulomegaly and proteinuria in a patient with idiopathic pulmonary hypertension. J Am Soc Nephrol 1997; 8: 1966–1970. [DOI] [PubMed] [Google Scholar]
- 104. Sato M, Muragaki Y, Saika S, Roberts AB, Ooshima A. Targeted disruption of TGF‐beta1/Smad3 signaling protects against renal tubulointerstitial fibrosis induced by unilateral ureteral obstruction. J Clin Invest 2003; 112: 1486–1494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Chang Y, Qi X, Li Z, Wang F, Wang S, Zhang Z, Xiao C, Ding T, Yang C. Hepatorenal syndrome: insights into the mechanisms of intra‐abdominal hypertension. Int J Clin Exp Pathol 2013; 6: 2523–2528. [PMC free article] [PubMed] [Google Scholar]
- 106. Chevalier RL, Forbes MS, Thornhill BA. Ureteral obstruction as a model of renal interstitial fibrosis and obstructive nephropathy. Kidney Int 2009; 75: 1145–1152. [DOI] [PubMed] [Google Scholar]
- 107. Gilbert RE, Connelly K, Kelly DJ, Pollock CA, Krum H. Heart failure and nephropathy: catastrophic and interrelated complications of diabetes. Clin J Am Soc Nephrol 2006; 1: 193–208. [DOI] [PubMed] [Google Scholar]
- 108. Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, Lerma EV, Mezue K, Molitch M, Mullens W, Ronco C, Tang WHW, McCullough PA, American Heart Association Council on the Kidney in Cardiovascular Disease , Council on Clinical Cardiology . Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation 2019; 139: e840–e878. [DOI] [PubMed] [Google Scholar]
- 109. Kihm LP, Hankel V, Zugck C, Remppis A, Schwenger V. Recompensation of heart and kidney function after treatment with peritoneal dialysis in a case of congestive heart failure. Case Rep Med 2011; 2011: 197816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Webb DJ, Vachiery JL, Hwang LJ, Maurey JO. Sildenafil improves renal function in patients with pulmonary arterial hypertension. Br J Clin Pharmacol 2015; 80: 235–241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Sandner SE, Zimpfer D, Zrunek P, Rajek A, Schima H, Dunkler D, Grimm M, Wolner E, Wieselthaler GM. Renal function and outcome after continuous flow left ventricular assist device implantation. Ann Thorac Surg 2009; 87: 1072–1078. [DOI] [PubMed] [Google Scholar]
- 112. Butler J, Geisberg C, Howser R, Portner PM, Rogers JG, Deng MC, Pierson RN 3rd. Relationship between renal function and left ventricular assist device use. Ann Thorac Surg 2006; 81: 1745–1751. [DOI] [PubMed] [Google Scholar]
- 113. Singh M, Shullo M, Kormos RL, Lockard K, Zomak R, Simon MA, Bermudez C, Bhama J, McNamara D, Toyoda Y, Teuteberg JJ. Impact of renal function before mechanical circulatory support on posttransplant renal outcomes. Ann Thorac Surg 2011; 91: 1348–1354. [DOI] [PubMed] [Google Scholar]
- 114. Felker GM, Rogers JG. Same bridge, new destinations rethinking paradigms for mechanical cardiac support in heart failure. J Am Coll Cardiol 2006; 47: 930–932. [DOI] [PubMed] [Google Scholar]
- 115. Zimpfer D, Wieselthaler G, Czerny M, Fakin R, Haider D, Zrunek P, Roethy W, Schima H, Wolner E, Grimm M. Neurocognitive function in patients with ventricular assist devices: a comparison of pulsatile and continuous blood flow devices. ASAIO J 2006; 52: 24–27. [DOI] [PubMed] [Google Scholar]
- 116. Iwashima Y, Yanase M, Horio T, Seguchi O, Murata Y, Fujita T, Toda K, Kawano Y, Nakatani T. Effect of pulsatile left ventricular assist system implantation on Doppler measurements of renal hemodynamics in patients with advanced heart failure. Artif Organs 2012; 36: 353–358. [DOI] [PubMed] [Google Scholar]
- 117. Husain‐Syed F, Mucino‐Bermejo MJ, Ronco C, Seeger W, Birk HW. Peritoneal ultrafiltration for refractory fluid overload and ascites due to pulmonary arterial hypertension. Ann Hepatol 2015; 14: 929–932. [DOI] [PubMed] [Google Scholar]
- 118. Umgelter A, Reindl W, Franzen M, Lenhardt C, Huber W, Schmid RM. Renal resistive index and renal function before and after paracentesis in patients with hepatorenal syndrome and tense ascites. Intensive Care Med 2009; 35: 152–156. [DOI] [PubMed] [Google Scholar]
- 119. Lu R, Mucino‐Bermejo MJ, Ribeiro LC, Tonini E, Estremadoyro C, Samoni S, Sharma A, Zaragoza Galvan Jde J, Crepaldi C, Brendolan A, Ni Z, Rosner MH, Ronco C. Peritoneal dialysis in patients with refractory congestive heart failure: a systematic review. Cardiorenal Med 2015; 5: 145–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. Durand PY, Chanliau J, Gamberoni J, Hestin D, Kessler M. Measurement of hydrostatic intraperitoneal pressure: a necessary routine test in peritoneal dialysis. Perit Dial Int 1996; 16: S84–S87. [PubMed] [Google Scholar]
- 121. Dejardin A, Robert A, Goffin E. Intraperitoneal pressure in PD patients: relationship to intraperitoneal volume, body size and PD‐related complications. Nephrol Dial Transplant 2007; 22: 1437–1444. [DOI] [PubMed] [Google Scholar]
- 122. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. [DOI] [PubMed] [Google Scholar]
- 123. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010; 23: 685–713 quiz 786‐8. [DOI] [PubMed] [Google Scholar]
- 124. Kosmala W, Przewlocka‐Kosmala M, Rojek A, Mysiak A, Dabrowski A, Marwick TH. Association of abnormal left ventricular functional reserve with outcome in heart failure with preserved ejection fraction. JACC Cardiovasc Imaging 2018; 11: 1737–1746. [DOI] [PubMed] [Google Scholar]
- 125. Kusunose K, Yamada H, Nishio S, Ishii A, Hirata Y, Seno H, Saijo Y, Ise T, Yamaguchi K, Yagi S, Soeki T, Wakatsuki T, Sata M. RV myocardial strain during pre‐load augmentation is associated with exercise capacity in patients with chronic HF. JACC Cardiovasc Imaging 2017; 10: 1240–1249. [DOI] [PubMed] [Google Scholar]
- 126. Tello K, Axmann J, Ghofrani HA, Naeije R, Narcin N, Rieth A, Seeger W, Gall H, Richter MJ. Relevance of the TAPSE/PASP ratio in pulmonary arterial hypertension. Int J Cardiol 2018; 266: 229–235. [DOI] [PubMed] [Google Scholar]
- 127. Guazzi M, Dixon D, Labate V, Beussink‐Nelson L, Bandera F, Cuttica MJ, Shah SJ. RV contractile function and its coupling to pulmonary circulation in heart failure with preserved ejection fraction: stratification of clinical phenotypes and outcomes. JACC Cardiovasc Imaging 2017; 10: 1211–1221. [DOI] [PubMed] [Google Scholar]
- 128. Bateman GA, Cuganesan R. Renal vein Doppler sonography of obstructive uropathy. AJR Am J Roentgenol 2002; 178: 921–925. [DOI] [PubMed] [Google Scholar]
- 129. Kashani KB, Mao SA, Safadi S, Amiot BP, Glorioso JM, Lieske JC, Nyberg SL, Zhang X. Association between kidney intracapsular pressure and ultrasound elastography. Crit Care 2017; 21: 251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Taniguchi T, Ohtani T, Kioka H, Tsukamoto Y, Onishi T, Nakamoto K, Katsimichas T, Sengoku K, Chimura M, Hashimoto H, Yamaguchi O, Sawa Y, Sakata Y. Liver stiffness reflecting right‐sided filling pressure can predict adverse outcomes in patients with heart failure. JACC Cardiovasc Imaging 2019; 12: 955–964. [DOI] [PubMed] [Google Scholar]
- 131. Kraemer M, Rode C, Wizemann V. Detection limit of methods to assess fluid status changes in dialysis patients. Kidney Int 2006; 69: 1609–1620. [DOI] [PubMed] [Google Scholar]
- 132. Nunez J, Minana G, Nunez E, Chorro FJ, Bodi V, Sanchis J. Clinical utility of antigen carbohydrate 125 in heart failure. Heart Fail Rev 2014; 19: 575–584. [DOI] [PubMed] [Google Scholar]
- 133. Nunez J, Sanchis J, Bodi V, Fonarow GC, Nunez E, Bertomeu‐Gonzalez V, Minana G, Consuegra L, Bosch MJ, Carratala A, Chorro FJ, Llacer A. Improvement in risk stratification with the combination of the tumour marker antigen carbohydrate 125 and brain natriuretic peptide in patients with acute heart failure. Eur Heart J 2010; 31: 1752–1763. [DOI] [PubMed] [Google Scholar]
- 134. D'Aloia A, Faggiano P, Aurigemma G, Bontempi L, Ruggeri G, Metra M, Nodari S, Dei Cas L. Serum levels of carbohydrate antigen 125 in patients with chronic heart failure: relation to clinical severity, hemodynamic and Doppler echocardiographic abnormalities, and short‐term prognosis. J Am Coll Cardiol 2003; 41: 1805–1811. [DOI] [PubMed] [Google Scholar]
- 135. Nunez J, Llacer P, Bertomeu‐Gonzalez V, Bosch MJ, Merlos P, Garcia‐Blas S, Montagud V, Bodi V, Bertomeu‐Martinez V, Pedrosa V, Mendizabal A, Cordero A, Gallego J, Palau P, Minana G, Santas E, Morell S, Llacer A, Chorro FJ, Sanchis J, Facila L, Investigators C‐H. Carbohydrate antigen‐125‐guided therapy in acute heart failure: CHANCE‐HF: a randomized study. JACC Heart Fail 2016; 4: 833–843. [DOI] [PubMed] [Google Scholar]
- 136. Ronco C, Kaushik M, Valle R, Aspromonte N, Peacock WF 4th. Diagnosis and management of fluid overload in heart failure and cardio‐renal syndrome: the “5B” approach. Semin Nephrol 2012; 32: 129–141. [DOI] [PubMed] [Google Scholar]
- 137. Genot N, Mewton N, Bresson D, Zouaghi O, Francois L, Delwarde B, Kirkorian G, Bonnefoy‐Cudraz E. Bioelectrical impedance analysis for heart failure diagnosis in the ED. Am J Emerg Med 2015; 33: 1025–1029. [DOI] [PubMed] [Google Scholar]
- 138. Massari F, Scicchitano P, Ciccone MM, Caldarola P, Aspromonte N, Iacoviello M, Barro S, Pantano I, Valle R. Bioimpedance vector analysis predicts hospital length of stay in acute heart failure. Nutrition 2019; 61: 56–60. [DOI] [PubMed] [Google Scholar]
- 139. Santarelli S, Russo V, Lalle I, De Berardinis B, Vetrone F, Magrini L, Di Stasio E, Piccoli A, Codognotto M, Mion MM, Castello LM, Avanzi GC, Di Somma S, network G . Prognostic value of decreased peripheral congestion detected by bioelectrical impedance vector analysis (BIVA) in patients hospitalized for acute heart failure: BIVA prognostic value in acute heart failure. Eur Heart J Acute Cardiovasc Care 2017; 6: 339–347. [DOI] [PubMed] [Google Scholar]
- 140. Smeets CJP, Lee S, Groenendaal W, Squillace G, Vranken J, De Canniere H, Van Hoof C, Grieten L, Mullens W, Nijst P, Vandervoort PM. The added value of in‐hospital tracking of the efficacy of decongestion therapy and prognostic value of a wearable thoracic impedance sensor in acutely decompensated heart failure with volume overload: prospective cohort study. JMIR Cardio 2020; 4: e12141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Kervella D, Lemoine S, Sens F, Dubourg L, Sebbag L, Guebre‐Egziabher F, Bonnefoy E, Juillard L. Cystatin C versus creatinine for GFR estimation in CKD due to heart failure. Am J Kidney Dis 2017; 69: 321–323. [DOI] [PubMed] [Google Scholar]
- 142. Beldhuis IE, Streng KW, van der Meer P, Ter Maaten JM, O'Connor CM, Metra M, Dittrich HC, Ponikowski P, Cotter G, Cleland JGF, Davison BA, Givertz MM, Teerlink JR, Bloomfield DM, Voors AA, Damman K. Trajectories of changes in renal function in patients with acute heart failure. J Card Fail 2019; 25: 866–874. [DOI] [PubMed] [Google Scholar]
- 143. Testani JM, Cappola TP, Brensinger CM, Shannon RP, Kimmel SE. Interaction between loop diuretic‐associated mortality and blood urea nitrogen concentration in chronic heart failure. J Am Coll Cardiol 2011; 58: 375–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Rao VS, Planavsky N, Hanberg JS, Ahmad T, Brisco‐Bacik MA, Wilson FP, Jacoby D, Chen M, Tang WHW, Cherney DZI, Ellison DH, Testani JM. Compensatory distal reabsorption drives diuretic resistance in human heart failure. J Am Soc Nephrol 2017; 28: 3414–3424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Ahmad T, Jackson K, Rao VS, Tang WHW, Brisco‐Bacik MA, Chen HH, Felker GM, Hernandez AF, O'Connor CM, Sabbisetti VS, Bonventre JV, Wilson FP, Coca SG, Testani JM. Worsening renal function in patients with acute heart failure undergoing aggressive diuresis is not associated with tubular injury. Circulation 2018; 137: 2016–2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Ghorbani A, Bhambhani V, Christenson RH, Meijers WC, de Boer RA, Levy D, Larson MG, Ho JE. Longitudinal change in galectin‐3 and incident cardiovascular outcomes. J Am Coll Cardiol 2018; 72: 3246–3254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Alam ML, Katz R, Bellovich KA, Bhat ZY, Brosius FC, de Boer IH, Gadegbeku CA, Gipson DS, Hawkins JJ, Himmelfarb J, Kestenbaum BR, Kretzler M, Robinson‐Cohen C, Steigerwalt SP, Tuegel C, Bansal N. Soluble ST2 and galectin‐3 and progression of CKD. Kidney Int Rep 2019; 4: 103–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148. Threefoot SA, Cabrera‐Gil C, Pearson JE Jr. Collateral circulation, renal function and histology after experimental obstruction of renal veins. Chest 1970; 58: 249–260. [DOI] [PubMed] [Google Scholar]
- 149. Robinson LS. The collateral circulation following ligation of the inferior vena cava; injection studies in stillborn infants. Surgery 1949; 25: 329–347. [PubMed] [Google Scholar]
- 150. Abraham WT, Stevenson LW, Bourge RC, Lindenfeld JA, Bauman JG, Adamson PB, Group CTS . Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow‐up results from the CHAMPION randomised trial. Lancet 2016; 387: 453–461. [DOI] [PubMed] [Google Scholar]
- 151. Prajczer S, Heidenreich U, Pfaller W, Kotanko P, Lhotta K, Jennings P. Evidence for a role of uromodulin in chronic kidney disease progression. Nephrol Dial Transplant 2010; 25: 1896–1903. [DOI] [PubMed] [Google Scholar]