

Abstract
In alcohol use disorder, drinking cessation is frequently associated with an alcohol withdrawal syndrome. Early in abstinence (within the first 2 months after drinking cessation), when patients do not exhibit physical signs of alcohol withdrawal syndrome anymore (such as nausea, tremor or anxiety), studies report various brain, sleep and cognitive alterations, highly heterogeneous from one patient to another. While the acute neurotoxicity of alcohol withdrawal syndrome is well-known, its contribution to structural brain alterations, sleep disturbances and neuropsychological deficits observed early in abstinence has never been investigated and is addressed in this study. We included 54 alcohol use disorder patients early in abstinence (from 4 to 21 days of sobriety) and 50 healthy controls. When acute physical signs of alcohol withdrawal syndrome were no longer present, patients performed a detailed neuropsychological assessment, a T1-weighted MRI and a polysomnography for a subgroup of patients. According to the severity of the clinical symptoms collected during the acute withdrawal period, patients were subsequently classified as mild alcohol withdrawal syndrome (mild-AWS) patients (Cushman score ≤ 4, no benzodiazepine prescription, N = 17) or moderate alcohol withdrawal syndrome (moderate-AWS) patients (Cushman score > 4, benzodiazepine prescription, N = 37). Patients with severe withdrawal complications (delirium tremens or seizures) were not included. Mild-AWS patients presented similar grey matter volume and sleep quality as healthy controls, but lower processing speed and episodic memory performance. Compared to healthy controls, moderate-AWS patients presented non-rapid eye movement sleep alterations, widespread grey matter shrinkage and lower performance for all the cognitive domains assessed (processing speed, short-term memory, executive functions and episodic memory). Moderate-AWS patients presented a lower percentage of slow-wave sleep, grey matter atrophy in fronto-insular and thalamus/hypothalamus regions, and lower short-term memory and executive performance than mild-AWS patients. Mediation analyses revealed both direct and indirect (via fronto-insular and thalamus/hypothalamus atrophy) relationships between poor sleep quality and cognitive performance. Alcohol withdrawal syndrome severity, which reflects neurotoxic hyperglutamatergic activity, should be considered as a critical factor for the development of non-rapid eye movement sleep alterations, fronto-insular atrophy and executive impairments in recently detoxified alcohol use disorder patients. The glutamatergic activity is involved in sleep-wake circuits and may thus contribute to molecular mechanisms underlying alcohol-related brain damage, resulting in cognitive deficits. Alcohol withdrawal syndrome severity and sleep quality deserve special attention for a better understanding and treatment of brain and cognitive alterations observed early in abstinence, and ultimately for more efficient relapse prevention strategies.
Keywords: alcohol use disorder, alcohol withdrawal syndrome, sleep, brain structure, cognition
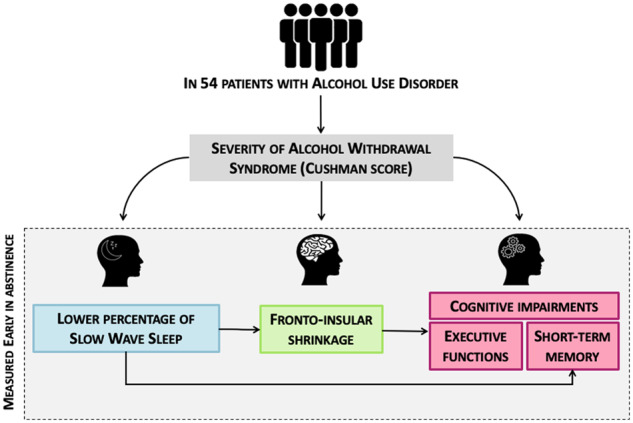
Even in the absence of severe alcohol withdrawal syndrome, moderate alcohol withdrawal syndrome was associated with a lower percentage of slow-wave sleep, which related to cognitive deficits both directly and indirectly via grey matter shrinkage. Alcohol withdrawal syndrome severity seems to contribute to the pathophysiology of brain, sleep and cognitive damage in alcohol use disorder patients.
Graphical Abstract
Graphical Abstract.
Introduction
In alcohol use disorder (AUD) patients, cessation of alcohol consumption is frequently associated with several clinical symptoms (tremor, nausea, anxiety, insomnia, etc.) that constitutes the alcohol withdrawal syndrome (AWS; American Psychiatric Association, 2013). The severity of AWS is variable in AUD patients, ranging from a mild clinical form to severe neurological complications such as seizures and delirium tremens, potentially leading to death (Jesse et al., 2017). From a neurobiological perspective, AWS results from a brain hyperexcitability due to increased glutamate transmission combined with decreased GABA transmission (De Witte et al., 2003). This excessive brain glutamate release is neurotoxic and has important consequences on brain functioning, mainly underlying the acute symptomatology of AWS (Tsai and Coyle, 1998; Lukoyanov et al., 1999; Kühn et al., 2014; Frischknecht et al., 2017).
This cerebral hyperexcitability is also known to be related to sleep abnormalities, which can persist several months after alcohol cessation and increase the risk of relapse (Begleiter and Porjesz, 1979; Chakravorty et al., 2016). Early in abstinence (from 2 to 8 weeks after detoxification, when acute physical symptoms of alcohol withdrawal are no more present), sleep abnormalities can be observed and consist of increased sleep latency and fragmentation, decreased sleep duration and sleep efficiency (defined as the ratio between time spent asleep and time in bed) as well as a decreased percentage of stage 3 (N3) of Non-rapid eye movement (NREM) sleep, also named slow-wave sleep (Heilig et al., 2010; Angarita et al., 2016). The potential alteration of rapid eye movement (REM) sleep is still debated (Gillin et al., 1990; Chakravorty et al., 2016).
Structural brain alterations and cognitive deficits have been well-described (Zahr et al., 2017) in recently sober AUD patients. Neuroimaging studies reported grey matter (GM) alterations mainly affecting two brain networks: the fronto-cerebellar (Kelly and Strick, 2003) and Papez circuits (Aggleton, 2012), which are involved in motor and executive abilities, and episodic memory, respectively. As a result, a large number of recently detoxified AUD patients present neuropsychological deficits including executive, working memory and episodic memory impairments (Stavro et al., 2013; Le Berre et al., 2017). The extent of these cognitive alterations is extremely variable. Some patients have preserved abilities, others exhibit mild-to-moderate deficits and others present severe impairments. This heterogeneity observed in the severity of AUD-related brain and cognitive deficits could be explained by several factors, such as demographical variables (Bates et al., 2002; Nolen-Hoeksema, 2004; Oscar-Berman et al., 2004), alcohol-related history (Zahr and Sullivan, 2008; Ritz et al., 2016), malnutrition and thiamine deficiency (Zahr and Sullivan, 2008; Pitel et al., 2011), liver disease (Junghanns et al., 2004; Ritz et al., 2016) and repeated alcohol withdrawals (Kouimtsidis et al., 2019).
Several studies reported that AUD patients who experienced multiple detoxifications (two or more) have more severe executive and decision-making deficits (Duka et al., 2003, 2011; Loeber et al., 2009), emotional impairments (Townshend and Duka, 2003; O’Daly et al., 2012), increased craving and anxiety-levels (Loeber et al., 2010), brain functional connectivity abnormalities (O’Daly et al., 2012) and altered cognitive recovery (Loeber et al., 2010) compared to patients with none or only one previous withdrawal. Beyond the frequency of alcohol-withdrawal experiences, AWS severity may contribute to the heterogeneity of altered brain structure and function observed in AUD patients. To date, studies mainly focused on the identification of clinical predictors to prevent the development of severe AWS (Goodson et al., 2014; Kim et al., 2015; Silczuk and Habrat, 2020). These investigations highlighted the role of the alcohol consumption level and the number of previous detoxifications (Duka et al., 2004) in the development of seizures and/or delirium tremens. To our knowledge, little is known regarding the effect of mild-to-moderate AWS on cognitive performance, GM volume and sleep quality in recently detoxified AUD patients.
The aim of the present study was thus to explore whether, even in absence of delirium tremens and/or seizures, AWS severity contributes to the heterogeneity of cognitive deficits, brain alterations and sleep changes observed in recently detoxified AUD patients.
Materials and methods
Participants
One hundred and four participants were included in this study: 54 AUD inpatients and 50 healthy controls (HC). None of them had a history of neurological, endocrinal, infectious diseases, depression [assessed using both the Beck Depression Inventory (BDI; Beck et al., 1961) and a psychiatric assessment] nor other forms of substance use disorder (except tobacco). All participants were informed about the study approved by the local ethics committee of Caen University Hospital (CPP Nord Ouest III, no. IDRCB: 2011-A00495-36) prior to their inclusion and provided their written informed consent. The study was conducted in France from 2016 to 2019.
AUD patients were recruited by clinicians while they were receiving withdrawal treatment as inpatients at Caen University Hospital. AUD patients met ‘alcohol dependence’ criteria according to the DSM-IV-TR [American Psychiatric Association (APA), 2000] or ‘severe AUD’ criteria according to the DSM-5 (American Psychiatric Association, 2013) for at least 5 years. HC were recruited to match the demographics (age, sex and education) of the AUD patients. They were interviewed with the Alcohol Use Disorder Identification Test (AUDIT; (Gache et al., 2005) to ensure that they did not meet the criteria for alcohol abuse (AUDIT <7 for men and <6 for women). None of the controls had a BDI (Gache et al., 2005) score >29 and a Mini-Mental State Examination (Folstein et al., 1975) score <26. Demographical data are presented in Table 1.
Table 1.
Demographic, clinical and alcohol-related data in healthy controls and AUD patients
| Healthy controls (HC) | Alcohol use disorder patients (AUD) |
Between-group comparisons | ||
|---|---|---|---|---|
| HC (N = 50) | mild-AWS (n = 17) | moderate-AWS (n = 37) | ||
| Demographics | ||||
| Age (years) | 44.02 ± 7.79 | 45.53 ± 11.36 | 46.86 ± 8.12 | NS |
| Education (years) | 12.30 ± 2.07 | 11.5 ± 2.18 | 11.69 ± 2.13 | NS |
| Sex ratio (M/F) | 34/16 | 13/4 | 31/6 | NS |
| Anxiety and depression factors | ||||
| BDI score* | 3.52 ± 3.99 | 12.29 ± 8.15 | 13.28 ± 8.96 | HC < mild-AWS†††; HC < moderate-AWS†††; mild-AWS = moderate-AWS |
| STAI-A (state anxiety)** | 26.52 ± 5.72 | 31.82 ± 11.97 | 32.05 ± 10.59 | HC = mild-AWS; HC < moderate-AWS††; mild-AWS = moderate-AWS |
| STAI-B (trait anxiety)** | 32.22 ± 6.84 | 49.18 ± 12.21 | 43.59 ± 11.28 | HC < mild-AWS†††; HC < moderate-AWS†††; mild-AWS = moderate-AWS |
| Alcohol history | ||||
| Abstinence before inclusion (days)* | 8.76 ± 3.73 | 11.22 ± 3.48 | Mild-AWS < moderate-AWS† | |
| AUDIT* | 2.60 ± 1.81 | 28.06 ± 5 | 28.89 ± 6.24 | HC < mild-AWS††† ; HC < moderate-AWS†††; mild-AWS = moderate-AWS |
| Daily alcohol consumption (units) | 15.63 ± 7.67 | 20.34 ± 8.39 | mild-AWS < moderate-AWS†,a | |
| Alcohol misuse (years) | 21.37 ± 10.16 | 20.62 ± 10.17 | NS | |
| Alcohol dependancy (years) | 13 ± 10.03 | 11.94 ± 11.47 | NS | |
| Alcohol withdrawal history | ||||
| Number of days between last benzodiazepines administration and inclusion | 2.78 ± 1.24 | |||
| Number of previous detoxifications | 1.94 ± 0.82 | 2.53 ± 1.70 | NS | |
| Highest Cushman score | 2.88 ± 0.92 | 5.86 ± 1.81 | Mild-AWS < moderate-AWS††† | |
| Total amount of benzodiazepine (equivalent diazepam) received (mg) | 0 ± 0 | 294.83 ± 221.82 | Mild-AWS < moderate-AWS††† | |
| Number of days of benzodiazepine prescription | 0 ± 0 | 9.05 ± 3.26 | Mild-AWS < moderate-AWS††† | |
HC = healthy controls; AUD = alcohol use disorder patients; mild-AWS (Cushman ≤ 4), moderate-AWS (Cushman >4 or the presence of a history of severe alcohol withdrawal history); BDI = Beck Depression scale.
Data were analysed using non-parametric tests for demographic, alcohol- and withdrawal-related variables and cognitive functions. Groups effects were tested with Kruskall–Wallis tests and post hoc comparisons were performed using Mann–Whitney U tests. We used a Chi2 test to compare the sex ratio in each group.
correlations between daily alcohol consumption on the one hand, and sleep quality, brain volume and cognitive abilities on the other hand were not significant neither in the entire group of AUD patients, nor in the two subgroups (data not shown).
Missing value for one patient.
Missing value for two patients.
NS = non-significant; †P < 0.05; ††P < 0.01; †††P < 0.001.
Experimental design
Assessment of AWS
All AUD inpatients included in this study underwent a symptom-triggered approach to the treatment of alcohol withdrawal, which requires to provide medication only when patients present alcohol-withdrawal symptoms (Saitz et al., 1994; Daeppen et al., 2002). The Cushman score was used to monitor the severity of AWS (Cushman et al., 1985), as recommended by the French Addiction Medicine Society and recognized by the European Federation of Addiction Societies (Société Française; SFA, 2017). This score takes the following clinical variables into account: hearth rate, systolic blood pressure, respiratory rate, tremor, sweating, agitation and sensorial disorders. Each variable is scored from 0 to 3 according to the severity of the symptom. The Cushman score refers to the sum of these subscores.
Alcohol withdrawal symptoms were systematically assessed every 4 h by the nursing staff supervised by a physician specialized in addiction medicine. When the Cushman score was, for the first time, superior or equal to 4, it was assessed a second time 30 min later to avoid false positive (e.g. caused by anxiety). When the Cushman score was higher than 4 twice in a row and/or when a history of severe alcohol withdrawal complications (seizure, delirium tremens) was known, a long-acting benzodiazepine with active metabolites (e.g. diazepam) was orally administered in order to alleviate AWS and prevent the development of a more severe AWS (Daeppen et al., 2002). In patients with hepatocellular or respiratory insufficiency, oxazepam was preferred to avoid over sedation or respiratory depression. A decrease in the benzodiazepine dosage was decided when the Cushman score was lower or equal to 2 for at least 24 h, at a rate of 15–30% of the total dose every 24–48 h.
AUD patients were classified into two groups according to the severity of AWS:
mild-AWS: a maximum Cushman score ≤4 and no benzodiazepine treatment required during the acute alcohol withdrawal period according to the symptom-triggered approach.
moderate-AWS: a maximum Cushman score >4 and/or the presence of a history of severe alcohol withdrawal complications resulting in a benzodiazepine administration during the acute alcohol withdrawal period.
None of the patients had undergone severe AWS defined by neurological complications such as delirium tremens or seizures during the acute withdrawal period examined in the course of the present study.
For all AUD patients, the maximum Cushman score and the number of previous detoxifications were collected. For patients whom benzodiazepines were prescribed, we also recorded the number of days and the total amount of benzodiazepines received during alcohol withdrawal. Alcohol-related variables and withdrawal history are summarized in Table 1.
Neuropsychological assessment
All participants underwent a detailed neuropsychological examination focusing on processing speed, short-term memory, executive functioning and episodic memory. Processing speed was measured with a composite score including the part A (time in seconds) of the Trail Making Test (Reitan, 1955) and the denomination condition (time in seconds) of the Stroop Test (Stroop, 1935). Short-term memory was assessed using verbal spans of the WAIS-III (Wechsler, 1997). For executive functions, a composite score was computed including performance on three tests assessing manipulation of information (verbal backward spans of the WAIS-III; Wechsler, 1997), inhibition (Stroop Test; Stroop, 1935) with the time in seconds needed to complete the interference condition minus time needed for the denomination condition, and mental flexibility (Modified Card Sorting Test, Cianchetti et al., 2005) with the number of perseverative errors. Two patients had missing data for one measure; their composite score assessing executive functions was therefore computed using remaining scores. Episodic memory was examined through the sum of the three free recalls of the French version of the Free and Cued Selective Reminding Test (Van der Linden et al., 2004). Neuropsychological data were transformed into z-scores using the mean and standard deviation obtained from the HC. The sign of all variables for which high scores were in the impaired direction (such as completion time or number of errors) was reversed so that all the z-scores had the same direction: higher z-scores reflecting better performance.
MRI data acquisition and preprocessing
Brain imaging examinations were conducted in 31 HC and 43 AUD patients (13 mild-AWS and 30 moderate-AWS) within the same week as the neuropsychological assessment. HC and the two subgroups of AUD patients were matched for age, sex and education level. All neuroimaging examinations were performed at Cyceron center (Caen, France).
A high-resolution T1-weighted anatomical image was acquired for each subject on a Philips Achieva 3T scanner (Philips Health-care/Philips Medical Systems International B.V., Eindhoven, the Netherlands) using a three-dimensional fast-field echo sequence (sagittal; repetition time, 20 ms; echo time, 4.6 ms; flip angle 10°; 180 slices; slice thickness: 1 mm; field of view 256 × 256 mm2; matrix, 256 × 256). The volumetric MRI data were analysed using the Statistical Parametric Mapping software (SPM12; Welcome Department of Cognitive Neurology, Institute of Neurology, London, UK). Preprocessing steps included segmentation of the MRI data into GM and spatial normalization to the Montreal Neurological Institute (MNI) template (voxel size = 1.5 mm3, matrix = 121 × 145 × 121). The normalized GM images were modulated by the Jacobian determinants to correct for non-linear warping so that the resulting brain volumes were corrected for brain size. The resulting images were smoothed by a Gaussian kernel of 8-mm full width at half maximum (FWHM). A GM mask was obtained taking the unmodulated GM images of HC normalized to the MNI space, averaging them, and thresholding the resultant mean image at 0.5. The resulting GM mask was applied to GM data analyses.
Sleep
A subgroup of 21 AUD (8 mild-AWS and 13 moderate-AWS) and 15 HC, matched for age, sex and education, underwent one night of polysomnography (PSG) using a portable recording device (Siesta®, Compumedics, Australia), allowing AUD patients to sleep at the addiction department and HC at their home. The PSG was conducted within the same week as the neuropsychological and MRI examinations. The PSG acquisition consisted of 20 EEG electrodes (Fp1, Fp2, F3, F4, F7, F8, T3, T4, C3, C4, P3, P4, O1, O2, FZ, CZ, PZ, vertex ground and a bi-mastoid reference) placed over the scalp according to the international 10–20 system, with impedances kept below 5 kΩ. We also recorded the electrooculogram (EOG), chin EMG, ECG, respiratory movements using abdominal and thoracic belts, respiratory airflow using nasal and oral thermistor, and oxygen saturation with a finger pulse oximeter. The EEG signal was digitalized at a sampling rate of 256 Hz. High-pass and low-pass filters were applied, respectively, at 0.3 and 35 Hz. PSG recordings were scored in 30-s epochs according to the American Association of Sleep Medicine (AASM, 2017) standard criteria. The following parameters were obtained: total sleep time (TST; in minutes), sleep efficiency [SE (%), corresponding to time spent asleep/time in bed], sleep onset latency (in minutes, referring to the time from lights-off to the first three epochs of any stage of sleep), wake after sleep onset (in minutes), time spent in each sleep stage (N1, N2, N3 and REM sleep, expressed as percentages of TST), arousal index (number of arousals/TST), stage shifts index (number of sleep stage transitions to N1/TST) and the Apnea-Hypopnea Index (AHI, corresponding to the number of respiratory events per hour of sleep). We also calculated a composite score to assess sleep fragmentation including the micro-arousal index, the arousal index and the number of stage transitions to N1.
All participants underwent a self-assessment of their sleep quality using the Pittsburg Sleep Quality Index (PSQI; Buysse et al., 1989) in its initial version (previous month) for HC and with an adapted version (previous week, to better reflect the different stages of alcohol treatment) for AUD patients. The Epworth Sleepiness Scale (ESS; Johns, 1991) was proposed to assess signs of daytime sleepiness in all participants.
Statistical analysis
To test the differences between HC and the two subgroups of AUD patients (mild-AWS and moderate-AWS), non-parametric Kruskall–Wallis’s tests were conducted on demographical variables (age and education) and a Chi2 test was performed to compare the sex ratio in each group. Mann–Whitney’s tests were performed between mild-AWS and moderate-AWS for alcohol- and withdrawal-related variables. Non-parametric Kruskall–Wallis’s tests were conducted on neuropsychological data and sleep measures followed by post hoc comparisons (Mann–Whitney’s tests) when appropriate. The statistical threshold was set to P < 0.05.
Neuroimaging data were analysed using SPM12 (Statistical Parametric Mapping, www.fil.ion.ucl.ac.uk/spm). More precisely, we conducted voxel-based ANCOVAs to compare GM volume between HC, mild-AWS and moderate-AWS patients, controlling for the intracranial volume. We corrected for multiple comparisons [family-wise error (FWE), P < 0.05] with a minimal cluster size (k) of 60 voxels (200 mm3). Then, comparisons between the two-subgroups of AUD patients were reported at P < 0.001 with a minimal cluster size (k) of 60 voxels (200 mm3). Only results surviving a cluster-level correction are reported.
Finally, the relationships between GM volume, sleep variables and cognitive performance were examined in the entire group of AUD patients with Spearman’s correlations. Only the variables for which we found a significant difference between mild-AWS and moderate-AWS were entered in the analyses. When we observed significant relationships between a sleep variable on the one hand and both a GM volume and a cognitive variable on the other hand, we performed causal mediation analyses to assess the directionality of the relationships. Mediations analyses allow to test whether the causal effect of an independent variable (X) on a dependent variable (Y) is explained by a mediating variable (M). In other words, X exerts its effects on Y because X affects M, which in turn, affects Y (Goldstone et al., 2018). Applied to our study, two models were tested to determine (i) whether GM volume mediates the relationships between sleep and cognitive performance or (ii) whether sleep mediates the relationships between GM volume and cognition. These analyses were performed using the ‘mediation’ R package (Tingley et al., 2014). We reported the average direct effects (ADE) and average causal mediation effect (ACME) estimated using non-parametric bootstrapping (5000 simulations, P < 0.05) for each model.
Data availability
All data and materials used within this study will be made available, upon reasonable request, to research groups wishing to reproduce/confirm our results.
Results
Comparisons between HC, mild-AWS and moderate-AWS patients
Demographical variables and anxiety-depression levels: Kruskall–Wallis tests with Group as a between-subject factor (HC, mild, moderate-AWS) did not reveal any significant effect of group for age [H(2,104) = 2.48, P = 0.29] and education [H(2,104) = 4.24, P = 0.12]. A Chi2-test showed that sex ratio was similar between groups (χ2 = 2.85, P = 0.24). Kruskall–Wallis tests showed a significant effect of group for depression [H(2,103) = 42, P < 0.0001], anxiety-state [H(2,102) = 8.55, P = 0.01] and anxiety-trait [H(2,102) = 32.83, P < 0.0001]. Mild-AWS and moderate-AWS were both more depressed than HC (all P-values < 0.0001) but did not differ from each other (P = 0.85). Only moderate-AWS differed from HC on the anxiety-state questionnaire (P = 0.004). Mild-AWS and moderate-AWS exhibited higher levels of anxiety-trait compared to HC (all P-values < 0.0001), but did not differ from each other (P = 0.14). Results are presented in Table 1.
Alcohol-related variables
A Kruskall–Wallis test showed a significant effect of group for the AUDIT score [H(2,103) = 76.97, P < 0.0001]. Post hoc comparisons revealed, as expected, that mild-AWS and moderate-AWS patients presented higher AUDIT scores than HC (all P-values = 0.0001) but did not differ from each other (P = 0.41). Mann–Whitney U tests did not show any significant difference between mild-AWS and moderate-AWS for the duration of alcohol misuse (U = 279.5, P = 0.73) and dependence (U = 265, P = 0.44), but moderate-AWS reported a higher daily alcohol consumption than mild-AWS patients (U = 191.5, P = 0.05; Table 1).
Alcohol withdrawal variables
Mild-AWS and moderate-AWS patients had an equivalent number of previous detoxifications (U = 265.5, P = 0.44). As expected, compared to mild-AWS patients, moderate-AWS patients had experienced a higher maximum Cushman score (U = 35.5, P < 0.0001), had received more diazepam (U = 0, P < 0.0001) and during a longer period (U = 0, P < 0.0001; Table 1).
Pattern of cognitive alterations
Kruskall–Wallis tests revealed a significant effect of group for processing speed [H(2, 104) = 29.7, P < 0.0001], short-term memory [H(2, 103) = 12.68, P = 0.002], executive functions [H(2, 104) = 23.38, P < 0.0001] and episodic memory [H(2, 104) = 22.32, P < 0.0001]. Post hoc comparisons indicated that mild-AWS patients presented lower performance than HC for episodic memory (U = 148, P < 0.0001) and processing speed (U = 177, P = 0.0004), but not for short-term memory (U = 422, P = 0.97) and executive performance (U = 384.5, P = 0.56). Compared to HC, moderate-AWS patients presented lower performance for all cognitive measures (all P-values < 0.001). Compared to mild-AWS patients, moderate-AWS patients had lower executive (U = 154, P = 0.003) and short-term memory performance (U = 178. 5, P = 0.01), but did not differ for processing speed and episodic memory (all P-values > 0.05; Table 2 and Fig. 1).
Table 2.
Cognitive performance and sleep variables in healthy controls and AUD patients
| Healthy controls (HC) | Alcohol Use Disorder patients (AUD) |
Between-group comparisons | ||
|---|---|---|---|---|
| HC (N = 50) | Mild-AWS (n = 17) | Moderate-AWS (n = 37) | ||
| Cognitive functions (z-score) | ||||
| Processing speed | 0 ± 1 | −0.62 ±1.13 | −0.97 ± 1.49 | HC > mild-AWS†††; HC > moderate-AWS†††; mild-AWS = moderate-AWS |
| Short-term memory | 0 ± 1 | −0.007 ± 0.93 | −0.82 ± 1.09 | HC = mild-AWS; HC > moderate-AWS†††; mild-AWS > moderate-AWS†† |
| Executive functions | 0 ± 0.64 | −0.13 ± 0.62 | −1.15 ± 1.40 | HC = mild-AWS; HC > moderate-AWS†††; mild-AWS > moderate-AWS† |
| Episodic memory* | 0 ± 1 | −1.12 ± 0.80 | −0.95 ±1.25 | HC > mild-AWS†††; HC > moderate-AWS†††; mild-AWS = moderate-AWS |
| Sleep architecturea | ||||
| Sleep latency (min) | 29.07 ± 17.71 | 14.06 ± 14.18 | 24.81 ± 15.11 | NS |
| Total sleep time (min) | 384.57 ± 53.75 | 376.87 ± 61.48 | 381.73 ± 69.30 | NS |
| Sleep efficiency (%) | 80.95 ± 6.87 | 88.54 ± 8.72 | 80.78 ± 7.54 | NS |
| Wake after sleep onset (min) | 61.03 ± 31.53 | 37.19 ± 34.14 | 64.23 ± 40.65 | NS |
| N1(%) | 11.15 ± 5.22 | 14.31 ± 5.72 | 20.91 ± 8.19 | HC = mild-AWS; HC > moderate-AWS†††; mild-AWS = moderate-AWS |
| N2 (%) | 46.49 ± 8.53 | 41.7 ± 5.78 | 45.63 ± 9.39 | NS |
| N3 (%) | 20.56 ± 8.15 | 20.08 ± 5.55 | 10.71 ± 4.60 | HC = mild-AWS; HC > moderate-AWS†††; mild-AWS > moderate-AWS†† |
| REM (%) | 21.79 ± 5.50 | 23.85 ± 6.41 | 22.75 ± 4.19 | NS |
| Apnea-hypopnea Index (AHI) | 13.59 ± 8.16 | 24.82 ± 13.57 | 26.77 ± 16.71 | HC < mild-AWS†; HC < moderate-AWS†; mild-AWS = moderate-AWS |
| Composite sleep fragmentation | 0 ± 0.85 | −0.33 ± 0.96 | −0.85 ± 1.18 | NS |
| Subjective sleep assessmenta | ||||
| PSQI total score** | 2.13 ± 1.35 | 7 ± 4.9 | 5.9 ± 2.64 | HC = mild-AWS; HC < moderate-AWS††; mild-AWS = moderate-AWS |
| ESS total score | 4.78 ± 2 | 6.37 ± 2.33 | 3.92 ± 2.56 | NS |
See legend of Table 1. PSQI = Pittsburgh Sleep Quality Index; ESS = Epworth Severity Scale.
Data were analysed using non-parametric tests: groups effects were tested with Kruskall–Wallis tests and post hoc comparisons were performed using Mann–Whitney U test.
For sleep analyses, subgroups consisted of 15 HC, 8 mild-AWS and 13 moderate-AWS patients.
Missing data for one patient.
Missing data for six AUD patients. NS: non-significant.
P < 0.05;
P < 0.01;
P < 0.001.
Figure 1.
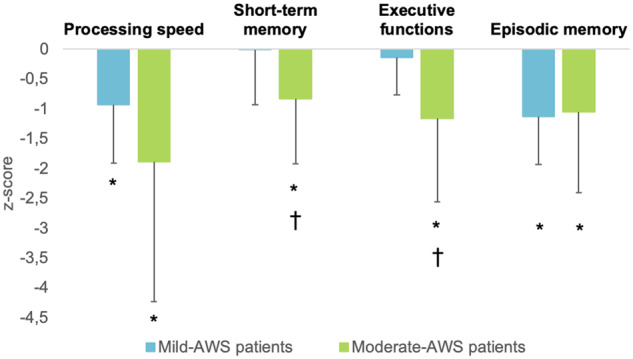
Neuropsychological performance according to the severity of the alcohol withdrawal syndrome. Z-scores were computed based of the mean and standard deviation of the HC (mean = 0; standard deviation = 1). *Significant difference compared to HC. †Significant difference compared to mild-AWS patients.
Pattern of GM alterations
Mild-AWS patients did not differ from HC regarding GM volume [P(FWE) < 0.05; Fig. 2A]. Compared to HC, moderate-AWS patients had significantly lower GM volume in frontal and prefrontal areas, insula, lateral and medial temporal cortices (including the hippocampus and parahippocampal gyrus), cingulate and occipital cortices, cerebellum, and in subcortical regions including the thalamus, putamen and caudate nuclei [P(FWE) < 0.05; Fig. 2B]. Compared to mild-AWS patients, moderate-AWS patients had significantly lower GM volume in the right inferior frontal cortex (Broadman area 44), the bilateral insula, a cluster encompassing the anterior cingulate cortex and the medial superior frontal cortex, occipito-parietal regions and limbic structures including the anterior part of the thalamus and the hypothalamus. All regions listed above are significant at P < 0.001 (uncorrected) threshold and survived the cluster-level correction (P < 0.05; Fig. 2C). The reverse comparison (mild-AWS patients < moderate-AWS patients) did not reveal any significant result.
Figure 2.

Structural brain abnormalities in AUD patients with mild and moderate alcohol withdrawal syndrome (AWS) compared to controls. (A) Absence of grey matter (GM) atrophy in mild-AWS patients compared to healthy controls (HC). (B) Pattern of GM atrophy in moderate-AWS patients compared to HC. Results are presented at P < 0.05 corrected for family-wise-error (FWE). (C) Brain areas showing lower GM volume in AUD-moderate patients compared to AUD-mild patients. Results are presented at P < 0.001 (uncorrected) but only results surviving a cluster-level correction are reported. Minimum cluster size: >60 voxels.
Pattern of sleep alterations
Non-parametric Kruskall–Wallis tests revealed a significant effect of group for both percentage of sleep stages N1 [H (2,N= 36) = 11.81 P = 0.003] and N3 [H (2,N= 36) = 15.87 P = 0.0004]. Post hoc comparisons (Mann–Whitney U tests) showed that compared to HC, mild-AWS patients had similar percentage of N1 (P = 0.24) and N3 sleep (P = 0.52). Compared to HC, moderate-AWS patients showed higher percentage of N1 (P = 0.0006) and lower percentage of N3 sleep (P = 0.0002). Compared to mild-AWS patients, moderate-AWS patients showed lower percentage of N3 sleep (P = 0.004; Table 2 and Fig. 3).
Figure 3.
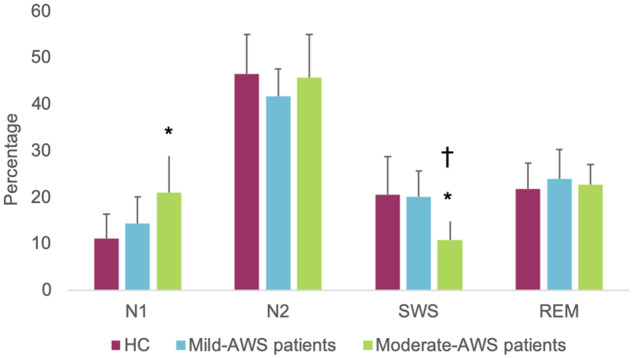
Time spent in each sleep stage expressed as a percentage of total sleep time according to the severity of the alcohol withdrawal syndrome. *Significant difference compared to HC. †Significant difference compared to mild-AWS patients.
A significant effect of group was observed for the apnea-hypopnea index (AHI) (H (2,N= 36) = 7.99 P = 0.02). Post hoc comparisons showed that mild-AWS patients and moderate-AWS patients exhibited a higher AHI compared to controls (P = 0.03 and P = 0.01, respectively) but did not differ from each other (P > 0.05). No group differences were observed for sleep latency, duration, efficiency and wake after sleep onset (all P-values > 0.05). Results remained unchanged when controlling for the AHI (data not shown).
A significant effect of group was observed for the PSQI score [H(2,N= 30) = 11.19, P = 0.004]. Post hoc comparisons showed that compared to HC, moderate-AWS patients had a higher score (P = 0.001). Mild-AWS patients did not differ from HC and moderate-AWS patients (all P-values > 0.05). No group difference was observed on the ESS score (P-value > 0.05; Table 2).
Relationships between GM volume, sleep and cognitive performance in the entire group of AUD patients
Signal values within the significant clusters obtained from the comparison mild-AWS > moderate-AWS were extracted. Then, we conducted Spearman’s correlations between GM volumes, sleep variables and cognitive performance in the entire group of patients. Only variables for which we found a significant difference between mild-AWS and moderate-AWS patients were entered in these analyses (i.e. short-term memory performance, executive abilities and N3 sleep). Short-term memory performance positively correlated with GM volume in the insula (rho = 0.51, P = 0.01), occipito-parietal cortex (rho = 0.62, P = 0.003), inferior frontal gyrus (rho = 0.45, P = 0.04) and thalamus/hypothalamus (rho = 0.45, P = 0.04), but not in the anterior cingulate cortex (P > 0.05). Executive performance positively correlated with all significant clusters of GM volume (insula: rho = 0.7, P = 0.0004; occipito-parietal cortex: rho = 0.66, P = 0.001; anterior cingulate cortex: rho = 0.57, P = 0.007; inferior frontal gyrus: rho = 0.53, P = 0.01; thalamus/hypothalamus: rho = 0.64, P = 0.002). GM volume in all significant clusters positively correlated with the percentage of N3 sleep (insula: rho = 0.52, P = 0.01; occipito-parietal cortex: rho = 0.55, P = 0.009; anterior cingulate cortex: rho = 0.43, P = 0.05; inferior frontal gyrus: rho = 0.56, P = 0.008; thalamus/hypothalamus: rho = 0.51, P = 0.02). Moreover, the percentage of N3 sleep positively correlated with short-term memory (rho = 0.48, P = 0.03) and executive performance (rho = 0.44, P = 0.04).
To better understand the directionality of the relationships between GM volume, N3 sleep and cognitive performance, we conducted mediation analyses and tested two models for each cluster. In the first one (Model 1), N3 sleep was the independent variable (X) and GM volume in the five significant clusters reported in the previous analysis was the mediator (M). In the second model (Model 2), GM volume was the independent variable (X) and N3 sleep was the mediator (M). In both models, cognitive variables (short-term memory or executive scores) were entered as the dependent variable (Y). First, considering short-term memory performance as the dependent variable, mediation analyses referring to both Models 1 and 2 were not significant (P > 0.05; Supplementary Table 1). Second, considering executive functions performance as the dependent variable, mediation analyses revealed that the volume of the bilateral insula (P = 0.006), right inferior frontal cortex (P = 0.02), occipito-parietal cortex (P = 0.01) and the cluster including the anterior thalamus and the hypothalamus (P = 0.02) significantly mediated the relationships between the percentage of N3 sleep and executive performance. None of the analyses referring to Model 2 was significant. Results of these mediation analyses are detailed in Table 3 and Fig. 4.
Table 3.
Mediation analyses between % N3 sleep, GM volumes and executive functioning in AUD patients
| ADE | ACME | ||||||
|---|---|---|---|---|---|---|---|
| Brain areas | Model | Estimate | CI95% | P -value | Estimate | CI95% | P-value |
| Bilateral insula | Model 1 | 0.02 | −0.03–0.09 | 0.47 | 0.04 | 0.01–0.09 | 0.006* |
| Model 2 | 7.05 | 3.01–9.91 | 0.003 | 0.69 | −1.18–3.61 | 0.46 | |
| Right inferior frontal gyrus | Model 1 | 0.02 | −0.05–0.10 | 0.51 | 0.04 | 0.004–0.010 | 0.02* |
| Model 2 | 5.98 | 0.92–10.95 | 0.02 | 0.99 | −3.06–4.34 | 0.56 | |
| Cingulate anterior gyrus | Model 1 | 0.04 | −0.02–0.11 | 0.22 | 0.02 | −0.007–0.07 | 0.11 |
| Model 2 | 3.57 | −0.83–7.37 | 0.08 | 1.15 | −1.01–4.13 | 0.24 | |
| Anterior thalamus/hypothalamus | Model 1 | 0.02 | −0.04–0.10 | 0.47 | 0.03 | 0.004–0.10 | 0.02* |
| Model 2 | 5.71 | 1.56–10.23 | 0.008 | 0.90 | −2.16–3.23 | 0.47 | |
| Occipito-parietal cortex | Model 1 | 0.02 | –0.04–0.09 | 0.56 | 0.05 | 0.008–0.10 | 0.02* |
| Model 2 | 7.77 | 1.82–12.74 | 0.02 | 0.96 | −2.95–4.98 | 0.54 |
ADE = average direct effect; ACME = average causal mediation effect; CI = confidence interval.
For the five GM clusters, two models were tested. In the first one (Model 1), the percentage of N3 sleep was the independent variable and the GM volume was the mediator. In the second model (Model 2), GM volume was the independent variable and the percentage of N3 sleep was the mediator. In all models, executive functions were entered as the dependent variable. Values in bold accompanied by a ‘*’ indicate the significance of the model.
Figure 4.
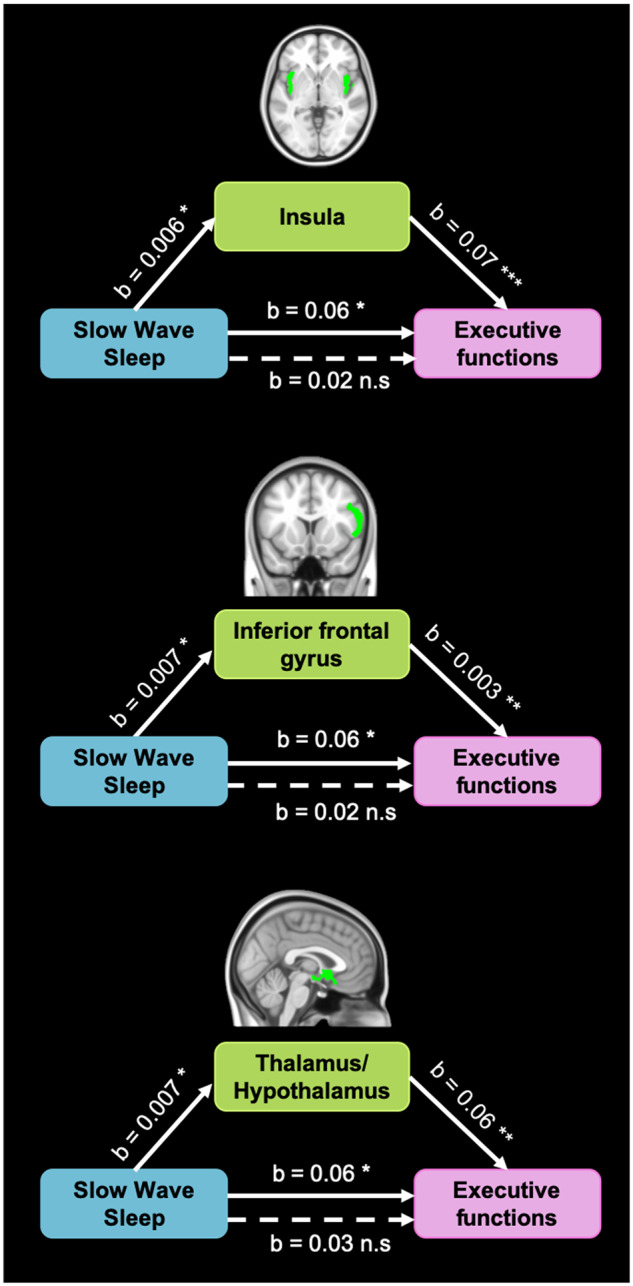
Results of mediation analyses showing that brain volume mediates the relationships between sleep and executive functions in recently detoxified AUD patients. Direct effects in filled arrows and indirect effects were represented in dotted arrows (when the effect of brain volume is partially out). *P < 0.05; **P < 0.01; ***P < 0.001. n.s., non-significant.
Discussion
The present study aimed at determining whether AWS severity contributes to the heterogeneity of sleep changes, brain alterations and cognitive deficits observed in AUD patients early in abstinence. We showed that AWS severity contributes to the pathophysiology of NREM sleep abnormalities, decrease GM volumes in fronto-insular and thalamus/hypothalamus regions as well as short-term memory and executive deficits in AUD patients early in abstinence. We also found that lower percentage of N3 sleep related to cognitive deficits (short-term memory and executive functions) both directly and indirectly via GM shrinkage in AUD patients.
We showed that 68% of AUD patients exhibited a moderate-AWS, which is a higher prevalence than the one reported in a previous study (Mirijello et al., 2015). In the present study, all patients were recruited in a special unit for alcohol detoxification. They were thus potentially at risk for AWS complications. Contrary to a previous study (Duka et al., 2004) in which only patients with severe alcohol withdrawal complications were included, we did not observe any association between multiple detoxifications and the severity of the current AWS. We also found that AUD patients with moderate-AWS reported higher alcohol consumption during the month preceding withdrawal than those with mild-AWS. This result suggests that during withdrawal, the brain hyperexcitability resulting from increased glutamate transmission combined to decreased GABA transmission may be related to the quantity of recent alcohol drinking (De Witte et al., 2003; Jesse et al., 2017).
Our study first confirms the pattern of sleep alterations observed in recently detoxified AUD patients, consisting of increased light sleep (N1), a lower percentage of N3 sleep (Gillin et al., 1990; Junghanns et al., 2009; de Zambotti et al., 2014, Irwin et al., 2016a; Singh et al., 2018) and the presence of a sleep complaint (Laniepce et al., 2019). It also specifies that only patients with moderate-AWS presented these objective sleep alterations, as well as self-reported sleep difficulties. The difference observed between moderate- and mild-AWS patients for N3 sleep is in accordance with a previous study showing that the number of alcohol withdrawal symptoms was negatively related to the percentage of N3 sleep (Gillin et al., 1990). Sleep changes may be directly related to AWS severity since N3 sleep has been associated with lower glutamate levels (Dash et al., 2009). Even when the clinical symptoms of AWS have faded, a hyper-glutamate activity may persist and alter brain regions involved in the generation and maintenance of sleep rhythms, resulting in lower percentage of N3 sleep (Dang-Vu, 2012). Sleep abnormalities observed in our group of moderate-AWS patients may thus be interpreted as a persistent subacute alcohol withdrawal symptom (Brower, 2001; Feige et al., 2007).
AWS severity was also related to structural brain alterations in the right inferior frontal cortex, the bilateral insula, the anterior cingulate cortex and the thalamus/hypothalamus, which are brain regions known to be affected in AUD patients (Pitel et al., 2012; Yang et al., 2016). Regarding the effect of AWS severity on the anterior cingulate cortex, studies using magnetic resonance spectroscopy reported increased glutamate levels in this brain region during alcohol withdrawal in both humans and rats (Lee et al., 2007; Hermann et al., 2012). Several studies suggested that the extent of structural brain abnormalities in AUD patients may be partially explained by alcohol withdrawal-related toxicity (De Witte et al., 2003; Duka et al., 2011; O’Daly et al., 2012; Trick et al., 2014; Frischknecht et al., 2017). During alcohol withdrawal, the glutamate-mediated excitotoxicity induces neuronal death, which may explain structural brain alterations observed early in abstinence in AUD patients (Tsai and Coyle, 1998). The frontal lobes being particularly rich in glutamatergic pathways (Kril et al., 1997), they are likely to be especially vulnerable to the severity of AWS. However, we do not exclude that these brain alterations may have been present before alcohol cessation because of the effects of chronic and heavy alcohol consumption or a family history of AUD or comorbidities such as liver disease or thiamine deficiency (Harper, 2009; Chen et al., 2012; Filippi et al., 2019). In this case, altered brain structure would constitute a vulnerability factor for exhibiting more severe AWS. Further studies including longitudinal measures of glutamate levels combined with structural MRI at different stages of the disease (active drinking, withdrawal period and abstinence) are now required.
Regarding cognitive abilities, our findings indicate that AWS severity may have deleterious effects on short-term memory and executive performance. While short-term memory deficits have previously been reported in AUD patients (Pitel et al., 2007), we suggest here that AWS may contribute to this alteration. Executive dysfunctions are frequent in AUD patients early in abstinence (Stavro et al., 2013) and could notably be influenced by alcohol history (Sullivan et al., 2000; Zinn et al., 2004; Maurage et al., 2014), associated liver disease (Ritz et al., 2016) and multiple detoxifications (Duka et al., 2004; Loeber et al., 2009). The present study suggests that beyond the repetition of alcohol withdrawals, the severity of AWS itself may represent another factor influencing the heterogeneity of executive impairments in AUD patients. By contrast, AWS severity does not appear to modulate processing speed and episodic memory deficits. Indeed, episodic memory was affected to the same extent in the two subgroups of patients. Previous studies suggested that episodic memory abilities may rather be influenced by thiamine metabolism (Pitel et al., 2011; Ritz et al., 2016).
Mediation analyses enabled us to deepen our understanding of the relationships between sleep, brain and cognition considering the severity of AWS. For the first time, we showed that poor restorative sleep (reflected by a lower percentage of N3 sleep) is related to cognitive deficits both directly and indirectly through GM shrinkage. In line with a previous study in sleep-deprived individuals (Chengyang et al., 2017), we demonstrated that poor restorative sleep is associated with short-term memory deficits in AUD patients. This relationship was not mediated by GM alterations, suggesting the potential contribution of other mechanisms such as altered functional activity of hippocampal-cortical circuits (Chengyang et al., 2017). Interestingly, we found that poor restorative sleep contributes to fronto-insular shrinkage that in turn results in executive deficits. Our results suggest a potential role of sleep in the pathophysiological mechanisms of alcohol-related GM alterations in AUD patients. Poor sleep quality may result from alcohol-related brain damage such as increased glutamate levels (Cortese et al., 2010), neuroinflammation (Irwin et al., 2016b) and oxidative stress (Villafuerte et al., 2015). These mechanisms may contribute to fronto-insular and thalamic/hypothalamic abnormalities in AUD patients recently detoxified. Fronto-insular regions, such as the right inferior frontal gyrus, have been related to executive deficits, notably during inhibition tasks (Levy and Wagner, 2011; Aron et al., 2014; Wiers et al., 2015). The insula promotes the integration and representation of interoceptive information into conscious feelings and viscerosensory signals leading to decision-making (Craig, 2009). The insula being also a neuronal substrate of craving, insular shrinkage may underpin the relationship between sleep alterations and relapse (Brower, 2003). Thus, these analyses seem to explain, at least partially, the potential associations existing between sleep, brain and cognition in AUD patients, by showing that N3 sleep contributes to GM shrinkage in fronto-insular and thalamus/hypothalamus regions resulting in executive deficits. We do not exclude that, on the contrary, alterations in other brain regions may induce sleep abnormalities that, in turn, underlie cognitive functioning.
The present study has several strengths, including a meticulous collection of information about AWS severity associated with a detailed cognitive assessment, an MRI scan and an objective sleep assessment in AUD patients examined early in abstinence. However, several limitations should be mentioned. First, the results of the present study were obtained in AUD patients without comorbidities nor other forms of substance use disorder (except tobacco). They cannot therefore be generalized to all AUD patients in Addiction departments given the frequency of comorbidities and multiple drug use. Second, all participants performed only one night of PSG-recording, which did not allow to control for ‘the first-night effect’. Third, although none of the AUD patients included in the present study fulfilled diagnostic criteria for current anxiety disorder and/or depression, higher self-report anxiety and depressive levels were reported by AUD patients compared to HC. Psycho-affective factors may influence sleep quality and cognitive performance in AUD patients as these factors are known to have a negative impact on neuropsychological abilities (Gualtieri and Morgan, 2008) and sleep quality (Baglioni et al., 2016). Nevertheless, the two groups of AUD patients did not differ from each other on these variables and results remained unchanged when psycho-affective factors (BDI, STAI-A, STAI-B scores) were added as covariates (data not shown). Finally, the current clinical measure of AWS severity makes it difficult to disentangle the direct effect of pathophysiological mechanisms underlying AWS (hyperglutamatergy) from the potential effect of AWS-related benzodiazepine treatment. AWS severity was treated with benzodiazepines, corresponding to the gold-standard for AWS treatment (Amato et al., 2010). Benzodiazepines are known to alter objective sleep quality and cognitive functions after an acute administration (Huron et al., 2001; Deakin et al., 2004; Roux and Kryger, 2010) and/or after a chronic consumption (Barker, 2004; Doghramji and Jangro, 2016; Fond et al., 2018). In the present study, AUD patients with benzodiazepine dependence prior the hospitalization were not included and patients who needed benzodiazepines during withdrawal were prescribed for only a few days (4–17 days). In addition, patients were included at least 48 h after the last benzodiazepine prescription (according to the half-life of the benzodiazepine used), after a progressive decrease of the benzodiazepine dosage starting when the Cushman score was lower or equal to 2 for at least 24 h, at a rate of 15–30% of the total dose every 24–48 h. Since prolonged diazepam intake may increase its terminal elimination time, we conducted supplementary analyses that did not show any correlation between the number of days since the last benzodiazepine prescription and our main results (Supplementary Table 2). This absence of relationship suggests that the differences observed between mild- and moderate-AWS patients do not result from the residual effects of benzodiazepines. However, further studies are required to specify the effects of short-term prescription of benzodiazepines on sleep quality, GM volumes and cognition in AUD patients.
Taken together, our results bring new insights on the pathophysiological mechanisms of sleep, structural brain alterations and cognitive deficits observed in recently detoxified AUD patients, showing the contribution of AWS severity. Moreover, we added novel evidence that poor sleep quality may contribute to cognitive deficits directly or indirectly through increased GM shrinkage in AUD patients early in abstinence. Further studies aiming at exploring brain, sleep or cognition in AUD patients should consider AWS severity to limit the heterogeneity of the AUD sample. For clinicians, these results suggest that a careful monitoring of AWS is not only useful to prevent the development of severe AWS complications, but also to predict sleep alterations, brain damage and cognitive deficits associated with a poor treatment outcome.
Supplementary material
Supplementary material is available at Brain Communications online.
Supplementary Material
Acknowledgements
The authors are grateful to the Cyceron MRI staff members for their help with patients and imaging examination acquisition, and Coralie Lannuzel, Stéphane Rehel, Ludivine Ritz and Hélène Beaunieux for their help at various stages of the study. We would also like to thank all the participants.
Funding
This work was supported by the French National Institute for Health and Medical Research (INSERM), the French National Agency for Research (ANR) and Conseil Regional de Normandie. A.L.’s doctoral fellowship was co-funded by European Union in the framework of the ERDF-ESF Operational Programme 2014–20 and Lundbeck.
Competing interests
The authors report no competing interests.
Glossary
- AASM =
American Association of Sleep Medicine
- ACME =
average causal mediation effect
- ADE =
average direct effects
- AHI =
Apnea-Hypopnea Index
- AUD =
alcohol use disorder
- AUDIT =
alcohol use disorder identification test
- AWS =
alcohol withdrawal syndrome
- BDI =
Beck Depression Inventory
- DSM =
diagnostic and statistical manual of mental disorders
- ESS =
Epworth Sleepiness Scale
- FWE =
Family-wise error
- FWHM =
full width at half maximum
- GM =
grey matter
- HC =
healthy controls
- MNI =
Montreal Neurological Institute
- NREM =
Non-rapid eye movement
- N1 =
stage 1
- N2 =
stage 2
- N3 =
stage 3
- PSG =
polysomnography
- PSQI =
Pittsburgh Sleep Quality Index
- REM =
rapid eye movement
- SE =
sleep efficiency
- SPM =
statistical parametric mapping
- STAI =
State-Trait Anxiety Inventory
- TST =
total sleep time
Contributor Information
Alice Laniepce, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Nicolas Cabé, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France; Service d’Addictologie, CHU Caen Normandie, 14000 Caen, France.
Claire André, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Françoise Bertran, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France; Unité d’exploration et de traitement des troubles du sommeil, CHU Caen Normandie, 14000 Caen, France.
Céline Boudehent, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France; Service d’Addictologie, CHU Caen Normandie, 14000 Caen, France.
Najlaa Lahbairi, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Angéline Maillard, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Alison Mary, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Shailendra Segobin, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
François Vabret, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France; Service d’Addictologie, CHU Caen Normandie, 14000 Caen, France.
Géraldine Rauchs, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France.
Anne-Lise Pitel, Normandie Univ, UNICAEN, PSL Université, EPHE, INSERM, U1077, CHU de Caen, GIP Cyceron, NIMH, 14000 Caen, France; Institut Universitaire de France (IUF), 75000 Paris, France.
References
- Aggleton JP. Multiple anatomical systems embedded within the primate medial temporal lobe: implications for hippocampal function. Neurosci Biobehav Rev 2012; 36: 1579–96. [DOI] [PubMed] [Google Scholar]
- Amato L, Minozzi S, Vecchi S, Davoli M. Benzodiazepines for alcohol withdrawal. Cochrane Database of Systematic Reviews 2010; Issue 3. Art. No.: CD005063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders, Fourth Edition, Text Revision (DSM-IV-TR). Arlington, VA: American Psychiatric Association; 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, Fifth edn. Arlington, VA: American Psychiatric Association; 2013. [Google Scholar]
- Angarita GA, Emadi N, Hodges S, Morgan PT. Sleep abnormalities associated with alcohol, cannabis, cocaine, and opiate use: a comprehensive review. Addict Sci Clin Pract 2016; 11: 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aron AR, Robbins TW, Poldrack RA. Inhibition and the right inferior frontal cortex: one decade on. Trends Cogn Sci 2014; 18: 177–85. [DOI] [PubMed] [Google Scholar]
- Baglioni C, Nanovska S, Regen W, Spiegelhalder K, Feige B, Nissen C, et al. Sleep and mental disorders: a meta-analysis of polysomnographic research. Psychol Bull 2016; 142: 969–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barker M. Persistence of cognitive effects after withdrawal from long-term benzodiazepine use: a meta-analysis. Arch Clin Neuropsychol 2004; 19: 437–54. [DOI] [PubMed] [Google Scholar]
- Bates ME, Bowden SC, Barry D. Neurocognitive impairment associated with alcohol use disorders: implications for treatment. Exp Clin Psychopharmacol 2002; 10: 193–212. [DOI] [PubMed] [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961; 4: 561–71. [DOI] [PubMed] [Google Scholar]
- Begleiter H, Porjesz B. Persistence of a “subacute withdrawal syndrome” following chronic ethanol intake. Drug Alcohol Depend 1979; 4: 353–7. [DOI] [PubMed] [Google Scholar]
- Brower KJ. Alcohol’s effects on sleep in alcoholics. Alcohol Res Health 2001; 25: 110–25. [PMC free article] [PubMed] [Google Scholar]
- Brower KJ. Insomnia, alcoholism and relapse. Sleep Med Rev 2003; 7: 523–39. [DOI] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research 1989; 28: 193–213. [DOI] [PubMed] [Google Scholar]
- Chakravorty S, Chaudhary NS, Brower KJ. Alcohol dependence and its relationship with insomnia and other sleep disorders. Alcohol Clin Exp Res 2016; 40: 2271–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen CH, Walker J, Momenan R, Rawlings R, Heilig M, Hommer DW. Relationship between liver function and brain shrinkage in patients with alcohol dependence. Alcohol Clin Exp Res 2012; 36: 625–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chengyang L, Daqing H, Jianlin Q, Haisheng C, Qingqing M, Jin W, et al. Short-term memory deficits correlate with hippocampal-thalamic functional connectivity alterations following acute sleep restriction. Brain Imaging Behav 2017; 11: 954–63. [DOI] [PubMed] [Google Scholar]
- Cianchetti C, Corona S, Foscoliano M, Scalas F, Sannio-Fancello G. Modified Wisconsin Card Sorting Test: proposal of a supplementary scoring method. Arch Clin Neuropsychol 2005; 20: 555–8. [DOI] [PubMed] [Google Scholar]
- Cortese BM, Mitchell TR, Galloway MP, Prevost KE, Fang J, Moore GJ, et al. Region-specific alteration in brain glutamate: Possible relationship to risk-taking behavior. Physiol Behav 2010; 99: 445–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craig AD. How do you feel—now? The anterior insula and human awareness. Nat Rev Neurosci 2009; 10: 59–70. [DOI] [PubMed] [Google Scholar]
- Cushman P, Forbes R, Lemer W, Stewart M. Alcohol withdrawal syndromes: clinical management with lofexidine. Alcoholism Clin Exp Res 1985; 9: 103–8. [DOI] [PubMed] [Google Scholar]
- SFA. Mésusage de l’alcool, dépistage, diagnostic, et traitement. Recommandation de bonne pratique. Princeps Éditions 2017; 37: 5-8.1 http://www.sfalcoologie.asso.fr/download/RBP2014-SFA-Mesusage-AA.pdf. [Google Scholar]
- Daeppen JB, Gache P, Landry U, Sekera E, Schweizer V, Gloor S, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomized treatment trial. Arch Intern Med 2002; 162: 1117–21. [DOI] [PubMed] [Google Scholar]
- Dang-Vu TT. Neuronal oscillations in sleep: Insights from functional neuroimaging. Neuromol Med 2012; 14: 154–67. [DOI] [PubMed] [Google Scholar]
- Dash MB, Douglas CL, Vyazovskiy VV, Cirelli C, Tononi G. Long-term homeostasis of extracellular glutamate in the rat cerebral cortex across sleep and waking states. J Neurosci 2009; 29: 620–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Witte P, Pinto E, Ansseau M, Verbanck P. Alcohol and withdrawal: from animal research to clinical issues. Neurosci Biobehav Rev 2003; 27: 189–97. [DOI] [PubMed] [Google Scholar]
- de Zambotti M, Baker FC, Sugarbaker DS, Nicholas CL, Trinder J, Colrain IM. Poor autonomic nervous system functioning during sleep in recently detoxified alcohol-dependent men and women. Alcohol Clin Exp Res 2014; 38: 1373–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deakin JB, Aitken MRF, Dowson JH, Robbins TW, Sahakian BJ. Diazepam produces disinhibitory cognitive effects in male volunteers. Psychopharmacology (Berl) 2004; 173: 88–97. [DOI] [PubMed] [Google Scholar]
- Doghramji K, Jangro WC. Adverse effects of psychotropic medications on sleep. Sleep Med Clin 2016; 11: 503–14. [DOI] [PubMed] [Google Scholar]
- Duka T, Gentry J, Malcolm R, Ripley TL, Borlikova G, Stephens DN, et al. Consequences of multiple withdrawals from alcohol. Alcohol Clin Exp Res 2004; 28: 233–46. [DOI] [PubMed] [Google Scholar]
- Duka T, Townshend JM, Collier K, Stephens DN. Impairment in cognitive functions after multiple detoxifications in alcoholic inpatients. Alcohol Clin Exp Res 2003; 27: 1563–72. [DOI] [PubMed] [Google Scholar]
- Duka T, Trick L, Nikolaou K, Gray MA, Kempton MJ, Williams H, et al. Unique brain areas associated with abstinence control are damaged in multiply detoxified alcoholics. Biol Psychiatry 2011; 70: 545–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feige B, Scaal S, Hornyak M, Gann H, Riemann D. Sleep electroencephalographic spectral power after withdrawal from alcohol in alcohol-dependent patients. Alcoholism Clin Exp Res 2007; 31: 19–27. [DOI] [PubMed] [Google Scholar]
- Filippi I, Hoertel N, Artiges E, Airagnes G, Guérin-Langlois C, Seigneurie A-S, et al. Family history of alcohol use disorder is associated with brain structural and functional changes in healthy first-degree relatives. Eur Psychiatr 2019; 62: 107–15. [DOI] [PubMed] [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state. J Psychiatr Res 1975; 12: 189–98. [DOI] [PubMed] [Google Scholar]
- Fond G, Berna F, Boyer L, Godin O, Brunel L, Andrianarisoa M, et al. ; The FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Benzodiazepine long-term administration is associated with impaired attention/working memory in schizophrenia: results from the national multicentre FACE-SZ data set. Eur Arch Psychiatry Clin Neurosci 2018; 268: 17–26. [DOI] [PubMed] [Google Scholar]
- Frischknecht U, Hermann D, Tunc-Skarka N, Wang G-Y, Sack M, van Eijk J, et al. Negative association between MR-spectroscopic glutamate markers and gray matter volume after alcohol withdrawal in the hippocampus: a translational study in humans and rats. Alcohol Clin Exp Res 2017; 41: 323–33. [DOI] [PubMed] [Google Scholar]
- Gache P, Michaud P, Landry U, Accietto C, Arfaoui S, Wenger O, et al. The Alcohol Use Disorders Identification Test (AUDIT) as a screening tool for excessive drinking in primary care: reliability and validity of a French version. Alcohol Clin Exp Res 2005; 29: 2001–7. [DOI] [PubMed] [Google Scholar]
- Gillin JC, Smith TL, Irwin M, Kripke DF, Schuckit M. EEG sleep studies in ‘pure’ primary alcoholism during subacute withdrawal: relationships to normal controls, age, and other clinical variables. Biol Psychiatry 1990; 27: 477–88. [DOI] [PubMed] [Google Scholar]
- Goldstone A, Willoughby AR, de Zambotti M, Franzen PL, Kwon D, Pohl KM, et al. The mediating role of cortical thickness and gray matter volume on sleep slow-wave activity during adolescence. Brain Struct Funct 2018; 223: 669–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodson CM, Clark BJ, Douglas IS. Predictors of severe alcohol withdrawal syndrome: a systematic review and meta-analysis. Alcohol Clin Exp Res 2014; 38: 2664–77. [DOI] [PubMed] [Google Scholar]
- Gualtieri CT, Morgan DW. The frequency of cognitive impairment in patients with anxiety, depression, and bipolar disorder: an unaccounted source of variance ie clinical trials. J Clin Psychiatry 2008; 69: 1122–30. [DOI] [PubMed] [Google Scholar]
- Harper C. The neuropathology of alcohol-related brain damage. Alcohol Alcohol 2009; 44: 136–40. [DOI] [PubMed] [Google Scholar]
- Heilig M, Egli M, Crabbe JC, Becker HC. Acute withdrawal, protracted abstinence and negative affect in alcoholism: are they linked? Addict Biol 2010; 15: 169–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hermann D, Weber-Fahr W, Sartorius A, Hoerst M, Frischknecht U, Tunc-Skarka N, et al. Translational magnetic resonance spectroscopy reveals excessive central glutamate levels during alcohol withdrawal in humans and rats. Biol Psychiatry 2012; 71: 1015–21. [DOI] [PubMed] [Google Scholar]
- Huron C, Servais C, Danion JM. Lorazepam and diazepam impair true, but not false, recognition in healthy volunteers. Psychopharmacology (Berl) 2001; 155: 204–9. [DOI] [PubMed] [Google Scholar]
- Irwin MR, Bjurstrom MF, Olmstead R. Polysomnographic measures of sleep in cocaine dependence and alcohol dependence: implications for age-related loss of slow wave, stage 3 sleep. Addiction 2016; 111: 1084–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry 2016; 80: 40–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jesse S, Bråthen G, Ferrara M, Keindl M, Ben-Menachem E, Tanasescu R, et al. Alcohol withdrawal syndrome: mechanisms, manifestations, and management. Acta Neurol Scand 2017; 135: 4–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991; 14: 540–5. [DOI] [PubMed] [Google Scholar]
- Junghanns K, Backhaus J, Veltrup C, Dageförde J, Brückmann H, Wetterling T. Mildly disturbed hepatic and pancreatic function during early abstention from alcohol is associated with brain atrophy and with disturbed psychometric performance. Alcohol Alcohol 2004; 39: 113–8. [DOI] [PubMed] [Google Scholar]
- Junghanns K, Horbach R, Ehrenthal D, Blank S, Backhaus J. Chronic and high alcohol consumption has a negative impact on sleep and sleep-associated consolidation of declarative memory. Alcohol Clin Exp Res 2009; 33: 893–7. [DOI] [PubMed] [Google Scholar]
- Kelly RM, Strick PL. Cerebellar loops with motor cortex and prefrontal cortex of a nonhuman primate. J Neurosci 2003; 23: 8432–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim DW, Kim HK, Bae EK, Park SH, Kim KK. Clinical predictors for delirium tremens in patients with alcohol withdrawal seizures. Am J Emerg Med 2015; 33: 701–4. [DOI] [PubMed] [Google Scholar]
- Kouimtsidis C, Duka T, Palmer E, Lingford-Hughes A. Prehabilitation in alcohol dependence as a treatment model for sustainable outcomes. A narrative review of literature on the risks associated with detoxification, from animal models to human translational research. Front Psychiatry 2019; 10: 339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kril JJ, Halliday GM, Svoboda MD, Cartwright H. The cerebral cortex is damaged in chronic alcoholics. Neuroscience 1997; 79: 983–98. [DOI] [PubMed] [Google Scholar]
- Kühn S, Charlet K, Schubert F, Kiefer F, Zimmermann P, Heinz A, et al. Plasticity of hippocampal subfield volume cornu ammonis 2 + 3 over the course of withdrawal in patients with alcohol dependence. JAMA Psychiatry 2014; 71: 806. [DOI] [PubMed] [Google Scholar]
- Laniepce A, Segobin S, Lannuzel C, Boudehent C, Ritz L, Urso L, et al. Neuropsychological and neuroimaging examinations of self‐reported sleep quality in alcohol use disorder with and without Korsakoff’s syndrome. Alcohol Clin Exp Res 2019; 43: 952–64. [DOI] [PubMed] [Google Scholar]
- Le Berre AP, Fama R, Sullivan EV. Executive functions, memory, and social cognitive deficits and recovery in chronic alcoholism: a critical review to inform future research. Alcohol Clin Exp Res 2017; 41: 1432–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee E, Jang DP, Kim JJ, An SK, Park S, Kim IY, et al. Alteration of brain metabolites in young alcoholics without structural changes. Neuroreport 2007; 18: 1511–4. [DOI] [PubMed] [Google Scholar]
- Levy BJ, Wagner AD. Cognitive control and right ventrolateral prefrontal cortex: reflexive reorienting, motor inhibition, and action updating. Ann N Y Acad Sci 2011; 1224: 40–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loeber S, Duka T, Márquez HW, Nakovics H, Heinz A, Mann K, et al. Effects of repeated withdrawal from alcohol on recovery of cognitive impairment under abstinence and rate of relapse. Alcohol Alcohol 2010; 45: 541–7. [DOI] [PubMed] [Google Scholar]
- Loeber S, Duka TT, Welzel H, Nakovics H, Heinz A, Flor H, et al. Impairment of cognitive abilities and decision making after chronic use of alcohol: the impact of multiple detoxifications. Alcohol Alcohol 2009; 44: 372–81. [DOI] [PubMed] [Google Scholar]
- Lukoyanov NV, Madeira MD, Paula-Barbosa MM Behavioral and neuroanatomical consequences of chronic ethanol intake and withdrawal. Physiol Behav 1999; 66: 337–46. [DOI] [PubMed] [Google Scholar]
- Maurage P, de Timary P, Billieux J, Collignon M, Heeren A. Attentional alterations in alcohol dependence are underpinned by specific executive control deficits. Alcohol Clin Exp Res 2014; 38: 2105–12. [DOI] [PubMed] [Google Scholar]
- Mirijello A, D’Angelo C, Ferrulli A, Vassallo G, Antonelli M, Caputo F, et al. Identification and management of alcohol withdrawal syndrome. Drugs 2015; 75: 353–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolen-Hoeksema S. Gender differences in risk factors and consequences for alcohol use and problems. Clin Psychol Rev 2004; 24: 981–1010. [DOI] [PubMed] [Google Scholar]
- O'Daly OG, Trick L, Scaife J, Marshall J, Ball D, Phillips ML, et al. Withdrawal-associated increases and decreases in functional neural connectivity associated with altered emotional regulation in alcoholism. Neuropsychopharmacology 2012; 37: 2267–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oscar-Berman M, Kirkley SM, Gansler DA, Couture A. Comparisons of Korsakoff and non-Korsakoff alcoholics on neuropsychological tests of prefrontal brain functioning. Alcohol Clin Exp Res 2004; 28: 667–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitel A-L, Chételat G, Le Berre AP, Desgranges B, Eustache F, Beaunieux H. Macrostructural abnormalities in Korsakoff syndrome compared with uncomplicated alcoholism. Neurology 2012; 78: 1330–3. [DOI] [PubMed] [Google Scholar]
- Pitel AL, Beaunieux H, Witkowski T, Vabret F, Guillery-Girard B, Quinette P, et al. Genuine episodic memory deficits and executive dysfunctions in alcoholic subjects early in abstinence. Alcoholism Clin Exp Res 2007; 31: 1169–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitel AL, Zahr NM, Jackson K, Sassoon SA, Rosenbloom MJ, Pfefferbaum A, et al. Signs of preclinical Wernicke’s encephalopathy and thiamine levels as predictors of neuropsychological deficits in alcoholism without Korsakoff’s syndrome. Neuropsychopharmacology 2011; 36: 580–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reitan RM The relation of the trail making test to organic brain damage. J Consult Psychol 1955; 19: 393–4. [DOI] [PubMed] [Google Scholar]
- Ritz L, Coulbault L, Lannuzel C, Boudehent C, Segobin S, Eustache F, et al. Clinical and biological risk factors for neuropsychological impairment in alcohol use disorder. PLoS One 2016; 11: e0159616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roux FJ, Kryger MH. Medication effects on sleep. Clin Chest Med 2010; 31: 397–405. [DOI] [PubMed] [Google Scholar]
- Saitz R, Mayo-Smith MF, Roberts MS, Redmond HA, Bernard DR, Calkins DR. Individualized treatment for alcohol withdrawal. A randomized double-blind controlled trial. JAMA 1994; 272: 519–23. [PubMed] [Google Scholar]
- Silczuk A, Habrat B. Alcohol-induced thrombocytopenia: current review. Alcohol 2020; 86: 9–16. [DOI] [PubMed] [Google Scholar]
- Singh LK, Nizamie SH, Tikka SK. Sleep architecture and EEG power spectra in recently detoxified alcohol dependent patients. Asian J Psychiatr 2018; 32: 126–36. [DOI] [PubMed] [Google Scholar]
- Stavro K, Pelletier J, Potvin S. Widespread and sustained cognitive deficits in alcoholism: a meta-analysis. Addict Biol 2013; 18: 203–13. [DOI] [PubMed] [Google Scholar]
- Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol 1935; 18: 643–62. [Google Scholar]
- Sullivan EV, Rosenbloom MJ, Pfefferbaum A. Pattern of motor and cognitive deficits in detoxified alcoholic men. Alcoholism Clin Exp Res 2000; 24: 611–21. [PubMed] [Google Scholar]
- Tingley D, Yamamoto T, Hirose K, Keele L, Imai K. Mediation: R package for causal mediation analysis. J Stat Softw 2014; 59: 1–38.26917999 [Google Scholar]
- Townshend JM, Duka T. Mixed emotions: alcoholics’ impairments in the recognition of specific emotional facial expressions. Neuropsychologia 2003; 41: 773–82. [DOI] [PubMed] [Google Scholar]
- Trick L, Kempton MJ, Williams SCR, Duka T. Impaired fear recognition and attentional set-shifting is associated with brain structural changes in alcoholic patients. Addict Biol 2014; 19: 1041–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsai G, Coyle JT. The role of glutamatergic neurotransmission in the pathophysiology of alcoholism. Annu Rev Med 1998; 49: 173–84. [DOI] [PubMed] [Google Scholar]
- Van der Linden M, Coyette F, Poitrenaud J, Kalafat M, Calicis F, Wyns C, et al. L’épreuve de rappel libre/rappel indicé à 16 items (RL/RI-16) In: L’évaluation des troubles de la mémoire : présentation de quatre tests de mémoire épisodique avec leur étalonnage. Solal, Marseille; 2004. p. 25–42. [Google Scholar]
- Villafuerte G, Miguel-Puga A, Murillo Rodríguez E, Machado S, Manjarrez E, Arias-Carrión O. Sleep deprivation and oxidative stress in animal models: a systematic review. Oxid Med Cell Longev 2015; 2015: 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler D. WAIS‐III administration and scoring manual. Psychological Corporation, San Antonio, TX; 1997.
- Wiers CE, Gawron CK, Gröpper S, Spengler S, Stuke H, Lindenmeyer J, et al. Decreased gray matter volume in inferior frontal gyrus is related to stop-signal task performance in alcohol-dependent patients. Psychiatry Res Neuroimaging 2015; 233: 125–30. [DOI] [PubMed] [Google Scholar]
- Yang X, Tian F, Zhang H, Zeng J, Chen T, Wang S, et al. Cortical and subcortical gray matter shrinkage in alcohol-use disorders: a voxel-based meta-analysis. Neurosci Biobehav Rev 2016; 66: 92–103. [DOI] [PubMed] [Google Scholar]
- Zahr NM, Pfefferbaum A, Sullivan EV. Perspectives on fronto-fugal circuitry from human imaging of alcohol use disorders. Neuropharmacology 2017; 122: 189–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahr NM, Sullivan EV. Translational studies of alcoholism: bridging the gap. Alcohol Res Health 2008; 31: 215–30. [PMC free article] [PubMed] [Google Scholar]
- Zinn S, Stein R, Swartzwelder HS. Executive functioning early in abstinence from alcohol. Alcohol Clin Exp Res 2004; 28: 1338–46. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data and materials used within this study will be made available, upon reasonable request, to research groups wishing to reproduce/confirm our results.