

Abstract
Children raised in families with low socioeconomic status (SES) are more likely to exhibit symptoms of psychopathology. However, the strength of this association, the specific indices of SES most strongly associated with childhood psychopathology, and factors moderating the association are strikingly inconsistent across studies. We conducted a meta-analysis of 120 estimates of the association between family SES and child psychopathology in 13 population-representative cohorts of children studied in the US since 1980. Among 26,715 participants aged 3–19 years, we observed small to moderate associations of low family income (g = 0.19), low Hollingshead index (g = 0.21), low subjective SES (g = 0.24), low parental education (g = 0.25), poverty status (g = 0.25), and receipt of public assistance (g = 0.32) with higher levels of childhood psychopathology. Moderator testing revealed that receipt of public assistance showed an especially strong association with psychopathology and that SES was more strongly related to externalizing than internalizing psychopathology. Dispersion in our final, random effects, model suggested that the relation between SES and child psychopathology is likely to vary in different populations of children and in different communities. These findings highlight the need for additional research on the mechanisms of SES-related psychopathology risk in children in order to identify targets for potential intervention.
Keywords: Socioeconomic status, Childhood, Adolescence, Psychopathology, Population health
1. Introduction
Children from low-SES families often have higher levels of psychopathology than their peers from higher-SES families, although the strength of this association and the particular aspects of SES that are most strongly related to child mental health differ across studies (Bradley & Corwyn, 2002; Duncan & Brooks-Gunn, 1999; Reiss, 2013; Yoshikawa, Aber, & Beardslee, 2012). Likewise, the strength of association between SES and child psychopathology may vary across different forms of psychopathology and as a function of age and intersecting identities including race, ethnicity, and gender in ways that are poorly understood. Examination of the relative strength of these associations may allow us to better discern which aspects of SES are most strongly associated with child psychopathology, with implication for studies on mechanisms underlying this association and, ultimately, intervention. Here, we present a meta-analysis of studies reporting on the associations of a wide range of SES metrics with child and adolescent psychopathology. We focus our meta-analysis on population-representative samples from the United States that are designed to allow inferences at the population-level. We examine variability in the strength of these associations across different domains of psychopathology, SES measures, and socio-demographic factors.
1.1. SES and child psychopathology
Family SES is conceptualized and measured in many different ways (Bradley & Corwyn, 2002; Diemer, Mistry, Wadsworth, López, & Reimers, 2013; Shavers, 2007). Most studies measure SES using one or more indices of a family’s access to resources, raising important questions about which of these indices of SES are most related to children’s psychopathology. We define SES as a family’s access to a variety of forms of resources, often measured using separate indices. These include economic (material resources such as money), human (e.g. non-material resources such as education), and social resources (e.g. resources available through social networks and connections) (Bradley & Corwyn, 2002; Coleman, 1988; Krieger, Williams, & Moss, 1997). Importantly, many reviews on SES measurement in psychology argue that family SES cannot be captured by a single index or by averaging separate indices, but instead must combine multiple sources of information synergistically (Bradley & Corwyn, 2002; Duncan & Magnuson, 2003). Nevertheless, most studies continue to use a small number of easily collectable measures. These measures have different strengths and weaknesses and vary in their ability to model particular SES-related risk pathways. Consequently, different SES measures may have distinct associations with child psychopathology (Duncan & Magnuson, 2003). Indeed, many studies have reported that child psychopathology is more strongly associated with one SES measure vs. another, but which effect is strongest varies between studies (Call & Nonnemaker, 1999; Davis, Sawyer, Lo, Priest, & Wake, 2010; Duncan & Brooks-Gunn, 1999; Loeber, 1998; McLaughlin, Costello, et al., 2012; McLeod & Shanahan, 1993).
1.1.1. Income and poverty
Family income and derived measures such as poverty status are the most widely utilized indices of SES. Although family income has been linked to childhood psychopathology, including in experimental designs (Costello, Compton, Keeler, & Angold, 2003; Gennetian & Miller, 2002; Yoshikawa, Aber, & Beardslee, 2012), this association has not always been replicated (Call & Nonnemaker, 1999; McLaughlin, Costello, et al., 2012). Among other factors, this variability could reflect the ways in which income is measured. Commonly used income measures include total family income (typically reported in ordinal bins rather than as a specific number), poverty status (income above or below the federal poverty line for a family of a given size), and family income proportional to the poverty line (income-to-needs ratio) (Diemer et al., 2013).
Indices lending themselves to the investigation of differences between families with very low income vs. all other families (such as poverty and receipt of public assistance), are often used as proxy measures for material hardship (i.e., whether a family is struggling to meet their basic needs) (Diemer et al., 2013; Gershoff, Aber, Raver, & Lennon, 2007). If material hardship drives associations of SES with child psychopathology, we would expect associations between income and psychopathology to be strongest when comparing families with very low income to those with moderate or high income who are less likely to face hardship. However, there is evidence of an SES gradient in health outcomes, including childhood psychopathology, across the entire income spectrum. Although physical and mental health problems in children and adults are most pronounced among people living in poverty, there is no threshold after which increased income is no longer associated with improved health outcomes (Goodman, 1999; Marmot, Ryff, Bumpass, Shipley, & Marks, 1997; Singh-Manoux, Adler, & Marmot, 2003). In other words, income is still associated with health outcomes across the entire income distribution, even in those with high enough income that scarcity (of food, medical care, or shelter) is unlikely to drive the association (Goodman, 1999; Marmot et al., 1997; Singh-Manoux et al., 2003). This pattern is not easily explained by hardship models. These separate pathways could produce differences in the strength of association of dichotomous versus continuous measures of SES with child psychopathology, as dichotomous measures of poverty or receipt of public assistance are more likely to reflect financial hardship, and continuous measures of income or income-to-needs ratio are more likely to reflect resource access across the SES spectrum.
1.1.2. Parental education
Parent education provides a measure of human (rather than material) capital in the family that is typically more stable than income (Diemer et al., 2013; Duncan & Magnuson, 2003) and that has been associated with child psychopathology in a number of studies (Call & Nonnemaker, 1999; Davis, Sawyer, Lo, Priest, & Wake, 2010; McLaughlin, Costello, et al., 2012). Educational background may influence parenting behaviors, parental investment, and the amount of cognitive stimulation that children experience in the home environment (e.g. increased language exposure and availability of learning materials)—all of which may influence psychopathology risk (Conger & Donnellan, 2007; Duncan & Magnuson, 2003; Hackman, Gallop, Evans, & Farah, 2015; Harris, Terrel, & Allen, 1999). As with income, parent education is often treated as a dichotomous variable. ‘Low parental education’ is often defined as a child having no parents who graduated high school. It is unclear if the use of a threshold is appropriate. For example, levels of psychopathology in adolescents whose parents completed some college but did not earn a degree may be as high or higher than levels of psychopathology in adolescents whose parents did not complete high school (McLaughlin, Costello, et al., 2012; Merikangas et al., 2010).
1.1.3. Composite measures
Composite SES measures, such as the Hollingshead Four Factor Index (Hollingshead, 1975), seek to summarize or combine information from multiple individual indices of SES. Ultimately, composites reduce the amount of information available for analysis and are not recommended (Bradley & Corwyn, 2002; Duncan & Magnuson, 2003). Several studies have shown no association between commonly used SES composite measures and child psychopathology (Twenge and Nolen-Hoeksema, 2002), and these null associations sometimes belie substantial associations between component SES measures and psychopathology (Call & Nonnemaker, 1999). In a study on parenting behaviors, Callahan and Eyberg (2010) found that the parent income, occupation, and education components of the Hollingshead considered separately predicted three times as much variance in behavior than the over-all Hollingshead composite score. Despite their limitations, composite measures are still frequently used.
1.1.4. Subjective social status
A final method for assessing SES utilizes subjective appraisals of SES. Subjective measures attempt to address limitations of single indices of SES by relying on respondents to summarize their overall SES in ways that more specific measures cannot (Andersson, 2018; Singh-Manoux et al., 2003). Subjective social status has shown robust associations with psychopathology in adolescents. In a nationally representative US sample of adolescents, youth who rated themselves as 1 rung higher on the school ladder had 14% lower odds of meeting criteria for a mental disorder, and were 21% less likely to meet criteria for a disruptive behavior disorder after controlling for other SES variables, a larger association than for any other SES measure (McLaughlin, Costello, et al., 2012). A meta-analysis by Quon and McGrath (2014) suggests that the direction of this association is relatively consistent across a variety of subjective SES measures and types of psychopathology in adolescents. While promising, subjective measures of SES have not been reported on as extensively in the literature as other measures, especially in population representative studies.
1.2. Variation across different forms of child psychopathology
The strength of association between SES and child psychopathology may differ by psychopathology domain. In particular, family SES is often more strongly associated with externalizing than internalizing psychopathology in children (Duncan & Brooks-Gunn, 1994; Lansford et al., 2006; Slopen, Fitzmaurice, Williams, & Gilman, 2010; Strohschein, 2005). However, the magnitude of this difference varies between study populations (Reiss, 2013), and a number of population-representative studies reported little evidence of moderation (W. Bor et al., 1997; McLaughlin, Costello, et al., 2012) or found that SES has stronger associations with internalizing psychopathology (Vollebergh et al., 2006; Wight, Botticello, & Aneshensel, 2006). This heterogeneity could be accounted for by an interaction where different SES measures are more strongly associated with internalizing versus externalizing symptoms or vice versa. For example, Velez, Johnson, and Cohen (1989) found that maternal education was associated with several forms of psychopathology, but income was only associated with externalizing psychopathology. Alternately, sample age may moderate the strength of association of SES with some forms of psychopathology but not others. Strohschein (2005) found that SES was associated with internalizing and externalizing psychopathology but that associations with internalizing psychopathology were attenuated with increasing age. Overall, the evidence suggests that externalizing psychopathology in children may be more strongly associated with family SES than internalizing symptoms, but the magnitude of this difference varies between populations for reasons that are poorly understood (Reiss, 2013).
1.3. Potential moderators of the association of SES with child psychopathology
Associations of SES with childhood psychopathology should be examined in the context of other demographic moderators in an intersectional framework. Structural factors (i.e. racism, sexism, and other forms of structural stigma) contribute to disparities in psychopathology in children as a function of sex, race, ethnicity, sexual orientation, and other identities (Alegria, Vallas, & Pumariega, 2010; Hatzenbuehler, Phelan, & Link, 2013; Zahn-Waxler, Shirtcliff, & Marceau, 2008). It is imperative to examine how these aspects of identity moderate the association of SES with childhood psychopathology (Bowleg, 2012). Indeed, variation in the strength of the SES-psychopathology association across different identities may contribute to inconsistent findings in the existing literature (Bradley & Corwyn, 2002). However, few such moderators have found consistent support. Although sex has sometimes been hypothesized to interact with SES in predicting both internalizing (Mendelson et al., 2008) and externalizing disorders (Piotrowska, Stride, Croft, & Rowe, 2015), empirical findings are mixed (Reiss, 2013). Interactions with age have been somewhat more consistent. Associations of psychopathology with family SES are often larger in younger children versus adolescents (Bradley & Corwyn, 2002; Duncan & Brooks-Gunn, 1999; Reiss, 2013), but similar across early and middle childhood (Duncan & Brooks-Gunn, 1994). Finally, although it has been hypothesized that children from racial/ethnic groups that have experienced systemic oppression and discrimination might be more vulnerable to developing psychopathology in low-SES environments (Duncan & Brooks-Gunn, 1999), many studies have found stronger associations of SES with psychopathology in Non-Hispanic White children than children from racial/ethnic minority groups (Costello, Keeler, & Angold, 2001; Dohrenwend et al., 1992; McLaughlin, Costello, et al., 2012; McLeod & Edwards, 1995), and still others have found no interaction between SES and race/ethnicity (McLeod & Shanahan, 1993). Overall, differences in the strength of association between family SES and child psychopathology in samples showing different compositions of age, sex, and race/ethnicity have not been fully explored.
An additional moderator of interest is historical period. Income inequality in the United States has increased in the past four decades and health inequities may correspondingly have changed over time (J. Bor, Cohen, & Galea, 2017). We are unaware of prior work examining whether the magnitude of the association between SES and child psychopathology has changed over time.
Lastly, estimates of the observed association between family SES and child psychopathology could vary based on study quality factors. Both low-SES and child psychopathology put burdens on families which make research participation more difficult, and lower participation rates of these populations makes sampling bias a serious concern in research on these topics (Ellard-Gray, Jeffrey, Choubak, & Crann, 2015; Granero Pérez, Ezpeleta, & Domenech, 2007). The use of probability sampling and proper sample weights in analysis can correct for this bias, making these practices important methodological moderators (Hernán, Hernández-Díaz, & Robins, 2004; Loeber, 1998). Additionally, while the most accurate estimates of childhood psychopathology utilize combined data from multiple reporters (Achenbach, McConaughy, et al., 1987; Cantwell, Lewinsohn, Rohde, & Seeley, 1997), many survey studies rely on a single reporter. Bias resulting from this limitation can be modeled by including psychopathology reporter as a study moderator. Finally, best practices in meta-analysis suggest including statistical adjustment as a potential moderator, in order to capture the potentially increased accuracy of effects which are controlled for covariates without limiting the number of effects available for analysis (Voils, Crandell, Chang, Leeman, & Sandelowski, 2011).
1.4. The present study
Herein, we present a meta-analysis of population-representative studies reporting on the association between family SES and child and adolescent psychopathology. Our first aim is to estimate the overall strength of the association between SES and psychopathology. Second, we examine variation in the strength of association across different measures of SES. Third, we investigate whether the strength of these associations vary across the two main classes of child psychopathology: externalizing vs internalizing problems. Finally, we test whether the strength of associations of SES with child psychopathology are moderated by sample demographics (sex, age, or race/ethnicity), study quality factors (adjustment for covariates, sample probability weighting, and psychopathology reporter), or study year. To obtain the most reliable estimates, we only include population-representative studies using well-characterized study populations which employed probability sampling to reduce sampling bias. Since such studies typically generate many papers, our approach was to conduct a meta-analysis of cohorts, as opposed to papers, in order to avoid incorporating duplicate associations from multiple papers using data from the same sample. We anticipated that these effects might vary substantially in different countries, for example with differences in levels of income inequality (Lund et al., 2010; Willms & Somer, 2001) or because of the varying relevance of specific indices of SES across different cultural contexts (Patel & Klein-man, 2003). For this reason, we focus only on U.S. samples.
2. Methods
2.1. Cohort identification
A cohort was defined as a set of study participants recruited as part of the same study and reported on as a sample across multiple papers. For example, the Great Smoky Mountains study contributed a single cohort. The Pittsburgh Youth Study contributed three cohorts, as three age groups were reported separately in publications (e.g., Loeber, 1998). A preliminary list of cohorts was constructed by identifying papers describing population-representative studies of psychopathology in youth that also collected data on family SES. Searches in PsychInfo, Pubmed, and Google Scholar were performed to identify papers that that: 1) reported on population-representative samples; 2) measured psychopathology; and 3) included children or adolescents (detailed search parameters are provided in appendix A). 73 Cohorts were identified for possible inclusion. Cohorts were screened according to the following criteria:
Included a validated measure of at least one of the following SES related measures: a) family income, b) parental education, c) receipt of public assistance, d) poverty status, e) subjective social status, or f) the Hollingshead Four Factor Model (Hollingshead, 1975). With the exception of subjective social status, SES measures reported by the child were not utilized.
Included a validated dichotomous (clinically thresholded) or continuous (severity) measure of at least one of the following psychopathology outcomes: a) ADHD, b) PTSD, c) depression, d) anxiety disorder, e) disruptive behavior disorder (e.g. operational defiant disorder, conduct disorder), f) internalizing psychopathology, g) externalizing psychopathology.
Recruited a sample that was representative of a clearly defined population of interest within the contiguous United States (e.g., children and caregivers from New York City). An adequate strategy for enumerating the population of interest prior to sampling and probability-based sampling was required.
Included participants between 5 and 18 years of age (inclusive). This range was selected as children below the age of 5 are not commonly assessed in population-representative studies of psychopathology, and those older than 18 are considered adults for psychological assessment purposes and may be expected to be economically independent from caregivers.
Examined a normative (typically developing) community sample. For example, samples recruited from mental health clinics, the juvenile justice system, or foster care were not included, as effect sizes in those samples would not be representative of the population at large.
Were published from 1980-present in English language journals.
The final analysis included effects from 13 cohorts (see Appendix A, Table A.1 for cohort descriptions; Fig. 1 for exclusion reasons).
Fig. 1.
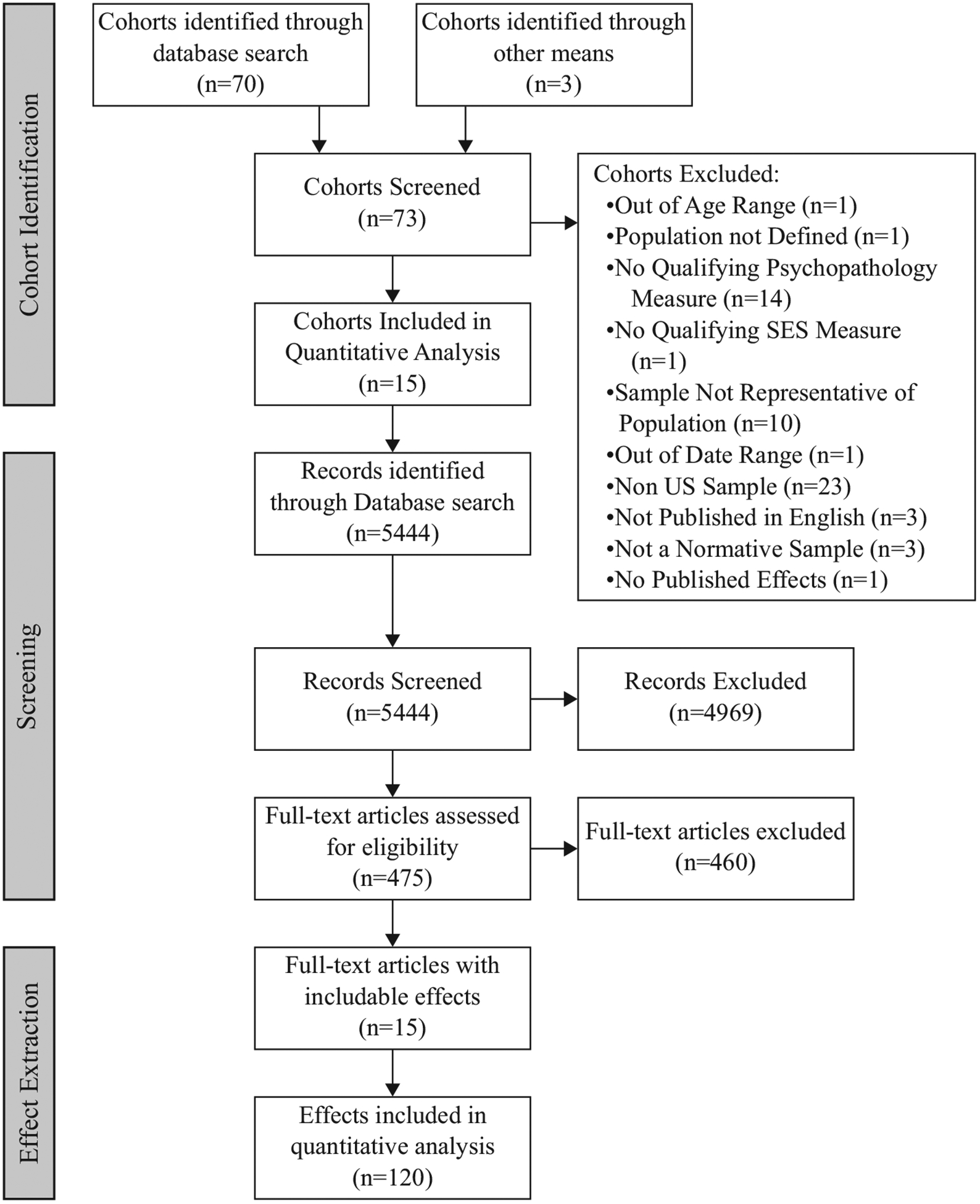
Search flow diagram.
2.2. Paper identification and review
For each cohort, a chronological list of publications was generated by database search and evaluated for review. PubMed was searched for the full name of the study in quotation marks. When associations of interest were not identified in the PubMed search, additional papers were identified by examining the full list of papers citing the initial study description paper, and/or Google Scholar searches for the name of the study in quotation marks followed by the name of the missing outcome variable. Abstracts were reviewed and relevant papers were examined for effects (see Fig. 1). Summary statistics and/or relevant data from 5 cohorts were provided by study authors (see Table A.1).
2.3. Article review, effect extraction, and coding
To avoid duplicating effects from the same cohort, a table delineating all possible effects (i.e., a table of SES measures × psychopathology measures) from each cohort was generated based on measures available in each study. We then identified papers that examined the full representative sample of the source study and reported at least one valid association of SES with psychopathology measured at the same time point. These papers were reviewed in chronological order and the first published effect of each type from each cohort was extracted (e.g., the first reported association of family income with externalizing symptoms). Wherever possible, unadjusted effects (e.g., bivariate correlation) were considered rather than adjusted effects (e.g., regression coefficients in a larger model). Only the first wave of data was included from longitudinal studies, except when investigators provided multiple waves in data files. A total of 120 effects were selected for inclusion in the final meta-analysis. Effect size and moderator coding was conducted exclusively by the first author.
SES variables were coded for maximal consistency between cohorts. For example, the most common reported measure of dichotomous income was family above/below the federal poverty line. Therefore, wherever possible poverty indicators were reduced to a dichotomous measure of family above/below poverty line (e.g., a study reporting a 2 × 3 frequency table of diagnoses in families with income proportional to the poverty line in bins of below 1, 1–2, and > 2 would be reduced to a 2 × 2 table of diagnosis in families above/below the poverty line). Similarly, parent education was coded wherever possible as a dichotomous measure of whether at least one parent had completed high school. When data were available, ordinal (binned) income variables were recoded as continuous income by taking the mid-point of each bin.
Psychopathology variables were coded as representing internalizing or externalizing psychopathology. Psychopathology measures were additionally coded as representing either continuous psychopathology (symptoms) or a dichotomous assessment of a diagnosis or significant level of impairment. Continuous measures of psychopathology were typically reported as broad, transdiagnostic assessments of symptom levels (e.g., the internalizing problems scale from the Child Behavior Checklist). Therefore, we did not enter continuous measures of diagnosis-specific psychopathology unless no measure of continuous internalizing/externalizing psychopathology was available for a particular cohort in order to maximize our ability to compare effects.
Effects were additionally coded for demographic and methodological moderators. Demographic moderators included average sample age, percent of sample that was female, racial composition of sample (percent identifying as Non-Hispanic White and percent identifying as Black, as these were the only values available across all cohorts), and study collection date (a year was selected for each cohort from the middle of the reported collection period). Methodological moderators included adjustment by covariates, type of diagnostic measure used (combined assessment vs. single reporter), and proper utilization of sample weights in calculation.
2.4. Effect size computation
Prior to meta-analysis and in line with statistical best practice, bias-free effect size parameters were calculated for each effect according to variable type (i.e., log odds ratio, standard mean difference, or correlation). Effects were then converted to Hedge’s g, an index of standard mean difference (interpreted identically to Cohen’s d) to allow for comparison between studies. Conversion formulas are listed in appendix B.
2.5. Analytic strategy
In order to model heterogeneity and account for non-independence of effect sizes, all effects were entered in to a three-level random-effects model in which variance was separately estimated between subjects (sampling variance), within cohorts, and between cohorts using restricted maximum likelihood estimation (Assink & Wibbelink, 2016). To further account for within-study dependent effects, we conducted sensitivity tests on all models using an imputed ‘high estimate’ of covariance between effects and found no significant variation in results.
Modeling was implemented in R v. 3.5.1 using the metafor package (v2.0–0; Viechtbauer, 2010). 95% Intervals were calculated for both confidence (resulting from error) and precision (resulting from observed dispersion of effects). Moderator tests were estimated separately for each potential moderator. A final model was then constructed using a model building approach: moderators with a significant Q(M) test, as well as corresponding interaction terms, were entered step wise into a series of combined models estimated using maximum likelihood. These models were then compared with the bivariate model and each other using log likelihood ratio tests and by comparing values of Akaike’s Information Criterion (AIC) in order to select a final model. Publication bias was controlled for by analysis of a funnel plot and a test for moderation based on whether an effect was a central finding of a publication (and thus subject to publication bias); these procedures produced little evidence that publication bias distorted our findings. Further details on analytic strategy and bias are available in appendix A and analysis code is available in appendix B. The IRB of the University of Washington approved all study procedures.
3. Results
The combined sample represented 26,715 children across the contiguous United States. The sample was 50.4% female, 47.45% Non-Hispanic White children, and 27% Black children. The sample was comprised of children aged 3–19, with an average age of 12.35 years. Of the effects entered, 53% used combined methods (multiple reporters) to assess psychopathology, and 86.7% were unadjusted for covariates. Most associations (85%) were taken from papers in which the association of family SES on psychopathology was not a primary focus of the work.
3.1. Overall association of SES with child psychopathology
In a bivariate model pooling all effects, lower SES was associated with a 0.25 standard deviation increase in child psychopathology (95% CI [0.18, 0.32]; see Table 1, Fig. 2).
Table 1.
Bivariate model summaries
| Model | K | est. [CI] | p | PI | σ2 (between) | σ2 (within) | Q | p(Q) |
|---|---|---|---|---|---|---|---|---|
| Full bivariate model: | 120 | g = 0.25*** [0.18,0.32] | <0.001 | [−0.05,0.55] | 0.016 [0.007,0.040] | 0.007 [0.004,0.012] | 497.17*** | <0.001 |
| Effects on symptoms: | ||||||||
| Parent Ed. | 10 | g = 0.25*** [0.14,0.35] | <0.001 | [−0.01,0.50] | 0.011 [0,0.076] | 0.003 [0,0.041] | 23.48* | 0.005 |
| Poverty | 10 | g = 0.25*** [0.13,0.38] | <0.001 | [−0.07,0.58] | 0.019 [0,0.125] | 0.004 [0,0.042] | 34.22*** | <0.001 |
| Public assistance | 12 | g = 0.26*** [0.14,0.37] | <0.001 | [−0.07,0.59] | 0.014 [0,0.090] | 0.011 [0,0.066] | 45.83*** | <0.001 |
| Income | 10 | r = −0.07 [−0.14,0] | 0.057 | [−0.24,0.10] | 0.006 [0.002,0.042] | 0 [0,0.002] | 54.42*** | <0.001 |
| Hollingshead | 5 | g = −0.09 [−0.22,0.04] | 0.172 | [−0.34,0.16] | 0.010 [0,0.209] | 0.002 [0,0.040] | 31.51*** | <0.001 |
| Effects on diagnosis: | ||||||||
| Parent Ed. | 21 | OR = 1.68*** [1.39,2.03] | <0.001 | [1.09,2.59] | 0.023 [0,0.206] | 0.016 [0,0.113] | 25.98 | 0.166 |
| Poverty | 21 | OR = 1.69*** [1.29,2.23] | <0.001 | [0.85,3.38] | 0.104 [0.026,0.553] | 0.002 [0,0.055] | 57.43*** | <0.001 |
| Public assistance | 14 | OR = 2.15*** [1.60,2.87] | <0.001 | [1.03,4.48] | 0.118 [0,0.532] | 0.001 [0,0.293] | 74.81*** | <0.001 |
| Income | 10 | g = −0.31*** [−0.40,−0.21] | <0.001 | [−0.49,−0.12] | 0.006 [0,0.100] | 0 [0,0.017] | 12.12 | 0.207 |
p < .05.
p < .001.
Fig. 2.

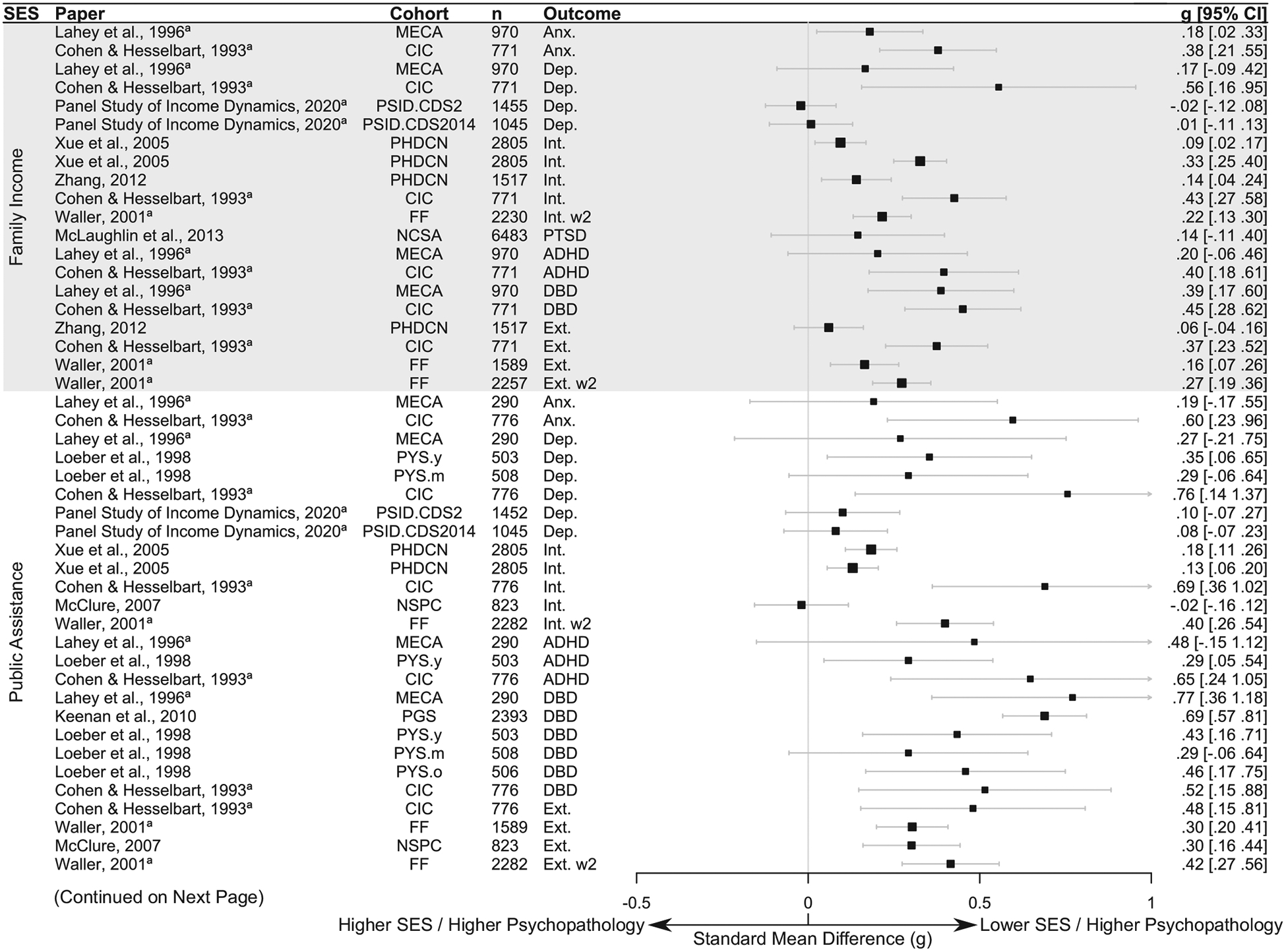
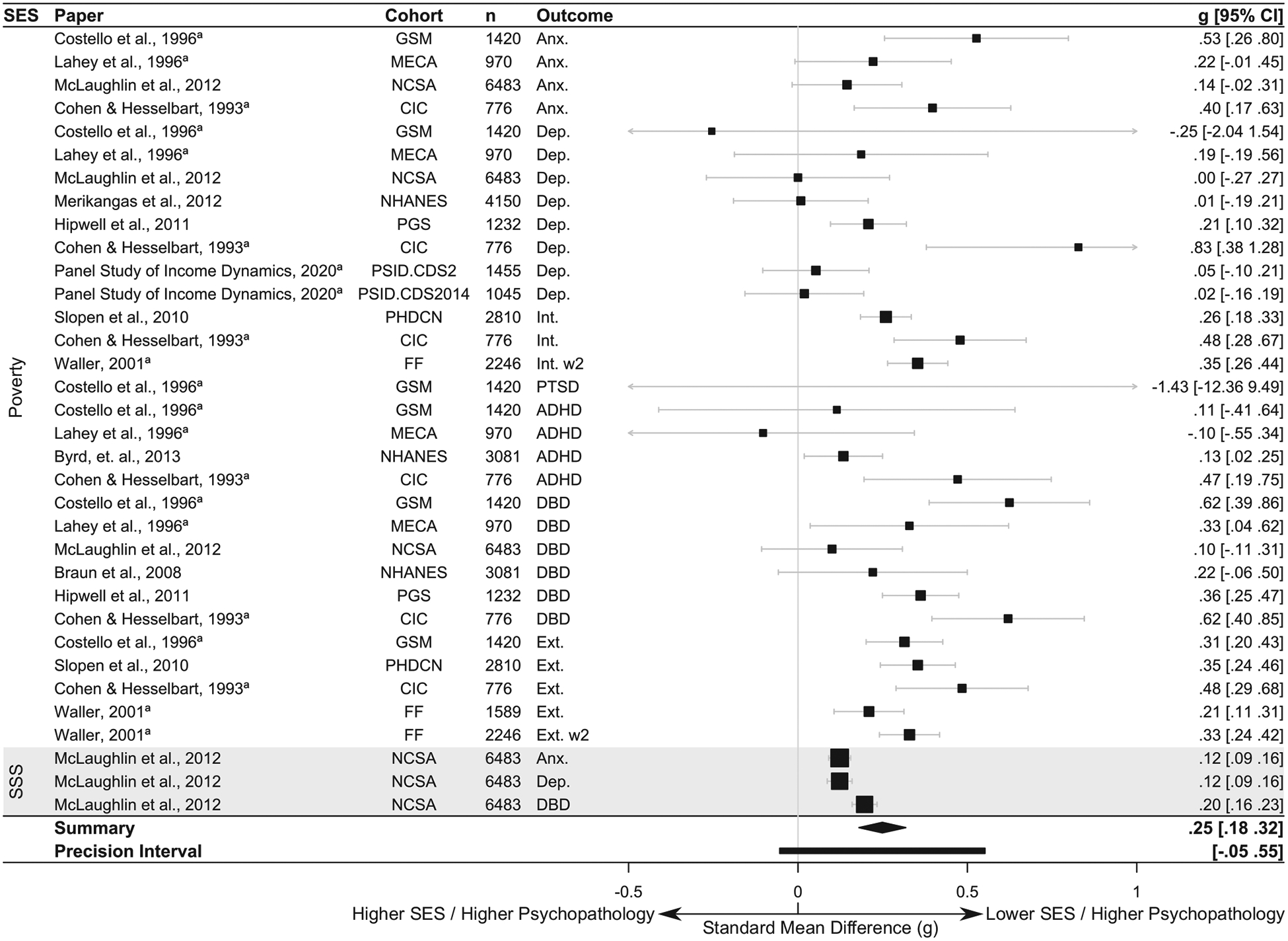
Forest plot of SMD (g) in psychopathology associated with low SES across SES and outcome measures (bivariate model). SSS=Subjective Social Status. a: effects were derived from data or summary statistics provided in correspondence with study authors.
3.2. Moderators of the association of SES with child psychopathology
The overall effect size of SES with child psychopathology varied significantly across specific SES measures, QM(5) = 12.87, p = .0246, and between externalizing and internalizing psychopathology, QM(1) =4.71, p = .03. No other moderators approached significance (all p < .45).
A model in which both SES index and psychopathology domain (internalizing versus externalizing) were entered together as moderators fit the data better than the bivariate (un-moderated) model by multiple fit indices. This moderated model fit the data similarly as a model that additionally included an interaction between these two moderators. We therefore selected the simpler model, without interactions, as our final model. Results from the model including an interaction between these two moderators as well as fit indices for each of these models are reported in Appendix B.
This final model suggested that every index of low-SES was associated with higher levels of internalizing and externalizing psychopathology in childhood, but that the size of this difference varied by both SES measure and psychopathology domain (see Table 2). Model predicted effect sizes, from lowest to highest, of each index of family SES with psychopathology (i.e. internalizing or externalizing) were low family income (g = 0.19), Hollingshead index (g = 0.21), low subjective SES (g = 0.24), poverty status (g = 0.25), low parental education (g =0.25), and receipt of public assistance (g = 0.32). Low-SES was associated with a higher standard mean difference in externalizing psychopathology (g = 0.28) versus internalizing psychopathology (g = 0.22) across SES measures.
Table 2.
Final model summary.
| Interaction model: | b | SE | p | 95% CI | |||
|---|---|---|---|---|---|---|---|
| Intercept (Family Income+Internalizing) | 0.165 | *** | 0.045 | <0.001 | 0.076 | - | 0.253 |
| Hollingshead | 0.022 | 0.068 | 0.751 | −0.112 | - | 0.156 | |
| Parental Ed | 0.063 | 0.039 | 0.088 | −0.009 | - | 0.135 | |
| Poverty status (poverty line) | 0.058 | 0.035 | 0.100 | −0.011 | - | 0.127 | |
| Receipt of public assistance | 0.129 | *** | 0.038 | <0.001 | 0.055 | - | 0.203 |
| Subjective SES | 0.047 | 0.068 | 0.471 | −0.084 | - | 0.181 | |
| Externalizing | 0.056 | * | 0.026 | 0.030 | −0.005 | - | 0.106 |
All moderator estimates represent deviation in SMD (g).
p < .05.
p < .001.
Moderation of the association between SES and child psychopathology by SES index and psychopathology type are illustrated in Fig. 3. The final model showed a significant test of moderation, QM(6) = 17.75, p = .01, as well as a significant test of residual heterogeneity after moderation was accounted for, QE(113) = 367.64, p < .0001. Residual heterogeneity appeared to be higher between cohorts (σ2 = 0.015, 95% CI [0.08, 0.20]), than within them (σ2 = 0.015, 95% CI [0.006, 0.039]). This suggests that a substantial degree of the unexplained variance in the model was due to un-modeled differences between cohorts. Overall dispersion in the effects was large, with 95% precision intervals ranging from small to quite large effects at all levels of the moderators.
Fig. 3.
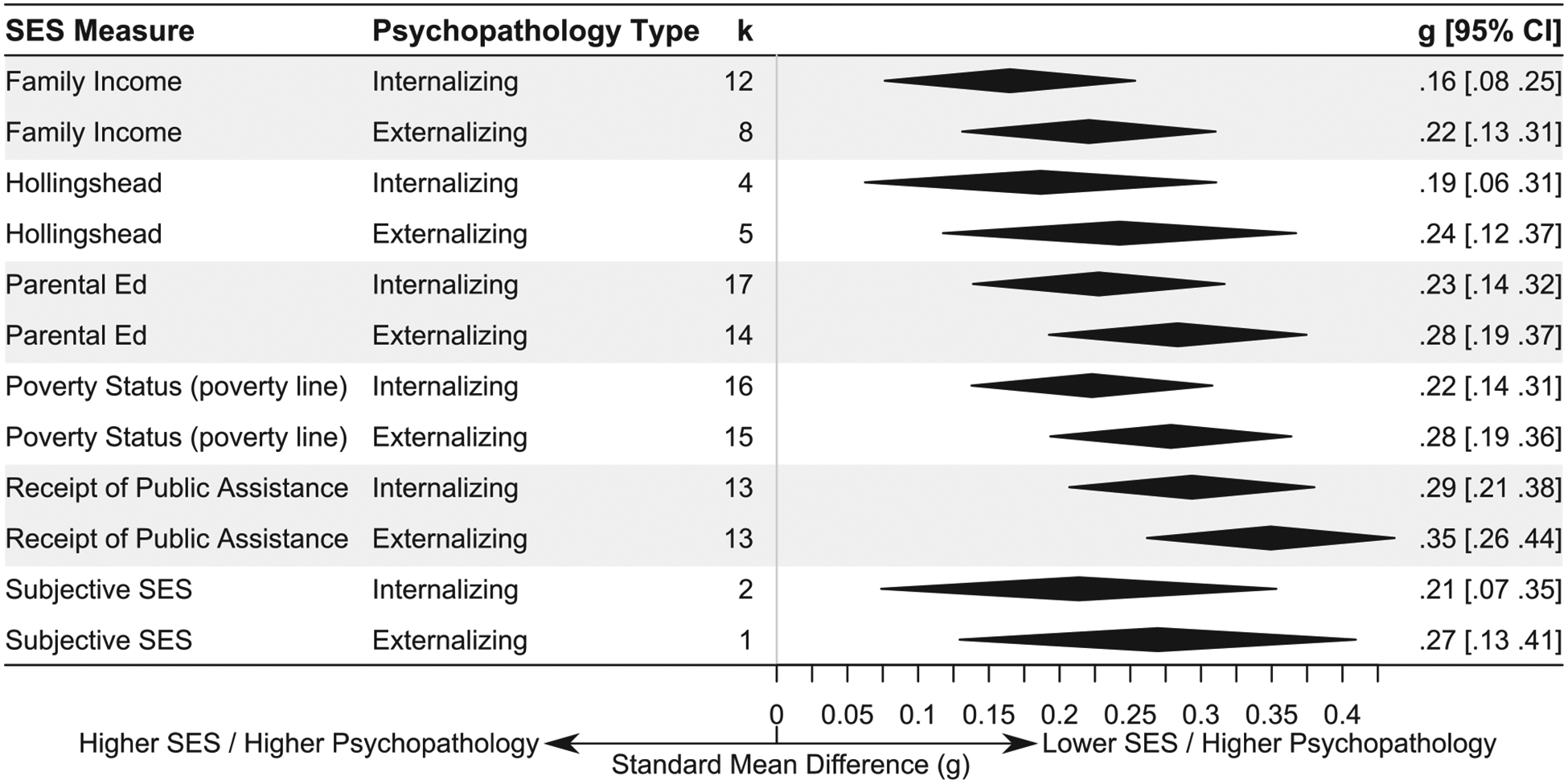
SMD in psychopathology predicted by the final model, at all levels of moderation.
To probe moderation by SES measure and for descriptive purposes, follow-up analyses were performed within each SES measure. To allow for analysis in the original (and more interpretable) effect size parameter, these models were further separated into models of continuous (symptoms) versus dichotomous (clinically significant) psychopathology. Three component models did not incorporate effects from more than one cohort and were discarded; those effects are summarized in Appendix A.
3.3. Associations of SES with psychopathology symptoms
Association of low-SES with continuous measures of psychopathology symptoms were similar across SES indices and generally small by Cohen’s (1988) criteria. On average, children whose parents had low levels of education had psychopathology 0.25 standard deviations (g) higher than their peers. Effect sizes were similar with poverty (g = 0.25) and public assistance (g = 0.26). Total family income did not show a significant correlation with psychopathology symptoms (r = −0.07, p = .057). The Hollingshead index also did not show a statistically significant association with childhood psychopathology (g = −0.09, p = .172). Each single SES-measure model of symptoms showed significant heterogeneity (all p(Q) < 0.005) with precision intervals encompassing trivial to moderate effects (see Table 1 for detailed model parameters).
3.4. Association of SES with mental disorders
Models examining association of low-SES with the presence of clinically significant mental disorders similarly showed consistent and small effect sizes (Chen, Cohen, & Chen, 2010). Children with low parent education were 68% more likely to exhibit clinically significant psychopathology, on average, than children with more highly educated parents. Children living in poverty were 69% more likely, and children in families receiving public assistance were 115% more likely to meet criteria for a mental disorder than children from higher-SES families. Family income was about 0.31 standard deviations lower for children with a mental disorder. Models examining the association of poverty and public assistance with clinically significant psychopathology showed significant heterogeneity (p(Q) < 0.001) with precision intervals encompassing trivial to large effects. Models examining parent education and family income did not show statistically significant heterogeneity (all p(Q) > 0.166; see Table 1).
4. Discussion
In 2017, 17.5% of U.S. children (about 12.8 million individuals) lived in families with income below the federal poverty line (U.S. Census Bureau, 2017), a figure that drastically under-estimates the number of children whose families struggle to afford food, shelter, healthcare, and other necessities (Beverly, 2001; Gershoff et al., 2007). Understanding the mental health of this large demographic of children is crucial to efforts to improve public health and reduce health inequalities. In our analysis, psychopathology symptoms were, on average, 0.25 standard deviations higher in children from lower-SES families than those from families with higher-SES. In models examining diagnosed mental disorders, this corresponded to a 68–115% higher risk of meeting criteria for a mental disorder for children from low-SES families. Our results revealed that some indices of SES (notably receipt of public assistance) have stronger associations with child psychopathology than others and that SES has stronger associations with childhood externalizing psychopathology than internalizing psychopathology, as has been suggested by other authors (Duncan & Brooks-Gunn, 1994; Slopen et al., 2010).
4.1. Mechanisms linking SES with child psychopathology
SES may increase risk for child psychopathology through a number of mediating pathways. These include lack of access to resources that support cognitive, social, emotional, and physical development; greater exposure to trauma and violence; cumulative exposure to stressors; and differences in family processes and functioning (Bradley & Corwyn, 2002; Conger, Conger, & Martin, 2010; Coulton, Crampton, Irwin, Spilsbury, & Korbin, 2007; Evans & Kim, 2010; Johnson et al., 2016; Lambert, King, Monahan, & Mclaughlin, 2017). While some of these pathways (e.g., variation in cognitive stimulation) may play a role in the association of SES with psychopathology across the entire SES distribution (Amso & Lynn, 2017), others are more related to financial hardship that is concentrated among families at the lowest end of the SES distribution.
Low-SES children have less access to many forms of resources that are important for healthy development (Bradley & Corwyn, 2002). For example, low-SES families are more likely to lack healthcare, live in substandard or unstable housing, and experience food insecurity (Evans, 2004; Gershoff, 2003; McLaughlin et al., 2012; Slopen et al., 2010; Zilanawala & Pilkauskas, 2012). These material hardships may influence psychopathology in numerous ways. For example, housing instability may increase psychopathology risk by disrupting children’s social support networks (Fowler, Henry, & Marcal, 2015). Food insecurity may also influence cognitive and brain development, including fronto-striatal systems underlying reward processing, in ways that can increase risk for depression and other forms of psychopathology (Dennison et al., 2019; Kar, Rao, & Chandramouli, 2008). Children suffering from psychopathology with restricted access to mental health services may be less likely to receive effective treatment and remit over time (Wadsworth and Achenbach, 2005).
In addition to lacking resources necessary to support basic needs, low SES has been associated with differences in many forms of social and cognitive stimulation that scaffold cognitive development, including language exposure, scaffolded interactions with caregivers, and the presence of learning materials in the home (Bradley, Corwyn, McAdoo, & Garcia Coll, 2001; Hart & Risley, 2003; Romeo et al., 2018; Rosen, Sheridan, Sambrook, Meltzoff, & McLaughlin, 2018). Differences in cognitive stimulation mediate the association of SES with the structure and function of fronto-parietal and fronto-temporal networks in the brain (Romeo et al., 2018; Rosen et al., 2018) that underlie complex cognitive functions, including executive functioning and language. Indeed, low levels of cognitive stimulation mediate the association of SES with executive functioning (Hackman et al., 2015; Rosen et al., 2020), a set of cognitive processes that regulate goal-directed behavior and vary consistently as a function of childhood SES (Lawson, Hook, & Farah, 2018). Low cognitive stimulation also mediates the association of SES with the structure and function of the fronto-parietal network (Rosen et al., 2018). Because difficulties with executive functioning are a transdiagnostic risk factor for the development of psychopathology (Hatoum, Rhee, Corley, Hewitt, & Friedman, 2018), variation in cognitive stimulation is also a plausible environmental mechanism explaining SES differences in child psychopathology.
Exposure to violence and other traumatic experiences may constitute an additional environmental pathway linking SES and child psychopathology. Exposure to trauma is more common in children from lower-SES families than their higher-SES peers (Costello, Erkanli, Fairbank, & Angold, 2002; Coulton et al., 2007; McLaughlin et al., 2013). Children exposed to trauma identify potential threats with less perceptual information, exhibit elevated emotional reactivity, and have more difficulty effectively regulating these emotional responses (see McLaughlin, Colich, Rodman, & Weissman, 2020; McLaughlin & Lambert, 2017 for reviews of this literature). These alterations in emotional processing are a mechanism linking childhood trauma with increased risk for multiple forms of psychopathology (Heleniak, Jenness, Stoep, McCauley, & McLaughlin, 2016; Lambert et al., 2017; McLaughlin & Lambert, 2017).
Differences in family processes may also underlie the association of SES with child psychopathology. For example, Conger et al. (2010) have proposed parental investment and parental stress as key pathways in the SES-child psychopathology association. Investment refers not only to investment of resources in material necessities such as food, healthcare, and shelter, but also the investment of time in child rearing. Raising a family without sufficient financial resources places increased demands of many kinds on parents, which may divert time and attention away from supervision and towards efforts needed to provide for the family’s basic needs (e.g., the need to take on multiple jobs, thereby increasing the amount of time spent outside the home). Experimental evidence suggests that differences in parental supervision of children may be a key mechanism linking family SES with child psychopathology. In a natural experiment of families whose income increased following the opening of a casino that provided an income supplement to families, reductions in externalizing psychopathology in children in families who received this income supplement were mediated by increases in parental supervision (Costello et al., 2003). Increased parental stress resulting from low-SES may also result in greater risk for child psychopathology through influences on harsh parenting behaviors (see Conger et al., 2010 for review). Although these types of family processes have often been examined as mediators of the association between SES and child psychopathology, parenting may also moderate this association. For example, some evidence suggests that the association of SES with child health is stronger in children who experience harsh parenting (Browne & Jenkins, 2012).
Although each of these pathways is likely to play a role in the link between SES and child psychopathology, cumulative risk models focus on how the accumulation of environmental risks and stressors among children from low-SES families contribute to elevations in chronic stress and, ultimately, psychopathology. Numerous types of chronic stressors are more commonly experienced among children living in poverty than their higher-SES peers, including crowding, noise exposure, substandard housing, neighborhood violence, parental separation, family conflict, and others (Evans, 2004; Evans & Kim, 2010). Given the well-established association between these types of stressors and psychopathology in children (Grant, Compas, Thurm, McMahon, & Gipson, 2004), stress pathways likely play a key role in the link between SES and child psychopathology. A number of biological pathways may also contribute to the association of chronic stress with child psychopathology, in addition to changes in brain structure and function associated with low levels of cognitive stimulation (e.g., Rosen et al., 2018). Chronic stress and low-SES in childhood are associated with reductions in the volume of the hippocampus, an area of the brain that subserves learning, memory, and emotion regulation (Hackman et al., 2015; Hanson et al., 2015; Hanson, Chandra, Wolfe, & Pollak, 2011). Chronic stress has also been shown to explain links between SES and brain function during emotion regulation (Kim et al., 2013), an important transdiagnostic factor in the development of psychopathology (Aldao, Gee, Reyes, & Seager, 2016).
As noted earlier, many of these pathways are not associated with SES in a linear fashion. For example, food insecurity, unsafe housing, lack of access to healthcare, and exposure to community violence are most likely to be experienced by families experiencing material hardship—the state of not having enough resources to meet basic needs—rather than SES itself. SES and material hardship are often conflated, but the relation of SES with material hardship is weaker than is often assumed: not all children from low SES families will experience hardship and families experiencing hardship are not always low-SES by traditional indices. For example, many families with income above the poverty line still face substantial hardship (Beverly, 2001; Gershoff, 2003; Short, 2005). In a study in Chicago, Mayer and Jencks (1989) found that income-to-needs ratio explained only 24% of variance in material hardship measures. Relatedly, direct measures of material hardship have frequently shown stronger and more consistent associations with child psychopathology than SES measures alone (e.g. Gershoff et al., 2007; McLaughlin, Green, Alegría, et al., 2012; Mistry, Biesanz, Chien, Howes, & Benner, 2008; Zilanawala & Pilkauskas, 2012), making them extremely promising tools for future research on psychopathology and economic adversity. That said, effects of SES on child psychopathology are likely to persist after material hardship is accounted for, as family income and child psychopathology are associated across the entire income distribution including among middle and high-SES families who can afford to meet their basic needs (Goodman, Slap, & Huang, 2003). Other pathways are likely related to SES across the entire SES distribution. For example, cognitive stimulation is positively associated with SES even in middle and high-SES families (Amso, Salhi, & Badre, 2019; Hart & Risley, 2003). Future research is needed to identify the mechanisms that play the largest role in explaining the association of SES with child psychopathology to inform interventions to reduce these disparities.
4.2. Moderators of the SES-psychopathology association
Moderation tests revealed that some measures of family SES showed stronger associations with child psychopathology than others. Notably, receipt of public assistance showed an especially strong relation with child psychopathology, with a model predicted standard mean difference of 0.32, which is 28% larger than the overall pooled effect of g =0.25. Among low-SES families, those most in need are more likely to apply for and receive assistance, and the aid they receive is unlikely to fully address their needs (DePolt, Moffitt, & Ribar, 2009; Wilde, 2007). Consequently, families who apply and qualify for public assistance face more severe and longer lasting material hardship than families who are low-SES according to other indices but are not receiving public assistance (Purtell, Gershoff, & Aber, 2012). For example, among households with combined income less than 130% of the federal poverty line in 2018, approximately 47.5% of those receiving supplemental nutritional assistance program benefits (food stamps) experienced food insecurity, compared to 23.3% of those not receiving such assistance (Coleman-Jensen, Rabbitt, Gregory, & Singh, 2019).
In our models, low-SES was associated with a greater standard mean increase in externalizing psychopathology (g = 0.28) versus internalizing psychopathology (g = 0.22). This is consistent with previous studies showing stronger relationships between SES and externalizing relative to internalizing psychopathology (Achenbach, Verhulst, Edel-brock, Baron, & Akkerhuis, 1987; Costello et al., 2003; Strohschein, 2005). A number of proposed links between SES and psychopathology are likely to have stronger influence on externalizing relative to internalizing psychopathology. Some studies have suggested that parental monitoring and behavioral control may have particularly strong links to externalizing vs. internalizing behavior (Goldner et al., 2016; Pettit, Laird, Dodge, Bates, & Criss, 2001), perhaps because higher levels of monitoring allow for a greater degree of responsiveness to problem behaviors characteristic of externalizing psychopathology. An illustration particularly relevant to this review comes from Costello et al., 2003 natural experiment, which showed supervision-mediated reductions in psychopathology in families receiving an income supplement that were specific to externalizing symptoms. That said, the relation of psychopathology to parental monitoring is complex and some studies have not found an especially strong relation to externalizing problems (See McKee, Colletti, Rakow, Jones, & Forehand, 2008 for review). Differences in executive functioning related to low levels of cognitive stimulation may be particularly likely to increase risk for externalizing psychopathology (Slopen et al., 2010; Strohschein, 2005), especially ADHD (Bloemen et al., 2018). Lastly, children growing up in low-SES neighborhoods may be subject to increased social pressures towards antisocial behavior. For example, Duncan and Brooks-Gunn (1994) found that externalizing symptoms, but not internalizing symptoms, among pre-school aged children were associated with the proportion of their neighbors living under the poverty line (after controlling for family SES). Neighborhood SES has also been frequently associated with the related construct of delinquency (See Yoshikawa, 1994 for review).
Notably, we did not find evidence for moderation by age. This is surprising, given a consensus in the literature that SES shows a stronger association with psychopathology in younger children (Bradley & Corwyn, 2002; Duncan & Brooks-Gunn, 1999; Piotrowska et al., 2015; Reiss, 2013). Because our participants were mostly in middle childhood and adolescence, the stronger association of SES with psychopathology in younger children may not have been captured. Additionally, we limited our review to cross-sectional studies, and the developmental course of these effects may be more visible in longitudinal designs. Importantly, there is good evidence to suggest that the timing and duration of low-SES influences child psychopathology (Duncan & Brooks-Gunn, 1999; Rekker et al., 2015; Strohschein, 2005). For example, McLeod and Shanahan (1993) found that a history of persistent poverty showed associations with different forms of psychopathology, and that these associations were explained by different mediating factors, relative to concurrent poverty.
4.3. Dispersion of effects
All of our included studies were from large population-representative studies of high quality that we would expect to yield accurate effect sizes. As such, much of the variability in effect size we observed likely represents meaningful differences across cohorts rather than error. This is reflected in our results by a substantial dispersion in the predicted association between family SES and psychopathology. Precision intervals across levels of moderators generally ranged from trivial to rather large effects (as high as g = 0.44). This is highly consistent with previous qualitative and quantitative reviews which have also found variability in the strength of association between SES and child psychopathology (Bradley & Corwyn, 2002; Duncan & Magnuson, 2003; Piotrowska et al., 2015; Reiss, 2013; Yoshikawa, Aber, & Beardslee, 2012). Importantly, our analysis suggests that this dispersion remains substantial even after a variety of potential moderators (age, sex, and racial composition of sample, variation in SES measure, psychopathology domain, psychopathology reporter, date of data collection, use of statistical adjustment, use of probability weighting in analysis, and study year) were accounted for. Although some variability was accounted for by un-modeled differences between effects within cohorts, our results suggest that the majority of the dispersion may have been related to differences between cohorts.
Because cohorts varied in the communities they sampled, one explanation is that commonly used SES measures may reflect different realities for families in different communities. Family SES may be more or less related to more proximal risk factors in different samples, producing variation in the overall strength of association between SES and psychopathology. For example, cost of living differences could be expected to moderate the association between income-derived measures of SES and material hardship. This is particularly true for measures that assess poverty status or income relative to the poverty line – since the federal poverty line does not incorporate regional variation in cost of living, it is likely to reflect a conservative but reasonable estimate of hardship in some communities while capturing only the most extreme hardship in others (Gershoff, 2003). Similarly, children’s access to cognitive stimulation might have a different relation to SES in communities where the cost of enrichment activities (such as high quality childcare) is high or low relative to a community’s average level of income. Non-income based indices of SES may also have different meanings in different samples. For example, the number of well-compensated jobs held by individuals without college degrees varies substantially by state – from 15% in Washington DC to 62% in Wyoming in 2015 (Georgetown University Center on Education and the Workforce, 2017). This source of heterogeneity is accentuated when researchers make assumptions about meaningful parent education thresholds. High school completion is often used, but there is evidence that completing college may be more appropriate (McLaughlin, Costello, et al., 2012). In reality, the most appropriate threshold may vary by population.
Alternative measurement strategies may better account for these types of differences between families and communities than more traditional SES measurements. Researchers interested in the effects of material hardship should be encouraged to assess hardships such as residential instability, food insecurity, difficulty paying bills, and healthcare access directly. Another promising alternative strategy for measuring SES is to employ measures of subjective social status. Among adults, ratings of subjective social status relative to a self-identified community are more closely related to health outcomes than ratings of status relative to the nation, suggesting that these measures may be able to account for contextual differences between communities (Cundiff, Smith, Uchino, & Berg, 2013; Ghaed & Gallo, 2007). Subjective social status measures may additionally account for variation in the relevance of different forms of resources to different families and across intersecting identities such as race. In one study, for example, income was less strongly related to subjective assessments of status in Black vs White or Hispanic U.S. populations (Wolff, Acevedo-Garcia, Subramanian, Weber, & Kawachi, 2010). In adolescents, a meta-analysis by Quon and McGrath (2014) found little evidence of heterogeneity in the strength of association of subjective social status and adolescent psychopathology. However, most research on associations between subjective social status and health outcomes has focused on adult health, and more research will be needed to fully explore the meaning and implications of these measures in pediatric samples.
4.4. Limitations
Although our study had a number of strengths, several limitations should be kept in mind. We focused our review on high quality studies with large subject counts and rigorous study design. This necessarily limits the total number of associations available for analysis. This limitation, together with a relatively small amount of variance represented between cohorts for our various moderator variables, also limited our power to detect moderation. In particular, our analysis of moderation by children’s race was limited to examination of the percent of each cohort identified as non-Hispanic white and Black, as these were the only categories consistently reported across cohorts. Our analysis by Black identity was also confounded by our inability to control for the racial and ethnic composition of the rest of the sample (for example, in some cohorts non-Black participants were largely non-Hispanic white, and in others there was a substantial proportion of other identities, such as Native-American participants in the Great Smoky Mountain study). Studies vary widely in the assessment of race, ethnicity, and coding of multi-racial participants. This makes it difficult to compare results between studies, as particular racial and ethnic groups are categorized differently in different studies. The field would benefit from a standard approach to assessing and reporting on race and ethnicity. In addition, future research on this question would benefit from a stronger intersectional framework investigating differences in the association of SES with child psychopathology not only by race and sex, but also their interaction with one another and other types of identities including ethnicity, sexual orientation, gender identity, disability, immigration status, and others.
Our meta-analysis focused solely on correlational studies. This means that we are unable to make causal inferences or isolate specific mechanisms based on these results. Of special note, associations of receipt of public assistance with child psychopathology should not be interpreted as a damaging effect of public assistance on child psychopathology but rather as an effect of severe material hardship. Our focus on unadjusted effects also limited our ability to comment on mechanisms, as the observed associations could plausibly result from other risk factors which are themselves correlated to low SES, such as exposure to violence (McLaughlin et al., 2012). Experimental studies provide unique insights in to mechanisms, and the largest ever study evaluating the effect of an income supplement on child development is currently underway (Duncan, 2018). This study will shed light on the mediating pathways that play the most meaningful role in linking SES with child psychopathology.
Prior evidence suggests that the timing and duration of low SES moderates its associations with child psychopathology (Duncan & Brooks-Gunn, 1999; Rekker et al., 2015; Strohschein, 2005), and we were unable to explore these patterns given the cross-sectional nature of our data. We were also restricted by the way that SES is commonly measured in the population-representative studies. For example, we presented effects associated with poverty status and not having a parent who completed high school. These thresholds are commonly used, but other thresholds (e.g. income required to meet basic expenses, college completion) may be more predictive (Allegretto, 2006; McLaughlin, Costello, et al., 2012) and should be explored in future research. Our outcome variables were likewise limited to forms of psychopathology commonly assessed in population-based studies, and we did not consider less common diagnoses which may be of interest (e.g. OCD, thought disorder) or more recent conceptualizations of psychopathology which would not appear in older publications such as a general psychopathology factor (Caspi et al., 2014). We also did not include forms of psychopathology that typically emerge in late adolescence, such as substance use and eating disorders, given that our power to detect these effects would have been low based on the age range of our samples. Our moderator analyses were limited to broad demographic variables typically reported in population-based studies. Other potential moderators, such as parenting and other family process factors (Browne & Jenkins, 2012), were not considered. We considered variation across time using study year as a moderator when, in reality, the association of SES with childhood psychopathology may vary in response to specific economic and policy changes.
Lastly, our primary analysis presents all effects in the metric of SMD (g). This approach is not unusual in meta-analysis and allows for comparison of the largest number of effects. However, it does make assumptions about the nature of the underlying data and additionally makes some comparisons less interpretable. To address this limitation, we additionally present a set of bivariate models in the original effect size metrics appropriate to the constituent variables (e.g., OR for associations between two dichotomous variables).
4.5. Conclusion
We present a meta-analysis of population-based studies investigating the association of different metrics of family SES with child psychopathology. We found a small pooled association of SES with psychopathology across studies, such that children from low-SES families showed more symptoms of psychopathology and were more likely to meet criteria for a mental disorder than children from higher-SES families. This association was particularly strong for receipt of public assistance, a measure especially likely to be related to material hardship. Further, the association of SES was stronger with externalizing versus internalizing psychopathology. The strength of association between SES and child psychopathology showed strong dispersion, especially between different cohorts. This dispersion may help explain wide variation in the reported strength of association between family SES and child psychopathology in previous studies and suggests that the association of family SES with child psychopathology may vary substantially in magnitude across different populations within the United States. These results underscore the importance of identifying specific mechanisms linking SES with child psychopathology, as well as protective factors. By exploring how and why SES is associated with child psychopathology, mechanistic research promises to identify targets for new interventions tailored to reduce socioeconomic disparities in mental health and improve the lives of a large and vulnerable group of children. More broadly, our findings speak to the importance of incorporating a greater focus on child mental health in interventions and policy strategies aimed at providing economic assistance and support for low-SES families, as changes in policy to ensure that all families have access to a basic living wage and the resources they need to support their children will ultimately be the most effective strategy for reducing the burden of child psychopathology associated with low-SES.
Supplementary Material
Acknowledgments
The authors would like to thank Jane Costello, Stephanie Kasen, Gordon Keeler, and Benjamin Lahey for their assistance with data preparation. This manuscript reflects the views of the authors and may not reflect the opinions or views of all the study investigators or the NIMH.
Author biography
Matthew Peverill, is a Ph.D. candidate in Clinical Child Psychology at the University of Washington.
Melanie A. Dirks is an Associate Professor of Psychology at McGill College.
Tomás Narvaja is a student at the University of Washington, School of Medicine.
Kate L. Herts is an Assistant Professor of Psychology in Clinical Psychiatry at Weill Cornell Medicine.
Jonathan S. Comer is a Professor of Psychology and Psychiatry at Florida International University.
Katie A. McLaughlin is an Associate Professor of Psychology at Harvard University.
Footnotes
Declaration of Competing Interest
None.
Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.cpr.2020.101933.
References
- Achenbach TM, McConaughy SH, & Howell CT (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101(2), 213–232. 10.1037/0033-2909.101.2.213. [DOI] [PubMed] [Google Scholar]
- Zilanawala A, & Pilkauskas NV (2012). Material hardship and child socioemotional behaviors: differences by types of hardship, timing, and duration. Children and Youth Services Review, 34(4), 814–825. 10.1016/j.childyouth.2012.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Achenbach TM, Verhulst FC, Edelbrock C, Baron DG, & Akkerhuis G,W (1987). Epidemiological comparisons of American and Dutch children: II. Behavioral/emotional problems reported by teachers for ages 6 to 11. Journal of the American Academy of Child, 26(3), 326–332. [DOI] [PubMed] [Google Scholar]
- Aldao A, Gee DG, Reyes ADL, & Seager I (2016). Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Development and Psychopathology, 28, 927–946. 10.1017/S0954579416000638, 4pt1. [DOI] [PubMed] [Google Scholar]
- Alegria M, Vallas M, & Pumariega A (2010). Racial and ethnic disparities in Pediatric mental health. Child and Adolescent Psychiatric Clinics of North America, 19(4), 759–774. 10.1016/j.chc.2010.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allegretto SA (2006). Basic family budgets: Working Families’ incomes often fail to meet living expenses around the United States. International Journal of Health Services, 36(3), 443–454. 10.2190/A0GA-6R7Y-XFM3-EBJY. [DOI] [PubMed] [Google Scholar]
- Amso D, & Lynn A (2017). Distinctive mechanisms of adversity and socioeconomic inequality in child development: A review and recommendations for evidence-based policy. Policy Insights From the Behavioral and Brain Sciences, 4(2), 139–146. 10.1177/2372732217721933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amso D, Salhi C, & Badre D (2019). The relationship between cognitive enrichment and cognitive control: a systematic investigation of environmental influences on development through socioeconomic status. Developmental Psychobiology, 61(2), 159–178. 10.1002/dev.21794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andersson MA (2018). An odd ladder to climb: Socioeconomic differences across levels of subjective social status. Social Indicators Research, 136(2), 621–643. 10.1007/s11205-017-1559-7. [DOI] [Google Scholar]
- Assink M, & Wibbelink CJM (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology, 12(3), 154–174. 10.20982/tqmp.12.3.p154. [DOI] [Google Scholar]
- Beverly SG (2001). Material hardship in the United States: Evidence from the survey of income and program participation. Social Work Research, 25(3), 143–151. 10.1093/swr/25.3.143. [DOI] [Google Scholar]
- Bloemen AJP, Oldehinkel AJ, Laceulle OM, Ormel J, Rommelse NNJ, & Hartman CA (2018). The association between executive functioning and psychopathology: General or specific? Psychological Medicine, 48(11), 1787–1794. 10.1017/S0033291717003269. [DOI] [PubMed] [Google Scholar]
- Bor J, Cohen GH, & Galea S (2017). Population health in an era of rising income inequality: USA, 1980–2015. The Lancet, 389(10077), 1475–1490. 10.1016/S0140-6736(17)30571-8. [DOI] [PubMed] [Google Scholar]
- Bor W, Najman JM, Andersen MJ, O’callaghan M, Williams GM, & Behrens BC (1997). The relationship between low family income and psychological disturbance in young children: An Australian longitudinal study. The Australian and New Zealand Journal of Psychiatry, 31(5), 664–675. 10.3109/00048679709062679. [DOI] [PubMed] [Google Scholar]
- Bowleg L (2012). The problem with the phrase women and minorities: Intersectionality—An important theoretical framework for public health. American Journal of Public Health, 102(7), 1267–1273. 10.2105/AJPH.2012.300750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradley RH, & Corwyn RF (2002). Socioeconomic status and child development. Annual Review of Psychology, 53(1), 371. [DOI] [PubMed] [Google Scholar]
- Bradley RH, Corwyn RF, McAdoo HP, & Garcia Coll C (2001). The home environments of children in the United States part I: Variations by age, ethnicity, and poverty status. Child Development, 72(6), 1844–1867. 10.1111/1467-8624.t01-1-00382. [DOI] [PubMed] [Google Scholar]
- Browne DT, & Jenkins JM (2012). Health across early childhood and socioeconomic status: examining the moderating effects of differential parenting. Social Science & Medicine, 74(10), 1622–1629. 10.1016/j.socscimed.2012.01.017. [DOI] [PubMed] [Google Scholar]
- Call KT, & Nonnemaker J (1999). Socioeconomic disparities in adolescent health: contributing factors. Annals of the New York Academy of Sciences, 896(1), 352–355. 10.1111/j.1749-6632.1999.tb08139.x. [DOI] [PubMed] [Google Scholar]
- Callahan CL, & Eyberg SM (2010). Relations between parenting behavior and SES in a clinical sample: Validity of SES measures. Child and Family Behavior Therapy, 32(2), 125–138. 10.1080/07317101003776456. [DOI] [Google Scholar]
- Cantwell DP, Lewinsohn PM, Rohde P, & Seeley JR (1997). Correspondence between adolescent report and parent report of psychiatric diagnostic data. Journal of the American Academy of Child & Adolescent Psychiatry, 36(5), 610–619. 10.1097/00004583-199705000-00011. [DOI] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Belsky DW, Goldman-Mellor SJ, Harrington H, Israel S, … Moffitt TE (2014). The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2(2), 119–137. 10.1177/2167702613497473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Census Bureau. (2017). Income and Poverty in the United States: 2017 https://www.census.gov/library/publications/2018/demo/p60-263.html.
- Chen H, Cohen P, & Chen S (2010). How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Communications in Statistics: Simulation and Computation, 39(4), 860–864. 10.1080/03610911003650383. [DOI] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences. L. Erlbaum Associates. [Google Scholar]
- Coleman JS (1988). Social capital in the creation of human capital. American Journal of Sociology, 94, S95–S120. [Google Scholar]
- Coleman-Jensen A, Rabbitt MP, Gregory CA, & Singh A (2019). Household Food Security in the United States in 2018 (ERR-270). U.S. Department of Agriculture, Economic Research Service. [Google Scholar]
- Conger RD, Conger KJ, & Martin MJ (2010). Socioeconomic status, family processes, and individual development. Journal of Marriage and the Family, 72(3), 685–704. 10.1111/j.1741-3737.2010.00725.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger RD, & Donnellan MB (2007). An interactionist perspective on the socioeconomic context of human development. Annual Review of Psychology, 58(1), 175–199. 10.1146/annurev.psych.58.110405.085551. [DOI] [PubMed] [Google Scholar]
- Costello EJ, Compton SN, Keeler G, & Angold A (2003). Relationships between poverty and psychopathology: a natural experiment. JAMA, 290(15), 2023 10.1001/jama.290.15.2023. [DOI] [PubMed] [Google Scholar]
- Costello EJ, Erkanli A, Fairbank JA, & Angold A (2002). The prevalence of potentially traumatic events in childhood and adolescence. Journal of Traumatic Stress, 15(2), 99–112. 10.1023/A:1014851823163. [DOI] [PubMed] [Google Scholar]
- Costello EJ, Keeler GP, & Angold A (2001). Poverty, race/ethnicity, and psychiatric disorder: A study of rural children. American Journal of Public Health, 91(9), 1494–1498. 10.2105/AJPH.91.9.1494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coulton CJ, Crampton DS, Irwin M, Spilsbury JC, & Korbin JE (2007). How neighborhoods influence child maltreatment: a review of the literature and alternative pathways. Child Abuse & Neglect, 31(11–12), 1117–1142. 10.1016/j.chiabu.2007.03.023. [DOI] [PubMed] [Google Scholar]
- Cundiff J, Smith T, Uchino B, & Berg C (2013). Subjective social status: Construct validity and associations with psychosocial vulnerability and self-rated health. International Journal of Behavioral Medicine, 20(1), 148–158. 10.1007/s12529-011-9206-1. [DOI] [PubMed] [Google Scholar]
- Davis E, Sawyer M, Lo S, Priest N, & Wake M (2010). Socioeconomic risk factors for mental health problems in 4–5-year-old children: Australian population study. Academic Pediatrics, 10(1), 41–47. 10.1016/j.acap.2009.08.007. [DOI] [PubMed] [Google Scholar]
- Dennison MJ, Rosen ML, Sambrook KA, Jenness JL, Sheridan MA, & McLaughlin KA (2019). Differential associations of distinct forms of childhood adversity with neurobehavioral measures of reward processing: A developmental pathway to depression. Child Development, 90(1), e96–e113. 10.1111/cdev.13011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DePolt RA, Moffitt RA, & Ribar DC (2009). Food stamps, temporary assistance for needy families and food hardships in three american cities. Pacific Economic Review, 14(4), 445–473. 10.1111/j.1468-0106.2009.00462.x. [DOI] [Google Scholar]
- Diemer MA, Mistry RS, Wadsworth ME, López I, & Reimers F (2013). Best practices in conceptualizing and measuring social class in psychological research. Analyses of Social Issues and Public Policy, 13(1), 77–113. 10.1111/asap.12001. [DOI] [Google Scholar]
- Dohrenwend BP, Levav I, Shrout PE, Schwartz S, Naveh G, Link BG, … Stueve A (1992). Socioeconomic status and psychiatric disorders: The causation-selection issue. Science, 255(5047), 946–952. [DOI] [PubMed] [Google Scholar]
- Duncan GJ (2018). Baby’s First Years (BFY) (no. https://clinicaltrials.gov/ct2/show/study/NCT03593356). https://clinicaltrials.gov/ct2/show/study/NCT03593356.
- Duncan GJ, & Brooks-Gunn J (1994). Economic deprivation and early childhood development. Child Development, 65(2), 296–318. 10.1111/1467-8624.ep9405315105. [DOI] [PubMed] [Google Scholar]
- Duncan GJ, & Brooks-Gunn J (1999). Income effects across the life span: Integration and interpretation. Russell Sage Foundation. [Google Scholar]
- Duncan GJ, & Magnuson KA (2003). Off with Hollingshead: Socioeconomic resources, parenting, and child development In Bornstein MH, & Bradley RH (Eds.), Socioeconomic status, parenting, and child development. Mahwah, N.J.: Routledge. [Google Scholar]
- Ellard-Gray A, Jeffrey NK, Choubak M, & Crann SE (2015). Finding the hidden participant: Solutions for recruiting hidden, hard-to-reach, and vulnerable populations. International Journal of Qualitative Methods, 14(5). 10.1177/1609406915621420, 1609406915621420. [DOI] [Google Scholar]
- Evans GW (2004). The environment of childhood poverty. American Psychologist, 59 (2), 77–92. 10.1037/0003-066X.59.2.77. [DOI] [PubMed] [Google Scholar]
- Evans GW, & Kim P (2010). Multiple risk exposure as a potential explanatory mechanism for the socioeconomic status-health gradient: Multiple risk exposure and SES-health gradient. Annals of the New York Academy of Sciences, 1186(1), 174–189. 10.1111/j.1749-6632.2009.05336.x. [DOI] [PubMed] [Google Scholar]
- Fowler PJ, Henry DB, & Marcal KE (2015). Family and housing instability: longitudinal impact on adolescent emotional and behavioral well-being. Social Science Research, 53, 364–374. 10.1016/j.ssresearch.2015.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gennetian LA, & Miller C (2002). Children and welfare reform: a view from an experimental welfare program in Minnesota. Child Development, 73(2), 601. [DOI] [PubMed] [Google Scholar]
- Georgetown University Center on Education and the Workforce. (2017). Good jobs that pay without a Ba: A state-by-state analysis. 132. [Google Scholar]
- Gershoff ET (2003). Low income and the development of America’s kindergartners. New York, NY: National Center for Children in Poverty, Columbia University Mailman School of Public Health; (Living at the Edge Research Brief No. 4) https://academiccommons.columbia.edu/doi/10.7916/D8H139RR/download. [Google Scholar]
- Gershoff ET, Aber JL, Raver CC, & Lennon MC (2007). Income is not enough: Incorporating material hardship into models of income associations with parenting and child development. Child Development, 78(1), 70–95. 10.1111/j.1467-8624.2007.00986.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghaed SG, & Gallo LC (2007). Subjective social status, objective socioeconomic status, and cardiovascular risk in women. Health Psychology, 26(6), 668–674. 10.1037/0278-6133.26.6.668. [DOI] [PubMed] [Google Scholar]
- Goldner JS, Quimby D, Richards MH, Zakaryan A, Miller S, Dickson D, & Chilson J (2016). Relations of parenting to adolescent externalizing and internalizing distress moderated by perception of neighborhood danger. Journal of Clinical Child & Adolescent Psychology, 45(2), 141–154. 10.1080/15374416.2014.958838. [DOI] [PubMed] [Google Scholar]
- Goodman E (1999). The role of socioeconomic status gradients in explaining differences in US adolescents’ health. American Journal of Public Health, 89(10), 1522–1528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman E, Slap GB, & Huang B (2003). The public health impact of socioeconomic status on adolescent depression and obesity. American Journal of Public Health, 93 (11), 1844–1850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granero Pérez R, Ezpeleta L, & Domenech JM (2007). Features associated with the non-participation and drop out by socially-at-risk children and adolescents in mental-health epidemiological studies. Social Psychiatry and Psychiatric Epidemiology, 42(3), 251–258. 10.1007/s00127-006-0155-y. [DOI] [PubMed] [Google Scholar]
- Grant KE, Compas BE, Thurm AE, McMahon SD, & Gipson PY (2004). Stressors and child and adolescent psychopathology: Measurement issues and prospective effects. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 33(2), 412–425. doi: 10.1207/s15374424jccp3302_23. [DOI] [PubMed] [Google Scholar]
- Hackman DA, Gallop R, Evans GW, & Farah MJ (2015). Socioeconomic status and executive function: developmental trajectories and mediation. Developmental Science, 18(5), 686–702. 10.1111/desc.12246. [DOI] [PubMed] [Google Scholar]
- Hanson JL, Chandra A, Wolfe BL, & Pollak SD (2011). Association between income and the hippocampus. PLoS One, 6(5). 10.1371/journal.pone.0018712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanson JL, Nacewicz BM, Sutterer MJ, Cayo AA, Schaefer SM, Rudolph KD, … Davidson RJ (2015). Behavioral problems after early life stress: contributions of the hippocampus and amygdala. Biological Psychiatry, 77(4), 314–323. 10.1016/j.biopsych.2014.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris YR, Terrel D, & Allen G (1999). The influence of education context and beliefs on the teaching behavior of African American mothers. Journal of Black Psychology, 25(4), 490–503. 10.1177/0095798499025004002. [DOI] [Google Scholar]
- Hart B, & Risley TR (2003). The early catastrophe. The 30 million word gap. American Educator, 27(1), 4–9. [Google Scholar]
- Hatoum AS, Rhee SH, Corley RP, Hewitt JK, & Friedman NP (2018). Do executive functions explain the covariance between internalizing and externalizing behaviors? Development and Psychopathology, 30(4), 1371–1387. 10.1017/S0954579417001602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML, Phelan JC, & Link BG (2013). Stigma as a fundamental cause of population health inequalities. American Journal of Public Health, 103(5), 813–821. 10.2105/AJPH.2012.301069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heleniak C, Jenness JL, Stoep AV, McCauley E, & McLaughlin KA (2016). Childhood maltreatment exposure and disruptions in emotion regulation: a transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cognitive Therapy and Research, 40(3), 394–415. 10.1007/s10608-015-9735-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hernán MA, Hernández-Díaz S, & Robins JM (2004). A structural approach to selection bias. Epidemiology, 15(5), 615–625. 10.1097/01.ede.0000135174.63482.43. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB (1975). Four factor index of social status [unpublished manuscript].
- Johnson SB, Riis JL, & Noble KG (2016). State of the art review: poverty and the developing brain. Pediatrics, 137(4). 10.1542/peds.2015-3075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kar BR, Rao SL, & Chandramouli BA (2008). Cognitive development in children with chronic protein energy malnutrition. Behavioral and Brain Functions, 4(1), 31 10.1186/1744-9081-4-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim P, Evans GW, Angstadt M, Ho SS, Sripada CS, Swain JE, … Phan KL (2013). Effects of childhood poverty and chronic stress on emotion regulatory brain function in adulthood. Proceedings of the National Academy of Sciences, 110(46), 18442–18447. 10.1073/pnas.1308240110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krieger N, Williams DR, & Moss NE (1997). Measuring social class in US public health research: Concepts, methodologies, and guidelines. Annual Review of Public Health, 18(1), 341–378. 10.1146/annurev.publhealth.18.1.341. [DOI] [PubMed] [Google Scholar]
- Lambert HK, King k. M., Monahan k. C., & Mclaughlin KA (2017). Differential associations of threat and deprivation with emotion regulation and cognitive control in adolescence. Development and Psychopathology, 29(3), 929–940. 10.1017/S0954579416000584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lansford JE, Malone PS, Stevens KI, Dodge KA, Bates JE, & Pettit GS (2006). Developmental trajectories of externalizing and internalizing behaviors: Factors underlying resilience in physically abused children. Development and Psychopathology, 18(1), 35–55. 10.1017/S0954579406060032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawson GM, Hook CJ, & Farah MJ (2018). A meta-analysis of the relationship between socioeconomic status and executive function performance among children. Developmental Science, 21(2). 10.1111/desc.12529, 1-N.PAG. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loeber R (1998). Antisocial behavior and mental health problems: Explanatory factors in childhood and adolescence. Lawrence Erlbaum Associates. [Google Scholar]
- Lund C, Breen A, Flisher AJ, Kakuma R, Corrigall J, Joska JA, … Patel V (2010). Poverty and common mental disorders in low and middle income countries: a systematic review. Social Science & Medicine, 71(3), 517–528. 10.1016/j.socscimed.2010.04.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marmot MG, Ryff CD, Bumpass LL, Shipley M, & Marks NF (1997). Social inequalities in health: Next questions and converging evidence. Social Science & Medicine, 44(6), 901–910. 10.1016/S0277-9536(96)00194-3. [DOI] [PubMed] [Google Scholar]
- Mayer SE, & Jencks C (1989). Poverty and the distribution of material hardship. The Journal of Human Resources, 24(1), 88 10.2307/145934. [DOI] [Google Scholar]
- McKee L, Colletti C, Rakow A, Jones DJ, & Forehand R (2008). Parenting and child externalizing behaviors: Are the associations specific or diffuse? Aggression and Violent Behavior, 13(3), 201–215. 10.1016/j.avb.2008.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Colich NL, Rodman AM, & Weissman DG (2020). Mechanisms linking childhood trauma exposure and psychopathology: A transdiagnostic model of risk and resilience. BMC Medicine, 18(1), 96 10.1186/s12916-020-01561-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Costello EJ, Leblanc W, Sampson NA, & Kessler RC (2012). Socioeconomic status and adolescent mental disorders. American Journal of Public Health, 102(9), 1742–1750. 10.2105/AJPH.2011.300477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Green JG, Alegría M, Costello EJ, Gruber MJ, Sampson NA, & Kessler RC (2012). Food insecurity and mental disorders in a national sample of U.S. adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 51(12), 1293–1303. 10.1016/j.jaac.2012.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2012). Childhood adversities and first onset of psychiatric disorders in a national sample of adolescents. Archives of General Psychiatry, 69(11), 1151–1160. 10.1001/archgenpsychiatry.2011.2277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Koenen KC, Hill ED, Petukhova M, Sampson NA, Zaslavsky AM, & Kessler RC (2013). Trauma exposure and posttraumatic stress disorder in a national sample of adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 52(8), 815–830. e14 10.1016/j.jaac.2013.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, & Lambert HK (2017). Child trauma exposure and psychopathology: Mechanisms of risk and resilience. Current Opinion in Psychology, 14(Suppl. C), 29–34. 10.1016/j.copsyc.2016.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLeod JD, & Edwards K (1995). Contextual determinants of children’s responses to poverty. Social Forces, 73(4), 1487. [Google Scholar]
- McLeod JD, & Shanahan MJ (1993). Poverty, parenting, and children’s mental health. American Sociological Review, 58(3), 351–366. 10.2307/2095905. [DOI] [Google Scholar]
- Mendelson T, Kubzansky LD, Datta GD, & Buka SL (2008). Relation of female gender and low socioeconomic status to internalizing symptoms among adolescents: a case of double jeopardy? Social Science & Medicine, 66(6), 1284–1296. 10.1016/j.socscimed.2007.11.033. [DOI] [PubMed] [Google Scholar]
- Merikangas KR, He J, Burstein M, Swanson SA, Avenevoli S, Cui L, … Swendsen J (2010). Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Study-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. 10.1016/j.jaac.2010.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mistry RS, Biesanz JC, Chien N, Howes C, & Benner AD (2008). Socioeconomic status, parental investments, and the cognitive and behavioral outcomes of low-income children from immigrant and native households. Early Childhood Research Quarterly, 23(2), 193–212. 10.1016/j.ecresq.2008.01.002. [DOI] [Google Scholar]
- Patel V, & Kleinman A (2003). Poverty and common mental disorders in developing countries. Bulletin of the World Health Organization, 81, 609–615. 10.1590/S0042-96862003000800011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pettit GS, Laird RD, Dodge KA, Bates JE, & Criss MM (2001). Antecedents and behavior-problem outcomes of parental monitoring and psychological control in early adolescence. Child Development, 72(2), 583–598. 10.1111/1467-8624.00298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piotrowska PJ, Stride CB, Croft SE, & Rowe R (2015). Socioeconomic status and antisocial behaviour among children and adolescents: A systematic review and meta-analysis. Clinical Psychology Review, 35, 47–55. 10.1016/j.cpr.2014.11.003. [DOI] [PubMed] [Google Scholar]
- Purtell KM, Gershoff ET, & Aber JL (2012). Low income families’ utilization of the federal “safety net”: Individual and state-level predictors of TANF and food stamp receipt. Children and Youth Services Review, 34(4), 713–724. 10.1016/j.childyouth.2011.12.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quon EC, & McGrath JJ (2014). Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychology : Official Journal of the Division of Health Psychology, American Psychological Association, 33(5), 433–447. 10.1037/a0033716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reiss F (2013). Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Social Science & Medicine, 90, 24–31. 10.1016/j.socscimed.2013.04.026. [DOI] [PubMed] [Google Scholar]
- Rekker R, Pardini D, Keijsers L, Branje S, Loeber R, & Meeus W (2015). Moving in and out of poverty: The within-individual association between socioeconomic status and juvenile delinquency. PLoS One, 10(11), Article e0136461 10.1371/journal.pone.0136461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romeo RR, Leonard JA, Robinson ST, West MR, Mackey AP, Rowe ML, & Gabrieli JDE (2018). Beyond the 30-million-word gap: children’s conversational exposure is associated with language-related brain function. Psychological Science, 29 (5), 700–710. 10.1177/0956797617742725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen ML, Hagen MP, Lurie LA, Miles ZE, Sheridan MA, Meltzoff AN, & McLaughlin KA (2020). Cognitive stimulation as a mechanism linking socioeconomic status with executive function: a longitudinal investigation. Child Development, 91(4), e762–e779. 10.1111/cdev.13315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen ML, Sheridan MA, Sambrook KA, Meltzoff AN, & McLaughlin KA (2018). Socioeconomic disparities in academic achievement: A multi-modal investigation of neural mechanisms in children and adolescents. NeuroImage, 173, 298–310. 10.1016/j.neuroimage.2018.02.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shavers VL (2007). Measurement of socioeconomic status in health disparities research. Journal of the National Medical Association, 99(9), 1013–1023. [PMC free article] [PubMed] [Google Scholar]
- Short KS (2005). Material and financial hardship and income-based poverty measures in the USA. Journal of Social Policy, 34(1), 21–38. [Google Scholar]
- Singh-Manoux A, Adler NE, & Marmot MG (2003). Subjective social status: Its determinants and its association with measures of ill-health in the Whitehall II study. Social Science &Medicine, 56(6), 1321–1333. 10.1016/S0277-9536(02)00131-4. [DOI] [PubMed] [Google Scholar]
- Slopen N, Fitzmaurice G, Williams DR, & Gilman SE (2010). Poverty, food insecurity, and the behavior for childhood internalizing and externalizing disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 49(5), 444–452. [DOI] [PubMed] [Google Scholar]
- Strohschein L (2005). Household income histories and child mental health trajectories. Journal of Health and Social Behavior, 46(4), 359–375. 10.1177/002214650504600404. [DOI] [PubMed] [Google Scholar]
- Twenge JM, & Nolen-Hoeksema S (2002). Age, gender, race, socioeconomic status, and birth cohort difference on the children’s depression inventory: a meta-analysis. Journal of Abnormal Psychology, 111(4), 578–588. 10.1037/0021-843X.111.4.578. [DOI] [PubMed] [Google Scholar]
- Velez CN, Johnson J, & Cohen P (1989). A longitudinal analysis of selected risk factors for childhood psychopathology. Journal of the American Academy of Child & Adolescent Psychiatry, 28(6), 861–864. 10.1097/00004583-198911000-00009. [DOI] [PubMed] [Google Scholar]
- Viechtbauer W (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. [Google Scholar]
- Voils CI, Crandell JL, Chang Y, Leeman J, & Sandelowski M (2011). Combining adjusted and unadjusted findings in mixed research synthesis. Journal of Evaluation in Clinical Practice, 17(3), 429–434. 10.1111/j.1365-2753.2010.01444.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vollebergh WAM, van Dorsselaer S, Monshouwer K, Verdurmen J, van der Ende J, & ter Bogt T (2006). Mental health problems in early adolescents in the Netherlands. Social Psychiatry and Psychiatric Epidemiology, 41(2), 156–163. [DOI] [PubMed] [Google Scholar]
- Wight RG, Botticello AL, & Aneshensel CS (2006). Socioeconomic context, social support, and adolescent mental health: a multilevel investigation. Journal of Youth and Adolescence, 35(1), 115–126. Scopus. doi: 10.1007/s10964-005-9009-2. [DOI] [Google Scholar]
- Wadsworth ME, & Achenbach TM (2005). Explaining the Link between low socioeconomic status and psychopathology: testing two mechanisms of the social causation hypothesis. Journal of Consulting and Clinical Psychology, 73(6), 1146–1153. 10.1037/0022-006X.73.6.1146. [DOI] [PubMed] [Google Scholar]
- Wilde PE (2007). Measuring the effect of food stamps on food insecurity and hunger: research and policy considerations. The Journal of Nutrition, 137(2), 307–310. 10.1093/jn/137.2.307. [DOI] [PubMed] [Google Scholar]
- Willms JD, & Somer MA (2001). Family, classroom, and school effects on childrens educational outcomes in Latin America. School Effectiveness and School Improvement, 12(4), 409–445. 10.1076/sesi.12.4.409.3445. [DOI] [Google Scholar]
- Wolff LS, Acevedo-Garcia D, Subramanian SV, Weber D, & Kawachi I (2010). Subjective social status, a new measure in health disparities research: Do race/ ethnicity and choice of referent group matter? Journal of Health Psychology, 15(4), 560–574. 10.1177/1359105309354345. [DOI] [PubMed] [Google Scholar]
- Yoshikawa H (1994). Prevention as cumulative protection: effects of early family support and education on chronic delinquency and its risks. Psychological Bulletin, 115(1), 28–54. 10.1037/0033-2909.115.1.28. [DOI] [PubMed] [Google Scholar]
- Yoshikawa H, Aber JL, & Beardslee WR (2012). The effects of poverty on the mental, emotional, and behavioral health of children and youth: implications for prevention. American Psychologist, 67(4), 272–284. 10.1037/a0028015. [DOI] [PubMed] [Google Scholar]
- Zahn-Waxler C, Shirtcliff EA, & Marceau K (2008). Disorders of childhood and adolescence: gender and psychopathology. Annual Review of Clinical Psychology, 4(1), 275–303. 10.1146/annurev.clinpsy.3.022806.091358. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.