

Abstract
Objectives
Precise and quantitative assessment of the trend of cancer burden enables policymakers and health managers to prioritize diseases and allocate resources better. This infers what caused a decrease or increase in the rate of cancer occurrence, and if it denotes timing of implementation of a control measure, it presents the impact on the disease rate. This study’s objective was to evaluate trends in child and adult cancer in Iraq from 2000 onwards.
Methods
We used the registries of the Iraqi Ministry of Health that were gathered from all governorates from 2000–2016. Data were presented as incidence rates to depict the trends of different types of cancers distributed by age, gender, and governorates.
Results
Breast cancer witnessed a significant increase with predominance in females. Lung cancer rate increased significantly from 4.08 to 5.60/100 000 (p = 0.038), affecting males more than females. The brain cancer trend showed a bimodal pattern (two peaks in 2004 and 2011) with no significant trend change (p = 0.788). Both genders were similarly affected. The trend of stomach and colorectal cancer showed an accelerated increase after 2007.
Conclusions
Almost all cancers (particularly lung and gastrointestinal) showed constantly raising trends, especially after 2007. Only cervical and laryngeal cancer had a decreasing trend. Most cancers were predominant in males.
Keywords: Cancer, Trend, Incidence, Iraq
Introduction
Cancer represents a growing threat to public health worldwide with its incidence rates rising in most countries since 1990 due to population growth, aging, and the raised prevalence of unhealthy behaviors and certain risk factors, including smoking.1,2 The number of cancer cases reached 17.5 million worldwide, raised by 33% since 2005.3,4
The Republic of Iraq is an Arabic country located in the South-East of the Asian continent bordered by Turkey, Iran from the north and east; Jordan, Syria, Saudi Arabia, and Kuwait from the south and west; and one coastal margin at the north of Arabian Gulf. The capital is Baghdad. Iraq is characterized by diverse ethnic groups including Arab, Kurd, Turkmen, and others with two main official languages: Arabic and Kurdish. The total area of Iraq is about 438 000 km2 occupied by about 38 million population as 2018 estimate, with more clustering in the capital (about eight million). Iraq was in a state of continuous wars for the last four decades that caused great damage to the infrastructure of the health care services. The prevalence of some cancer risk factors (obesity, smoking, unhealthy diet, diabetes) has recently changed in Iraq with no sufficient preventive measures been implemented. Iraq has high incidence rates in breast, lung, and bladder cancers, besides a growing burden of many others.5
Precise and quantitative assessment of the trend of cancer burden enables policymakers and health managers to prioritize diseases and allocate resources better, infer what caused a decrease or increase in the rate of cancer occurrence, and if it denotes timing of implementation of a control measure, it presents the impact on the disease rate.6
This study was designed to be a descriptive analysis. We did not aim to prove any relation between the weaponry used during the last US invasion to Iraq (2003) and the change in the trend of cancer as digging for causal relation needs a long prospective design that was not feasible at that time from a practical point of view considering the available resources.
The objective of the study was to sketch a picture for the trend of different types of cancer in Iraq during this time of chaos (attributed to continuous conflicts) that caused severe damage to the infrastructure of the health care services (and all the supporting services like electricity, safe water supply, and environmental health) in addition to the change in the lifestyle of the people.
Methods
In this descriptive study, we used the Surveillance Department of the Iraqi Ministry of Health registries, which were gathered from all governorates’ health directorates and health facilities from 2000 to 2016. These data were supported and confirmed by the Iraqi cancer centers, chemotherapy and radiotherapy centers, and then referred to the Iraqi Cancer Board. Data were presented as incidence rates, reviewed, double-checked, and analyzed to depict the trends of different types of cancers in Iraq distributed by age (regarding child cancer), gender, and governorates, the total of each disease for each governorate was computed, and then summed to obtain the total for Iraq. We categorized Iraq geographically into three regions to ease sketching the trend. These were: the North region including Erbil, Sulaymaniyah, Dohuk, and Nineveh; the Middle region including Baghdad, Babel, Najaf, Karbala, Al-Qadisiyah, Salaheddin, Diyala, Anbar, Kirkuk, and Wasit; and the South region that includes Basrah, ThiQar, Missan, and Muthanna.
The total population for each governorate (and for Iraq) was obtained from the Central Statistical Organization. We subdivided child cancer into three age categories; less than five, five to less than 10, and 10 to less than 15 years old.
Data about different adult and child cancers were collected with more focus on the most prevalent cancers, namely: breast, lung and bronchus, bladder, brain, cervix, ovary, prostate, larynx, stomach, colon, rectum, liver, pancreas, and thyroid, in addition to leukemia, Hodgkin, and non-Hodgkin lymphoma.
Data after 2016 were not available as cancer data are usually collected, analyzed, and interpreted every four years. We used SPSS Statistics (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) to treat the data and estimate the rates.
Results
Breast cancer had witnessed a significant increase (p = 0.007) with predominance in the female gender (female to male ratio 29:1) mostly in the adult age group. Lung cancer rate increased significantly from 4.08 to 5.60/100 000 (p = 0.038). It affected males more than females with a ratio of 3:1, and tends to increase with age. The brain cancer trend showed a bimodal pattern (two peaks in 2004 and 2011) with no significant trend change (p = 0.788). Both genders and age groups were similarly affected [Figure 1].
Figure 1.
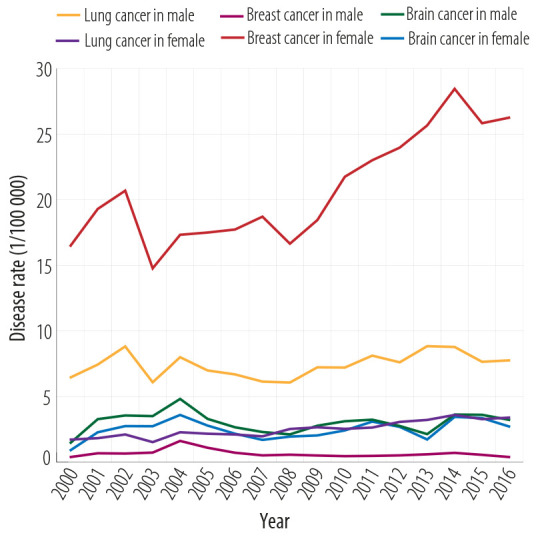
Breast, brain, and lung cancer.
Bladder cancer depicted a non-significant change over the studied period. Male cases were three times more than female’s with predominance in the > 45 years age group. The rate of ovarian cancer significantly increased since 2007, while the trend of cervical cancer went down significantly (p = 0.008). The prostatic cancer rate significantly rose over the study period from 1.85 to 4.13 (p = 0.041) [Figure 2].
Figure 2.
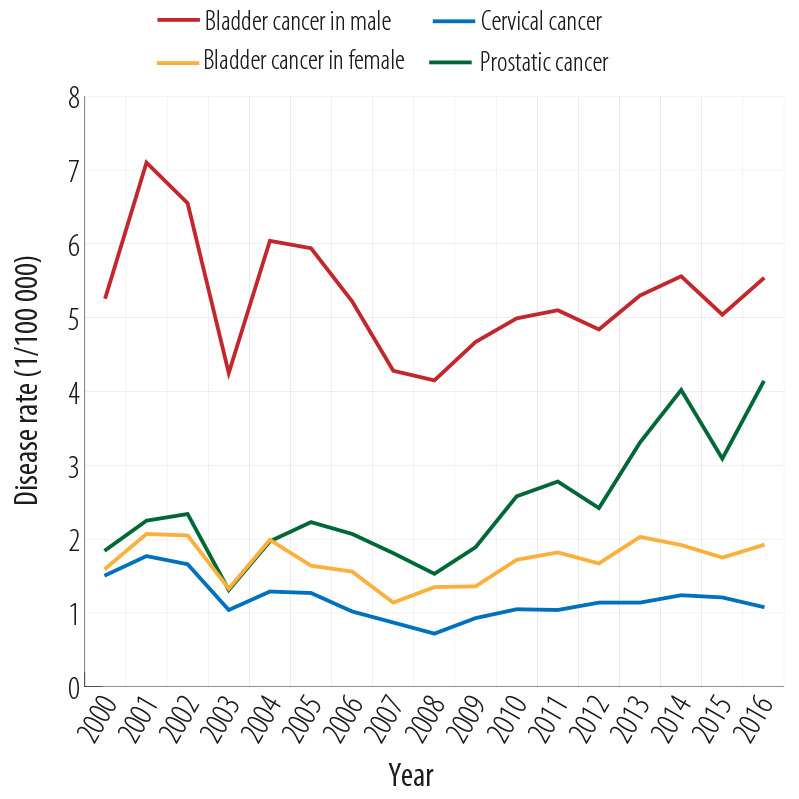
Rates of bladder, cervical, and prostatic cancer from 2000 to 2016.
Figure 3 demonstrates the trend of gastrointestinal cancers; stomach cancer showed an accelerated increase in the rate after 2007 (p < 0.001). Both genders showed similar rates, and the prevalence increased with age. Colorectal cancer depicted a significant increase in occurrence after 2007 (p < 0.001). Both genders were similarly affected. Liver cancer started with a rate of 0.40/100 000 in the year 2000, with a peak in 2005, then increased from 2008 to 2016 (0.82/100 000 to 1.91/100 000). Both genders were equally affected.
Figure 3.

Rates of stomach, liver, and colorectal cancer from 2000 to 2016.
Thyroid cancer showed a significantly elevated trend since 2007 from 0.62 to 2.96/100 000 (p = 0.003). The male to female ratio was 2.5:1. Pancreatic cancer more than doubled between the years 2000 and 2016 from 0.72 to 1.46/100 000. The trend of laryngeal cancer presented a significant down slopping rate. Males were affected more than females with a ratio of 3:1 [Figure 4].
Figure 4.
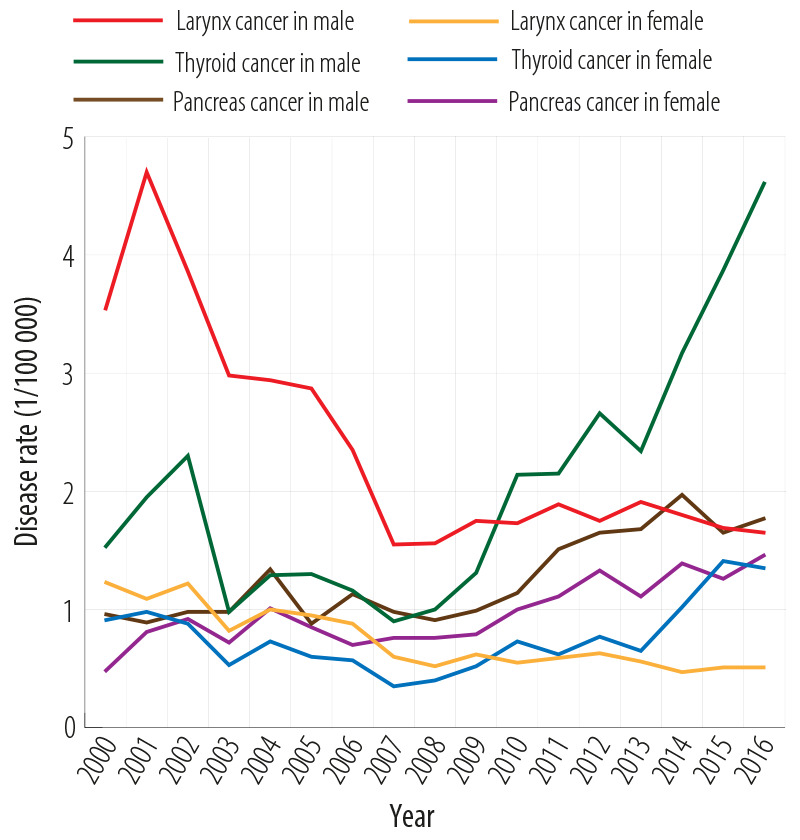
Rates of thyroid, larynx, and pancreas cancers from 2000 to 2016.
Leukemia showed a non-significant increasing trend, started with a rate of 3.24/100 000 in 2000 and ended with a rate of 4.37 in 2016 with a peak of 5.9 in 2004, both genders were equally affected. Hodgkin disease also showed a non-significant increase (from 1.40 to 1.44/100 000), affecting both sexes equally, while non-Hodgkin lymphoma showed a significant increase in its rate from 2007 forward, affecting both genders equally [Figure 5]. Skin cancer showed a gradual decrease to 2008, followed by a gradual increase for both sexes.
Figure 5.
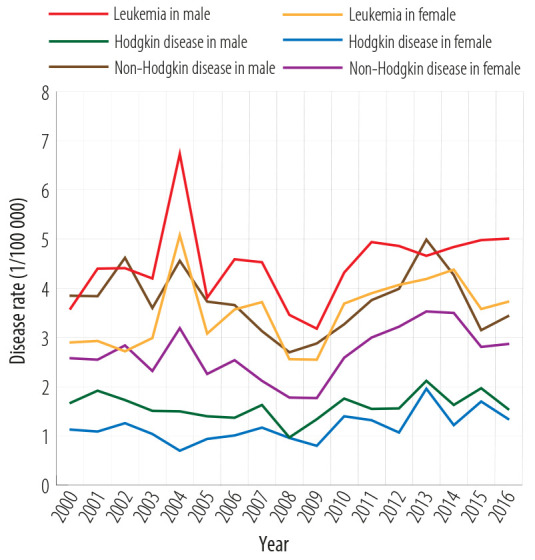
Rates of leukemia, Hodgkin’s, and non-Hodgkin’s disease from 2000 to 2016.
The trends of childhood cancer have not significantly changed over the studied time. It tended to affect males more than females (1.5:1) and was slightly higher in children less than five years of age [Figure 6].
Figure 6.

Rates of child cancer distributed by age groups between 2000 and 2016.
Figure 7 shows the trend of total cancer in Iraq by governorates. The Middle region showed the highest trend followed by the South and then the North.
Figure 7.

Total cancer rate in Iraq distributed by Iraq province from 2000 to 2016.
Table 1 shows the percent change in all cancers’ incidence rate for the periods 2000–2008, 2008–2016, and 2000–2016.
Table 1. Percent change in cancer incidence rates.
| Cancer type | Rate 2000 | Rate 2008 | Percentage change 2000–2008 | Rate 2016 | Percentage change 2008–2016 | Percentage change 2000–2016 |
|---|---|---|---|---|---|---|
| Breast | 8.43 | 8.56 | 1.54 | 13.19 | 54.09 | 56.47 |
| Lung | 4.08 | 4.31 | 5.64 | 5.60 | 29.93 | 37.25 |
| Brain | 1.17 | 2.03 | 73.50 | 2.97 | 46.31 | 153.85 |
| Bladder | 3.44 | 2.76 | -19.77 | 3.75 | 35.87 | 9.01 |
| Stomach | 1.80 | 1.48 | -17.78 | 2.04 | 37.84 | 13.33 |
| Colorectal | 2.43 | 2.07 | -14.81 | 3.74 | 80.68 | 53.91 |
| Liver | 0.40 | 0.82 | 105.00 | 1.91 | 132.93 | 377.50 |
| Pancreatic | 0.72 | 0.76 | 5.56 | 1.46 | 92.11 | 102.78 |
| Skin | 2.23 | 1.15 | -48.43 | 1.92 | 66.96 | -13.90 |
| Larynx | 2.40 | 0.52 | -78.33 | 0.51 | -1.92 | 78.75- |
| Thyroid | 1.22 | 0.70 | -42.62 | 2.96 | 322.86 | 142.62 |
| Leukemia | 3.24 | 3.01 | -7.10 | 4.37 | 45.18 | 34.88 |
| Hodgkin’s disease | 1.40 | 0.97 | -30.71 | 1.44 | 48.45 | 2.86 |
| Non-Hodgkin’s disease | 3.20 | 2.24 | -30.00 | 3.16 | 41.07 | 1.25 |
| Ovarian | 2.11 | 1.78 | -15.64 | 3.05 | 71.35 | 44.55 |
| Cervical | 1.51 | 1.02 | -32.45 | 1.14 | 11.76 | -24.50 |
| Prostate | 1.85 | 1.53 | -17.30 | 4.13 | 169.93 | 123.24 |
| Childhood | 9.55 | 7.34 | -23.14 | 9.92 | 35.15 | 3.87 |
| All cancers* | 51.18 | 44.58 | -14.50 | 67.86 | 51.73 | 29.73 |
*Includes other rare cancers (not mentioned).
Discussion
The trend of total cancers in Iraq from 2000–2016 showed an overall increase, more obvious after 2007. This can not be explained merely by improving case detection or registration as the health system is still suffering from many weaknesses. Many factors are thought to be responsible for this increase, related mainly to the successive wars since 1980 that caused great devastation of the infrastructure, especially that of the health system.7-9 However, as this study was designed to be a descriptive one to sketch the trend of cancer in time of war, this design did not allow us to prove a causal relationship between different types of cancer and the probable risk factors like radioactive contamination or changes in the lifestyle.
The rate of cancers had increased from 44.58 to 67.86/100 000 from 2008–2016 with a percent change of more than 50%. This finding goes with a similar regional and global trend, but these were more gradual and stepwise. The global trend of 2005–2015 had a percent change of 6.4%.10 Unfortunately, we could not find previous reliable studies in Iraq about cancer trends before the war to compare.
The breast cancer incidence rate increased progressively from 8.43 in 2000 to 8.56/100 000 in 2008 (1.54% change) and then to 13.19 in 2016 (54.09% change). This increase is classically thought to be related to a higher prevalence of some known risk factors like smoking, high body mass index, physical inactivity, low intake of fruits/vegetables, and family history of breast cancer in addition to age.11 Iran already has a higher incidence of breast cancer of 22/100 000 but with a percent change of 15.2, while it is 12.9/100 000 in Saudi Arabia.12-14 In Oman, the 20-year trends data show breast cancer to be the most common malignancy affecting Omani women (21.2% of all cancer cases).15
The lung cancer incidence rate increased from 4.08 in 2000 to 4.31 in 2008 up to 5.60 in 2016, still lower than many regional countries. The median Arab countries rate is 16.33/100 000.16 The burden of lung and breast cancers is represented by their high mortality rate as they occupy the first leading cause of cancer deaths in both males and females respectively, higher in low- and middle-income countries,17 this is in addition to their financial burden as the estimated per patient cost of breast cancer can reach up to US$ 15 000.18
The brain cancer trend showed a bimodal pattern (two peaks in 2004 and 2011) with no significant trend change, and both genders were similarly affected. A significantly raised trend was seen from 2000–2004 that regressed down later to 2.03 to increase again in 2008 and thereafter, but ended with a rate of 2.97 in 2016. This rate was lower than the regional countries such as Jordan and Iran (5.1 and 2.74/100 000 respectively), and the global rate (3.4/100 000).19 However, weak registration and the preference of most patients to seek treatment outside Iraq (attributed to the distrust in the deteriorated health system) might serve in the apparently low incidence of brain cancer compared to some of the regional countries. Brain tumors are considered the most common solid tumors that develop during childhood comprising 20% of all neoplasm and the primary cause of cancer deaths in this age group.20 Those who survive may suffer long term sequels from the tumor or its treatment.21
The incidence rate of bladder cancer in 2016 was 3.75, rising from 3.44 in 2000. This rate is still lower than many regional countries such as Lebanon (18.8), Turkey (14.4), and Iran (7.7/100 000).22
Gastrointestinal cancers (including stomach, colorectal, liver, and pancreatic cancers) witnessed an overall rise in its trend that became steady and more significant after 2008. This was most obvious with liver cancer, which increased from 0.40 in 2000 to 1.91/100 000 in 2016. The same was true regarding stomach cancer that ended with a rate of 2.04/100 000, which was opposed by a declined trend worldwide23 and regionally, as in Oman.24 The raised trend of colorectal cancer was similar to other low- and middle-income countries, including regional countries where the trend was continuously rising, while it was stabilized or started to decrease in high-income countries.12,15,25
Although the occurrence of both liver and pancreatic cancers in Iraq is lower than the regional countries such as Iran26 or Saudi Arabia; the rapidity of increase in the rate of liver cancer is alarming (as these cancers were not commonly seen in Iraq previously), while it is decreasing in Saudi Arabia.27
The burden of these cancers is attributed mainly to their high mortality rate where after lung cancer, stomach, colorectal, and liver cancers represent the second, third and fourth leading causes of cancer deaths worldwide.3
Cancer of hematopoietic and lymphoid tissue including leukemia, Hodgkin’s, and non-Hodgkin’s lymphomas showed the same swinging trend to 2008, followed by a gradual rise to 2016. Leukemia rate increased from 3.24 to 4.37 with a peak in 2004 that reached up to 5.90/100 000. Such a trend was also seen in Saudi Arabia (3.15/100 000) and Iran (6.25/100 000).28,29
Cervical cancer was one of two cancers (the other was laryngeal cancer) that witnessed a decrease in its rate compared to that of the year 2000. It dropped down from 1.51/100 000 to 1.14 in 2016, apart from an increase in 2008 (1.02 /100 000). This goes with the trend of many countries as reported by the Globocan study,30 Saudi Arabia,27 and Jordan.31 Cervical cancer remains the fourth most common female cancer contributing to 7.5% of all female cancer deaths in 2012,19 but it forms l < 5% of female cancer deaths in Iraq.32
On the contrary, both ovarian and prostatic cancers showed a raised trend during the study period 2000–2016. The ovarian cancer incidence rate increased from 2.11 in 2000 to 3.05/100 000 in 2016 and prostatic cancer from 1.85 to 4.13/100 000 in 2016. Although the rising trend of prostatic cancer seems to be global,33 but the rapid increase in incidence by 2.2-fold indicates an alarming change in the occurrence of this cancer that needs a thorough searching for the possible changes in the risk factors. However, many regional countries have the same rising trend but with a higher incidence, like Iran (10.37/100 000)34 and Turkey (27.7/100 000).35 The burden of prostatic cancer is from its financial cost required for diagnosis, surgery, and post-surgical therapy with a minimum estimation of about US$ 5000.36 Prostatic cancer is the second most diagnosed malignancy and the fifth leading cause of cancer deaths in males with an age-standardized global mortality rate of 7.8/100 000 and a Western Asia rate of 13.7/100 000.33
Cancer of the larynx was the second cancer that witnessed a decrease in its trend over the study period. It went down from 2.40/100 000 to 0.51/100 000. Such a trend was also seen in Iran and Lebanon but with higher incidence rates (9.1 and 5.7/100 000, respectively).37,38 Thyroid cancer had an increased overall trend from 1.22 to 2.96/100 000, more evident after 2007 with a significant drop in 2003. This goes with the global trend of low and middle-income countries39 and regional countries such as Iran (2.2/100 000)40 and Jordan (2.6/100 000).41 These two cancers (larynx and thyroid) revealed a gender difference with male predilection in laryngeal cancer (male to female ratio 3:1) and female predilection in thyroid cancer (female to male ratio 3:1) that seems to be a worldwide trend.42
The trend of child cancer showed no significant change over the study period and remained between 9.55 and 9.92/100 000. This represents 7.5–8.5% of the total cancers in Iraq and a mean of 1000 child cancer per year. Although this goes with the global rate of 10/100 00043 and some regional rates such as Jordan (9.9/100 000)44 and Iran (17.5/100 000),45 there still is a burden from its high mortality that reaches up to 98% in the developing countries whereas it is as low as 15% in developed countries.46 A study in Iraq in 2007 concluded that childhood leukemia rates in Basra more than doubled over 15 years (1993–2007).47
The trend of total cancers in Iraq revealed a clear up slope especially after 2008, and particularly in the middle region, which might be attributed to the fact that this region was the main target during the 2003 war and exposed to a huge amount of bombing. However, cancer rates in Iraq seem to be lower than the regional and global rates. This might be due to poor registration, besides, many cancer cases in Iraq are diagnosed in the private sector, which is unfortunately not linked to the national surveillance system, and many of those patients seek treatment outside the country. This created a sort of underestimation.
As the primary data source was the registries of the Ministry of Health, there was no possible way to check for the completeness of data or the percentage of missing cases, therefore, validity could not be assured.
Conclusion
It can be concluded from the results of this study that almost all cancers (particularly lung and gastrointestinal) showed constantly raising trends, especially after 2007. Only cervical and laryngeal cancers had a dropping trend. Most of the cancers are predominant in males. Generally, if the trend kept on going in this ascending curve, then the coming years may witness (with better reporting) a dramatic increase in the trend of cancers in Iraq.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
References
- 1.Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, MacIntyre MF, et al. Global Burden of Disease Cancer Collaboration The global burden of cancer 2013. JAMA Oncol 2015. Jul;1(4):505-527 . 10.1001/jamaoncol.2015.0735 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Badwe RA, Dikshit R, Laversanne M, Bray F. Cancer incidence trends in India. Jpn J Clin Oncol 2014. May;44(5):401-407 . 10.1093/jjco/hyu040 [DOI] [PubMed] [Google Scholar]
- 3.Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, et al. Global Burden of Disease Cancer Collaboration Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 2017;3(4):524-548 . 10.1001/jamaoncol.2016.5688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.WHO. Cancer/ fact sheet/ media center. [cited 2018 April 1]. Available from: http://www.who.int/mediacentre/factsheets/fs297/en/.
- 5.WHO IARC. Estimated Cancer Incidence, Mortality and prevalence worldwide in 2012.fact sheet. Population fact sheet. [cited 2018 February 21]. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx.
- 6.Funk S, Bogich TL, Jones KE, Kilpatrick AM, Daszak P. Quantifying trends in disease impact to produce a consistent and reproducible definition of an emerging infectious disease. PLoS One 2013. Aug;8(8):e69951 . 10.1371/journal.pone.0069951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Fathi RA, Matti LY, Al-Salih HS, Godbold D. Environmental pollution by depleted uranium in Iraq with special reference to Mosul and possible effects on cancer and birth defect rates. Med Confl Surviv 2013. Jan-Mar;29(1):7-25 . 10.1080/13623699.2013.765173 [DOI] [PubMed] [Google Scholar]
- 8.AL-Hashimi M. Wang X. Trend of leukemia in Ninawa/Iraq. Clin Exp Med Sci 2013;1(5-8):353-362. [Google Scholar]
- 9.Lafta RK, Al-Nuaimi MA. War or health: a four-decade armed conflict in Iraq. Med Confl Surviv 2019. Sep;35(3):209-226 . 10.1080/13623699.2019.1670431 [DOI] [PubMed] [Google Scholar]
- 10.GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016. Oct;388(10053):1545-1602 . 10.1016/S0140-6736(16)31678-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lafta RK, Saeed EQ, Isa SA. Risk factors of breast cancer among women (A sample from Baghdad). IJCM 2013;26(1):1-6. [Google Scholar]
- 12.Rafiemanesh H, Salehiniya H, Lotfi Z. Breast cancer in iranian woman: incidence by age group, morphology and trends. Asian Pac J Cancer Prev 2016;17(3):1393-1397 . 10.7314/APJCP.2016.17.3.1393 [DOI] [PubMed] [Google Scholar]
- 13.Jazayeri SB, Saadat S, Ramezani R, Kaviani A. Incidence of primary breast cancer in Iran: Ten-year national cancer registry data report. Cancer Epidemiol 2015. Aug;39(4):519-527 . 10.1016/j.canep.2015.04.016 [DOI] [PubMed] [Google Scholar]
- 14.Alghamdi IG, Hussain II, Alghamdi MS, El-Sheemy MA. The incidence rate of female breast cancer in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001-2008. Breast Cancer (Dove Med Press) 2013. Oct;5:103-109 . 10.2147/BCTT.S50750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Al-Lawati NA, Al-Bahrani BJ, Al-Raisi SS, Al-Lawati JA. Twenty-year trends of cancer incidence in Omanis, 1996-2015. Oman Med J 2019. Jul;34(4):361-387. [PMC free article] [PubMed] [Google Scholar]
- 16.Salim EI, Jazieh AR, Moore MA. Lung cancer incidence in the arab league countries: risk factors and control. Asian Pac J Cancer Prev 2011;12(1):17-34. [PubMed] [Google Scholar]
- 17.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011. Mar-Apr;61(2):69-90 . 10.3322/caac.20107 [DOI] [PubMed] [Google Scholar]
- 18.Daroudi R, Akbari Sari A, Nahvijou A, Kalaghchi B, Najafi M, Zendehdel K. The economic burden of breast cancer in Iran. Iran J Public Health 2015. Sep;44(9):1225-1233. [PMC free article] [PubMed] [Google Scholar]
- 19.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015. Mar;136(5):E359-E386 . 10.1002/ijc.29210 [DOI] [PubMed] [Google Scholar]
- 20.Askari K, Janeshin S, Taherzadeh-Amlashi M, Seyed-Saadat S, Mashouf M. Central nervous system tumors in Guilan, Iran: Epidemiological Features Over 10 Years. Caspian Journal of Neurological Science 2015;1(1):19-26 . 10.18869/acadpub.cjns.1.1.19 [DOI] [Google Scholar]
- 21.Gunn ME, Lähdesmäki T, Malila N, Arola M, Grönroos M, Matomäki J, et al. Late morbidity in long-term survivors of childhood brain tumors: a nationwide registry-based study in Finland. Neuro Oncol 2015. May;17(5):747-756 . 10.1093/neuonc/nou321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pakzad R, Mohammadian-Hafshejani A, Mohammadian M, Pakzad I, Safiri S, Khazaei S, et al. Incidence and mortality of bladder cancer and their relationship with development in asia. Asian Pac J Cancer Prev 2015;16(16):7365-7374 . 10.7314/APJCP.2015.16.16.7365 [DOI] [PubMed] [Google Scholar]
- 23.Balakrishnan M, George R, Sharma A, Graham DY. Changing trends in stomach cancer throughout the world. Curr Gastroenterol Rep 2017. Aug;19(8):36 . 10.1007/s11894-017-0575-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Al-Mahrouqi H, Parkin L, Sharples K. Incidence of stomach cancer in oman and the other gulf cooperation council countries. Oman Med J 2011. Jul;26(4):258-262 . 10.5001/omj.2011.62 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017. Apr;66(4):683-691 . 10.1136/gutjnl-2015-310912 [DOI] [PubMed] [Google Scholar]
- 26.Almasi Z, Mohammadian-Hafshejani A, Salehiniya H. Incidence, mortality, and epidemiological aspects of cancers in Iran; differences with the world data. J BUON 2016. Jul-Aug;21(4):994-1004. [PubMed] [Google Scholar]
- 27.Bazarbashi S, Al Eid H, Minguet J. Cancer Incidence in Saudi Arabia: 2012 Data from the Saudi Cancer Registry. Asian Pac J Cancer Prev 2017. Sep;18(9):2437-2444. doi:. 10.22034/APJCP.2017.18.9.2437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Alghamdi IG, Hussain II, Alghamdi MS, Dohal AA, El-Sheemy MA. The incidence of leukemia in Saudi Arabia. Descriptive epidemiological analysis of data from the Saudi Cancer Registry 2001-2008. Saudi Med J 2014. Jul;35(7):674-683. [PubMed] [Google Scholar]
- 29.Koohi F, Salehiniya H, Shamlou R, Eslami S, Ghojogh ZM, Kor Y, et al. Leukemia in Iran: epidemiology and morphology trends. Asian Pac J Cancer Prev 2015;16(17):7759-7763 . 10.7314/APJCP.2015.16.17.7759 [DOI] [PubMed] [Google Scholar]
- 30.IARC. Cervical cancer, estimated incidence, mortality and prevalence worldwide in 2012. [cited 2018 April 12]. Available from: http://globocan.iarc.fr/old/FactSheets/cancers/cervix-new.asp.
- 31.Sharkas G, Arqoub K, Khader Y, Nimri O, Shroukh W, Jadallah H, et al. Trends in the incidence of cervical cancer in Jordan, 2000–2013. J Oncol 2017;2017:6827384 . 10.1155/2017/6827384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.WHO. Cancer Country Profiles-Iraq. [cited 2018 April 15]. Available from: http://www.who.int/cancer/country-profiles/irq_en.pdf.
- 33.Wong MC, Goggins WB, Wang HH, Fung FD, Leung C, Wong SY, et al. Global incidence and mortality for prostate cancer: analysis of temporal patterns and trends in 36 countries. Eur Urol 2016. Nov;70(5):862-874 . 10.1016/j.eururo.2016.05.043 [DOI] [PubMed] [Google Scholar]
- 34.Pakzad R, Rafiemanesh H, Ghoncheh M, Sarmad A, Salehiniya H, Hosseini S, et al. Prostate cancer in Iran: trends in incidence and morphological and epidemiological characteristics. Asian Pac J Cancer Prev 2016;17(2):839-843 . 10.7314/APJCP.2016.17.2.839 [DOI] [PubMed] [Google Scholar]
- 35.Zorlu F, Zorlu R, Divrik RT, Eser S, Yorukoglu K. Prostate cancer incidence in Turkey: an epidemiological study. Asian Pac J Cancer Prev 2014;15(21):9125-9130 . 10.7314/APJCP.2014.15.21.9125 [DOI] [PubMed] [Google Scholar]
- 36.Roehrborn CG, Black LK. The economic burden of prostate cancer. BJU Int 2011. Sep;108(6):806-813 . 10.1111/j.1464-410X.2011.10365.x [DOI] [PubMed] [Google Scholar]
- 37.Mirzaei M, Hosseini SA, Ghoncheh M, Soheilipour F, Soltani S, Soheilipour F, et al. Epidemiology and trend of head and neck cancers in Iran. Glob J Health Sci 2015. May;8(1):189-193 . 10.5539/gjhs.v8n1p189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Shamseddine A, Saleh A, Charafeddine M, Seoud M, Mukherji D, Temraz S, et al. Cancer trends in Lebanon: a review of incidence rates for the period of 2003-2008 and projections until 2018. Popul Health Metr 2014. Mar;12(1):4 . 10.1186/1478-7954-12-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer 2015. May;136(9):2187-2195 . 10.1002/ijc.29251 [DOI] [PubMed] [Google Scholar]
- 40.Safavi A, Azizi F, Jafari R, Chaibakhsh S, Safavi AA. Thyroid cancer epidemiology in Iran: a time trend study. Asian Pac J Cancer Prev 2016;17(1):407-412 . 10.7314/APJCP.2016.17.1.407 [DOI] [PubMed] [Google Scholar]
- 41.Sharkas GF, Tarawneh MR, Nimri OF. AL- Zughul MJ, Arqoub KH. Epidemiology of thyroid cancer in Jordan from 1996 to 2008. Middle East J Cancer 2011;2(3 & 4):117-123. [Google Scholar]
- 42.Dorak MT, Karpuzoglu E. Gender differences in cancer susceptibility: an inadequately addressed issue. Front Genet 2012. Nov;3:268. 10.3389/fgene.2012.00268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Fathi A, Bahadoram M, Amani F. Epidemiology of childhood cancer in northwest Iran. Asian Pac J Cancer Prev 2015;16(13):5459-5462 . 10.7314/APJCP.2015.16.13.5459 [DOI] [PubMed] [Google Scholar]
- 44.Ismail SI, Soubani M, Nimri JM, Al-Zeer AH. Cancer incidence in Jordan from 1996 to 2009–a comprehensive study. Asian Pac J Cancer Prev 2013;14(6):3527-3534 . 10.7314/APJCP.2013.14.6.3527 [DOI] [PubMed] [Google Scholar]
- 45.Khazaei S, Khazaei S, Mansori K, Ayubi E. Childhood cancer patterns in Iran: challenges and future directions. Iran J Public Health 2017. Aug;46(8):1145-1146. [PMC free article] [PubMed] [Google Scholar]
- 46.Haileamlak A. The Challenge of Childhood Cancer in Developing Countries. Ethiop J Health Sci 2016. May;26(3):199-200 . 10.4314/ejhs.v26i3.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hagopian A. Riyadh K Lafta, Tim K Takaro, Jenan Hassan, Scott Davis, Dana Mirick. Trends in childhood leukemia in Basra, Iraq, 1990-2007. AJPH June 2010 [cited 2018 May 1]. Available from: http://ajph.aphapublications.org/cgi/doi/10.2105/AJPH.2009.164236. [DOI] [PMC free article] [PubMed]