

ABSTRACT
The Coronavirus epidemic quickly spread in Italy from China. In particular, it affected Bergamo province where Romano di Lombardia hospital is situated. Therefore, this hospital felt the urgency to requalify its activity in no time. It transformed itself into a unique centralized subintensive department to treat COVID-19 patients.
The factors that made it possible to adequately face the stress due to patients’ hospitalization were human resources and innovative elements to provide oxygen therapy. It is to underline that the logistic and methodological reality was not planned to cope with this emergency.
KEYWORDS: COVID-19, reorganization, emergency, resilience
1. Introduction
In December 2019 an epidemic characterized by a severe lung disease caused by a new Coronavirus, named SARS-CoV-2, was described for the first time in the Chinese city of Wuhan, in Hubei province [1].
The first Italian case of disease due to SARS-CoV-2 was reported on 20 February 2020 in Codogno Hospital, in Lodi province [2]. But epidemiological evidences [3] prove that the virus was present, though unidentified, in a large area of Lombardy as from the very first days of 2020. In particular, Bergamo province was among the areas most severely affected by the new epidemic [4], with significantly high numbers of cases and victims (9,815 and 2,480 till 7 April 2020, respectively).
In this article, we describe the impact that the emergency due to SARS-CoV-2 has had in ‘SS. Trinità’ Hospital in Romano di Lombardia. Our hospital is one of ASST Bergamo Ovest Hospitals (Azienda Socio Sanitaria Territoriale di Bergamo Ovest, corresponding to Healthcare Public Centre of western Bergamo province), and it was in the heart of the epidemic epicenter.
2. The impact of the epidemic
When the epidemic started, Romano di Lombardia Hospital had:
-a Medicine Ward with 60 beds
-a Surgery/Orthopedy Ward with 24 beds
-a Rehabilitation Ward with 42 beds
-a Ward for Subacute patients with 18 beds
-an Emergency Room Department (ERD)
The first case of new Coronavirus disease (COVID-19) in Romano di Lombardia Hospital occurred on 23 February and the positivity was confirmed by a test on 25 February. It was the case of a 21-year-old woman hospitalized in the Medicine Ward. She suffered from interstitial pneumonia and therefore she was transferred to the Infectious Diseases Department of ‘Papa Giovanni XXIII’ Hospital in Bergamo.
As from 26 February, a specific area of the Hospital was dedicated to COVID-19 patients. It had nine beds and it was isolated from the other hospital wards. The situation suddenly got more and more critical. In some days, there were 14 patients hospitalized in ERD, 4–5 ambulances queuing while waiting to admit patients, and many more ambulances were invited to go to other hospitals by the Emergency Operative Centre 118.
The diagnosis of more SARS-CoV-2 infections in other patients and the high pressure on ERD urged to reorganize all the wards of the Hospital, unifying them from a functional point of view and employing all the medical, nursing, and sanitary staff in a unique structure to treat COVID-19 patients. Only the Rehabilitation Ward was closed. The hospital was then a new homogeneous COVID-19 department with 100 beds in total.
When the emergency started, the number of Non-Invasive Ventilation (NIV) devices we had was absolutely inadequate to our needs, being the main clinical goal to supply our patients with oxygen therapy in suitable concentration. To make things worse, there was an almost total shortage of more devices and NIV circuits, difficult to be found on the market.
Because of the almost complete absence of generators, handmade connections between available NIV circuits, oxygen distributors, and compressed air were created, so it was possible to supply oxygen concentration (FiO2) up to at least 30%, using positive end-expiratory pressure (PEEP) of 5–7,5-10 cm H2O.
As it was very difficult to find generators, the engineers and plumbers of our hospital helped to assemble devices with a better seal. These could supply oxygen concentrations up to 50–60%, so as to permit, in Non-Invasive Ventilation, the use of both face masks and continuous positive airway pressure (C-PAP) hoods, added to the normal oxygen supply in reservoir masks, Venturi masks, and nasal prongs.
These devices, obtained in a very short time, were placed in every Hospital room.
(Figure 1) by means of a Y-shaped metal connector we built the connection between the oxygen openings, the compressed air openings, and the corrugated pipe of the mask or of the NIV CPAP hood; inside the Y it is possible to insert a joint that permits to supply oxygen by means of Venturi mask or nasal prongs (when NIV is not necessary).
Figure 1.
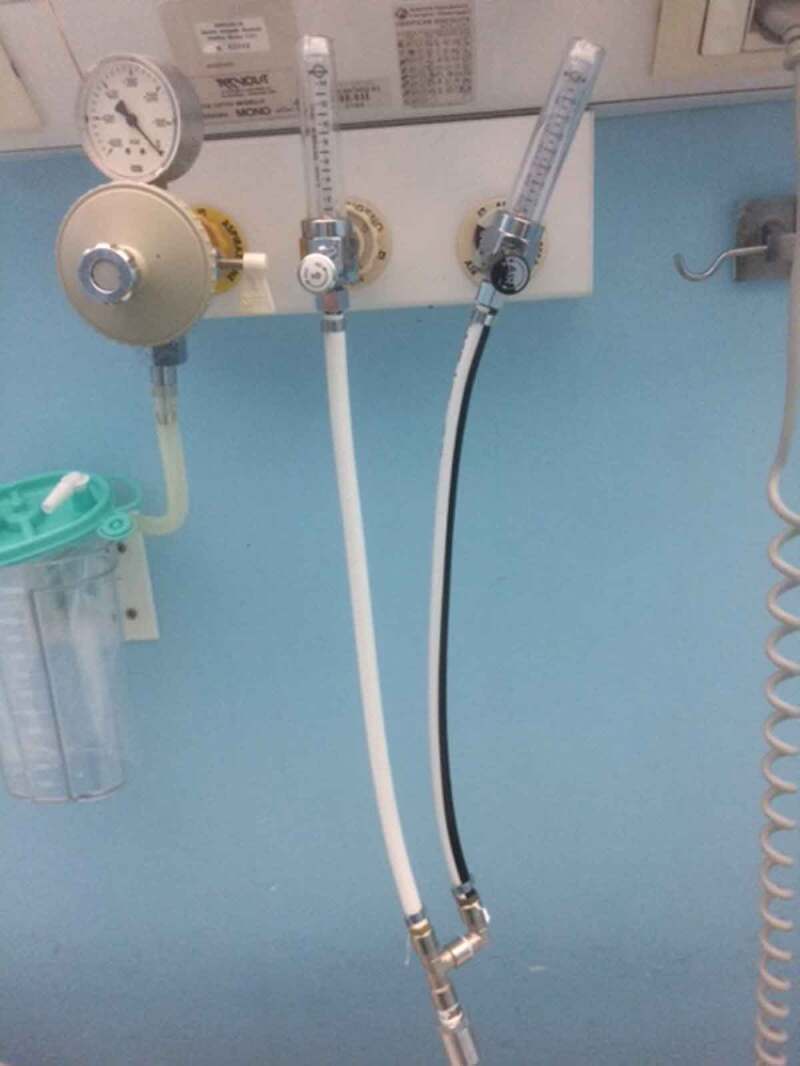
by means of a Y-shaped metal connector we built the connection between the oxygen openings, the compressed air openings and the corrugated pipe of the mask or of the NIV C-PAP hood; inside the Y it is possible to insert a joint that permits to supply oxygen by means of a Venturi mask or nasal prongs (when NIV is not necessary)
3. The organizing response
The wards that up to a few days before used to be ordinary hospital wards were converted into a unique large subintensive therapy ward with 100 beds.
ERD continued accepting patients for usual emergencies, but these patients were later sent to other hospitals. So also ERD was concretely transformed into another Subintensive Therapy Ward with 12 more beds and the possibility to offer NIV in the way mentioned above.
The management of the entire Hospital was granted by the medical and nursing staff working there on duty in that period:
-internal doctors, including two infectious disease specialists and one cardiologist
-surgeons
-orthopedicians
-rehabilitation specialists including two pneumologists and two cardiologists
-all the nurses and sanitary staff of the Hospital
Anaesthesists granted their presence in active shifts all day long and not only on call, as before COVID-19 emergency, acting also in the Operating Theatre on intubated patients, waiting to be moved to an Intensive Care Unit (ICU), which is not present in Romano di Lombardia Hospital.
Normal activity was carried out in the ERD by medical, nursing, and sanitary staff.
4. New organization and methodology of the clinical work
The system of work of the sanitary staff was modified and constantly updated according to our patients’ clinical and attendance needs. This implied a continuous learning of theoretical and practical technical notions.
The Crisis Board located in the hub Hospital in Treviglio coordinated all the work done by our Hospital. This made it possible to assist patients in the best way, with the resources available, while working in a situation of constant emergency. Sometimes the sanitary team was incomplete, because some members affected by COVID-19 were absent.
The operating management was carried out homogeneously by all the staff also thanks to:
-clinical-organizational daily briefings
-active contributions to find strategies to face critical structural aspects of a hospital that had to offer subintensive assistance standard, without an ICU
The clinical management of our hospitalized patients mainly followed:
-the Guidelines of the Lombardy section of SIMIT (Italian Society of Infectious and Tropical Diseases), which were in constant evolution and continuously updated [5]
-the internal protocol, arranged with Treviglio hub Hospital, constantly redefined in the team and then transformed into concrete official operating instructions of work [6]
All the doctors and nurses acquired theoretical and practical knowledge to cope with Non-Invasive Ventilation (use of face masks, C-PAP hoods, patients’ pronation), antiviral, anti-inflammatory, sedative, and palliative therapies.
Our patients were not allowed to receive visits from their relatives, so our sanitary staff represented the only link between patients and their families. Therefore, every doctor also had the task to keep regular daily phone contacts with patients’ families to give medical information. In addition, Red Cross staff organized video calls so that it was possible for patients to see and talk to their loved ones.
5. Statistical Data
In the six-week period between 26 February and 7 April 1187 patients arrived at our ERD; 343 of them were hospitalized.
Out of all the patients hospitalized:
-222 were clinically cured, dismissed, and sent home or to hotels for quarantine
-24 were moved to ICU elsewhere, because their clinical conditions required intubation
-97 died
As to the total number of patients that arrived at our ERD:
-343 were hospitalized; 199 directly and 144 after temporary observation
-632 were dismissed and sent home
-34 were transferred to other hospitals
-44 returned for further visits
-95 left ERD premises
-12 were dismissed after temporary observation
-2 refused to be hospitalized
-25 died in our ERD
Table 1.
Total number of beds in Romano di Lombardia Hospital in pre-COVID period
| Medicine ward | 60 | |||||
| Surgery/Orthopedy ward | 24 | |||||
| Rehabilitation ward | 42 | |||||
| Subacute patients ward | 18 | |||||
| Total number | 144 | |||||
Table 2.
Total number of beds in Romano di Lombardia Hospital during Sars-CoV-2 epidemic
| New Subintensive COVID-19 ward | 100 | ||||
| Emergency Room ward | 12 | ||||
| Total number of beds | 112 | ||||
Table 3.
Total number of access to Romano di Lombardia ERD from 26 February to 7 April
| Patients subsequently admitted in Subintensive COVID-19 ward | 343 | ||||
| Patients managed and/or cured directly in ERD | 844 | ||||
| Total number of patients | 1187 | ||||
Table 4.
Patients admitted in the subintensive COVID-19 ward from 26 February to 7 April
| Patients resigned healed or sent somewhere else for quarantine | 222 | ||||
| Patients transferred to other ICU for aggravation | 24 | ||||
| Patients deceased in ward | 97 | ||||
| Total number of patients | 343 | ||||
Table 5.
Patients managed in ERD from 26 February to 7 April
| Patients discharged from ERD | 632 | ||
| Patients transferred to other Hospitals | 34 | ||
| Patients discharged with check-up recommended | 44 | ||
| Patients leaving ERD by own decision | 95 | ||
| Patients discharged after intensive short observation | 12 | ||
| Patients refusing hospitalization | 2 | ||
| Patients deceased in ERD | 25 | ||
| Total number of patients | 844 | ||
During the emergency the most important critical aspects were:
-the lack of adequate possibilities to obtain Non-Invasive Ventilation systems suitable to the requirements
-the rapid increase in the number of patients that needed hospitalization (in a few days our 100 beds were fully occupied)
-the clinical needs which could undergo a quick worsening evolution and require intensive care
-hard-working shifts for the staff on duty
-the shortage of sanitary staff due to disease. It is to underline that, thanks to the availability and to an adequate and constant use of individual protective equipment of all the healthcare staff, it was possible to limit the professional exposure (in both Treviglio and Romano Hospitals only 9.6% of the sanitary staff was positive to the virus)
-the emotional-relational stress especially when dealing with dead patients’ families
Therefore, the daily moments of clinical-organizational briefings were used also to improve the way to cope with working stress and to sidetrack hidden or evident situations of burn out.
6. Conclusions
The COVID-19 emergency has shown that it is possible to prepare structures of complex and advanced clinical management in a very short period, starting from low/medium intensive treatment wards thanks to:
-a complete revision of methods, programs, and working actions
-a rapid adaptation of all the staff to the changed and urgent new clinical/assistance necessities of patients
In this critical emergency it was possible to efficiently convert our Hospital into a COVID-19 Hospital thanks to some indispensable requisites:
-the generosity of all the staff
-the resilience in acquiring organizational methods and theoretical/practical notions previously unknown
-the cooperation at any level with the counterparts in Treviglio hub Hospital, with a company overview approach, which will probably have positive effects also when the present emergency is over.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- [1].Zhu N, Zhang D, Wang W, et al. China novel coronavirus investigating and research team. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020. February 20;382(8):727–733. Epub 2020 Jan 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Grasselli G, Pesenti A, Cecconi M.. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy. Early experience and forecast during an emergency response. JAMA. Published online 2020. March 13. DOI: 10.1001/jama.2020.4031 [DOI] [PubMed] [Google Scholar]
- [3].Zehender G, Lai A, Bergna A, et al. Genomic characterisation and phylogenetic analysis of SARS-COV-2 in Italy. medRxiv preprint. 2020. DOI: 10.1101/2020.03.15.20022870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Invernizzi I In tutti i paesi, decessi in crescita esponenziale. L’Eco di Bergamo, 2020. March 4.
- [5].SIMIT Società Italiana di Malattie Infettive e Tropicali – Sezione Regione Lombardia . Vademecum per la cura delle persone con malattia da COVI-19. Edizione. 2020. 13:1–15 marzo;2.0. [Google Scholar]
- [6].Istruzione Operativa Gestione paziente ricoverato affetto da COVID-19 (IODS59), ASST Bergamo Ovest, 1 April 2020