

Abstract
Incentive salience, or the attribution of motivational value to stimuli, is a biopsychological process that is disrupted in alcohol use disorder (AUD). The Addictions Neuroclinical Assessment (ANA) is a framework to characterize heterogeneity in addiction and establish a common assessment battery for research and clinical use. The ANA framework hypothesizes three constructs that correspond to processes in the etiology, course, and treatment of addiction: incentive salience, negative emotionality, and executive function. The current study extends prior findings on the ANA by validating the incentive salience construct among participants (n=563) in a multisite prospective study of individuals entering treatment for AUD. We used confirmatory factor analysis to test a one-factor model of incentive salience. Indicators included items assessing perception of urges to drink from the Alcohol Dependence Scale, Impaired Control Scale, and Marlatt Relapse Interview. Results indicated the one-factor model fit the data well (χ2 (12)=19.42, p=0.08; RMSEA=0.034 [90% CI: 0.000, 0.060], CFI=0.992) and was measurement invariant across sex. Incentive salience was associated with drinking patterns (e.g., drinks per day, r=.447 [95% CI: .379, .514]); reasons for drinking (urges/temptation r=.529 [95% CI: .460, .599]); testing personal control, r=.384 (95% CI: .308, .461); social pressure, r=.549 (95% CI: .481, .617); and family history of AUD, r=.134. The incentive salience factor demonstrated greater predictive validity for drinking outcomes compared to alternative preexisting scales. Overall, this study provides support for the construct validity and measurement invariance of the ANA incentive salience construct in a sample of individuals seeking AUD treatment.
Keywords: Incentive salience, Alcohol use disorder, Addictions Neuroclinical Assessment, Alcohol addiction research domain criteria, Craving
1. Introduction
Incentive salience describes the psychological processes of attributing motivational value to stimuli, making stimuli attractive or rewarding. These processes are mediated by mesocorticolimbic dopamine systems, which are specifically associated with “wanting” rather than “liking” stimuli (Berridge & Robinson, 2016). Evidence from animal models (Cofresí et al., 2019) as well as human laboratory and clinical studies (Zilverstand et al., 2018) supports high incentive salience toward substance-related cues and contexts as a central feature in several theoretical models of addiction. This body of research has converged to demonstrate that compulsive substance use arises when “mesolimbic systems become sensitized and hyperreactive to the incentive motivational properties of drug cues,” even if “liking” of the substance decreases (Berridge & Robinson, 2016, p. 673).
Exploring core psychological processes, such as incentive salience, may be a promising direction for research on the development and treatment of substance use disorders. Recent efforts to improve treatment outcomes for alcohol use disorder (AUD) have focused on the idea that individuals with AUD show marked heterogeneity in terms of their drinking behavior, motivations for drinking, drinking-related consequences, and underlying neurobiological characteristics (Litten et al., 2015). One framework that research has proposed to characterize heterogeneity in AUD is the Alcohol Addiction Research Domain Criteria (AARDoC), which aims to organize AUD research on multiple levels of analysis around core constructs related to the etiology, course, and treatment of AUD. To test AARDoC hypotheses in a practical and accessible way, Kwako and colleagues have developed and begun to test the Addictions Neuroclinical Assessment (ANA; Kwako, Momenan, Litten, Koob, & Goldman, 2016). The ANA comprises assessment measures across levels of analysis (e.g., self-report, behavior, neurocircuit) in three core domains, as proposed in AARDoC, that may be disrupted in addiction: incentive salience, negative emotionality, and executive function. Gaining a clearer understanding of the heterogeneity in AUD phenotypes, particularly phenotypes that are grounded in core neurobiological features of addiction, may inform why individuals respond differently to certain types of treatment (Witkiewitz et al., 2019).
An important goal of the ANA is to develop a common battery to measure these domains, which may include self-report, behavioral, and neuroimaging assessments. A recent study by Kwako and colleagues was the first to validate the three domain ANA model using factor analytic techniques among a sample of drinkers who varied with respect to treatment-seeking and AUD status (Kwako et al., 2019). The studies derived the indicators in this model from self-report and behavioral measures. Additional recent work has replicated and extended these initial findings by validating the negative emotionality domain in a longitudinal sample of AUD treatment-seekers using an even briefer set of commonly used self-report measures (Votaw et al., 2020). These previous studies have not used identical assessment batteries to measure ANA domains. However, replicating comparable ANA constructs across multiple samples and with separate assessment instruments is an important step with respect to establishing the validity of the core construct and testing which instruments function as the most promising indicators of ANA domains across samples.
1.1. Measuring the incentive salience domain
Measures of incentive salience are commonly utilized in human laboratory studies that evaluate pharmacotherapies for substance use disorders, including visual analog scales assessing desire to use drug, progressive ratio responding, drug purchase tasks (i.e., participants can either receive money or self-administer drug), and cue reactivity (Plebani et al., 2012; Walsh et al., 2016; Yardley & Ray, 2017). Cue reactivity tasks have also been outcomes in outpatient clinical trials of behavioral treatments for substance use disorders (e.g., Jurado-Barba et al., 2015; Nosen, Littlefield, Schumacher, Stasiewicz, & Coffey, 2014), and greater cue reactivity may predict poorer outcomes following treatment (Kvamme et al., 2019).
As described, incentive salience primarily captures motivated “wanting” (Berridge & Robinson, 2016). Kwako and colleagues (2016) initially proposed only one self-report measure of incentive salience—the Obsessive Compulsive Drinking Scale—in addition to behavioral and neuroimaging assessments of intentional bias, delay discounting, cue reactivity, and drug-related choice. However, researchers have criticized the substantial time burden of the full ANA assessment battery and research must continue to address whether simpler assessment strategies (e.g., self-report) adequately capture the core, underlying neurobiological processes (Ghitza, 2017).
1.2. Current study
The current study replicated and extended findings from Kwako and colleagues (2019) by evaluating the incentive salience domain among a sample of individuals entering treatment for AUD as part of a multisite prospective study. Kwako and colleagues found evidence for incentive salience as a unidimensional latent construct represented by individual self-report items from a single scale measuring preoccupation and drive toward alcohol. Research should continue to evaluate the incentive salience domain among independent samples of treatment-seekers, given that various treatment modalities either directly or indirectly attempt to impact incentive salience and motivation for various types of rewards. We report the evaluation of the negative emotionality domain in the current study sample elsewhere (Votaw et al., 2020). The current study could not adequately assess executive function domain in the study sample because the original study did not include relevant executive function measures.
The primary aim of the current analysis was to utilize confirmatory factor analysis to further examine the dimensionality of the incentive salience construct using additional self-report indicators from multiple scales that are theorized to correspond to neurobiological and behavioral assessments of incentive salience (see Table 1). Next, we examined measurement invariance of the incentive salience construct across sex or, in other words, testing whether the construct is being measured in the same way among female and male participants. Establishing invariance is necessary to examine sex differences in a construct. The need to establish sex invariance in incentive salience is highlighted by prior evidence of sex differences in processes underlying alcohol cue reactivity and reward processing (Barker & Taylor, 2019; Becker & Chartoff, 2019; Kaag et al., 2019). To assess the construct validity (including concurrent and discriminant validity) of the incentive salience construct in this sample, we examined associations between incentive salience and drinking patterns, common drinking situations, family history of AUD, social support, and religious beliefs. To assess the predictive validity of the incentive salience construct, we evaluated whether it was a better predictor of 12-month drinking outcomes than preexisting scales of similar constructs.
Table 1.
Descriptive statistics of indicators of the incentive salience factor and construct validity parameters.
| Measure | ||
|---|---|---|
| Indicators | n | M (SD) or % |
| ADSa Item 18: Do you almost constantly think about drinking and alcohol? | 495 | |
| 0 = No | 201 | 40.6% |
| 1 = Yes | 294 | 59.4% |
| ADS Item 25: After taking one or two drinks, can you usually stop? | 490 | |
| 0 = No | 62 | 12.7% |
| 1 = Yes | 428 | 87.3% |
| ICSb Item 6: I have found it difficult to limit the amount I drank. | 555 | |
| 1 = Never | 12 | 2.2% |
| 2 = Rarely | 48 | 8.6% |
| 3 = Sometimes | 122 | 22.0% |
| 4 = Often | 214 | 38.6% |
| 5 = Always | 159 | 28.6% |
| ICS Item 13: I have had an irresistible urge to continue drinking once I started. | 559 | |
| 1 = Never | 14 | 2.5% |
| 2 = Rarely | 33 | 5.9% |
| 3 = Sometimes | 96 | 17.1% |
| 4 = Often | 212 | 37.7% |
| 5 = Always | 204 | 36.2% |
| ICS Item 14: I have found it difficult to resist drinking, even for a single day. | 548 | |
| 1 = Never | 56 | 10.2% |
| 2 = Rarely | 95 | 17.3% |
| 3 = Sometimes | 138 | 25.2% |
| 4 = Often | 172 | 31.4% |
| 5 = Always | 87 | 15.9% |
| ICS Item 23: I would have an irresistable urge to continue drinking once I started. | 559 | |
| 1 = Strongly Agree | 223 | 39.9% |
| 2 = Agree | 235 | 42.0% |
| 3 = Undecided | 51 | 9.1% |
| 4 = Disagree | 33 | 5.9% |
| 5 = Strongly Disagree | 17 | 3.0% |
| MRIc Item 50: Right before you took your first drink (after your last period of abstinence), how strong was your urge to drink? | 549 | |
| 1 | 21 | 3.8% |
| 2 | 14 | 2.6% |
| 3 | 25 | 4.6% |
| 4 | 92 | 16.8% |
| 5 | 67 | 12.2% |
| 6 | 77 | 14.0% |
| 7 | 253 | 46.1% |
| Construct Validity Analyses | n | M (SD) or % |
| Baseline Percent Days Abstinent | 562 | 47.0 (30.0) |
| Baseline Drinks per Drinking Day | 562 | 20.2 (13.0) |
| Baseline Drinks per Day | 562 | 11.4 (10.9) |
| Baseline Percent Heavy Drinking Days | 562 | 48.5 (30.0) |
| 12-Month Percent Heavy Drinking Days | 478 | 14.3 (28.5) |
| IDSd Testing Personal Control | 547 | 2.6 (0.7) |
| IDS Urges/Temptations | 544 | 2.6 (0.7) |
| IDS Social Pressure | 548 | 2.2 (0.6) |
| Family History of Alcohol Use Disorder | 531 | |
| 0 = No | 136 | 25.6% |
| 1=Yes | 395 | 74.4% |
| Religious Background and Behavior | 253 | 22.2 (9.3) |
| SSQe Friend Social Support | 560 | 7.3 (4.2) |
| SSQ Family Social Support | 556 | 7.2 (4.9) |
ADS: Alcohol Dependence Scale
ICS: Impaired Control Scale
MRI: Marlatt Relapse Interview
IDS: Inventory of Drinking Situations
SSQ: Perceived Social Support Questionnaire
2. Materials and methods
2.1. Data and participants
The current study was a secondary analysis of data (n=563) from the Relapse Replication and Extension Project (RREP; Lowman, Allen, Stout, & Group, 1996), a multisite, observational, prospective study intended to replicate and expand Marlatt’s taxonomy of relapse determinants (Marlatt, 1996) in a diverse sample. We recruited participants at admission from 15 inpatient and outpatient community alcohol treatment programs in Albuquerque, NM (1 site), Providence, RI (6 sites), and Buffalo, NY (8 sites). Type of treatment and time in treatment varied across sites and individuals, and we do not report these variables in the dataset.
The inclusion criteria for participants were: aged 18 years or older (21 years or older for RI sites); met criteria for alcohol use or dependence in the past six months through the Diagnostic Interview Schedule for DSM-III-R (DIS-R; Robins, Cottler, & Keating, 1989); could read at an 8th grade level; completed alcohol detoxification; and were willing to participate in all study procedures. Exclusion criteria included: meeting criteria for a substance use disorder more severe than alcohol; using drugs intravenously in the previous six months; or having major psychiatric disorders or cognitive impairments.
The participants (n=563) were majority male (58.8%) and non-Hispanic white (67.3%), with an average age of 34.3 years (SD=8.7). They were most frequently single (41.0%) or separated or divorced (34.2%). Participants finished an average of 12.0 years of education (SD=2.4) and were “homemakers” (40.0%), unemployed (28.1%), or employed part time (25.2%).
2.2. Measures
Study sites administered a standardized set of measures at admission to treatment (i.e., baseline) and follow-up assessments every two months for one year (Lowman et al., 1996). The current study primarily examined measures administered during the baseline assessment, as well as the Timeline Followback (described below) at both the baseline and 12-month follow-up assessment.
2.3. Indicators of incentive salience
2.3.1. Alcohol Dependence Scale (ADS).
The ADS is a 25-item questionnaire assessing alcohol dependence symptoms and severity in the past twelve months (Skinner & Allen, 1982). Items are summed to a total score between 0 and 47. Research has shown the ADS to have high internal consistency and concurrent validity (Saxon et al., 2007; Skinner & Allen, 1982; Williams & Ricciardelli, 1996). The current study includes items 18 and 25 as indicators in the model (see Table 1).
2.3.2. Impaired Control Scale (ICS).
The ICS is a 44-item questionnaire developed to measure impairment in control over alcohol use in the past six months (Heather et al., 1993, 1998). Research has shown the ICS to have high internal consistency, discriminant validity, and concurrent validity (Heather et al., 1993). The current study includes items 6, 13, 14, and 23 as indicators (Table 1) and the Failed Control subscale score in predictive validity analyses, which measures participants’ impaired restraint of their drinking over the past six months.
2.3.3. Situational Confidence Questionnaire (SCQ).
The SCQ is a 39-item questionnaire designed to assess abstinence self-efficacy in common alcohol use situations. Prior studies have found the SCQ to have high internal consistency (Annis & Graham, 1988), and we included items 17 through 20 as indicators (Table 1).
2.3.4. Marlatt Relapse Interview (MRI).
The MRI is a short interview method developed for this protocol that includes open-ended questions about the most recent relapse and drinking episode. In the current study, we included only item 47 as an indicator (Table 1).
2.4. Measures to examine construct validity
2.4.1. Comprehensive Drinker Profile (CDP).
The CDP is a standardized interview developed for clinical and research settings to evaluate severity of AUD (Miller & Marlatt, 1984). We used demographic and family history information from this interview in the current study, including sex, age, racial/ethnic identity, years of education, employment status, marital status, and family history of AUD.
2.4.2. Inventory of Drinking Situations (IDS).
The IDS is a 42-item questionnaire that asks in which situations participants drank heavily (Annis, 1982). The IDS has eight subscales, which are each summed individually. For the current study, we included three subscales, all of which showed acceptable internal consistency, including testing personal control (α=0.737), urges and temptations to drink (α=0.673), and social pressure to drink (α=0.673).
2.4.3. Form 90 Timeline Followback (TLFB).
We used the Form 90 (Sobell and Sobell, 1992), which uses the TLFB method (i.e., calendar and event-based cues), to collect daily drinking patterns. At baseline, participants retrospectively reported daily drinking in the 90 days prior to the assessment. At follow-ups, participants retrospectively reported drinking since the last study visit. We calculated several indicators of drinking patterns using these data: percent days abstinent, percent heavy drinking days (defined as 4/5+ drinks for women/men; National Institute on Alcohol Abuse and Alcoholism [NIAAA], n.d.), average drinks per day, and average drinks per drinking day. Previous studies have demonstrated that the TLFB has good reliability and validity (Maisto et al., 2008).
2.4.4. Religious Background and Beliefs Questionnaire (RBB).
The RBB is a 13-item questionnaire assessing the religious and spiritual behaviors and beliefs of the participant in the past year and over their lifespan (Connors et al., 1996). It is scored by summing all of the items and previous studies have shown it to have high internal consistency (Connors et al., 1996). In the current study, the RBB showed good internal consistency (α=0.849).
2.4.5. Perceived Social Support Questionnaire (SSQ).
The SSQ is a 28-item questionnaire assessing perceptions of how supportive participants’ relationships are with family and friends (Procidano & Heller, 1983). Fourteen items each are summed for a total score representing total social support from friends and social support from family. In the current study, the SSQ friends subscale showed somewhat low internal consistency (α=0.647) and the family subscale showed adequate internal consistency (α=0.730).
2.5. Statistical analyses
2.5.1. Confirmatory factor analysis (CFA).
We conducted CFA models of the incentive salience items using a diagonally weighted least squares (WLSMV) estimator in Mplus 8.2 (Muthén & Muthén, 2017). We utilized WLSMV estimation, given all items were ordered categorical (Li, 2016). We used a sandwich estimator to adjust the standard errors for clustering of individuals within research sites. Two independent reviewers initially selected indicators for the incentive salience latent factor based on substantive fit with the latent construct. We tested initial models with SCQ items 17–20; ADS items 18 and 25; ICS items 6, 13, 14, and 23; and MRI item 47. We tested initial models with correlated error terms for all items of the ICS and with correlated error terms for all items of the SCQ, and we dropped nonsignificant correlations from the model. We re-estimated models iteratively (as described below), until we considered model fit adequate based on a nonsignificant χ2 test, the Comparative Fit Index (CFI) > .95, Root Mean Square Error of Approximation (RMSEA) < .06 (Hu & Bentler, 1999), and all standardized factor loadings being greater than 0.40 (Kline, 2015).
2.5.2. Measurement invariance.
After selecting a final CFA model, we then tested measurement invariance of the construct by sex via multiple group CFA. This method allows for the incentive salience latent factor model to be tested separately among male and females and then evaluated for equivalent model fit and indicator item functioning. We tested the configural invariance model, which tests the overall factor structure by group (i.e., the same items measure the incentive salience latent factor within each group), with separate factor loadings, thresholds, and variances for males and females. To examine metric invariance, which tests whether factor loadings are equivalent by group (i.e., the association between incentive salience latent factor and item responses at the same level of incentive salience are the same within each group), we constrained the factor loadings to equality across males and females. To examine scalar invariance, which tests whether factor loadings and item response thresholds are equivalent by group (i.e., probability of item responses at the same level of incentive salience are the same within each group), we constrained the factor loadings and indicator thresholds to equality across males and females. We constrained residuals for categorical items to one for identification in all models (Widaman et al., 2010). For all invariance testing, we used the DIFFTEST model comparison tool in Mplus, given that the model χ2 test statistic cannot be used for χ2 difference testing with the WLSMV estimator. We also used model comparison criteria as a test of decrement in fit when testing for measurement invariance of negative change in CFI ≥.01 (Cheung & Rensvold, 2002) and a positive change in RMSEA ≥.015 (Chen, 2007).
2.5.3. Construct validity.
Next, we examined the construct validity of the incentive salience latent factor by testing convergent, discriminant, and predictive validity. We hypothesized that convergent validity would be supported by significant correlations between the incentive salience latent factor and baseline measures of drinking patterns—including percent days abstinent, drinks per drinking days, drinks per day, and percent heavy drinking days—self-reported high risk situations for heavy drinking on the IDS subscales that measured testing personal control, urges/temptations, and social pressure to drink, and a single item binary measure of family history of AUD. We hypothesized that the incentive salience factor being unrelated to social support and religious beliefs and behaviors would support discriminant validity. We hypothesized that significant associations between the incentive salience factor at baseline and percent heavy drinking days at the 12-month follow-up assessment would support predictive validity. Furthermore, we compared the predictive validity of the incentive salience factor to standalone scales with similar content, including the IDS and ICS. We hypothesized the incentive salience factor would demonstrate stronger predictive validity.
2.5.4. Sensitivity analyses using multiple imputation.
Given a small amount of missing item-level data (range of 1% to 12.9% missing), we conducted sensitivity analyses to assess the impact of missing data by re-estimating all models using multiple imputation with parameter estimates pooled across 50 imputed datasets (Hallgren et al., 2016). The imputation models included all indicators in the CFA and variables included in construct validity analyses.
3. Results
3.1. Descriptive statistics and initial CFA
Table 1 provides the descriptive statistics for the measures used in the current study. Participants’ responses to hypothesized indicators of the incentive salience domain indicated that they often thought about alcohol, that it would be difficult to limit the amount of alcohol they drank, and that they experienced strong and irresistible urges to drink before their most recent relapse and once they start drinking. In the three months prior to baseline, participants reported 47.0% (SD=30.0%) percent days abstinent, 48.5% (SD=30.0%) percent heavy drinking days, and they drank an average of 11.4 (SD=10.9) drinks per day and 20.2 (SD=13.0) drinks per drinking day. Nearly three quarters (74%) of participants had a family history of AUD.
3.2. Confirmatory factor analysis (CFA)
We first tested a model with a one-factor CFA model with SCQ items 17–20; ADS items 18 and 25; ICS items 6, 13, 14, and 23; and MRI item 47. We tested initial models with correlated error terms for all items of the ICS and with correlated error terms for all items of the SCQ. This model provided an adequate fit to the data (χ2 (32)=39.95, p=0.16; RMSEA= 0.021 [90% CI: 0.000, 0.040], CFI=0.992), but the standardized factor loadings for the SCQ items were all equal to or below +.10, indicating the SCQ items did not load with the other items. Additionally, the only significant correlated error terms were ICS item 13 with ICS items 6 and 23, thus we then dropped the SCQ items and additional correlated error terms of the ICS items from the model and we re-estimated the model.
The final model (Figure 1) with ADS items 18 and 25; ICS items 6, 13, 14, and 23; and MRI item 47, with correlated error terms from ICS item 13 with ICS items 6 and 23, provided an adequate fit to the data (χ2 (12)=19.42, p=0.08; RMSEA=0.034 [90% CI: 0.000, 0.060], CFI=0.992). Additionally, all factor loadings were greater than ±0.40 (see Table 2).
Figure 1.
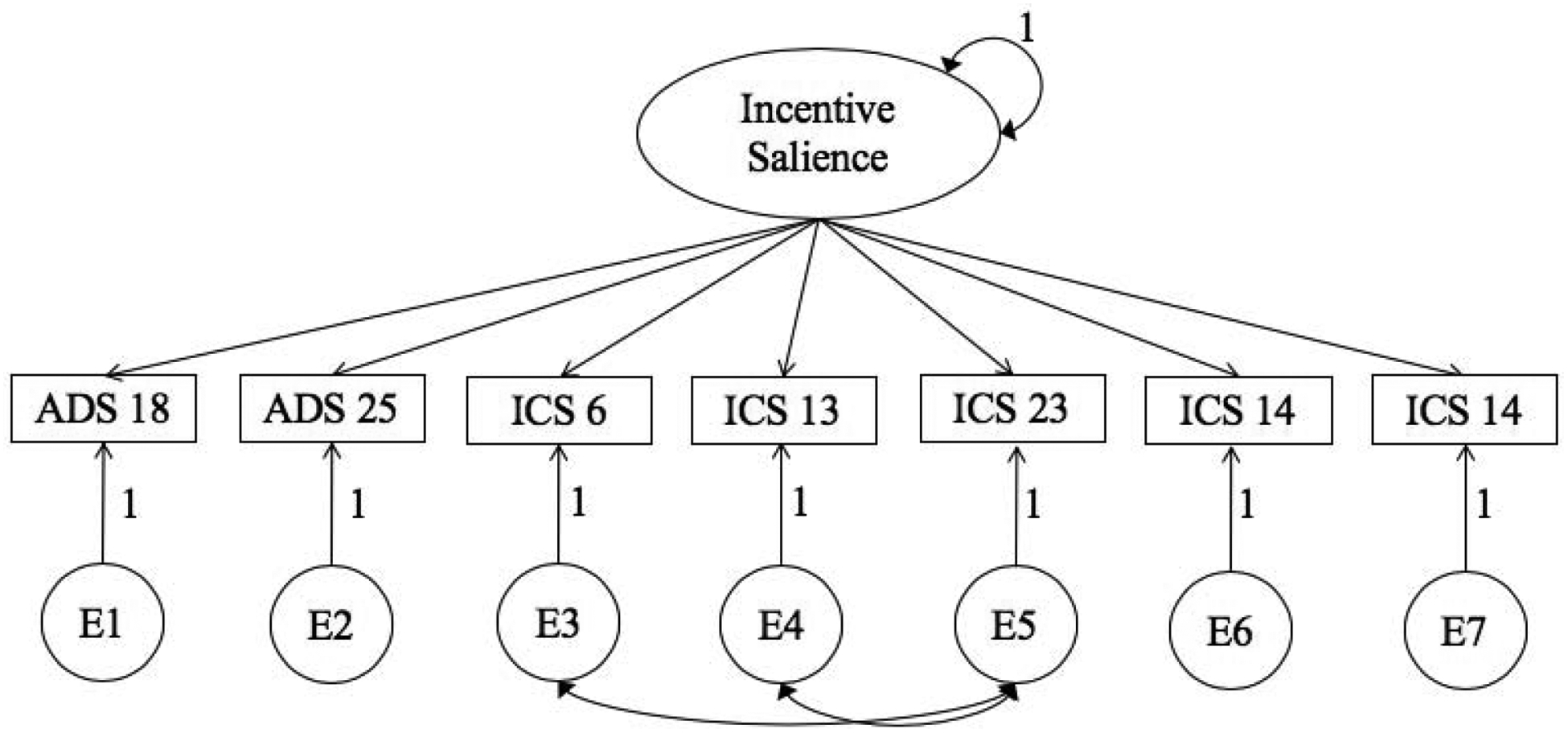
Final confirmatory factor analysis model.
Table 2.
Summary of confirmatory factor analyses of the incentive salience construct at baseline.
| Baseline (n=543) |
|
|---|---|
| Incentive Salience Indicators | Factor Loadings |
| ADS018 | 0.538 |
| ADS025 | 0.878 |
| ICS006 | 0.570 |
| ICS013 | 0.618 |
| ICS014 | 0.709 |
| ICS023 | −0.593 |
| MRI047 | 0.415 |
| Correlated Errors (SE) | |
| ICS006 with ICS013 | .121(.029) |
| ICS013 with ICS023 | −.122 (.028) |
| Model Fit Statistics | |
| Model χ2 (12) | 19.420 |
| p-value | .079 |
| Confirmatory Fit Index (CFI) | .992 |
| Root Mean Squared Error of Approximation (RMSEA) | .034 |
Note. All factor loadings and correlated errors were statistically significant (p < .05).
3.3. Measurement invariance across sex
Next, we examined whether the final model shown in Figure 1 was invariant across males and females. Results from the invariance testing indicated that the metric invariance model did not fit significantly worse than the configural model (Δχ2 (Δ7)=4.15, p=0.76; ΔRMSEA= 0.004, ΔCFI=0.003) and the scalar invariance model did not fit significantly worse than the metric model (Δχ2 (Δ24)=28.61, p=0.24; ΔRMSEA=0.006, ΔCFI=0.003). Thus, the incentive salience latent factor was invariant by sex.
3.4. Construct validity
Table 3 shows correlations between incentive salience and measures of convergent and discriminant validity 3. Incentive salience was significantly negatively associated with percent days abstinent and positively significantly associated with drinks per drinking day, drinks per day, percent heavy drinking days, testing personal control, urges/temptation, social pressure to drink, and family history of AUD. Incentive salience was not significantly related to religiosity or family social support, but was weakly related to friend social support.
Table 3.
Concurrent associations between the incentive salience construct and alcohol use, inventory of drinking situations, and sex.
| Baseline r (95% CI), p-value |
|
|---|---|
| Percent Days Abstinent | −0.284 (−0.370, −0.197), p<.001 |
| Drinks per Drinking Day | 0.431 (0.356, 0.506), p<.001 |
| Drinks per Day | 0.447 (0.379, 0.514), p<.001 |
| Percent Heavy Drinking Days | 0.345 (0.261, 0.430), p<.001 |
| IDS Testing Personal Control | 0.384 (0.308, 0.461), p<.001 |
| IDS Urges and Temptation | 0.529 (0.460, 0.599), p<.001 |
| IDS Social Pressure | 0.549 (0.481, 0.617), p<.001 |
| Sex (0 = women, 1 = men) | −0.022 (−0.121, 0.076), p=.656 |
| Family history (0 = no, 1 = yes) | 0.134 (0.034, 0.235), p=.009 |
| Religious Background and Behavior | −0.065 (−0.204, 0.075), p=.366 |
| SSQ Friend Social Support | −0.135 (−0.230, −0.040), p=.006 |
| SSQ Family Social Support | −0.097 (−0.198, 0.003), p=.058 |
Note. IDS = Inventory of Drinking Situations; SSQ = Social Support Questionnaire; 95% CI = bootstrapped 95% confidence interval; confidence intervals that do not include zero represent statistically significant associations between the incentive salience construct and concurrent alcohol use and drinking situations.
Predictive validity analyses demonstrated associations of the incentive salience factor, ICS, and IDS with 12-month drinking outcomes and we show these in Table 4. Incentive salience was significantly positively associated with percent heavy drinking days at 12-month follow-up and accounted for a greater proportion of the 12-month percent heavy drinking days variance (2.1% of the variance; R2=0.021, p=.003) than either the IDS (0.7% of the variance; R2=0.007, p=.010) or the ICS (0.67% of the variance; R2=0.011, p=.067).
Table 4.
Predictive associations of the incentive salience construct and similar scales with 12-month percent heavy drinking days outcomes.
| R2, p-value | |
|---|---|
| Incentive Salience Factor | R2=0.021, p=.003 |
| Inventory of Drinking Situations (IDS) | R2=0.007, p=.010 |
| Impaired Control Scale (ICS) | R2=0.011, p=.067 |
3.5. Sensitivity analyses using multiple imputation
Attrition analyses indicated missing data were not associated with any of the other variables in the model. However, given some item-level missing data, we re-estimated all models using multiple imputation, which is a robust method for handling missing data under the assumption that data were missing at random. The multiple imputation models did not yield substantive differences from the original analyses (see Supplementary Tables 1, 2, and 3).
4. Discussion
This study examined the factor structure, measurement invariance across sex, and construct validity of an incentive salience latent construct in a sample of individuals seeking treatment for AUD. Consistent with the originally proposed ANA, a single factor model showed good fit to the observed data, and the incentive salience construct was invariant across sex. Additionally, associations between incentive salience and more frequent and heavier drinking, family history of AUD, and drinking in situations related to testing personal control, urges/temptation, and social pressure to drink demonstrated convergent validity. Greater associations between incentive salience and 12-month drinking outcomes than similar preexisting measures showed predictive validity.
These findings are consistent with prior work modeling incentive salience, negative emotionality, and executive function as underlying latent constructs among individuals who ranged from healthy volunteers to those seeking treatment for AUD (Kwako et al., 2019). Although we did not replicate this prior work with an identical set of indicators, we demonstrated that a comparable single factor incentive salience construct could be modeled with additional items that assess perceived intensity of urges and ability to resist urges from several commonly used self-report measures. In particular, several items from the ICS, a measure that has demonstrated concurrent validity with important treatment outcome and drinking reduction variables (Heather et al., 1998), demonstrated good factor loadings on the incentive salience construct. Replicating this incentive salience factor in a different sample with a different set of indicators demonstrates the robustness of this latent construct within an AUD treatment-seeking population.
Although this study and prior work have validated the incentive salience latent construct utilizing self-report indicators, future research in this area should continue to evaluate the trade-off between using practical, easy-to-administer self-report measures versus task-based behavioral assessments of cue reactivity and incentive motivation toward stimuli. An extensive body of literature has characterized incentive salience using behavioral tasks that can detect sensitized incentive salience at levels below conscious awareness, such as faster pairing of alcohol words and positive words in implicit association tasks (Wiers et al., 2002). Functional MRI studies confirm that incentive salience behavioral tasks elicit activation in incentive salience neurocircuitry, and likewise, studies have demonstrated that self-reported craving for alcohol is associated with level of activation in incentive salience neurocircuitry (Cofresí et al., 2019). Given that sensitization in mesolimbic circuits in the brain mediate disruptions in incentive salience and that they manifest at both subjective and unconscious levels, an important future direction for research will be to investigate the trade-offs in specificity and practicality with using self-report versus behavioral or neurobiological indicators of the incentive salience latent construct as measured within a potential ANA assessment battery. It is quite possible that measuring an incentive salience construct with consistent fMRI tasks and parameters will further clarify AUD phenotypes and lend greater predictive validity (Voon et al., 2020). However, a simpler self-report approach may be more accessible to implement in a wide range of clinical and research settings.
Findings from this study must be considered in the context of several methodological limitations. First, the sample used in the current secondary data analysis comes from a study conducted more than 20 years ago with a sample that is predominantly male, non-Hispanic white, and without major psychiatric disorders (Lowman et al., 1996). Thus, replication in more contemporary and diverse samples, as well as those with co-occurring psychiatric disorder, is necessary to generalize our findings. The indicators included in these analyses may introduce bias given that they are all self-report retrospective measures, which recall bias may impact. Although easy to administer in clinical practice, these indicators may not be optimal for assessing the construct of incentive salience. Likewise, this study was not designed to assess the construct validity of incentive salience. Future studies on this topic should evaluate behavioral and neurobiological indicators, the ecological validity of this domain via experience sampling methods, and additional measures to establish convergent and discriminant validity (e.g., impulsivity).
In sum, the current study supports incentive salience as a latent construct with unidimensional factor structure, measurement invariance across sex, and good evidence of construct validity. This adds to a recent and growing evidence base on three core domains that capture heterogeneity within addictive disorders— incentive salience, negative emotionality, and executive function— as the ANA proposes. These findings may guide future research and clinical practice involving the role of incentive salience in precision medicine efforts. Continued work in this area is needed to eventually arrive at a common battery of measures that captures core phenotypic features of addiction.
Supplementary Material
Highlights.
The Addictions Neuroclinical Assessment includes a core incentive salience factor
Incentive salience factor was replicated in a multisite study of alcohol treatment
Confirmatory factor analysis showed univariate factor with good construct validity
Incentive salience predicted drinking outcomes beyond previous measures
This study supports and extends the ANA framework in a new sample
Acknowledgments
This work was supported by the National Institute of Alcoholism and Alcohol Abuse of the National Institutes of Health, award numbers R01AA022328 and T32AA018108. The content is the sole responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors have no conflicts of interest.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Annis H (1982). Inventory of drinking situations. Addiction Research Foundation. [Google Scholar]
- Annis H, & Graham J (1988). Situational confidence questionnaire (SCQ): User’s guide.
- Barker JM, & Taylor JR (2019). Sex differences in incentive motivation and the relationship to the development and maintenance of alcohol use disorders. Physiology and Behavior, 203(May 2017), 91–99. 10.1016/j.physbeh.2017.09.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker JB, & Chartoff E (2019). Sex differences in neural mechanisms mediating reward and addiction. Neuropsychopharmacology, 44(1), 166–183. 10.1038/s41386-018-0125-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berridge KC, & Robinson T (2016). Liking, wanting and the incentive salience theory of addiction. American Psychologist, 71(8), 670–679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen FF (2007). Sensitivity of goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling, 14(3), 464–504. 10.1080/10705510701301834 [DOI] [Google Scholar]
- Cheung GW, & Rensvold RB (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255. 10.1207/S15328007SEM0902_5 [DOI] [Google Scholar]
- Cofresí RU, Bartholow BD, & Piasecki TM (2019). Evidence for incentive salience sensitization as a pathway to alcohol use disorder. Neuroscience and Biobehavioral Reviews, 107(October), 897–926. 10.1016/j.neubiorev.2019.10.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connors GJ, Tonigan JS, & Miller WR (1996). A measure of religious background and behavior for use in behavior change research. Psychology of Addictive Behaviors, 10(2), 90–96. 10.1037/0893-164X.10.2.90 [DOI] [Google Scholar]
- Ghitza UE (2017). Commentary: Addictions Neuroclinical Assessment: A Neuroscience-Based Framework for Addictive Disorders. Frontiers in Psychiatry, 8 10.3389/fpsyt.2017.00002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallgren KA, Witkiewitz K, Kranzler HR, Falk DE, Litten RZ, O’Malley SS, & Anton RF (2016). Missing data in alcohol clinical trials with binary outcomes. Alcoholism: Clinical and Experimental Research, 40(7), 1548–1557. 10.1111/acer.13106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heather N, Booth P, & Luce A (1998). Impaired control scale: Cross-validation and relationships with treatment outcome. Addiction, 93(5), 761–771. [DOI] [PubMed] [Google Scholar]
- Heather N, Tebbutt JS, Mattick RP, & Zamir R (1993). Development of a scale for measuring impaired control over alcohol consumption: A preliminary report. Journal of Studies on Alcohol, 54(6), 700–709. 10.15288/jsa.1993.54.700 [DOI] [PubMed] [Google Scholar]
- Hu LT, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Jurado-Barba R, Rubio Valladolid G, Martinez-Gras I, Alvarez-Alonso MJ, Ponce Alfaro G, Fernandez A, Moratti S, Heinz A, & Jimenez-Arriero MA (2015). Changes on the modulation of the startle reflex in alcohol-dependent patients after 12 weeks of a cognitive-behavioral intervention. European Addiction Research, 21(4), 195–203. 10.1159/000371723 [DOI] [PubMed] [Google Scholar]
- Kaag AM, Wiers RW, de Vries TJ, Pattij T, & Goudriaan AE (2019). Striatal alcohol cue-reactivity is stronger in male than female problem drinkers. European Journal of Neuroscience, 50(3), 2264–2273. 10.1111/ejn.13991 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB (2015). Principles and practice of structural equation modeling. Guilford Press. [Google Scholar]
- Kvamme TL, Pedersen MU, Overgaard M, Rømer Thomsen K, & Voon V (2019). Pupillary reactivity to alcohol cues as a predictive biomarker of alcohol relapse following treatment in a pilot study. Psychopharmacology, 236(4), 1233–1243. 10.1007/s00213-018-5131-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwako LE, Momenan R, Litten RZ, Koob GF, & Goldman D (2016). Addictions neuroclinical assessment: A neuroscience-based framework for addictive disorders. Biological Psychiatry, 80(3), 179–189. 10.1016/j.biopsych.2015.10.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwako LE, Schwandt ML, Ramchandani VA, Diazgranados N, Koob GF, Volkow ND, Blanco C, & Goldman D (2019). Neurofunctional domains derived from deep behavioral phenotyping in alcohol use disorder. American Journal of Psychiatry, 176(9), 744–753. 10.1176/appi.ajp.2018.18030357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li C-H (2016). Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behavior Research Methods, 48(3), 936–949. 10.3758/s13428-015-0619-7 [DOI] [PubMed] [Google Scholar]
- Litten RZ, Ryan ML, Falk DE, Reilly M, Fertig JB, & Koob GF (2015). Heterogeneity of alcohol use disorder: Understanding mechanisms to advance personalized treatment. Alcoholism: Clinical and Experimental Research, 39(4), 579–584. 10.1111/acer.12669 [DOI] [PubMed] [Google Scholar]
- Lowman C, Allen J, Stout RL, Connors G, Longabaugh R, Maisto SA, Miller WR, Rubin A, Stour RL, Waldron D, Westerberg VS, & Zywiak WH (1996). Replication and extension of Marlatt’s taxonomy of relapse precipitants: Overview of procedures and results. Addiction, 91, S51–S71. 10.1111/j.1360-0443.1996.tb02327.x [DOI] [PubMed] [Google Scholar]
- Marlatt GA (1996). Taxonomy of high-risk situations for alcohol relapse: evolution and development of a. Addiction, 91(12s1), 37–50. 10.1046/j.1360-0443.91.12s1.15.x [DOI] [PubMed] [Google Scholar]
- Miller WR, & Marlatt GA (1984). Comprehensive Drinker Profile.
- Muthén LK, & Muthén BO (2017). Mplus users guide (Version 8). Muthén & Muthén. [Google Scholar]
- Nosen E, Littlefield AK, Schumacher JA, Stasiewicz PR, & Coffey SF (2014). Treatment of co-occurring PTSD-AUD: Effects of exposure-based and non-trauma focused psychotherapy on alcohol and trauma cue-reactivity. Behaviour Research and Therapy, 61, 35–42. 10.1016/j.brat.2014.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plebani JG, Ray LA, Morean ME, Corbin WR, Mackillop J, Amlung M, & King AC (2012). Human laboratory paradigms in alcohol research. Alcoholism: Clinical and Experimental Research, 36(6), 455–466. 10.1111/j.1530-0277.2011.01704.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Procidano ME, & Heller K (1983). Measures of perceived social support from friends and from family: Three validation studies. American Journal of Community Psychology, 11(1), 1–24. [DOI] [PubMed] [Google Scholar]
- Robins L, Cottler L, & Keating S (1989). The NIMH Diagnostic Interview Schedule, Version III, revised (DIS-III-R). National Institute on Mental Health. [Google Scholar]
- Saxon AJ, Kivlahan DR, Doyle S, & Donovan DM (2007). Further validation of the alcohol dependence scale as an index of severity. Journal of Studies on Alcohol and Drugs, 68(1), 149–156. 10.15288/jsad.2007.68.149 [DOI] [PubMed] [Google Scholar]
- Skinner HA, & Allen BA (1982). Alcohol dependence syndrome: Measurement and validation. Journal of Abnormal Psychology, 91(3), 199–209. 10.1037/0021-843X.91.3.199 [DOI] [PubMed] [Google Scholar]
- Voon V, Grodin E, Mandali A, Morris L, Doñamayor N, Weidacker K, Kwako L, Goldman D, Koob GF, & Momenan R (2020). Addictions NeuroImaging Assessment (ANIA): Towards an integrative framework for alcohol use disorder. Neuroscience and Biobehavioral Reviews, 113(March), 492–506. 10.1016/j.neubiorev.2020.04.004 [DOI] [PubMed] [Google Scholar]
- Votaw VR, Pearson MR, Stein E, & Witkiewitz K (2020). The Addictions Neuroclinical Assessment negative emotionality domain among treatment-seekers with alcohol use disorder: Construct validity and measurement invariance. Alcoholism: Clinical and Experimental Research, 44(3), 679–688. 10.1111/acer.14283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh SL, Nuzzo PA, Babalonis S, Casselton V, & Lofwall MR (2016). Intranasal buprenorphine alone and in combination with naloxone: Abuse liability and reinforcing efficacy in physically dependent opioid abusers. Drug and Alcohol Dependence, 162, 190–198. 10.1016/j.drugalcdep.2016.03.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widaman KF, Ferrer E, & Conger RD (2010). Factorial invariance within longitudinal structural equation models: Measuring the same construct across time. Child Development Perspectives, 4(1), 10–18. 10.1111/j.1750-8606.2009.00110.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiers RW, van Woerden N, Smulders FTY, & de Jong PJ (2002). Implicit and explicit alcohol-related cognitions in heavy and light drinkers. Journal of Abnormal Psychology, 111(4), 648–658. 10.1037/0021-843X.111.4.648 [DOI] [PubMed] [Google Scholar]
- Williams RJ, & Ricciardelli LA (1996). Expectancies relate to symptoms of alcohol dependence in young adults. Addiction (Abingdon, England), 91(7), 1031–1039. [PubMed] [Google Scholar]
- Witkiewitz K, Litten RZ, & Leggio L (2019). Advances in the science and treatment of alcohol use disorder. Science Advances, 5(9). 10.1126/sciadv.aax4043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yardley MM, & Ray LA (2017). Medications development for the treatment of alcohol use disorder: insights into the predictive value of animal and human laboratory models. Addiction Biology, 22(3), 581–615. 10.1111/adb.12349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zilverstand A, Huang AS, Alia-Klein N, & Goldstein RZ (2018). Neuroimaging impaired response inhibition and salience attribution in human drug addiction: A systematic review. Neuron, 98(5), 886–903. 10.1016/j.neuron.2018.03.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.