

Primary central nervous system lymphoma (PCNSL) is an uncommon, but aggressive non-Hodgkin lymphoma confined to the brain, leptomeninges, spinal cord, and eyes. Its incidence has increased substantially over the past decades among over 60-year-olds.1 The median age at diagnosis is around 65 years, and approximately onethird of newly diagnosed patients are >70 years.1 Nevertheless, elderly PCNSL patients, especially those over the age of 70 years, are frequently excluded from or under-represented in clinical trials due to concomitant comorbidities, poor performance status, or concerns regarding treatment-related sequelae.2,3 Prospective studies specifically designed for elderly PCNSL patients are scarce.4-6 Furthermore, the few available, somewhat outdated series mostly included relatively small numbers of patients (range, 10-107). These studies congruently showed that the prognosis of elderly patients remained poor and unchanged over the past decades, with overall survival (OS) ranging between 14-37 months. Collectively, apart from omitting consolidation radiotherapy after chemotherapy, the optimal treatment for elderly PCNSL patients is ill-defined.1,6,7
Population-based studies can complement prospective trials, especially in settings where data from prospective trials are scarce. At present, contemporary populationbased studies with detailed data regarding primary therapy specifically among >70-year old PCNSL patients to inform clinical practice are lacking. Therefore, in this contemporary, nationwide, population-based study, we assessed primary therapy and OS among >70 year old PCNSL patients diagnosed in the Netherlands.
Established in 1989, the nationwide Netherlands Cancer Registry (NCR) has an overall coverage of >95% of all malignancies in the Netherlands.8 We identified all >70-year old PCNSL patients diagnosed confirmed with cytology, histology, and/or flow cytometry between January 1st 2014 and December 31st 2017 from the NCR. Diffuse large B-cell PCNSL was defined using the International Classification of Diseases for Oncology morphology and topography codes (Online Supplementary Methods). Two patients diagnosed at autopsy were excluded. We included patients diagnosed from 2014 because the NCR has collected data on the therapeutic regimen from that year onwards. The NCR is based on comprehensive case notifications through the Nationwide Network of Histopathology and Cytopathology, and the National Registry of Hospital Discharges (i.e., outpatient and inpatient discharges). Information on dates of birth and diagnosis, sex, disease stage, topography, and morphology, performance score, and primary therapy was available for individual patients. This information is collected by trained registrars of the NCR through retrospective medical records review. Primary therapy was categorized into chemotherapy, radiotherapy only, and supportive care only. Corticosteroids are not standardly registered in the NCR and may have been given in all treatment groups. The category of chemotherapy was broken down by the exact therapeutic regimen. The Privacy Review Board of the NCR approved the use of anonymous data for this study.
The primary survival endpoint was OS, defined as the time from diagnosis until death. Patients were censored at emigration or end of follow-up (1st February 2019). OS was calculated for three age groups (71-74, 75-79, and ≥80 years) and according to primary treatment (chemotherapy, radiotherapy only, and supportive care only) using the Kaplan-Meier method. Survival distributions were compared with the log-rank test. Multivariable Cox regression was conducted to assess covariates (sex, age at diagnosis, a prior malignancy before PCNSL diagnosis, receipt of rituximab, and type of primary therapy) associated with OS. P<0.05 was considered statistically significant. Further details about the statistical analyses are available in the Online Supplementary Appendix.
Table 1.
Patients’ characteristics.
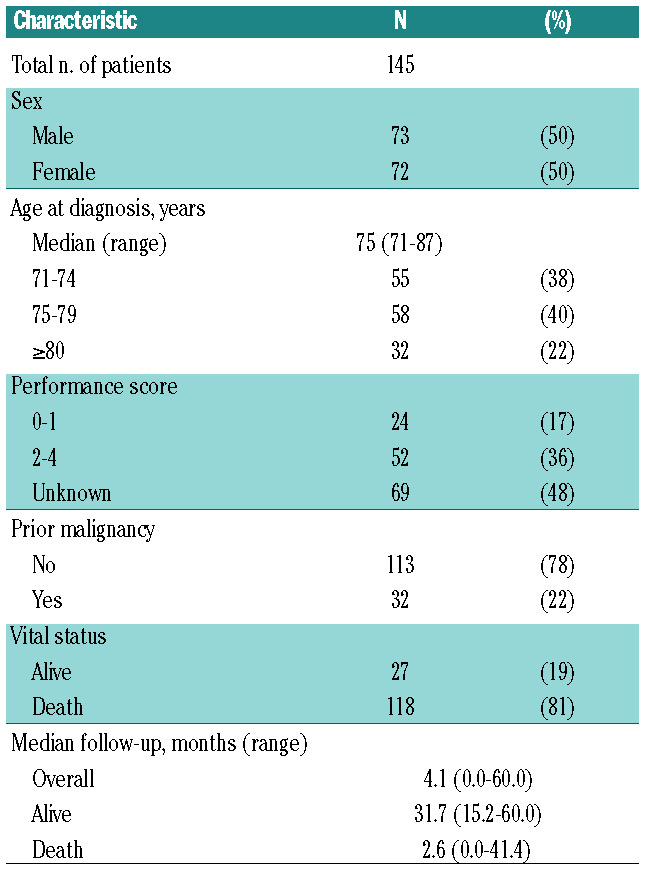
A total of 145 PCNSL patients >70 years old (50% males) were included in the study. Median age was 75 years (range, 71-87), with 55 (38%), 58 (40%), and 32 (22%) patients aged 71-74, 75-79, and ≥80 years at diagnosis, respectively (Table 1).
Overall, 43% of patients received chemotherapy, 20% radiotherapy only, and 37% supportive care only (Table 2). Numbers of patients receiving chemotherapy decreased with older age (58%, 40%, and 22% respectively across the three age groups), while radiotherapy only or supportive care only increased (P=0.002) (Table 2 and Online Supplementary Table S1). All 62 (43%) chemotherapy-treated patients except one were treated with either methotrexate (MTX) monotherapy (n=25) or a variety of MTX-based regimens (n=36) (Table 2). MTX with teniposide, carmustine, and prednisolone (MBVP) was the most commonly applied MTX-based regimen (25 of 36; 69%). Rituximab was added to chemotherapy in 17 of 62 (27%) patients (Table 2). Of note, 6 of 7 chemotherapy-treated patients aged ≥80 years were treated with MTX-monotherapy.
During follow-up, 118 (81%) patients died. The median follow-up of patients still alive was 31.7 months (range, 15.2-60.0). Overall, median OS was 4.1 months (95% confidence interval [CI]: 2.8-6.8) and 2-year OS was 25% (95%CI: 18%-32%) (Figure 1A). There were no significant differences in OS between the three age groups (P=0.185) (Figure 1B). The difference in OS between 71-74-year olds (7.7 months, 95%CI: 2.6-16.3) and those ≥75 years (3.9 months, 95%CI: 2.4-5.5) was also not statistically significant (P=0.08) (Online Supplementary Figure S1). OS according to primary treatment did show significant differences, with chemotherapy- treated patients having a superior median OS (16.3 months 95%CI: 7.8-35.2) compared with those who received radiotherapy only (7.7 months, 95%CI: 4.6-13.2) or supportive care only (1.4 months, 95%CI: 1.1-1.7; P<0.001) (Figure 1C). Two-year OS was 45% (95%CI: 32-57%) in those receiving chemotherapy, whereas it was exceedingly low in the other two treatment groups (Figure 1C). Multivariable Cox regression analysis revealed that primary treatment was the only factor associated with OS, whereas sex, age, a prior malignancy before PCNSL diagnosis, and receiving rituximab were not associated with OS (Online Supplementary Table S2). Excluding the four patients in the chemotherapy group who subsequently received whole-brain radiotherapy did not change survival estimates. Within the chemotherapy group, median OS for recipients of MTXmonotherapy was 5 months (95%CI: 2.6-41.4) and for MTX-based regimens 27 months (95%CI: 10.3-not reached) (Figure 1D) but was was not statistically significant (P=0.170). Also, and more importantly, the number of patients was too small to allow a meaningful comparison to be made. Therefore, a multivariable analysis of MTX only versus MTX-based regimens was not performed.
Figure 1.

Overall survival (OS) among patients over 70 years of age with primary central nervous system lymphoma in the Netherlands: 2014-2017. OS is shown for the total cohort (A), and according to age at diagnosis (B), treatment group (C), and the type of therapy with methotrexate (MTX) (D). The tables below (B-D) show the median OS, and the projected 1- and 2-year OS with associated 95% confidence intervals. CI: confidence interval.
In this contemporary, nationwide, population-based study among newly diagnosed PCNSL patients >70 years old we observed that the prognosis of these patients remains poor. This finding agrees with prior populationbased studies spanning the past decades.1
Age is a strong prognostic factor in adult PCNSL patients.9,10 However, within our study population of patients >70 years old, there was no clear prognostic gradient with increasing age, although with larger patient numbers, a statistically significant association between age and OS might be seen. Instead, despite the small patient numbers, treatment was a strong prognostic factor. Although only 22% of patients aged ≥80 years received chemotherapy (which possibly hints towards selection bias or confounding by indication) this finding suggests that treatment, more than age, influences survival in elderly patients judged fit enough to receive therapy. Selection bias might also have impacted MTXmonotherapy versusMTX-based chemotherapy; performance status and comorbidity, in particular renal insufficiency, might have influenced the choice of chemotherapeutic regimen.
Prior prospective studies provided evidence that highdose MTX, especially when combined with alkylating chemotherapy, is the most efficacious treatment for elderly PCNSL patients.11 Although there are conflicting data on the therapeutic value of chemoradiation over chemotherapy alone in elderly PCNSL patients,11,12 it is unquestionable that consolidation with radiotherapy in this population carries a high risk of neurotoxicity and severe cognitive decline.13
Controversy remains regarding the therapeutic value of rituximab in PCNSL. Findings from the current study and a recent randomized phase III trial among PCNSL patients aged 18-70 years showed no added therapeutic value of rituximab on survival outcomes.3 However, our results should be interpreted with caution given the low number of rituximab-treated patients. Similarly, a metaanalysis of 343 patients with PCNSL aged 50-67 years showed a possible positive effect of rituximab on PFS but not on OS.14 In contrast, a recent population-based study among 164 adult PCNSL patients diagnosed between 2005-2010 in Austria, of whom 40% were >70 years old, after a short follow-up (median 12 months) suggested that rituximab might increase survival.15
The strength of the current study is the use of a nationwide population-based cancer registry. As such, our findings are not compromised by selection and/or referral biases to the extent encountered in clinical trials. Therefore, our study represents the general population of elderly PCNSL patients. Limitations of our study mainly concern the lack of data throughout most of the registry on comorbidities, the use of corticosteroids, and the dose of steroids and chemotherapeutic agents, relapse rates, and salvage treatment. In addition, the performance score is poorly documented in medical records, thereby hampering its inclusion in the regression analyses due to the high percentage of unknown values (48%) (Table 1); this limits its contribution to the clinical decision-making process based on performance status.
In summary, in this nationwide, population-based study, survival among PCNSL patients >70 years old remains poor in contemporary clinical practice. Nevertheless, our data demonstrate that MTX-based multi-agent chemotherapy, as compared with radiothera py only and supportive care only, results in the best outcome in elderly patients judged eligible to receive such treatment, with a 2-year OS of approximately 50%. The challenge remains to balance the benefits and risks of intensive chemotherapy in this patient group. Therefore, future prospective intervention studies are needed to assess which elderly patients can benefit from intensive chemotherapy or less intensive approaches.
Table 2.
Detailed information on primary therapy in over 70-year old patients with PCNSL.

Supplementary Material
Acknowledgments
The authors would like to thank the registration clerks of the Netherlands Cancer Registry (NCR) for their dedicated data collection. The nationwide population-based NCR is maintained and hosted by the Netherlands Comprehensive Cancer Organisation (IKNL).
References
- 1.van der Meulen M, Dinmohamed AG, Visser O, Doorduijn JK, Bromberg JEC. Improved survival in primary central nervous system lymphoma up to age 70 only: a population-based study on incidence, primary treatment and survival in the Netherlands, 1989-2015. Leukemia. 2017;31(8):1822-1825. [DOI] [PubMed] [Google Scholar]
- 2.Ferreri AJM, Cwynarski K, Pulczynski E, et al. Whole-brain radiotherapy or autologous stem-cell transplantation as consolidation strategies after high-dose methotrexate-based chemoimmunotherapy in patients with primary CNS lymphoma: results of the second randomisation of the International Extranodal Lymphoma Study Group-32 phase 2 trial. Lancet Haematol. 2017;4(11):e510-e523. [DOI] [PubMed] [Google Scholar]
- 3.Bromberg JEC, Issa S, Bakunina K, et al. Rituximab in patients with primary CNS lymphoma (HOVON 105/ALLG NHL 24): a randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2019; 20(2):216-228. [DOI] [PubMed] [Google Scholar]
- 4.Omuro A, Chinot O, Taillandier L, et al. Methotrexate and temozolomide versus methotrexate, procarbazine, vincristine, and cytarabine for primary CNS lymphoma in an elderly population: an intergroup ANOCEF-GOELAMS randomised phase 2 trial. Lancet Haematol. 2015;2(6):e251-e259. [DOI] [PubMed] [Google Scholar]
- 5.Fritsch K, Kasenda B, Schorb E, et al. High-dose methotrexate-based immuno-chemotherapy for elderly primary CNS lymphoma patients (PRIMAIN study). Leukemia. 2017;31(4):846-852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Siegal T, Bairey O. Primary CNS lymphoma in the elderly: the challenge. Acta Haematol. 2019;141(3):138-145. [DOI] [PubMed] [Google Scholar]
- 7.Mendez JS, Ostrom QT, Gittleman H, et al. The elderly left behindchanges in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro Oncol. 2018;20(5):687-694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schouten LJ, Hoppener P, van den Brandt PA, Knottnerus JA, Jager JJ. Completeness of cancer registration in Limburg, The Netherlands. Int J Epidemiol. 1993;22(3):369-376. [DOI] [PubMed] [Google Scholar]
- 9.Ferreri AJ, Blay JY, Reni M, et al. Prognostic scoring system for primary CNS lymphomas: the International Extranodal Lymphoma Study Group experience. J Clin Oncol. 2003;21(2):266-272. [DOI] [PubMed] [Google Scholar]
- 10.Abrey LE, Ben-Porat L, Panageas KS, et al. Primary central nervous system lymphoma: the Memorial Sloan-Kettering Cancer Center prognostic model. J Clin Oncol. 2006;24(36):5711-5715. [DOI] [PubMed] [Google Scholar]
- 11.Kasenda B, Ferreri AJ, Marturano E, et al. First-line treatment and outcome of elderly patients with primary central nervous system lymphoma (PCNSL)--a systematic review and individual patient data meta-analysis. Ann Oncol. 2015;26(7):1305-1313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Korfel A, Thiel E, Martus P, et al. Randomized phase III study of whole-brain radiotherapy for primary CNS lymphoma. Neurology. 2015;84(12):1242-1248. [DOI] [PubMed] [Google Scholar]
- 13.Thiel E, Korfel A, Martus P, et al. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (GPCNSL- SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol. 2010;11(11):1036-1047. [DOI] [PubMed] [Google Scholar]
- 14.Schmitt AM, Herbrand AK, Fox CP, et al. Rituximab in primary central nervous system lymphoma- a systematic review and metaanalysis. Hematol Oncol. 2019;37(5):548-557. [DOI] [PubMed] [Google Scholar]
- 15.Neuhauser M, Roetzer T, Oberndorfer S, et al. Increasing use of immunotherapy and prolonged survival among younger patients with primary CNS lymphoma: a population-based study. Acta Oncol. 2019;58(7):967-976. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.