

Abstract
Penile fracture is a well-recognized but uncommon urological emergency. It is a tear in the tunica albuginea with rupture of corpus cavernosum. It may be associated with injury to corpus spongiosum and urethra. Diagnosis is usually clinical and Urethral injury should be suspected in penile fracture, especially in those cases with urethral bleeding and bilateral cavernosal rupture. Penile fracture is most commonly caused by injury during sexual intercourse. It has also been described with masturbation, rolling over or falling onto the erect penis, and other scenarios. A cracking or popping sound followed by pain, rapid detumescence, discoloration and swelling of penile shaft and urethral bleeding are common presenting symptoms. Prompt surgical intervention with closure of tunica albuginea is the treatment of choice with satisfactory cosmetic and functional results. We report a case of fracture penis in a 25-year-old male who came to emergency department of our hospital.
Keywords: Fracture, masturbation, penis
Introduction
Penile fracture is a rare, yet likely underreported condition. It was first reported more than 1000 years ago.[1] Penile fracture is the disruption of tunica albuginea with rupture of corpus cavernosum. It typically occurs during vigorous sexual intercourse. A cracking sound followed by pain, rapid detumescence, and swelling of penile shaft are common presenting symptoms. Need for early diagnosis has been stressed, without waiting for specialized imaging studies.[2,3,4,5] Urethral injury should be suspected in penile fracture, especially in cases with urethral bleeding and bilateral cavernosal rupture. Treatment of choice is early surgical management. We report a case of young male aged 25 years.
Case Report
A 25-year-old man presented to our emergency department with history of pain, swelling and loss of tumescence with a cracking sound during masturbation. No history of difficulty while passing urine.
Physical examination revealed swollen penis. Left side of the shaft was tender to touch. Glans penis was not visible due to swelling of prepuce. Penis was in a flaccid state and deviated to right side. Foleys catheter was placed without any difficulty and clear urine drained. No evidence of peri-catheter bleeding. In view of above-mentioned findings, diagnosis of fracture penis was made which was later confirmed by USG penis. USG showed a 1.0-cm defect in left corpora cavernosum in mid shaft with heterogenous hematoma formation in the penile shaft, adjacent to the breech.
Patient was taken up for emergency hematoma evacuation and fracture repair. Circumferential sub-coronal incision given and penis degloved. Hematoma evacuated and a transverse tear, approximately 1.0 cm on tunica albuginea of left sided corpus cavernosum identified [Figure 1]. Closure of tunical defect was done with interrupted 3.0 vicryl suture. Hemostasis secured and skin closed using 3.0 rapid vicryl. Post-operative period was uneventful. Foleys catheter was removed on 3rd post-operative day. Patient was discharged on 4th post-operative day, in satisfactory condition with the advice to come for urology and psychiatric consultation, as an outpatient, after 1 week and to avoid sexual activity for 6 weeks. On routine follow up till 9 months, patient was voiding well with no erectile dysfunction, no pain or chordee on erection [Figure 2].
Figure 1.
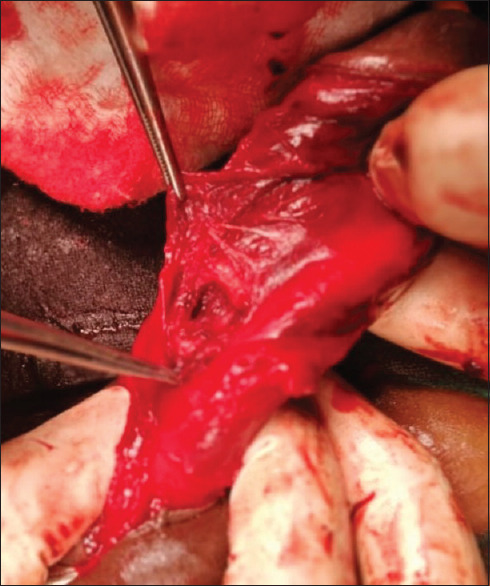
Intra-operative image
Figure 2.

Post-operative photograph
Discussion
Penile fracture is an uncommon urological emergency. The incidence is increasing however, it may still be under-reported due to associated guilt and embarrassment. Tunica albuginea is a bilaminar structure composed of collagen and elastin. The outer layer determines the strength and thickness of tunica. It varies in different locations along the shaft and is thinnest ventro-laterally.[6] It has remarkable tensile strength and can resist rupture until intra-cavernous pressure increases to more than 1500 mm Hg. The thickness of tunica albuginea decreases from 2 mm, in a flaccid penis to 0.25 mm, in erect penis and sudden increase in intracorporeal pressure due to trauma during an erection could easily result in rupture.[7] Although trauma during sexual intercourse has been considered as most common cause of penile fracture, it has also been described with masturbation, rolling over or falling onto the erect penis, and other scenarios.[8] Barros et al. (2017) reported that “doggy style” was more commonly associated with double fractures of penis.[9] Penile fracture has also been reported by straddle injury to non-erect Penis.[10] The typical history and clinical examination usually help us to diagnose this condition. However, in equivocal cases USG or MRI can establish the diagnosis. Most cases reported in literature describes imaging modalities being used to localize site of albuginea rupture and to exclude presence of a concomitant urethral injury.[11] Pre-operative urethrography or flexible cystoscopy should be considered when urethral injury is suspected. Prompt surgical intervention usually leads to satisfactory cosmetic and functional results.
Fracture of Penis is a rare urological emergency. These patients may first present to primary care physician to avoid delay in seeking medical attention. If primary care physician is not aware of this uncommon clinical entity, this may delay diagnosis and appropriate urological management which can increase complications of penile fracture. The diagnosis of penile fracture is usually clinical but imaging studies may help in equivocal cases. Early surgical treatment offers good outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
References
- 1.Eke N. Fracture of penis. BR J Surg. 2001;82:555–65. doi: 10.1046/j.1365-2168.2002.02075.x. [DOI] [PubMed] [Google Scholar]
- 2.Restrapo JA, Estrada CG, Garcia HA. Clinical experience in the management of penile fracture at Hospital Universitario del Valle. Arch Esp Urol. 2010;63:291–5. [PubMed] [Google Scholar]
- 3.Rosenstein D, McAninch JW. Urologic emergencies. Med Clin North Am. 2004;88:495–518. doi: 10.1016/S0025-7125(03)00190-1. [DOI] [PubMed] [Google Scholar]
- 4.Nomura JT, Sierzenski PR. Ultrasound diagnosis of penile fracture. J Emerg Med. 2010;38:362–5. doi: 10.1016/j.jemermed.2008.03.010. [DOI] [PubMed] [Google Scholar]
- 5.Taha KM. A typical presentation of penile fracture. Urol Nephrol Open Access J. 2020;8:42–4. [Google Scholar]
- 6.Hsu GL, Brock G, Martinez-Pineiro L, von Heyden B, Lue TF, Tanagho EA. Anatomy and strength of tunica albuginea: Its relevance to penile prosthesis extrusion. J Urol. 1994;151:1205–8. doi: 10.1016/s0022-5347(17)35214-x. [DOI] [PubMed] [Google Scholar]
- 7.Jack GS, Garraway I, Reznichek R, Raifer J. Current treatment options for penile fractures. Rev Urol. 2004;6:114–20. [PMC free article] [PubMed] [Google Scholar]
- 8.Al Ansari A, Talib RA, Shamsodini A, Hayati A, Canguven O, Al Naimi A, et al. Which is guilty in self-induced penile fractures: Marital status, culture or geographic region? A case series and literature review. Int J Impot Res. 2013;25:221–3. doi: 10.1038/ijir.2013.16. [DOI] [PubMed] [Google Scholar]
- 9.Barros R, Schulze L, Ornellas AA, Koifman L, Favorito LA. Relationship between sexual position and severity of penile fracture. Int J impot Res. 2017;29:207–9. doi: 10.1038/ijir.2017.24. [DOI] [PubMed] [Google Scholar]
- 10.Williams JM, Anderson JB, Laborde EL. Penile fracture caused by straddle injury to a nonerect penis. Urology. 2020;42:e47–8. doi: 10.1016/j.urology.2020.04.076. [DOI] [PubMed] [Google Scholar]
- 11.Falcone M, Garaffa G, Castiglione F, Ralph D. Current management of penile fracture: An up-to-date systematic review. Sex Med Rev. 2018;6:253–62. doi: 10.1016/j.sxmr.2017.07.009. [DOI] [PubMed] [Google Scholar]