

Abstract
To study the effect of continuous irrigation of rotating nickel-titanium instrument with several common clinical fluids on the diameter, breaking length and breaking position of nickel-titanium instrument, so as to provide some reference and theoretical basis for clinical operation and instrument improvement.
A standardized curved root canal model was established, and ProTaper Universal (PTU) F1 instrument was selected for root canal preparation. The nickel-titanium F1 instrument was flushed with distilled water, 0.9% NaCl, 0.2% chlorhexidine, 1% sodium hypochlorite and 5% sodium hypochlorite, and the diameter, length and position of the instrument before and after breakage were recorded.
Only 5% sodium hypochlorite influenced the diameter of 6 mm marker points under different irrigation conditions (P < .05). There was no statistical difference in the length of broken instruments among all the groups, and torsional deformation mainly occurred at the end of broken instruments. The broken positions of instruments in all the groups were located at the bending segment of the root canal. The breaking frequency of the 5% sodium hypochlorite group was the highest in the area 3–5.5 mm away from apical foramen, while the other 4 groups had the highest breaking frequency in the area 0 to 1.5 mm away from apical foramen.
External irrigation with different fluids did not influence the breaking length of instruments. The closer to the apical foramen was, the higher the breaking frequency of instruments was. However, only 5% sodium hypochlorite can affect the diameter of rotary nickel-titanium instruments, and may lead to early breakage of the instrument, indicating that the use of disinfectants, except 5% sodium hypochlorite, cannot reduce breakage resistance of nickel-titanium instrument compared with distilled water flushing. Furthermore, 5% hypochlorite could not be recommended for irrigation in clinical practice.
Keywords: break, continuous irrigation, nickel-titanium file, root canal preparation
1. Introduction
Because of the complexity of the root canal system, the fracture of instrument needle in root canal preparation and therapy is considered one of the most common challenging complications.[1,2] Recently, there are no steps of flushing with liquid while preparing root canals with rotating nickel-titanium instruments. Fluid is useful for root canal therapy due to its characteristics of lubrication, cooling and removal of debris. Therefore, we hypothesized that the introduction of liquid in advance during root canal preparation could improve fatigue resistance and prolong the service life of nickel-titanium rotary instrument, which has been proved in previous experiments.[3,4] However, different disinfectants may also have different effects on the preparation of nickel-titanium rotary instruments.
At present, surface grooves or cracks of rotating nickel-titanium instruments were observed and noted by scanning electron microscopy, and wear was explained qualitatively based on the degree of defect. However, there are few studies on whether the diameter of different parts of nickel-titanium instruments can be changed after using a certain number of times. If the diameter of different parts of rotating nickel-titanium instruments decreases with wear, the prepared root canal taper will also be smaller. Subsequently, the corresponding tapered gum tip may not reach the physiological apical foramen and could be locked in the upper end of the root canal wall in advance, thus affecting the effect of root canal filling. When this happens in the clinic, clinicians will be very troubled and confused. The purpose of this study was to investigate whether different liquids flushing nickel-titanium rotary instrument could affect the diameter of different sites before and after the breakage of rotary nickel-titanium instruments, to further analyze the breaking length and the breaking location of instruments in standardized root canals, and to explore the morphological changes of the broken ends of instruments, so as to provide some reference and theoretical basis for clinical operation and device modification.
2. Materials and methods
2.1. Materials and instruments
Protaper Universial F1 instrument (Dentsply, Switzerland), X smart plus machine nickel-titanium motor equipment (Dentsply, USA), electron microscope (Optical Instrument World, China), SK2610B Precision parts measurement system (Sack Digital, China, 0.001 mm), resin transparent root canal model (Hebei Hanru Crafts Co., Ltd., China), Aohua Laser AHL-FB50 (Shenzhen Aohua Laser Co., Ltd., China), Pointer push-pull force meter and fixture (Nanjing Su Metrology Instrument Co., Ltd., China), 360° universal sucker table pliers (G-CRAFT Company, China), and dental punch (Beijing Meide Innovation Technology Co., Ltd., China), etc. Since animal experiment or human was not involved in this study, the ethical approval was not necessary.
2.2. Exclusion criteria
The surface of the nickel-titanium instrument was observed under an electron microscope, and the pictures were archived. If the following defects appeardc on the surface, they were eliminated:
-
(1)
different degrees of cracks;
-
(2)
pitted structures;
-
(3)
partial protrusions or scratches on the surface of the instrument;
2.3. Experimental group
According to the literature, the sample size of studies similar to our experiment was between 15 and 20 .[5,6] Thus, the sample size of nickel-titanium instrument in each test group was set at 20. Additionally, according to the different flushing fluids, our experimental group was divided into the following five groups:
-
(1)
Distilled water (the control group);
-
(2)
0.9% NaCl;
-
(3)
0.2% chlorhexidine;
-
(4)
1% sodium hypochlorite;
-
(5)
5% sodium hypochlorite.
2.4. Methods
2.4.1. Laser labeling of specific sites of PTU F1
Twenty PTU F1 pins in each group were fixed on the silicone rubber template in accordance with numbered sequence, which ensured that the tips of PTU F1 pins were leveled with each other (Fig. 1). After the laser marking program was started, the fiber laser mode was selected. Six laser marking lines were set up at a 3-mm interval and a 0.1-mm line width, and marking parameters were set to speed: 200 mm/s, power: 30%, and frequency: 500 KHz. The laser indicator was opened and made to level with the tips of PTU F1 (Fig. 1A). Before laser marking, the first and second laser lines (blue solid lines) were not selected in the program, but other laser markers (red dotted lines) were selected to work, which enabled accurate and uniform laser marking at 6 mm, 9 mm, 12 mm, and 15 mm (Fig. 1B).
Figure 1.
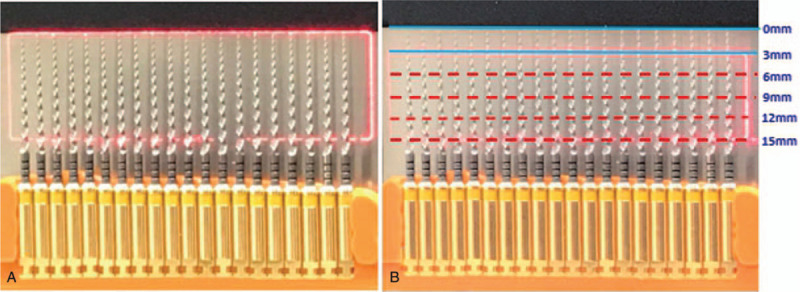
The method of laser marking.
2.4.2. Root canal preparation
The PTU F1 was removed from the silicone rubber template according to the numbered sequence to carry out root canal preparation experiment at room temperature. The stop ring was placed at 18 mm, and the motor of X-Smart plus was set at 350 rpm/min with a torque of 3 Ncm. The rotation was clockwise and unidirectional. The vertical pressure of each preparation to the root canal side was kept at 10 N, so that the filing needle could stay for 2 seconds in the root canal each time. At the same time, the flusher was used, and the needle was continuously flushed outside the root canal at about 1 cm perpendicular to the needle. The liquid flow rate was set to 220 ml/min, so that the working length of the root canal can be prepared repeatedly to 18 mm. In this experiment, only the control group did not undergo extra-canal irrigation for root canal preparation. However, none of the five groups changed the existing clinical irrigation methods (five times after nickel-titanium instruments entered the root canal, and the root canal was dredged with No. 10 enlarged needle and irrigated with lateral opening needle). Each root canal was prepared by the above methods until the needle was broken and a new needle was replaced, and the above operations were repeated (Fig. 2).
Figure 2.
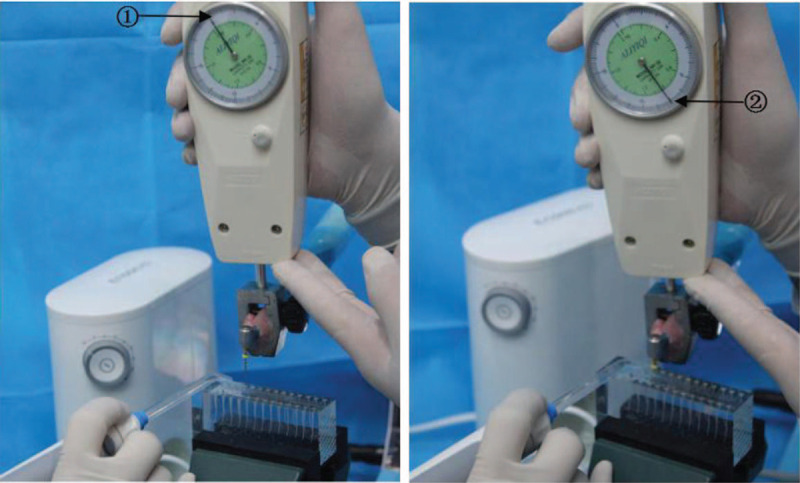
Method of root canal preparation. Note: (1) refers to 0N when no force is applied, (2) refers to 10N when pressing down.
2.5. Detection parameters
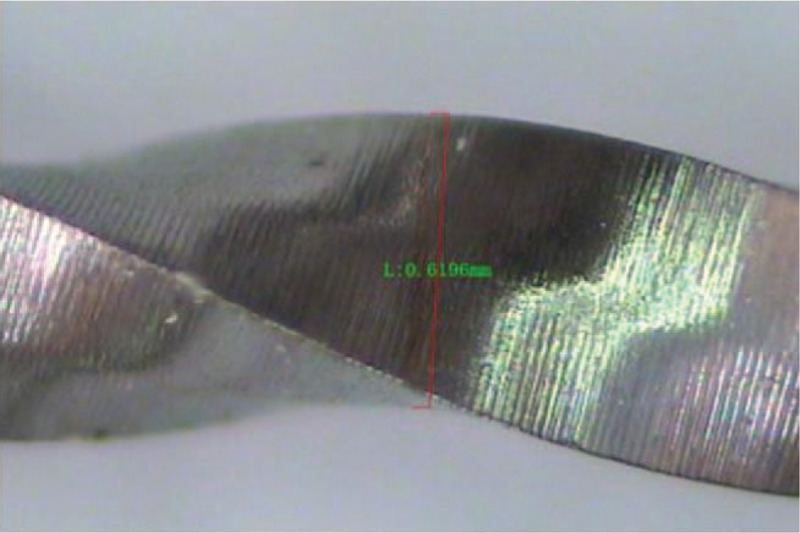
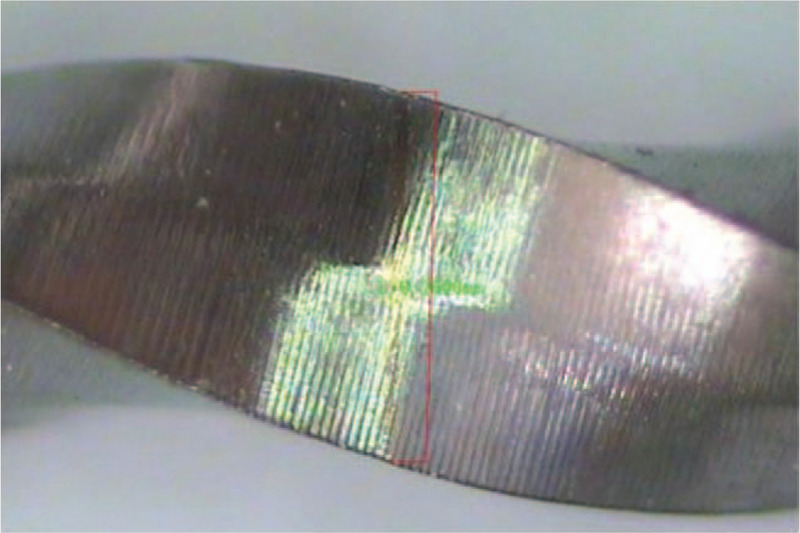
Before root canal preparation, the original diameter of each PTU F1 laser marker site was measured and recorded on the silicone rubber template using electron microscopy. After breakage, the broken PTU F1 was restored to the silicone rubber template in accordance with its numbered sequence, and its diameter of different laser marker sites of PTU F1 was measured and recorded again (Figs. 3–6).
Figure 3.
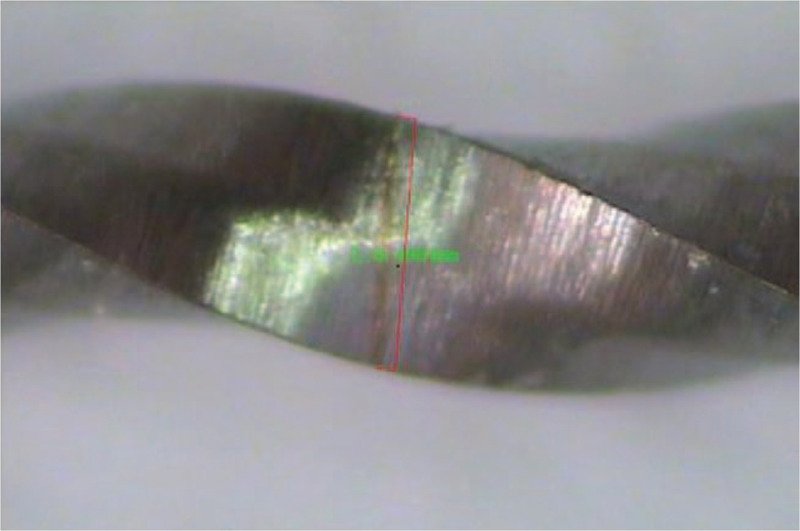
Measurement at the 6-mm laser marker site.
Figure 6.
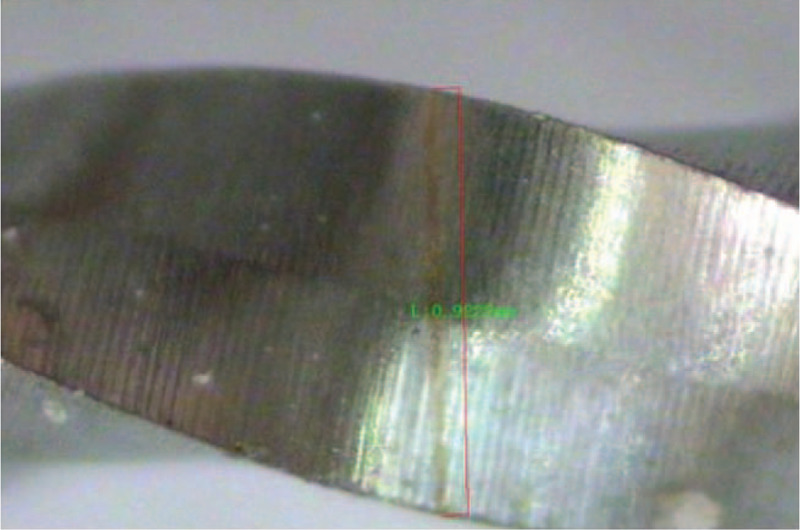
Measurement at the 15-mm laser marker site.
Figure 4.
Measurement at the 9-mm laser marker site.
Figure 5.
Measurement at the 12-mm laser marker site.
The breaking location of PTU F1 in root canal was recorded (Fig. 7). The formula for calculating the breaking length of PTU F1 was as follows:
Figure 7.
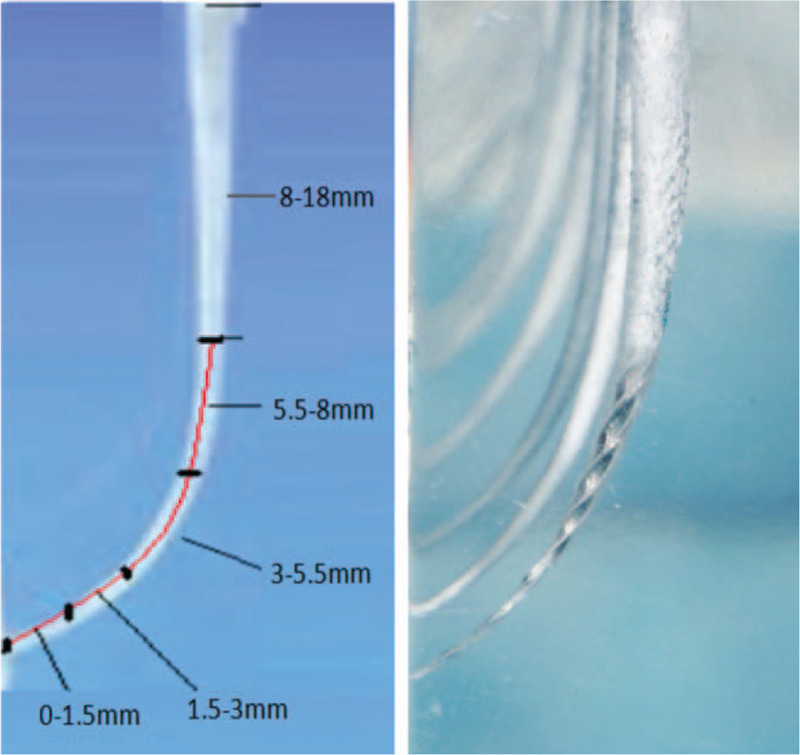
Distribution of location of broken PTU F1 in area away from the apical foramen. Note: “0 to 1.5 mm” refers to the broken PTU F1 located at area 0 to 1.5 mm from the apical foramen of the module, which is equivalent to 80% to 100% of complete root canal preparation. By inference, “1.5 to 3 mm” is equivalent to 60% to 80% of the complete root canal preparation, “3 to 5.5 mm” is equivalent to 40% to 60% of complete root canal preparation, “5.5 to 8 mm” is equivalent to 20% to 40% of complete root canal preparation, “8 to 10 mm” is equivalent to 0% to 20% of complete root canal preparation, respectively.
Breaking length = Original length of needle − Remaining length after breaking.
2.6. Statistical analysis
SPSS 21.0 was used for statistical analysis. The diameter of specific sites and breaking length were described as mean±SD. Kolmogorov-Smimov test showed that the data were normally distributed, and the homogeneity of variance test was performed. The paired t test of diameters of instruments before and after the breaking of specific sites was performed, and the variance of breaking length of nickel-titanium instruments under five different irrigation conditions was analyzed. P < .05 was considered statistically significant.
3. Results
3.1. Different liquids did not change the diameter before and after breakage except 5% sodium hypochlorite group.
Root canal preparation was performed under different liquid conditions. At the 6-mm laser marking site, the 5% sodium hypochlorite group showed statistical difference in diameter change before and after breakage, while there was no significant change in diameter before and after breakage in the other four groups (Table 1). In addition, there was no significant change in the diameter of the 5 groups before and after breakage at the 9 mm, 12 mm and 15 mm laser marking sites (Tables 2–4).
Table 1.
Diameter Change of instrument before and after breakage at the laser marking site of 6 mm.
| Groups | n | Diameter before breakage (mm) | Diameter after breakage (mm) | P value |
| Distilled water (control group) | 20 | 0.5075 ± 0.0117 | 0.5022 ± 0.0138 | >.05 |
| 0.9% NaCl | 20 | 0.4936 ± 0.0082 | 0.4947 ± 0.0115 | >.05 |
| 0.2% chlorhexidine | 20 | 0.4825 ± 0.0103 | 0.4899 ± 0.0141 | >.05 |
| 1% sodium hypochlorite | 20 | 0.4958 ± 0.0107 | 0.4920 ± 0.0134 | >.05 |
| 5% sodium hypochlorite | 20 | 0.4831 ± 0.0137 | 0.4935 ± 0.0145 | <.01 |
Table 2.
Diameter Change of instrument before and after breakage at the laser marking site of 9 mm.
| Groups | n | Diameter before breakage (mm) | Diameter after breakage (mm) | P value |
| Distilled water (control group) | 20 | 0.6517 ± 0.0146 | 0.6477 ± 0.0143 | >.05 |
| 0.9% NaCl | 20 | 0.6336 ± 0.0167 | 0.6356 ± 0.0147 | >.05 |
| 0.2% chlorhexidine | 20 | 0.6244 ± 0.0179 | 0.6287 ± 0.0157 | >.05 |
| 1% sodium hypochlorite | 20 | 0.6314 ± 0.0157 | 0.6353 ± 0.0140 | >.05 |
| 5% sodium hypochlorite | 20 | 0.6337 ± 0.0167 | 0.6234 ± 0.0156 | >.05 |
Table 4.
Diameter Change of instrument before and after breakage at the laser marking site of 15 mm.
| Groups | n | Diameter before breakage (mm) | Diameter after breakage (mm) | P value |
| Distilled water (control group) | 20 | 0.9124 ± 0.0206 | 0.9129 ± 0.0149 | >.05 |
| 0.9% NaCl | 20 | 0.9209 ± 0.0128 | 0.9194 ± 0.0193 | >.05 |
| 0.2% chlorhexidine | 20 | 0.9138 ± 0.0208 | 0.9122 ± 0.0248 | >.05 |
| 1% sodium hypochlorite | 20 | 0.9129 ± 0.0244 | 0.9120 ± 0.0233 | >.05 |
| 5% sodium hypochlorite | 20 | 0.9006 ± 0.0262 | 0.9045 ± 0.0217 | >.05 |
Table 3.
Diameter Change of instrument before and after breakage at the laser marking site of 12 mm.
| Groups | n | Diameter before breakage (mm) | Diameter after breakage (mm) | P value |
| Distilled water (control group) | 20 | 0.7564 ± 0.0174 | 0.7545 ± 0.0211 | >.05 |
| 0.9% NaCl | 20 | 0.7560 ± 0.0200 | 0.7603 ± 0.0193 | >.05 |
| 0.2% chlorhexidine | 20 | 0.7568 ± 0.0153 | 0.7559 ± 0.0161 | >.05 |
| 1% sodium hypochlorite | 20 | 0.7523 ± 0.0141 | 0.7494 ± 0.0180 | >.05 |
| 5% sodium hypochlorite | 20 | 0.7544 ± 0.0181 | 0.7498 ± 0.0171 | >.05 |
3.2. Different liquids had no effect on breaking length.
In the experiment, the breaking length of instrument needle ranged from 2.4853 mm to 2.7644 mm (95% confidence interval). The breaking lengths of the five preparatory methods were 2.5358 ± 0.4157 mm in the distilled water group, 2.5052 ± 0.5905 mm in the 0.9% NaCl group, 2.5908 ± 0.5494 mm in the 0.2% chlorhexidine group, 2.9040 ± 0.7286 mm in the 1% sodium hypochlorite group, and 2.5884 ± 1.0555 mm in the 5% sodium hypochlorite group. The results of variance analysis demonstrated that there was no statistical difference in the breaking length among the 5 groups (Table 5).
Table 5.
Breaking length of PTU F1 under different flushing conditions.
| Groups | n | Breaking length | P value |
| Distilled water (control group) | 20 | 2.5358 ± 0.4157 | >.05 |
| 0.9% NaCl | 20 | 2.5052 ± 0.5905 | >.05 |
| 0.2% chlorhexidine | 20 | 2.5908 ± 0.5494 | >.05 |
| 1% sodium hypochlorite | 20 | 2.9040 ± 0.7286 | >.05 |
| 5% sodium hypochlorite | 20 | 2.5884 ± 1.0555 | >.05 |
3.3. All breakage occurred in the curved segment and none in the straight path segment.
In this experiment, our results showed that no events of breakage of PTU F1 occurred in the straight path segment of the root canal model (area 8–18 mm from the apical foramen), while all the locations of broken PTU F1were distributed in the curved segment (area 0–8 mm from the apical foramen). Additionally, the frequency of breakage of the distilled water group, 1% sodium hypochlorite solution group, 0.2% chlorhexidine group and 0.9% NaCl group were the highest in the area 0 to 1.5 mm away from the apical foramen, followed by area 1.5 to 3 mm from the apical foramen. However, in the 5% sodium hypochlorite group, the breakage frequency was the highest in the area 3–5.5 mm, but no breakage occurred in the area 0 to 1.5m (Fig. 8).
Figure 8.
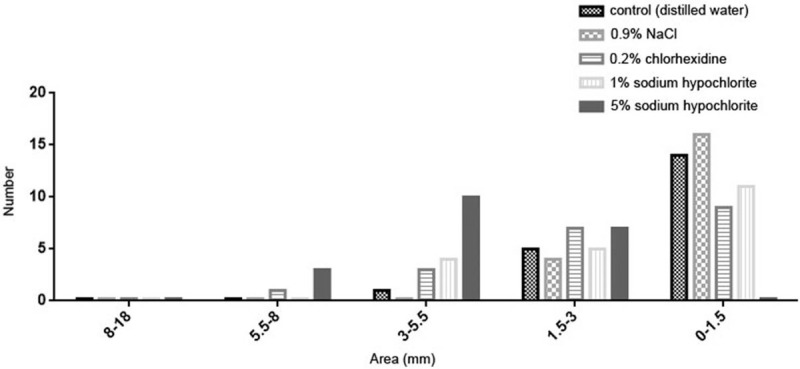
Frequency of regional distribution of broken PTU F1 in different groups.
4. Discussion
4.1. Marking method of nickel-titanium rotary instruments
Nowadays there is no relevant report on the method of marking the surface of nickel-titanium instruments. Maybe most scholars believe that no matter what the method is, the surface integrity of nickel-titanium rotary instruments will inevitably be destroyed, which may affect breaking resistance of the instruments. In order to quantitatively study the diameter changes of different sites before and after breakage of nickel-titanium rotary instruments, a reliable and non-destructive method is required to mark nickel-titanium rotary instruments accurately. Compared with traditional marking methods such as mechanical stamping, electrolithography and corrosion, the laser marking method generally has no special requirement for materials, and has the advantages of no damage to the workpiece, no disturbance, no deformation, high efficiency and low individual cost. In this experiment, fiber laser was selected and a suitable marking parameter was found through continuous exploration and adjustment. In our preliminary experiment, the accuracy of laser marking was verified, and the breaking resistance of the instrument was not affected.
4.2. Selection of root canal irrigation solution
There are some common solutions used in root canal irrigation, including sodium hypochlorite, chlorhexidine, EDTA, 0.9%NaCl, hydrogen peroxide, distilled water, etc. Sodium hypochlorite is a broad-spectrum antimicrobial reagent widely used in root canal therapy, which can dissolve the necrotic pulp tissue components, and can effectively remove the smear layer of root canal wall. 0.5% to 5.25% sodium hypochlorite solution is commonly used in clinic. With the increase of its concentration, the antimicrobial effect will increase, but the tissue toxicity and ability of corrosion will also increase at the same time.[7] However, there are different opinions on whether sodium hypochlorite will corrode nickel-titanium rotary instruments. It is suggested that the presence of sodium hypochlorite in root canal therapy may corrode rotating nickel-titanium instruments, thereby limiting fatigue resistance of instruments.[8] Nevertheless, Cavalleri et al believed sodium hypochlorite would not affect the structure of nickel-titanium rotary instruments through corrosion.[9] Secondly, 0.2% to 2%chlorhexidine is another commonly used irrigation solution for root canal therapy, which has strong broad-spectrum antimicrobial and bactericidal effect, but it possesses no ability to dissolve tissue and remove the smear layer and infectious debris from the root canal wall. In addition, 0.9% NaCl is another indispensable irrigation solution for root canal therapy, which is often used with other irrigation solutions to remove other disinfectants or residual debris in root canals. However, 0.9% NaCl has a certain conductivity, and the handle and body of nickel-titanium rotary instrument are made of different metals. Thus, galvanic battery reaction may occur during irrigation, which may lead to corrosion.
In summary, 1% and 5% sodium hypochlorite, 0.2% chlorhexidine and 0.9% NaCl were included in the experiment, and distilled water was selected as the control group. EDTA and hydrogen peroxide were not included in this experiment. The chemical and antimicrobial effects of hydrogen peroxide are relatively weak, and there will be bubbles in the process of irrigation, which may squeeze debris out of the apical foramen. At present, hydrogen peroxide is seldom used for root canal irrigation in the clinic, so hydrogen peroxide is excluded in this experiment. In addition, EDTA has remarkable effect in dredging curved or small calcified root canals, but still many controversies remain about the clinical application of EDTA. It is reported that root canal wall exposure to 17% EDTA for 10 minutes would affect dentin hardness and lead to a larger diameter of dentinal tubules.[10] Therefore, it is not recommended to excessively use EDTA in the clinic. Moreover, because of its ability to soften tooth tissue or affect the properties of module possibly, EDTA may interfere with fatigue resistance of nickel-titanium instruments. Thus, EDTA was not included in this experiment as a flushing solution.
4.3. The effect of different liquids on the diameter before and after breaking
In this experiment, there was no significant difference in diameter between different groups before and after breaking at the 9, 12, and 15-mm laser marking sites. However, at the 6-mm laser marking site, the diameter after breaking was statistically larger than that before breaking in the 5% sodium hypochlorite group. During root canal preparation, the 9, 12 and 15-mm laser marking sites were all in the straight path segment of the root canal model. The diameter of instrument is larger in this section, and instrument cannot undergo bending, which suffers less wear and deformation. No obvious deformation was found in the 9 to 15 mm section of each group of nickel-titanium needles by electron microscopy. We speculated that although different irrigation liquids may have a corrosive effect on the surface of the instrument, the edge of the instrument may become blunter after breaking, but it will not lead to a change in the diameter of the 9 to 15 mm section of instrument.
However, in the preparation of root canals, nickel-titanium rotary instruments mainly work in the bending section of our root canal model, which are subject to larger tensile and compressive stresses. The closer to the tip of the instrument is, the greater the tension and compression stress, and the more serious the deformation and wear of the instrument may be, causing that the diameter of the 3-mm laser marking site could not be measured again after the instrument was broken. Electron microscopy found that a small number of PTU F1 were deformed at the 6-mm laser marking site in different groups, and the frequency of deformation was especially higher in the 5% sodium hypochlorite group. 0.2% chlorhexidine and 0.9% NaCl had no tissue solubility, and 1% sodium hypochlorite had weak ability of corrosion. These liquids have no obvious corrosive effect on nickel-titanium rotary instruments and no influence on the diameter of the 3-mm laser marking site before and after breakage. Therefore, continuous external irrigation with these liquids during root canal preparation could not reduce breakage resistance of instruments. However, nickel-titanium instrument may be corroded in high concentration sodium hypochlorite solution, and the application of 5% sodium hypochlorite to flush PTU F1 during root canal preparation will reduce breakage resistance of the instrument.[3] Some scholars believed that 5% sodium hypochlorite may cause damage to the edge and flat surface of nickel-titanium rotary instruments, resulting in corrosion products such as nickel-titanium oxide and calcium carbonate, which accelerate wear and deformation of the edge of instruments.[11] When the instrument is deformed, it may lead to larger or smaller diameter, while wear will lead to smaller diameter. We assumed that the PTU F1 of the 5% sodium hypochlorite group had severe deformation and wear at the 6-mm laser marking site simultaneously, and the effect of deformation was greater than that of wear, so the diameter of PTU F1 became larger after breaking at the 6-mm marking site.
4.4. The effect on breaking length
In this experiment, the breaking length of instrument needle ranged from 2.4853 mm to 2.7644 mm (95% confidence interval), and the average breaking length was 2.6249 ± 0.7032 mm. The results of variance analysis showed no statistical difference in the breaking length among the five groups. Therefore, we speculated that there was no direct relationship between the breaking length of instrument and continuous irrigation with different fluids, which may be more affected by the curvature of the prepared root canal or the types of instruments, which is similar to Sattapan et al.[12] The breaking forms can be divided into fatigue breakage and over-torsion breakage.[12,13] The results of electron microscopy showed that more than 90% of the broken ends of F1 instruments were distorted. Cyclic fatigue has been considered to be the main reason for the breakage of nickel-titanium instrument, and the broken ends seldom undergo deformation.[11] However, previous studies have shown that metal root canals are usually used to measure the cyclic fatigue resistance of nickel-titanium rotary instruments.[14–17] We believe that there is no taper change in metal root canals, and there are significant differences between metal root canals and clinical teeth in root canal morphology, hardness and other physical properties. Moreover, when rotating nickel-titanium instruments in metal root canals, there will be no locking events due to greater friction, so the incidence of fatigue fracture in metal root canals is higher. However, the standardized transparent resin bending root canal module was used in this experiment. The root canal was smaller, the degree of bending was greater, and the hardness of the module was higher, which is in accordance with clinical reality. Therefore, excessive torsion is the main reason for the breakage of this experimental instrument.
4.5. Distribution of locations of broken PTU F1 in the root canal
In this study, all the locations of broken PTU F1were distributed in the curved segment (area 0–8 mm from the apical foramen) of the root canal model, but no events of breakage occurred in the straight path segment (area 8–18 mm from the apical foramen). The closer to the apical foramen was, the greater the frequency of breakage was. In the 5% sodium hypochlorite group, the breakage frequency was the highest in the area 3 to 5.5 mm away from the apical foramen, but no breakage occurred in the area 0 to 1.5 m. However, the frequency of breakage of the other four groups were the highest in the 0 to 1.5 mm area, followed by the 1.5 to 3 mm area. Our analysis suggests that it may be due to the corrosiveness of 5% sodium hypochlorite, which accelerated the breakage of PTU F1, and the instrument has already broken in the 1.5–8 mm area before reaching the 0 to 1.5 mm area. Therefore, in the 5% sodium hypochlorite group, with the increase of root canal preparation depth, the frequency of instrument needle breakage increased first in the 5.5 to 18 mm reach, and reached the maximum in the 3 to 5.5 mm area, while the frequency of instrument needle breakage decreased in the 0 to 3 mm area. It is recommended that root canal preparation should be more cautious as it approaches the apical foramen to prevent breakage of instruments.
5. Conclusion
To summarize, except 5% sodium hypochlorite, there was no significant effect on the diameter of the 6, 9, 12, and 15-mm laser marking sites when flushing with different liquids. The intense corrosion of high concentration of sodium hypochlorite may contribute to the effect of 5% sodium hypochlorite on the diameter of the 6-mm laser marking site. There was no difference in the breaking length of PTU F1 instruments under five different flushing conditions, and most of the broken ends were distorted. The position of broken instruments in the root canal is mainly located in the curved section of the root canal, and the closer to the apical foramen is, the more difficult it is to prepare, and the higher the rate of breakage is. The use of 5% sodium hypochlorite for continuous irrigation of instrument needles may lead to early breakage of instruments. These results indicated that the use of disinfectants, except 5% sodium hypochlorite, cannot reduce breakage resistance of nickel-titanium instrument compared with distilled water flushing. Besides, 5% hypochlorite could not be recommended for irrigation in further clinical practice.
Author contributions
Conceptualization: Changjian Li, Jing Wang.
Funding acquisition: Yanfeng Li.
Investigation: Le Liu, Xin Wang, Haiyun Liu, Jiaxin Bao.
Methodology: Changjian Li, Yanfeng Li, Xin Wang, Haiyun Liu, Jiaxin Bao.
Software: Changjian Li.
Writing – original draft: Changjian Li.
Writing – review & editing: Yanfeng Li, Jing Wang.
Footnotes
Abbreviation: PTU = ProTaper universal.
How to cite this article: Li C, Liu L, Li Y, Wang X, Liu H, Bao J, Wang J, Fan J. Preventing nickel-titanium rotary instrument from breakage by continuous irrigation with different fluids during root canal preparation. Medicine. 2021;100:3(e23865).
CL, LL, and YL contributed equally to this work.
This research was supported by Capital Clinical Application Research and Results Promotion Project (No. Z171100001017154), General Hospital Transformation Project (2017TM-030), General Hospital Clinical Research Supporting Fund (2018FC-304M-TSYS-05) and Capital's Funds for Health Improvement and Research (CFH2020-2-5021). The authors acknowledge Feixiang County Ruyi Arts & Crafts Co., Ltd. (Taiwan Enterprise Mainland Company) for cooperating with the simulation of curved root canal resin modules and Shanghai Yirui Dental Materials Co., Ltd. We also acknowledge Shenzhen Yujia Medical Devices Co., Ltd. for providing materials and device.
The authors declare no conflicts of interest.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Parashos P, Messer HH. Rotary NiTi instrument fracture and itsconsequences. J Endodont 2006;32:1031–43. [DOI] [PubMed] [Google Scholar]
- [2].Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endodont 2013;39:569–81. [DOI] [PubMed] [Google Scholar]
- [3].Li C, Li Y, Xia D, et al. The effect of the modified root canal preparation method with different liquid continuous flushing on the anti-fracture properties of mechanical nickel-titanium file. J Pract Stomatol 2018;34:260–4. [Google Scholar]
- [4].Xia D, Li Y, Chai G, et al. Establishment of a model of root canal preparation. Chin J Med Phys 2017;34:416–22. [Google Scholar]
- [5].Fu M, Zhang Z, Hou B. Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endodont 2011;37:619–22. [DOI] [PubMed] [Google Scholar]
- [6].Madarati AA, Qualtrough AJ, Watts DC. Vertical fracture resistance of roots after ultrasonic removal of fractured instruments[J]. Int Endodont J 2010;43:424–9. [DOI] [PubMed] [Google Scholar]
- [7].Zehnder M. Root canal irrigants. J Endodont 2006;32:389–98. [DOI] [PubMed] [Google Scholar]
- [8].Pedullà E, Grande NM, Plotino G, et al. Cyclic fatigue resistance of two reciprocating nickel-titanium instruments after immersion in sodium hypochlorite. Int Endodont J 2011;37:1139–42. [DOI] [PubMed] [Google Scholar]
- [9].Cavalleri G, Cantatore G, Costa A, et al. The corrosive effects of sodium hypochlorite on nickel-titanium endodontic instruments: assessment by digital scanning microscope. Miner Stomatol 2009;58:225–31. [PubMed] [Google Scholar]
- [10].Calt S, Serper A. Time-dependent effects of EDTA on dentin structures. J Endodont 2002;28:17–9. [DOI] [PubMed] [Google Scholar]
- [11].Berutti E, Angelini E, Rigolone M, et al. Influence of sodium hypochlorite on fracture properties and corrosion of ProTaper Rotary instruments. Int Endodont J 2006;39:693–9. [DOI] [PubMed] [Google Scholar]
- [12].Sattapan B, Nervo GJ, Palamara JE, et al. Defects in rotary nickel-titanium files after clinical use. J Endodont 2000;26:161–5. [DOI] [PubMed] [Google Scholar]
- [13].Shen Y, Cheung GS, Peng B, et al. Defects in nickel-titanium instruments after clinical use. Part 2: Fractographic analysis of fractured surface in a cohort study. J Endodont 2009;35:133–6. [DOI] [PubMed] [Google Scholar]
- [14].Topçuoğlu HS, Düzgün S, Akti A, et al. Laboratory comparison of cyclic fatigue resistance of WaveOne Gold, Reciproc and WaveOne files in a canal with a double curvature. Int Endodont J 2016;50:713–7. [DOI] [PubMed] [Google Scholar]
- [15].Chi CW, Li CC, Lin CP, et al. Cyclic fatigue behavior of nickel-titanium dental rotary files in clinical simulated root canals. J Formosan Med Assoc 2016;116:306–12. [DOI] [PubMed] [Google Scholar]
- [16].Elnaghy AM, Elsaka SE. Effect of sodium hypochlorite and saline on cyclic fatigue resistance of WaveOne Gold and Reciproc reciprocating instruments. Int Endodont J 2016;50:991–8. [DOI] [PubMed] [Google Scholar]
- [17].Kaval ME, Capar ID, Ertas H. Evaluation of the cyclic fatigue and torsional resistance of novel nickel-titanium rotary files with various alloy properties. J Endodont 2016;42:1840–3. [DOI] [PubMed] [Google Scholar]