

Abstract
While fecal incontinence and constipation can be measured through physiological testing, the subjective experience of severity and impact on health-related quality of life lead to both being most effectively captured through patient-reported measures. Patient-reported measures of severity and impact help to determine baseline symptoms, guide clinical decision making, and compare various treatments. Here, we take pause to review the psychometric qualities that make effective instruments, and discuss some of the most commonly used instruments along with the reasons behind their use. In addition, we highlight the benefits of a standardized instrument designed to evaluate the major symptoms of patients presenting with pelvic floor disorders (including fecal incontinence and constipation). Ultimately, we aim to provide guidance in choosing appropriate instruments for clinical and research use.
Keywords: patient-reported outcomes, fecal incontinence metrics, constipation metrics, severity measures
Following recommendations from the US Food and Drug Administration (FDA) to increase measurement of patient-reported outcomes (PROs), there has been increased attention to properly administering and interpreting PRO metrics. 1 2 Examples of PROs include self-reported measurements of severity, patient-validated self-report tools, and disease-specific quality of life (QOL) questionnaires. These measures are particularly important when assessing the frequency, severity, and impact of fecal incontinence (FI) and constipation.
FI is a symptom and is thus most effectively captured through subjective assessment rather than through physiologic studies. While measures such as anal manometry, defecography, endoanal ultrasonography, electromyography, and nerve conduction studies exist to guide treatment and identify potential underlying causes of incontinence, patient reports provide the greatest measure of FI severity and impact on daily life. 3 Furthermore, multiple studies have demonstrated that physiological testing does not always identify patients with FI, as seen with ultrasonography and anal manometry. 4 5
Similarly, constipation is categorized as a functional bowel disorder, meaning that it may not present through obvious physiological or anatomical abnormalities. 6 In addition, some patient-reported measures can distinguish between obstructive and slow-transit constipation, which allows for improved diagnosis and treatment. Constipation severity and impact are therefore also best measured through subjective patient assessment.
Patient-reported measures help to determine baseline symptoms, standardize diagnosis, guide clinical decision making, and compare different treatment outcomes. 7 8 9 Here, we discuss the psychometric evaluation and development of commonly used metrics for FI and constipation, how these instruments can be administered and scored in the clinic, as well as which aspects of symptom severity and impact they capture. With the publication of the Rome IV criteria for both conditions in 2016, review of existing instruments is necessary to determine consistency with the most recent diagnostic criteria from the Rome Foundation. 6 10 Ultimately, while numerous instruments exist to measure both conditions, a standardized instrument for patients presenting with pelvic floor disorders (including FI and constipation) would provide profound clinical and research benefits, and such a tool is discussed below.
Types of Metrics
Instruments to measure FI and constipation can be categorized as grading systems of severity, severity measures, or impact measures. 3 11
Grading Systems of Severity
Grading systems of severity are descriptive measures primarily developed for FI, and assign incontinence categories a grade in an ordinal fashion. 3 For example, Williams et al defined five categories of FI: (1) continent; (2) incontinence to flatus; (3) occasional incontinence to liquids; (4) occasional incontinence to solids, frequent incontinence to liquids; (5) frequent episodes of incontinence to solids and liquids. 12 While these systems may be intuitive and easy to use when describing patients, they neglect frequency and focus primarily on sphincter performance; for example, severity increases from gas to liquid to solid stool. 3 This system does not capture the increased severity of a patient suffering from frequent incontinence to liquid stools compared with a patient suffering from infrequent incontinence to solid stools. 3
Severity Measures
Severity measures attempt to go a step beyond grading systems by accounting for frequency, and are developed for both FI and constipation. Many FI severity measures include assessment of incontinence to gas, liquid stool, and solid stool. These measures vary in their range of frequencies, and can be unweighted (assigning equal value to the same frequency of different categories of incontinence) or weighted (assigning variable weights to the same frequency of different categories of incontinence). 3 Patient input is particularly important when determining how to weight instruments.
Some severity measures include summary scores, while others do not. The subset of severity measures lacking summary scores may provide insight into the population-level incidence of symptoms, but they are more difficult to implement in research due to a lack of a summary score or domain score. 3 Examples include the Mayo Clinic Fecal Incontinence Questionnaire and the Malouf Postoperative Questionnaire. 13 14
Impact Measures
Impact measures, or QOL measures, are also developed for both FI and constipation, and account for the effect of condition on QOL. 3 Here, QOL refers to health-related quality of life (HRQOL). Health-related quality of life (HRQOL) is a construct that captures an individual's perception of their health, and is generally described in five domains: behavioral, cognitive, emotional, physical, and social. 7 These measures help to account for how the impact of FI and constipation can vary with individual factors, such as age, culture, gender, lifestyle, and occupation. 15 These measures also help account for lifestyle restrictions that patients may impose to limit incontinence severity, which may not be revealed by severity measures. 3 Additionally, impact measures reveal how impact varies with severity; for example, a seemingly small improvement in severity may lead to a large improvement in QOL. 3 One study of 502 patients suffering from FI showed a moderate correlation between Fecal Incontinence Severity Index (FISI) scores and Fecal Incontinence Quality of Life Scale (FIQOL) scores, and a weak correlation with the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36), and thus highlights the importance of using severity measures in conjunction with impact measures. 16 17 18 19
Instruments that assess measurement of impact can be sorted into three categories. 11
Generic QOL scales (e.g., the SF-36) assess a wide range of HRQOL topics, making them applicable to a wide breadth of populations. 11 19 While these scales can detect differences between individuals with and without FI or constipation, they may lack responsiveness to clinically meaningful changes. 20 21
Specialized QOL scales (e.g., a depression scale) are designed around a specific aspect of QOL. 20 While these scales may not be as specific as condition-specific scales, they allow for comparison of that aspect between populations that may not share the same disease or affliction. 11
Condition-specific or disease-specific scales are designed to assess elements of a particular condition and are most applicable to the targeted population. 11 These scales can be further split into three groups. Traditional condition-specific scales can be used within a population who share a condition; for example, the FIQOL can be administered in adult populations with FI. 17 20 Systemic condition-specific scales can be used systematically across different disorders; for example, the Gastrointestinal Quality of Life Index (GIQLI) assesses domains beyond FI and can be used with individuals suffering from various gastrointestinal disorders. 22 Population-specific condition-specific scales are targeted for use with individuals who share a condition, for example, those with multiple sclerosis. 23
Psychometric Evaluation
Good measures are reliable, valid, sensitive to change, and easy to complete. 9 11 Evaluation is an ongoing process that depends on assessment of reliability and validity. 3
Reliability
Reliability is how well an instrument reflects the underlying phenomenon versus random error, and a reliable instrument should have greater variability between patients than within. 7
Test-retest reliability is the reproducibility of a measure over repeated administrations, and is evaluated through the intraclass correlation coefficient. 7 24 Instruments that have an r > 0.70 and a p > 0.05 are considered to have acceptable test-retest reliability. 7 25
Internal consistency is the consistency of items in an instrument that measure similar aspects of a variable, and is evaluated through the average correlation of items in a measure. 7 25 Instruments that have a Cronbach's α above 0.70 are considered to have acceptable internal consistency. 7 25
Validity
Validity is how well instruments measure what they set out to measure. 3
Face validity is an “eye-ball” test of the extent to which an instrument appears to measure what it is intended to. 3
Content validity is the extent to which an instrument includes important and necessary elements of a construct while excluding unrelated elements. 3 7 This can be assessed by patient input, expert opinion, or literature review. 7 11
Criterion validity is the correlation of an instrument to a gold standard measurement of the construct. 7 11 26 This comparison to a standard criterion can be further branched into two forms of criterion validity. 7 Concurrent criterion validity is assessed between two instruments at the same time, with an r above 0.70 reflecting acceptable concurrent validity. Predictive criterion validity is assessed at an initial time point and at an additional time point the instrument is set to predict, with an r above 0.70 reflecting acceptable predictive validity. 7
Discriminative validity is the ability to differentiate between groups; for example, those with and without FI. 7 9 Instruments that have an r less than 0.30 and a p less than 0.05 are considered to have acceptable discriminative validity. 7
Construct validity is the extent to which an instrument measures the construct of interest. 26 In the absence of a criterion standard, construct validity can be evaluated by testing hypotheses that a valid instrument would be expected to detect; for example, detecting a difference between a group of continent and incontinent adults. 3 Construct validity can also be evaluated by finding if an instrument shows convergent construct validity through significant positive correlations with related instruments ( r > 0.70) and divergent construct validity through significant negative correlations with unrelated or dissimilar ones ( r < 0.30). 3
Sensitivity or responsiveness to change is the ability of an instrument to track clinically important changes, and can be split into two forms. 3 7 Instruments that have an r < 0.30 and a p < 0.05 are considered to have acceptable sensitivity to change. 7 Internal responsiveness to change reflects the capacity to measure change over time, while external responsiveness reflects the capacity of an instrument to correlate with changes in another instrument measuring health status. 11
Fecal Incontinence Measures
The Rome IV criteria released in 2016 classify FI as a “functional anorectal disorder” (Section F), and define it as: “the recurrent uncontrolled passage of fecal material for at least 3 months.” 10 Under the Rome diagnostic criteria, FI includes:
“Recurrent uncontrolled passage of fecal material in an individual with a developmental age of at least 4 years.” 10
Severity Measures of Fecal Incontinence
In addition to validity, reliability, structure, and scoring, the four FI severity instruments discussed here were reviewed for inclusions beyond gas/liquid/solid, rectal urgency, pad usage, lifestyle alteration, and FI-related medications ( Table 1 ). 18 27 28 29 While some severity measures of FI are limited to the frequency of the three main incontinence categories, two instruments described below include incontinence to mucus. 18 28 Additionally, within severity instruments, measurements of impact (pad usage and lifestyle alteration) exist in a gray area between severity and QOL. 20 On one hand, they enrich the understanding of patient symptoms, since patients may restrict activities to avoid episodes; but on the other hand, these inclusions may introduce a metric of subjective fastidiousness. 11 Two instruments below include items assessing impact. 27 29 Patients with FI consider rectal urgency highly unpredictable and distressing, but only one instrument discussed here includes urgency. 29 30 Lastly, one instrument includes an item for taking FI-related (constipating) medications. 29
Table 1. Severity measures of fecal incontinence.
| Instrument | Pescatori Incontinence Score 28 | Wexner/Cleveland Clinic Florida Incontinence Score (CCFIS) 27 | Fecal Incontinence Severity Index (FISI) 18 | Vaizey/St. Mark's Incontinence Score (SMIS) 29 |
|---|---|---|---|---|
| Citation | Pescatori et al, 1992 | Jorge and Wexner, 1993 | Rockwood et al, 1999 | Vaizey et al, 1999 |
| Google Scholar citations (as of 9/29/2019) | 362 | 2430 | 658 | 997 |
| Reliability | Yes | Yes | Yes | Yes |
| Validity | Yes | Yes | Yes | Yes |
| Structure | 3 items Degree of incontinence –A, flatus/mucus –B, liquid stool –C, solid stool |
5 items Item x frequency –Solid –Liquid –Gas –Wears pad –Lifestyle alteration |
4 items Type of incontinence –Gas –Mucus –Liquid stool –Solid stool |
7 items Item x frequency –Solid stool –Liquid stool –Gas –Alteration of lifestyle Yes/no –Needs to wear a pad or plug –Taking constipating medicines –Lack of ability to defer defecation for 15 minutes |
| Frequency categories | 3 categories –1, Less than once a week –2, At least once a week –3, Every day |
5 categories –Never (0) –Rarely (< 1/month) –Sometimes (< 1/week, ≥ 1/month) –Usually (< 1/day, ≥ 1/week) –Always (≥ 1/day) |
6 categories –2 or more times a day –Once a day –2 or more times a week –Once a week –1 to 3 times a month –Never |
5 categories –Never (no episodes in the past 4 weeks) –Rarely (1 episode in the past 4 weeks) –Sometimes (> 1 episode in the past 4 weeks but < 1 a week) –Weekly (1 or more episodes a week but < 1 a day) –Daily (1 or more episodes a day) |
| Score method | Weighted –ABC-123 classification: A1 (2), A2 (3), B1 (3), A3 (4), B2 (4), C1 (4), B3 (5), C2 (5), C3 (6) |
Unweighted –Frequency classification: never (0), rarely (1), sometimes (2), usually (3), always (4) |
Weighted –Patient-derived and surgeon-derived weighting chart |
Weighted Item x frequency –Never (0), rarely (1), sometimes (2), weekly (3), daily (4) Yes/no –Pad/plug: no (0), yes (2) –Constipating medicines: no (0), yes (2) –Urgency: no (0), yes (4) |
| Score range | 0 (full continence) 6 (daily incontinence for solid stool) |
0 (perfect continence) 20 (complete incontinence) |
Patient-derived 0 (least severe) 61 (most severe) Surgeon-derived 0 (least severe) 59 (most severe) |
0 (perfect continence) 24 (complete incontinence) |
| 1. Other | Mucus | No | Mucus | No |
| 2. Pad usage | No | Yes | No | Yes |
| 3. Lifestyle alteration | No | Yes | No | Yes |
| 4. Urgency | No | No | No | Yes |
| 5. Medication | No | No | No | Yes |
| Inclusions | 1/5 | 2/5 | 1/5 | 4/5 |
The Pescatori Incontinence Score is a degree x frequency matrix designed to assess FI severity. 28 This score follows an ABC-123 classification system, scoring based on three incontinence degree categories and three frequencies (1 = less than once a week, 2 = at least once a week, 3 = every day). 28 Scores are based on adding the category letter value (A = 1, B = 2, C = 3) with the frequency value, resulting in a score range from 0 for full continence to a maximum of 6 for daily incontinence for solid stool. 28 While this score does not include pad usage, lifestyle alteration, urgency, or FI-related medications, it does notably include incontinence to mucus in addition to the traditional gas/liquid/solid. 28
The Wexner/Cleveland Clinic Florida Incontinence Score (CCFIS) consists of an item x frequency matrix designed to assess FI severity. 27 The CCFIS is composed of five items (solid, liquid, gas, wears pad, and lifestyle alteration) and five frequencies (never = 0, rarely = 1, sometimes = 2, usually = 3, always = 4), for a total score ranging from 0 for full continence to 20 for complete incontinence. 27 The CCFIS includes pad usage and lifestyle alteration, and assigns all five items the same weight. 27 The CCFIS is noted for being easily understood and correlated with patients' own symptom perception, and has led to the instrument being particularly well-cited ( Table 1 ). 21 31 32
The FISI consists of a type x frequency matrix designed to assess FI severity. 18 The FISI is composed of four types of incontinence (gas, mucus, liquid, solid) by six frequencies (2 or more times a day, once a day, 2 or more times a week, once a week, 1 to 3 times a month, never). 18 To create an externally developed weighting system, an abbreviated 20-cell type-frequency matrix (without “never”) was presented to patients and colorectal surgeons who were instructed to rank each cell from 1 (least severe) to 20 (most severe). 18 These rankings were then averaged to create one patient-derived scoring system (ranging from 0 to 61) and one surgeon-derived (ranging from 0 to 59). 18 Similar to the Pescatori Incontinence Score, the FISI includes incontinence to mucus. 18 One criticism of the FISI is that the index includes patients who suffer from incontinence 1 to 3 times per month in the same frequency category, while patients may consider episodes 3 times a month far more severe than 1 episode a month. 18
The Vaizey/St. Mark's Incontinence Score (SMIS) consists of an item x frequency matrix similar to the CCFIS, but with a few adjustments. 29 The SMIS includes four items (solid, liquid, gas, and alteration of lifestyle) by five frequencies (never = 0, rarely = 1, sometimes = 2, weekly = 3, daily = 4), and changes the use of a pad/plug to a yes/no question. 29 The SMIS also includes the use of constipating medications and the lack of ability to defer defecation for 15 minutes (urgency) as additional yes/no questions. 29 While wearing a pad/plug and constipating medications are weighted as 2 for yes and 0 for no, urgency is weighted as 4 for yes and 0 for no—introducing weighting not seen with the CCFIS. 29 The total score ranges from 0 for continent individuals to 24 for incontinent individuals. 29 Vaizey et al examined the test-retest reliability of the SMIS, CCFIS, and Pescatori Incontinence Score in 13 incontinent patients, and found acceptable reliability in all scales except the Pescatori Incontinence Score. 29 The SMIS is a commonly-cited instrument, and one study found both the SMIS and CCFIS exhibited excellent intraobserver (initial and 6 week time points) and interobserver reliability (completion by a physician and nurse) ( Table 1 ). 32
Impact Measures of Fecal Incontinence
In addition to validity, reliability, structure, and scoring, the three FI impact instruments included here were reviewed for inclusion of the five major aspects of HRQOL: physical, social, emotional, cognitive, and behavioral ( Table 2 ). 17 33 34 While two instruments adequately include all five aspects, one instrument integrated three. 17 33 34
Table 2. Impact measures of fecal incontinence.
| Instrument | Fecal Incontinence Quality of Life Scale (FIQOL) 17 | Manchester Health Questionnaire (MHQ) 33 | TyPE Specification 34 |
|---|---|---|---|
| Citation | Rockwood et al, 2000 | Bugg et al, 2001 | Wexner et al, 2002 |
| Google Scholar citations (as of 9/29/2019) | 1083 | 113 | 147 |
| Reliability | Yes: IC | Yes: TR, IC | No |
| Validity | Yes: DV, CCSV | Yes: FV, CCSV | No |
| Structure | 4 domains, 29 items –Lifestyle ( 10 items ) –Coping/behavior ( 9 items ) –Depression/self-perception ( 7 items ) –Embarrassment ( 3 items ) |
9 domains, 32 items –General health –Impact incontinence –Role –Physical function –Social function –Personal function –Emotional function –Energy –Severity measures |
2 domains, 20 items –Fear of leakage ( 10 items ) –Occurrence of leakage ( 10 items ) |
| Score method | Domain scores range from 1 to 5 | Domain scores range from 0 to 100 | Items scored along a 5-point Likert scale |
| Score range | Lower (lower QOL) Higher (higher QOL) |
Lower (higher QOL) Higher (lower QOL) |
Lower (higher QOL) Higher (lower QOL) |
| 1. Physical | Yes | Yes | Yes |
| 2. Social | Yes | Yes | Yes |
| 3. Emotional | Yes | Yes | No |
| 4. Cognitive | Yes | Yes | No |
| 5. Behavioral | Yes | Yes | Yes |
| HRQOL Inclusions | 5/5 | 5/5 | 3/5 |
Abbreviations: CCRV, concurrent criterion validity; CCSV, convergent construct validity; CRV, criterion validity; CSV, construct validity; CV, content validity; DCSV, divergent construct validity; DV, discriminative validity; FV, face validity; IC, internal consistency; PCRV, predictive criterion validity; QOL, quality of life; SC, sensitivity to change; TR, test-retest reliability.
The FIQOL scale is a 29-item disease-specific questionnaire designed to assess the impact of FI. 17 The FIQOL is composed of four domains containing 3 to 10 questions each: lifestyle, coping/behavior, depression/self-perception, and embarrassment. 17 The score for each domain is calculated by finding the mean of the included questions, resulting in a domain score between 1 and 5, with a lower score indicating a lower QOL. 17 The FIQOL adequately captures the five major aspects of HRQOL. 17 Of the three FI impact instruments discussed here, the FIQOL is the most well-cited, which is likely due to adequate validation and ease of use ( Table 2 ).
The Manchester Health Questionnaire (MHQ) is a 32-item questionnaire designed to assess the impact of FI. 33 The MHQ was adapted from a validated measure of urinary incontinence, the King's Health Questionnaire, and although it is not female-specific, the MHQ has primarily been used to measure FI impact in females. 33 35 The MHQ is composed of nine domains that effectively represent HRQOL: general health, impact incontinence, role, physical function, social function, personal function, emotional function, energy, and severity. 33 MHQ domain scores range from 0 to 100, with a higher score representing a lower QOL. 33
The TyPE Specification is a 20-item questionnaire designed to assess the impact of FI. 34 The TyPE Specification consists of 10 items (walking, vigorous exercise, household chores, visiting friends, driving, sexual relationships, employment, traveling, church or temple attendance, and shopping), and each item is answered twice; once for “fear of leakage” (the first domain), and once for “occurrence of leakage” (the second domain). 34 Higher TyPE specification scores indicate lower QOL. 34 Unlike the two FI impact measures discussed above, the TyPE Specification was not formally assessed for reliability or validity. 34 Additionally, the TyPE does not include two aspects of HRQOL: cognitive function and emotional function. 34
Constipation Measures
The Rome IV criteria released in 2016 classify functional constipation as a “functional bowel disorder” (Section C), and define it as: “a functional bowel disorder in which symptoms of difficult, infrequent, or incomplete defecation predominate.” 6 Under the Rome diagnostic criteria, functional constipation includes two or more of the following:
“Straining during more than one-fourth (25%) of defecations
Lumpy or hard stools (BSFS 1–2) more than one-fourth (25%) of defecations
Sensation of incomplete evacuation more than one-fourth (25%) of defecations
Sensation of anorectal obstruction/blockage more than one-fourth (25%) of defecations
Manual maneuvers to facilitate more than one-fourth (25%) of defecations (e.g., digital evacuation, support of the pelvic floor)
Fewer than 3 spontaneous bowel movements per week.” 6
Severity Measures of Constipation
In addition to validity, reliability, structure, and scoring, the four constipation severity instruments discussed here were reviewed for their inclusion of the Rome diagnostic criteria discussed above ( Table 3 ). 6 8 36 37 38 39 Interestingly, while all four instruments discussed here incorporate (c) incomplete evacuation, none of them effectively include (d) sensation of blockage or (f) frequency. 6 36 37 38 39 The two most recent instruments include three items from the Rome criteria, while one includes two items, and the other includes only one. 6 36 37 38 39
Table 3. Severity measures of constipation.
| Instrument | Constipation Assessment Scale (CAS) 38 | Constipation Scoring System (CSS) 36 | Patient Assessment of Constipation—Symptoms (PAC-SYM) 37 | Constipation Severity Instrument (CSI) 39 |
|---|---|---|---|---|
| Citation | McMillan and Williams, 1989 | Agachan et al, 1996 | Frank et al, 1999 | Varma et al, 2008 |
| Google Scholar citations (as of 9/29/2019) | 223 | 865 | 270 | 102 |
| Reliability | Yes: TR, IC | Yes | Yes: TR, IC | Yes: TR, IC |
| Validity | Yes: CV, DV | Yes: CV, CRV, DV | Yes: FV, CV, CRV, DV, CSV, CCSV, DCSV, SC | Yes: FV, CV, CRV, DV, CCSV, DCSV |
| Structure | 8 items –Abdominal distension or bloating –Change in amount of gas passed rectally –Less frequent bowel movements –Oozing liquid stool –Rectal fullness or pressure –Rectal pain with bowel movement –Small volume of stool –Unable to pass stool |
8 items –Frequency of bowel movements –Painful evacuation –Incomplete evacuation –Abdominal pain –Length of time per attempt –Assistance for defecation –Unsuccessful attempts for evacuation per 24 hours –Duration of constipation |
3 domains, 12 items –Stool symptoms –Rectal symptoms –Abdominal symptoms |
3 domains, 19 items –Obstructive defecation –Colonic inertia –Pain |
| Score method | 3-point Likert scales | 3-point and 5-point Likert scales | 5-point Likert scales | 4-point and 5-point Likert scales |
| Score range | 0 (no problem) 16 (severe constipation) |
0 (no problem) 30 (severe constipation) |
0 (no problem) 48 (severe constipation) |
0 (no problem) 73 (severe constipation) |
| Threshold score | Not reported | More than 15 | Not reported | Not reported |
| Completion time | ∼2 minutes | Not reported | 4–6 minutes | Not reported |
| Time frame | Last week | 0 to more than 20 years | Previous 2 weeks | Past month and present |
| a. Straining | No | No | Yes | Yes |
| b. Lumpy/hard | No | No | Yes | No |
| c. Incomplete evacuation | Yes | Yes | Yes | Yes |
| d. Sensation of blockage | No | No | No | No |
| e. Manual maneuvers | No | Yes | No | Yes |
| f. Frequency | No | No | No | No |
| Rome inclusions | 1/6 | 2/6 | 3/6 | 3/6 |
Abbreviations: CCRV, concurrent criterion validity; CCSV, convergent construct validity; CRV, criterion validity; CSV, construct validity; CV, content validity; DCSV, divergent construct validity; DV, discriminative validity; FV, face validity; IC, internal consistency; PCRV, predictive criterion validity; SC, sensitivity to change; TR, test-retest reliability.
The Constipation Assessment Scale (CAS) is a measure designed to assess constipation severity. 38 The CAS scores eight items from the last week on a 3-point Likert scale from 0 (no problem) to 2 (severe problem), for a total score between 0 and 16. 38 The CAS does not report a threshold score to assist as a cutoff for constipation, but the instrument only takes ∼2 minutes to complete—making it easy to use in the clinic. 38 Out of the six Rome IV diagnostic criteria, the CAS only includes (c) incomplete evacuation. 38
The Constipation Scoring System (CSS) is a measure designed to assess constipation severity. 36 The CSS scores eight items on a 5-point Likert scale for seven items (0–4) and a 3-point Likert scale for one item (0–2), for a total score between 0 and 30. 36 The CSS reports a threshold score of 15 or above as indicative of constipation, but does not report a time for completion. 36 Out of the Rome IV criteria, the CSS includes (c) incomplete evacuation, and (e) manual maneuvers. 36 Of the four constipation severity instruments discussed here, the CSS is the most well-cited, which may be due to the benefits of a threshold score ( Table 3 ).
The Patient Assessment of Constipation—Symptoms (PAC-SYM) is a measure designed to assess constipation severity. 37 The PAC-SYM scores 12 items from the previous 2 weeks along a 5-point Likert scale (0–4), providing a total score between 0 (no problem) to 48 (severe constipation). 37 The items are separated into three domains: stool symptoms, rectal symptoms, and abdominal symptoms. 37 While the PAC-SYM does not report a threshold score, the instrument is designed for completion in 4 to 6 minutes. 37 The PAC-SYM includes three of the six Rome IV criteria: (a) straining, (b) lumpy/hart stool, and (c) incomplete evacuation. 37
The Constipation Severity Index (CSI) is a measure designed to assess constipation severity. 39 The CSI scores 19 items from the past month and present along 4-point and 5-point Likert scales, generating a total score between 0 (no problem) and 73 (severe constipation). 39 The items are separated into three domains: obstructive defecation, colonic inertia, and pain. 39 The CSI does not report a threshold score, nor an estimated time for completion. 39 The CSI includes three of the six Rome IV criteria: (a) straining, (c) incomplete evacuation, and (e) manual maneuvers. 39
Impact Measures of Constipation
In addition to validity, reliability, structure, and scoring, the two constipation impact instruments included here were reviewed for inclusion of the five major aspects of HRQOL: physical, social, emotional, cognitive, and behavioral ( Table 4 ). While the first instrument adequately includes all five aspects, the second instrument is missing physical function. 40 41
Table 4. Impact measures of constipation.
| Instrument | Patient Assessment of Constipation—Quality of Life (PAC-QOL) 40 | Constipation-related Quality of Life (CR-QOL) 41 |
|---|---|---|
| Citation | Marquis et al, 2005 | Wang et al, 2009 |
| Google Scholar citations (as of 9/29/2019) | 383 | 28 |
| Reliability | Yes: TR, IC | Yes: TR, IC |
| Validity | Yes: SC | Yes: DV, CCSV |
| Structure | 4 domains, 28 items –Worries/concerns –Physical discomfort –Psychosocial discomfort –Satisfaction |
4 domains, 18 items –Social impairment ( 5 items ) –Distress ( 6 items ) –Eating habits ( 3 items ) –Bathroom attitudes ( 4 items ) |
| Score method | 5-point Likert scales –Frequency: none of the time (0), all of the time (4) –Severity: not at all (0), extremely (4) |
5-point Likert scales –Frequency: never (1), always (5) –Severity: not at all (1), extremely (5) |
| Score range | 0 (higher QOL) 112 (lower QOL) |
18 (higher QOL) 90 (lower QOL) |
| Time frame | Past 2 weeks | Past 12 months |
| 1. Physical | Yes | No |
| 2. Social | Yes | Yes |
| 3. Emotional | Yes | Yes |
| 4. Cognitive | Yes | Yes |
| 5. Behavioral | Yes | Yes |
| HRQOL Inclusions | 5/5 | 4/5 |
Abbreviations: CCRV, concurrent criterion validity; CCSV, convergent construct validity; CRV, criterion validity; CSV, construct validity; CV, content validity; DCSV, divergent construct validity; DV, discriminative validity; FV, face validity; QOL, quality of life; IC, internal consistency; PCRV, predictive criterion validity; SC, sensitivity to change; TR, test-retest reliability.
The Patient Assessment of Constipation—Quality of Life (PAC-QOL) is the companion impact measure to the PAC-SYM discussed earlier, and is a disease-specific questionnaire designed to assess the impact of constipation. 40 The PAC-QOL scores 28 items from the past 2 weeks along 5-point Likert scales, generating a score between 0 (higher QOL) and 112 (lower QOL). 40 The items are separated into four domains: worries/concerns, physical discomfort, psychosocial discomfort, and satisfaction. 40 The PAC-QOL effectively captures the five major aspects of HRQOL, which may have contributed to its widespread use ( Table 4 ).
The constipation-related quality of life (CR-QOL) is the companion impact measure to the CSI discussed earlier, and is a disease-specific questionnaire designed to assess the impact of constipation. 41 The CR-QOL scores 18 items from the past 12 months along 5-point Likert scales, generating a score between 18 (higher QOL) and 90 (lower QOL). 41 The items are separated into four domains: social impairment, distress, eating habits, and bathroom attitudes. 41 The CR-QOL sufficiently captures all main aspects of HRQOL except physical function. 41
Combined Measures
Severity Measures of Both Fecal Incontinence and Constipation
The Patients with Fecal Incontinence and Constipation Questionnaire (FICQ) and the Fecal Incontinence and Constipation Assessment (FICA) are both combined severity measures of FI and constipation ( Table 5 ). 42 43 These joint instruments may be valuable for assessing two conditions in one instrument, and the FICA is one of the few constipation instruments to efficiently implement the Bristol Stool Scale—a scale that can assist in distinguishing constipation-predominant irritable bowel syndrome from functional constipation. 44 Unfortunately, the FICA contains 98 items and the FICQ contains 47. 42 43 The length of these questionnaires may make them difficult to implement in the clinic; even after considering the benefit of assessing two conditions.
Table 5. Severity measures of both fecal incontinence and constipation.
| Instrument | Patients with Fecal Incontinence and Constipation Questionnaire (FICQ) 43 | Fecal Incontinence and Constipation Assessment (FICA) 42 |
|---|---|---|
| Citation | Osterberg et al, 1996 | Bharucha et al, 2004 |
| Google Scholar citations (as of 9/29/2019) | 107 | 90 |
| Reliability | Yes | Yes |
| Validity | Yes | Yes |
| Structure | 47 items –Constipation ( 15 items ) –Incontinence ( 12 items ) –Other symptoms ( 10 items ) –Obstetric events ( 7 items ) –Social and psychological impact ( 3 items ) |
8 domains, 98 items –General bowel habits –Abdominal pain –Treatment of constipation –Fecal incontinence –Urinary symptoms –Anorectal disease –Health care utilization –Quality of life |
One Tool for Patient-Reported Measures of Pelvic Floor Disorders
A measure that can feasibly assess both FI and constipation in the clinic would provide valuable insight. Along with urinary incontinence, lower urinary tract symptoms, male sexual function, and female sexual function, FI and constipation exist as pelvic floor disorders. Since patients suffering from pelvic floor disorders may be treated by clinicians across specialties, a universal set of validated measures would foster a common language of patient-reported symptoms. 45 The Pelvic Floor Disorders Consortium (PFDC) laid the framework for this common language through expert discussion and consensus on the best available instruments for the major symptom categories related to pelvic floor disorders: FI, constipation, urinary incontinence, lower urinary tract symptoms, and sexual dysfunction. 45 The consensus resulted in a battery of recommended instruments called the IMPACT (Initial Measurement of Patient Reported Pelvic Floor Complaints Tool), which will allow for a common initial assessment through a short form with 35 questions for men and 45 for women. 45 The IMPACT will support patients through coordination of care across specialties (e.g., colorectal surgeons, urogynecologists, urologists, gastroenterologists, and physiotherapists), which will allow for comparison of treatment options, and accurate interpretation of patient-perceived severity and impact. 45 In addition, the IMPACT will facilitate research by supporting pooling of data for meta-analyses and long-term data collection with validated instruments. 45
The PFDC Working Group on Patient Reported Outcomes concluded that instruments should be valid, easy to use in the clinic (brief), responsive to change, and familiar across specialties. 45 For FI severity, 12 panelists recommend the CCFIS in conjunction with the SMIS. 27 29 45 For a preferred FI QOL instrument, the panelists selected the FIQOL. 17 45 The panelists were especially interested in instruments that included urgency, since patients with FI consider rectal urgency highly unpredictable and distressing. 30
For constipation severity, 12 panelists recommend the PAC-SYM in conjunction with the CSI. 37 39 45 For a preferred constipation QOL instrument, the panelists selected the PAC-QOL. 40 45 The panelists were especially interested in finding a combination of instruments to support delineation and characterization of the constipation spectrum, including obstructed defecation syndrome, slow transit constipation, and irritable bowel syndrome. 45
The “IMPACT Bowel Function Assessment Tool, Short Form” combines repeated questions while retaining all scoring powers, leading to a compact 12-question section on bowel function that includes six instruments: CCFI, SMIS, PAC-SYM, CSI, Colorectal-anal Distress Inventory 8 (CRADI-8), and Bristol Stool Scale (BSS) ( Fig. 1 ). 27 29 37 39 44 45 46
Fig. 1.
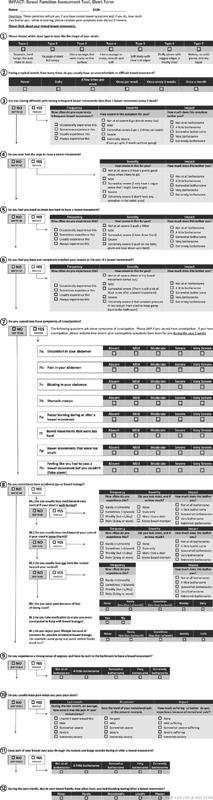
IMPACT (Initial Measurement of Patient-Reported Pelvic Floor Complaints Tool) bowel function, short form. (Reprinted with permission from Wolters Kluwer Health, Inc.: Bordeianou LG, Anger JT, Boutros M, et al. Measuring Pelvic Floor Disorder Symptoms Using Patient-Reported Instruments: Proceedings of the Consensus Meeting of the Pelvic Floor Consortium of the American Society of Colon and Rectal Surgeons, the International Continence Society, the American Urogynecologic Society, and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction. Dis Colon Rectum 2020;63(1):15–17 ( https://journals.lww.com/dcrjournal ).)
Conclusion
In this review, we have detailed several metrics that can be used to quantify FI and constipation. Each of the scores incorporates various measures of severity, frequency, and impact on QOL, and accordingly the scores described have unique advantages and disadvantages. It is important to note that while many of the instruments discussed here have already demonstrated at least one form of reliability and one form of validity, all could benefit from continuing validation in additional populations to demonstrate generalizability. 9 Still, there are commonalities among the most commonly cited instruments discussed here. The most well-used instruments are responsive to change, easy to use in the clinic, and straightforward to score and interpret. 11 A recent consensus within the pelvic floor community will allow for future comprehensive assessment of patient symptoms and experiences, as well as comparison across centers and studies.
Conflict of Interest None.
First co-authors.
References
- 1.McLeod L D, Coon C D, Martin S A, Fehnel S E, Hays R D. Interpreting patient-reported outcome results: US FDA guidance and emerging methods. Expert Rev Pharmacoecon Outcomes Res. 2011;11(02):163–169. doi: 10.1586/erp.11.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.U.S. Department of Health and Human Services FDA Center for Drug Evaluation and Research; U.S. Department of Health and Human Services FDA Center for Biologics Evaluation and Research.U.S. Department of Health and Human Services FDA Center for Devices and Radiological Health. Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance Health Qual Life Outcomes 2006479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Baxter N N, Rothenberger D A, Lowry A C. Measuring fecal incontinence. Dis Colon Rectum. 2003;46(12):1591–1605. doi: 10.1007/BF02660762. [DOI] [PubMed] [Google Scholar]
- 4.Karoui S, Savoye-Collet C, Koning E, Leroi A M, Denis P. Prevalence of anal sphincter defects revealed by sonography in 335 incontinent patients and 115 continent patients. AJR Am J Roentgenol. 1999;173(02):389–392. doi: 10.2214/ajr.173.2.10430142. [DOI] [PubMed] [Google Scholar]
- 5.Rasmussen O O, Sørensen M, Tetzschner T, Christiansen J. Dynamic anal manometry in the assessment of patients with obstructed defecation. Dis Colon Rectum. 1993;36(10):901–907. doi: 10.1007/BF02050623. [DOI] [PubMed] [Google Scholar]
- 6.Lacy B E, Mearin F, Chang L. Bowel disorders. Gastroenterology. 2016;150(06):1393–1407. doi: 10.1053/j.gastro.2016.02.031. [DOI] [PubMed] [Google Scholar]
- 7.Lee J T, Madoff R D, Rockwood T H. Quality-of-life measures in fecal incontinence: is validation valid? Dis Colon Rectum. 2015;58(03):352–357. doi: 10.1097/DCR.0000000000000290. [DOI] [PubMed] [Google Scholar]
- 8.McCrea G L, Miaskowski C, Stotts N A, Macera L, Hart S A, Varma M G. Review article: self-report measures to evaluate constipation. Aliment Pharmacol Ther. 2008;27(08):638–648. doi: 10.1111/j.1365-2036.2008.03626.x. [DOI] [PubMed] [Google Scholar]
- 9.Wang J Y, Varma M G. Measures for fecal incontinence, constipation, and associated quality of life. Semin Colon Rectal Surg. 2010;21(01):22–26. [Google Scholar]
- 10.Rao S SC, Bharucha A E, Chiarioni G. Anorectal disorders. Gastroenterology. 2016;150(06):1430–1442. doi: 10.1053/j.gastro.2016.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Van Koughnett J A, Boutros M, Wexner S D. Switzerland: Springer, Cham; 2017. Signs and symptoms in coloproctology: data collection and scores; pp. 127–150. [Google Scholar]
- 12.Williams N S, Patel J, George B D, Hallan R I, Watkins E S.Development of an electrically stimulated neoanal sphincter Lancet 1991338(8776):1166–1169. [DOI] [PubMed] [Google Scholar]
- 13.Malouf A J, Norton C S, Engel A F, Nicholls R J, Kamm M A.Long-term results of overlapping anterior anal-sphincter repair for obstetric trauma Lancet 2000355(9200):260–265. [DOI] [PubMed] [Google Scholar]
- 14.Reilly W T, Talley N J, Pemberton J H, Zinsmeister A R.Validation of a questionnaire to assess fecal incontinence and associated risk factors: Fecal Incontinence Questionnaire Dis Colon Rectum 20004302146–153., discussion 153–154 [DOI] [PubMed] [Google Scholar]
- 15.Chaliha C, Stanton S L. The ethnic cultural and social aspects of incontinence--a pilot study. Int Urogynecol J Pelvic Floor Dysfunct. 1999;10(03):166–170. doi: 10.1007/s001920050039. [DOI] [PubMed] [Google Scholar]
- 16.Bordeianou L, Rockwood T, Baxter N, Lowry A, Mellgren A, Parker S. Does incontinence severity correlate with quality of life? Prospective analysis of 502 consecutive patients. Colorectal Dis. 2008;10(03):273–279. doi: 10.1111/j.1463-1318.2007.01288.x. [DOI] [PubMed] [Google Scholar]
- 17.Rockwood T H, Church J M, Fleshman J W.Fecal incontinence quality of life scale: quality of life instrument for patients with fecal incontinence Dis Colon Rectum 200043019–16., discussion 16–17 [DOI] [PubMed] [Google Scholar]
- 18.Rockwood T H, Church J M, Fleshman J W. Patient and surgeon ranking of the severity of symptoms associated with fecal incontinence: the fecal incontinence severity index. Dis Colon Rectum. 1999;42(12):1525–1532. doi: 10.1007/BF02236199. [DOI] [PubMed] [Google Scholar]
- 19.Ware J E, Jr, Sherbourne C D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(06):473–483. [PubMed] [Google Scholar]
- 20.Rockwood T H. Incontinence severity and QOL scales for fecal incontinence. Gastroenterology. 2004;126(01) 01:S106–S113. doi: 10.1053/j.gastro.2003.10.057. [DOI] [PubMed] [Google Scholar]
- 21.Rothbarth J, Bemelman W A, Meijerink W J. What is the impact of fecal incontinence on quality of life? Dis Colon Rectum. 2001;44(01):67–71. doi: 10.1007/BF02234823. [DOI] [PubMed] [Google Scholar]
- 22.Eypasch E, Williams J I, Wood-Dauphinee S. Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg. 1995;82(02):216–222. doi: 10.1002/bjs.1800820229. [DOI] [PubMed] [Google Scholar]
- 23.Wiesel P H, Norton C, Roy A J, Storrie J B, Bowers J, Kamm M A. Gut focused behavioural treatment (biofeedback) for constipation and faecal incontinence in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2000;69(02):240–243. doi: 10.1136/jnnp.69.2.240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Streiner D L, Norman G R. Oxford: Oxford University Press; 1994. A Practical Guide to Their Development and Use; pp. 104–127. [Google Scholar]
- 25.Nunnally J C, Bernstein I H. New York: McGraw Hill; 1994. Psychometric Theory; pp. 248–292. [Google Scholar]
- 26.Izumi K. The measures to evaluate constipation: a review article. Gastroenterol Nurs. 2014;37(02):137–146. doi: 10.1097/SGA.0000000000000034. [DOI] [PubMed] [Google Scholar]
- 27.Jorge J M, Wexner S D. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993;36(01):77–97. doi: 10.1007/BF02050307. [DOI] [PubMed] [Google Scholar]
- 28.Pescatori M, Anastasio G, Bottini C, Mentasti A. New grading and scoring for anal incontinence. Evaluation of 335 patients. Dis Colon Rectum. 1992;35(05):482–487. doi: 10.1007/BF02049407. [DOI] [PubMed] [Google Scholar]
- 29.Vaizey C J, Carapeti E, Cahill J A, Kamm M A. Prospective comparison of faecal incontinence grading systems. Gut. 1999;44(01):77–80. doi: 10.1136/gut.44.1.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Norton N J. The perspective of the patient. Gastroenterology. 2004;126(01) 01:S175–S179. doi: 10.1053/j.gastro.2003.10.081. [DOI] [PubMed] [Google Scholar]
- 31.Brown H W, Wexner S D, Lukacz E S. Factors associated with care seeking among women with accidental bowel leakage. Female Pelvic Med Reconstr Surg. 2013;19(02):66–71. doi: 10.1097/SPV.0b013e31828016d3. [DOI] [PubMed] [Google Scholar]
- 32.Hussain Z I, Lim M, Stojkovic S. The test-retest reliability of fecal incontinence severity and quality-of-life assessment tools. Dis Colon Rectum. 2014;57(05):638–644. doi: 10.1097/DCR.0000000000000118. [DOI] [PubMed] [Google Scholar]
- 33.Bug G J, Kiff E S, Hosker G. A new condition-specific health-related quality of life questionnaire for the assessment of women with anal incontinence. BJOG. 2001;108(10):1057–1067. doi: 10.1111/j.1471-0528.2001.00245.x. [DOI] [PubMed] [Google Scholar]
- 34.Wexner S D, Baeten C, Bailey R. Long-term efficacy of dynamic graciloplasty for fecal incontinence. Dis Colon Rectum. 2002;45(06):809–818. doi: 10.1007/s10350-004-6302-1. [DOI] [PubMed] [Google Scholar]
- 35.Kelleher C J, Cardozo L D, Khullar V, Salvatore S. A new questionnaire to assess the quality of life of urinary incontinent women. Br J Obstet Gynaecol. 1997;104(12):1374–1379. doi: 10.1111/j.1471-0528.1997.tb11006.x. [DOI] [PubMed] [Google Scholar]
- 36.Agachan F, Chen T, Pfeifer J, Reissman P, Wexner S D. A constipation scoring system to simplify evaluation and management of constipated patients. Dis Colon Rectum. 1996;39(06):681–685. doi: 10.1007/BF02056950. [DOI] [PubMed] [Google Scholar]
- 37.Frank L, Kleinman L, Farup C, Taylor L, Miner P., Jr Psychometric validation of a constipation symptom assessment questionnaire. Scand J Gastroenterol. 1999;34(09):870–877. doi: 10.1080/003655299750025327. [DOI] [PubMed] [Google Scholar]
- 38.McMillan S C, Williams F A. Validity and reliability of the Constipation Assessment Scale. Cancer Nurs. 1989;12(03):183–188. doi: 10.1097/00002820-198906000-00012. [DOI] [PubMed] [Google Scholar]
- 39.Varma M G, Wang J Y, Berian J R, Patterson T R, McCrea G L, Hart S L. The constipation severity instrument: a validated measure. Dis Colon Rectum. 2008;51(02):162–172. doi: 10.1007/s10350-007-9140-0. [DOI] [PubMed] [Google Scholar]
- 40.Marquis P, De La Loge C, Dubois D, McDermott A, Chassany O. Development and validation of the Patient Assessment of Constipation Quality of Life questionnaire. Scand J Gastroenterol. 2005;40(05):540–551. doi: 10.1080/00365520510012208. [DOI] [PubMed] [Google Scholar]
- 41.Wang J Y, Hart S L, Lee J, Berian J R, McCrea G L, Varma M G. A valid and reliable measure of constipation-related quality of life. Dis Colon Rectum. 2009;52(08):1434–1442. doi: 10.1007/DCR.0b013e3181a51196. [DOI] [PubMed] [Google Scholar]
- 42.Bharucha A E, Locke G R, III, Seide B M, Zinsmeister A R. A new questionnaire for constipation and faecal incontinence. Aliment Pharmacol Ther. 2004;20(03):355–364. doi: 10.1111/j.1365-2036.2004.02028.x. [DOI] [PubMed] [Google Scholar]
- 43.Osterberg A, Graf W, Karlbom U, Påhlman L. Evaluation of a questionnaire in the assessment of patients with faecal incontinence and constipation. Scand J Gastroenterol. 1996;31(06):575–580. doi: 10.3109/00365529609009130. [DOI] [PubMed] [Google Scholar]
- 44.Heaton K W, O'Donnell L J. An office guide to whole-gut transit time. Patients' recollection of their stool form. J Clin Gastroenterol. 1994;19(01):28–30. doi: 10.1097/00004836-199407000-00008. [DOI] [PubMed] [Google Scholar]
- 45.Bordeianou L G, Anger J T, Boutros M. Measuring Pelvic Floor Disorder Symptoms Using Patient-Reported Instruments: Proceedings of the Consensus Meeting of the Pelvic Floor Consortium of the American Society of Colon and Rectal Surgeons, the International Continence Society, the American Urogynecologic Society, and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction. Dis Colon Rectum. 2020;63(01):6–23. doi: 10.1097/DCR.0000000000001529. [DOI] [PubMed] [Google Scholar]
- 46.Barber M D, Kuchibhatla M N, Pieper C F, Bump R C. Psychometric evaluation of 2 comprehensive condition-specific quality of life instruments for women with pelvic floor disorders. Am J Obstet Gynecol. 2001;185(06):1388–1395. doi: 10.1067/mob.2001.118659. [DOI] [PubMed] [Google Scholar]