

Abstract
The trauma memory is a crucial feature of PTSD etiology and maintenance. Nonetheless, the nature of memories associated with childbirth-related posttraumatic stress disorder (CB-PTSD) requires explication. The present study, as part of a larger project on psychological outcomes of childbirth, utilized a multi-method approach to characterize childbirth memories in relation to CB-PTSD symptoms. We here assessed 413 women who completed self-report measures pertaining to CB-PTSD, postpartum depression, and childbirth memories. Additionally, a subset of 209 women provided written childbirth narratives, analyzed using Linguistic Inquiry and Word Count software. Women endorsing CB-PTSD symptoms on the PTSD-Checklist (PCL)-5 reported more incoherent childbirth memories with more emotional and sensory details, and more frequent involuntary recall and reliving of the memory. They also indicated the childbirth experience was more central to their identity. Written narratives in those with probable CB-PTSD were characterized by less (positive) affective processes, and more cognitive processes. We infer that childbirth memories in women who endorse symptoms of CB-PTSD in the early postpartum period resemble those described in the general PTSD literature. This suggests that childbirth may be experienced as traumatic and evoke a traumatic memory, implicated in symptom endorsement. Opportunities for therapeutic interventions modifying traumatic memories of childbirth in women at risk for CB-PTSD need to be investigated. Future research examining characteristics of traumatic childbirth memories is needed to advance our understanding of this overlooked postpartum condition.
Keywords: stress disorders, post-traumatic, childbirth, memory, narratives
Childbirth can involve actual or perceived threat of death and/or serious injury (Say et al., 2014). Consequently, some women experience symptoms of childbirth-related posttraumatic stress disorder (CB-PTSD) (Czarnocka and Slade, 2000; Dekel et al., 2019b; Thiel et al., 2018), which can result in a debilitating condition with adverse consequences for mother, offspring, and the entire family. In community samples, up to 6% of postpartum women are expected to meet DSM diagnostic criteria for PTSD even after delivering a healthy baby at term (Dekel et al., 2017). Prevalence in high-risk groups may reach 20% (Yildiz et al., 2017). Although memory of the trauma is a crucial feature of PTSD etiology and maintenance (Dekel et al., 2016b; Dekel and Bonanno, 2013; Ehlers and Clark, 2000; Pitman, 1989; Pitman and Orr, 2012), there is a gap in knowledge pertaining to the memory of childbirth and its association with CB-PTSD. A better understanding of childbirth memory and subsequent PTSD may improve diagnosis and prognosis.
It has been suggested that how individuals remember the traumatic experience is a function of their wellbeing. The trauma memory has been specifically linked with the endorsement of PTSD. It has been proposed that traumatic memories are re-experienced as disconnected from other autobiographical information and as such the autobiographical memory of the trauma in PTSD will show specific types of disruptions. These disruptions are thought to be central to the development and the enduring nature of the symptoms.
Several characteristics of the trauma memory have been linked to PTSD in non-postpartum samples (Ogle et al., 2016). In contrast to the memory of the traumatic event among individuals who do not develop PTSD, trauma memories in PTSD are characterized by emotional and sensory details, are involuntarily recalled and relived as if happening in the present, are central to the sufferer’s identity, and may lack coherence (Berman et al., 2020; Berntsen et al., 2003; Berntsen and Rubin, 2007; Ehlers and Clark, 2000; Michael et al., 2005; Rubin et al., 2011, 2004), although evidence for the latter is mixed (Berntsen et al., 2003; Rubin et al., 2011). These features of the trauma memory may in part reflect problems with the encoding of the traumatic information (Brewin, 1996; Ehlers and Clark, 2000). Trauma memories may be uniquely encoded into autobiographical memory, distinct from other memories, resulting in deficits in verbal recall (Brewin, 1996; Ehlers and Clark, 2000). Moreover, while most traumatic events are predominantly linked to negative emotions, childbirth is a complex event that is often associated with both positive and negative emotions (Slade et al., 1993). Hence the extent to which a traumatic childbirth memory in CB-PTSD will resemble the memory of other known traumatic events in non-childbirth-related PTSD warrants investigation.
To the best of our knowledge, there are only a handful of prior studies on traumatic childbirth memories in CB-PTSD. Based on self-report assessments, women with probable CB-PTSD report involuntarily recalling their childbirth experience more frequently. They describe their childbirth memories as characterized by emotional and sensory details, and being less coherent and more central to their identity (Foley et al., 2014). Narrative approaches, have yielded inconsistent findings regarding coherence of the traumatic childbirth memory (Ayers, 2007; Ayers et al., 2015; Briddon et al., 2011). This inconsistency may be due to samples limited in size and overall symptom severity, as well as methodological differences.
Importantly, previous studies have relied on a single methodology. Close-ended questions in standard psychometric questionnaires favor report of uncertain information (Lipton, 1976), may elicit misleading (Farrar and Goodman, 1992) and inaccurate information (Zaragoza and Mitchell, 1996), and may provoke inflated positive responses, indicative of self-deception (Taylor, 1983). In contrast, free recall paradigms, as in narrative approaches, allow reporting of the traumatic event to freely emerge. This way, participants are encouraged to report their own subjective story, including cognitions, perceptions, actions, and emotions (Dekel et al., 2016a; Dekel and Bonanno, 2013). The diverging strengths and weaknesses of self-report versus narrative assessments may be of particular significance when examining PTSD, in which unique encoding of trauma memories into autobiographical memory is hypothesized to result in involuntary deficits in verbal recall (Brewin, 1996; Ehlers and Clark, 2000). Thus, in PTSD, certain information may be accessed by questionnaires but not by free recall paradigms.
In an attempt to offer a broad investigation of childbirth memories and their association with CB-PTSD, the present study is the first to adopt a multi-method approach using both a self-report measure and linguistic coding of childbirth narratives. Based on the literature reviewed, we hypothesize that women who endorse CB-PTSD symptoms will self-report more emotional and sensory memory, involuntary recall, reliving, and centrality of the childbirth memory to their identity. Because of prior inconclusive evidence, no hypothesis regarding directionality of coherence was made. Additionally, we expect to find the same pattern in childbirth narratives, with CB-PTSD symptom endorsement being associated with more perceptual, affective, and cognitive processes.
Methods
Participants and Procedure
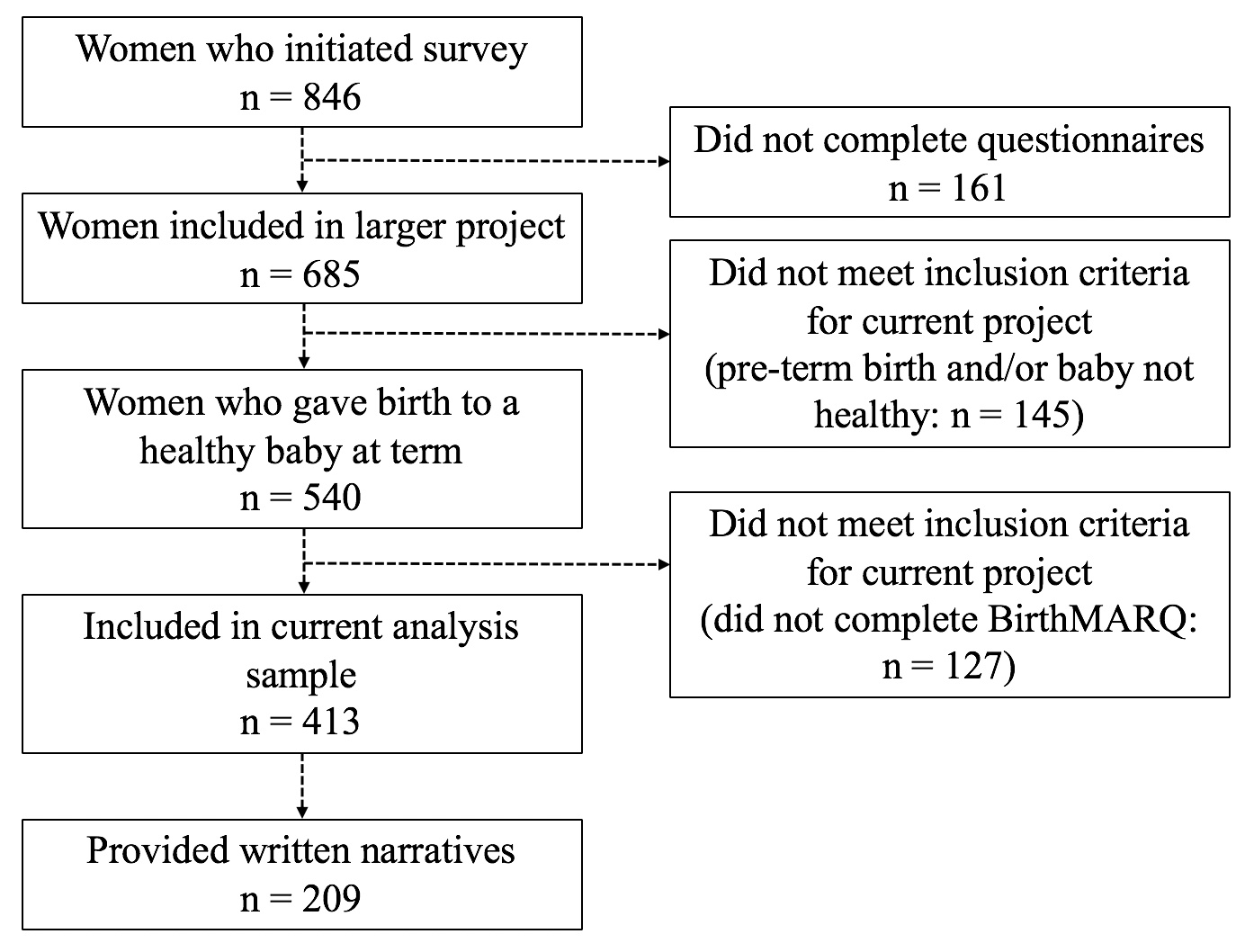
The current project is part of a larger study on psychological outcomes of childbirth (Dekel et al., 2019a, 2019b). Announcements on postpartum websites (e.g., Postpartum Progress) recruited participant candidates between November 2016 and April 2017. Inclusion criteria for the larger project included a live birth within the past six months and age ≥ 18. Participants were informed that they were implying consent by completing the anonymous online survey. The project was approved by the Partners Healthcare Human Research Committee and conducted in accordance with the Helsinki Declaration.
The larger project studied 685 women. For the current project, we only included the 413 participants who had delivered a healthy baby at term and who completed the study’s measures. Of these, 209 provided written narratives (see Flow Chart, Supplementary Material).
Measures
Socio-demographics and childbirth-related information.
We collected sociodemographic (e.g., age, education, marital status, mental health history) and childbirth-related information (e.g., mode of delivery, sleep deprivation, complications during labor and/or delivery) as single items. To assess mental health history, women were asked “Prior to your recent childbirth, did you suffer from a mental health problem(s)?”. Women then had the option to indicate having had PTSD prior to giving birth. Sleep deprivation was defined as less than 6 hours of sleep in the night prior to giving birth.
CB-PTSD symptoms were assessed using the PTSD Checklist for DSM-5 (PCL-5) (Weathers et al., 2013), which calls for the participant to rate symptom severity associated with an index event, in this case “the most recent childbirth. over the past month on 20 items from 0 (not at all) to 4 (extremely). Scores range from 0 to 80, with scores above 32 indicating clinically relevant symptom levels (Bovin et al., 2016). The PCL-5 has good psychometric properties (Blevins et al., 2015) and has been used to evaluate CB-PTSD (Scheepstra et al., 2017). For the present study, PCL-5 internal consistency was Cronbach’s α=0.95.
In accordance with DSM-5, we classified participants as probable CB-PTSD when endorsing at least one re-experiencing (cluster B) item, one avoidance (cluster C) item, two alterations in cognitions and mood (cluster D) items, and two reactivity and hyperarousal (cluster E) items. We conceptualized item endorsement as score ≥ 2 (at least moderate severity). We further assessed DSM-5 diagnostic criterion G, viz., symptoms create distress or functional impairment, with two additional PCL-5 items, again operationalizing scores ≥ 2 on either or both of these items as criterion G endorsement. Participants were classified as probable CB-PTSD when meeting DSM-5 criteria for PTSD and endorsing criterion G.
Childbirth memory qualities were evaluated using the Birth Memories and Recall Questionnaire (BirthMARQ) (Foley et al., 2014). Participants rated 21 items from 1 (strongly disagree) to 7 (strongly agree). Ratings were used to compute six subscales (emotional memory, reliving, centrality of memory, sensory memory, recall, incoherence (inverse of coherence). The BirthMARQ has good psychometric properties (Foley et al., 2014). In the current study, α=0.83 for the entire scale, and 0.75–0.90 for the six subscales.
Childbirth narratives were collected in a free recall paradigm under the instruction: “In your own words, please briefly describe anything that comes to mind about your delivery experience, focusing on thoughts, emotions, and your physical experience.” We used Linguistic Inquiry and Word Count (LIWC) (Pennebaker et al., 2015) software for this analysis. Based on an external dictionary including almost 6400 words and word stems, LIWC categorizes written text along numerous linguistic dimensions. The software evaluates each word in the narrative against the dictionary and assigns it to one or more categories. Output includes percentage scores for each linguistic dimension per narrative (i.e., total number of words referring to a specific dimension divided by total narrative word count). For the current project, we used LIWC software to investigate four categories, viz., affective (i.e., words such as “happy”, “cried”), cognitive (i.e., words such as “cause”, “ought”, “know”), perceptual (i.e., words such as “look”, “heard”) processes, and death (i.e., words such as “kill”, “dead”)., as well as total word count. LIWC categories have demonstrated good psychometric properties regarding external, predictive, and construct validity (Pennebaker et al., 2015, 2007; Pennebaker and King, 1999).
Incoherence.
After reading each narrative, and without knowledge of the participants’ questionnaire scores or diagnosis, two raters separately scored incoherence from 0 (coherent) to 10 (incoherent). Scoring was based on the rules established by Foa and colleagues, particularly focusing on repetition utterances, disorganized, organized, and unfinished thoughts (Foa et al., 1995; Halligan et al., 2003; Murray et al., 2002). Interrater reliability was good (ICC=0.87). Raters’ scores were averaged into a single, interval incoherence variable.
Postpartum depression was evaluated using the 6-item Depression subscale of the Brief Symptom Inventory (BSI) (Derogatis, 1993). Participants rated each item’s severity over the past week from 0 (not at all) to 4 (extremely). Scores on each of the 6 items were summed. The BSI has good psychometric properties (Derogatis, 1993) and has previously been used in postpartum samples (Ross et al., 2003). For the present sample, α=0.92.
Data Analyses
Data analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS) version 25. We used Little’s Missing Completely At Random (MCAR) test to examine missing data patterns. Independent t-tests, chi-square tests, and Fisher’s exact tests were used to (1) compare BirthMARQ responders (n=413) versus BirthMARQ non-responders (n=127) and narrative responders (n=209) versus narrative non-responders (n=204) regarding sociodemographic and childbirth-related variables and the PCL-5; and (2) investigate potential differences between the CB-PTSD and no-CB-PTSD groups on sociodemographic and childbirth-related variables. Associations between the various memory outcome measures and demographic and childbirth-related measures, as well as the PCL-5 were assessed using Pearson product-moment correlations.
We utilized Multivariate Analysis of Covariance (MANCOVA) to test for differences between CB-PTSD and no-CB-PTSD groups on the six BirthMARQ subscales simultaneously, adjusting for premorbid and childbirth-related variables. In order to test whether CB-PTSD symptom endorsement is associated with different patterns in written narratives, we used Multivariate Analysis of Variance (MANOVA) to test for group differences on the five LIWC categories, as well as incoherence coding, simultaneously.
Results
Responders versus Non-Responders
Among the 540 women who delivered a healthy baby at term, BirthMARQ responders (n=413) had more days passed since birth than BirthMARQ non-responders (n=127) (Mdiff=−11.31, t(538)=−2.07, p=0.04). More BirthMARQ responders (46%) than BirthMARQ non-responders (34%) reported labor or delivery complications (Fisher’s exact test p=0.01). Among those classified as probable CB-PTSD (n=86), 92% (n=79) opted to complete the BirthMARQ, whereas 74% (n=334) of those with no-CB-PTSD (n=454) did so (Fisher’s exact test p<0.001). Further, among those classified as probable CB-PTSD, BirthMARQ responders (n=79) had significantly lower endorsement of cluster C, i.e., avoidance, than BirthMARQ non-responders (n=7) (Mdiff=1.57, t(84)=2.73, p=0.045).
Narrative responders (n=209) were less likely than narrative non-responders (n=204) to have an annual household income lower than $20.000 (narrative responders: 3%; narrative non-responders: 11%; X2(4,N=413)=12.86, p=0.01). More narrative responders than narrative non-responders reported labor or delivery complications (responders: 51%; non-responders: 41%; Fisher’s exact test p=0.04). On the PCL-5, narrative responders reported higher re-experiencing (Mdiff=−0.95, t(407.69)=−1.98, p=0.049) and avoidance (Mdiff=−0.49, t(401.14)=−2.09, p=0.04) than narrative non-responders.
More of those classified as probable CB-PTSD (61%, n=48) than no-CB-PTSD (48%, n=161) opted to provide narratives (Fisher’s exact test p=0.046). There were no differences between narrative responders and narrative non-responders classified as probable CB-PTSD regarding any of the PCL-5 symptom clusters, or demographic or childbirth-related information.
Demographics and Descriptives
For the sample of responders whose data were analyzed (n=413), mean age was 31 (SD=5). They were studied at mean 102 (SD=53) days postpartum. The majority resided in North America (86%, n=336), held a higher education degree (73%, n=303), was married (94%, n=389), Caucasian (91% n=376), and middle class (median household income=$50,000–$99,000, n=143). Most women were primiparous (53%, n=220) and delivered vaginally (68%, n=282). PCL-5 scores ranged from 0 to 80 (M=21.9, SD=18.9). Nineteen percent (19%, n=79) were classified as probable CB-PTSD.
Differences between the CB-PTSD (n=79) and no-CB-PTSD (n=334) included prior mental health problems (CB-PTSD: 63%; no-CB-PTSD: 36%; Fisher’s exact test p<0.001), prior non-childbirth related PTSD (CB-PTSD: 20%; no-CB-PTSD: 4%; p<0.001), pain (on a 1–5 scale) during labor and/or delivery (Mdiff=0.34, t(109.0)=−2.34, p=0.02), and current symptoms of depression (on a 0–4 scale) (Mdiff=1.39, t(411)=−11.21, p<0.001). In the CB-PTSD group, more women reported unscheduled Caesarean section (CB-PTSD: 27%; no-CB-PTSD: 11%; Fisher’s exact test p=.001), labor and/or delivery complications (CB-PTSD: 75%; no-CB-PTSD: 39%; p<0.001), and sleep deprivation (CB-PTSD: 86%; no-CB-PTSD: 63%; p<0.001).
CB-PTSD and Self-Reported Childbirth Memories
Pearson correlations between BirthMARQ subscales, sociodemographic and childbirth-related information, and PCL-5 total and cluster scores can be found in Table 1.
Table 1.
Pearson Correlations Between Premorbid and Childbirth-Related Factors and BirthMARQ Subscales
| Emotional Memory | Reliving | Centrality of Memory | Sensory Memory | Recall | Incoherence | |
|---|---|---|---|---|---|---|
| Age | 0.05 | −0.05 | −0.14** | −0.09 | −0.08 | 0.05 |
| Education | 0.05 | −0.05 | −0.04 | −0.13** | −0.12* | −0.003 |
| Marital Status | −0.03 | 0.08 | 0.04 | 0.03 | 0.04 | 0.06 |
| Prior Mental Health | 0.12* | 0.06 | 0.08 | 0.09 | 0.08 | 0.07 |
| Problems | ||||||
| Prior PTSD | 0.16** | 0.14** | 0.14** | 0.19** | 0.20** | 0.16** |
| Days postpartum | 0.05 | −0.01 | 0.04 | −0.06 | 0.07 | 0.06 |
| Unscheduled C | 0.26** | 0.13** | 0.10* | −0.01 | 0.12* | 0.15** |
| Sleep deprivation | 0.25** | 0.08 | 0.12* | 0.02 | 0.13** | 0.21** |
| Complications | 0.41** | 0.14** | 0.20** | 0.02 | 0.23** | 0.25** |
| Pain during L&D | 0.16** | 0.05 | 0.15** | 0.004 | 0.15** | 0.05 |
| PCL-5 Total | 0.50** | 0.42** | 0.45** | 0.26** | 0.52** | 0.42** |
| PCL-5 Cluster B | 0.51** | 0.49** | 0.46** | 0.26** | 0.60** | 0.37** |
| PCL-5 Cluster C | 0.51** | 0.37** | 0.40** | 0.18** | 0.50** | 0.40** |
| PCL-5 Cluster D | 0.46** | 0.34** | 0.39** | 0.24** | 0.44** | 0.41** |
| PCL-5 Cluster E | 0.32** | 0.30** | 0.33** | 0.22** | 0.35** | 0.29** |
Note. BirthMARQ = Birth Memories and Recall Questionnaire. PCL-5 = PTSD Checklist for DSM-5. PTSD = Posttraumatic Stress Disorder. Prior PTSD indicates non-childbirth related PTSD. Unscheduled C = Unscheduled Caesarean section. Preferred mode refers to preferred mode of delivery. Complications refers to complications during labor and/or delivery. L&D = Labor and Delivery. Clusters B-E assessed with PCL-5.
p < 0.05;
p < 0.01
A MANCOVA including BirthMARQ subscales as simultaneous dependent variables indicated a significant effect of CB-PTSD group, adjusted for prior PTSD, sleep deprivation, labor and delivery complications, unscheduled Caesareans, pain during labor and delivery, and depression (Wilks’ λ=0.81, F(6,307)=11.70, p<0.001, ɳ2p=0.19). The CB-PTSD group scored higher on emotional memory, sensory memory, reliving, centrality of memory, recall, and incoherence than the no-CB-PTSD group (Table 2).
Table 2.
MANCOVA Comparisons and Univariate Effects of CB-PTSD Groups on BirthMARQ
| 95% CI for MDiff |
||||||||
|---|---|---|---|---|---|---|---|---|
| DV | df | df error | F | ɳ2p | CB-PTSD Group | Mean | Lower Bound | Upper Bound |
| Emotional Memory | 1 | 312 | 15.08** | 0.05 | CB-PTSD | 23.67 | 2.25 | 6.86 |
| No-CB-PTSD | 19.12 | |||||||
| Reliving | 1 | 312 | 22.95** | 0.07 | CB-PTSD | 17.05 | 2.55 | 6.11 |
| No-CB-PTSD | 12.72 | |||||||
| Centrality of Memory | 1 | 312 | 24.26** | 0.07 | CB-PTSD | 19.89 | 3.28 | 7.63 |
| No-CB-PTSD | 14.44 | |||||||
| Sensory Memory | 1 | 312 | 4.50* | 0.01 | CB-PTSD | 15.86 | 0.16 | 4.16 |
| No-CB-PTSD | 13.70 | |||||||
| Recall | 1 | 312 | 45.23** | 0.13 | CB-PTSD | 10.15 | 2.69 | 4.91 |
| No-CB-PTSD | 6.35 | |||||||
| Incoherence | 1 | 312 | 17.96** | 0.05 | CB-PTSD | 7.03 | 1.38 | 3.76 |
| No-CB-PTSD | 4.46 | |||||||
Note. MANCOVA = Multivariate Analysis of Covariance. BirthMARQ = Birth Memories and Recall Questionnaire. DV = Dependent variable. All DVs measured with BirthMARQ. ɳ2p= partial eta-squared. CB-PTSD = Childbirth-Related Posttraumatic Stress Disorder. CB-PTSD n = 79; no-CB-PTSD n = 332. Mean denotes estimated marginal means. 95% CI for MDiff = 95% Confidence Interval for the mean difference between the groups. Adjusted for prior PTSD, sleep deprivation, labor and delivery complications, unscheduled Caesarean, pain during labor and delivery, and depression.
p = 0.05;
p < 0.001
CB-PTSD and Childbirth Narratives
Because there were no significant associations between premorbid and childbirth-related factors and word count, affective, cognitive processes, perceptual processes, and death related words, as well as incoherence, we utilized MANOVA. The main effect of CB-PTSD group on the six simultaneous variables was significant (Wilks’ λ=0.85, F(9,199)=3.82, p<.001, ɳ2p=0.15). The CB-PTSD group made fewer references to affective processes and positive emotions, and more references to cognitive processes (Table 3).
Table 3.
Significant Univariate Effects of CB-PTSD vs. No-CB-PTSD Groups on LIWC Narrative Variables
| 95% CI for MDiff |
||||||||
|---|---|---|---|---|---|---|---|---|
| DV | df | df error | F | ɳ2p | Group | Mean | Lower Bound | Upper Bound |
| Affective processes | 1 | 207 | 5.78* | 0.03 | CB-PTSD | 5.37 | −2.07 | −0.21 |
| No-CB-PTSD | 6.51 | |||||||
| Positive emotions | 1 | 207 | 12.91** | 0.06 | CB-PTSD | 1.31 | −1.67 | −0.49 |
| No-CB-PTSD | 2.39 | |||||||
| Cognitive processes | 1 | 207 | 4.29* | 0.02 | CB-PTSD | 11.84 | 0.07 | 2.67 |
| No-CB-PTSD | 10.48 | |||||||
Note. MANOVA = Multivariate Analysis of Variance. DV = Dependent variable. All DVs quantified using Linguistic Inquiry and Word Count (LIWC) software. ɳ2p = partial eta-squared. CB-PTSD = Childbirth-Related Posttraumatic Stress Disorder. CB-PTSD n = 48; no-CB-PTSD n = 161. Mean denotes estimated marginal means. 95% CI for MDiff = 95% Confidence Interval for the mean difference between the groups.
p < 0.05;
p < 0.01
Discussion
Using a multi-method approach, we examined traumatic childbirth memories in relation to childbirth-related posttraumatic stress disorder. To the best of our knowledge, this is the first study to combine both a self-report (BirthMARQ) and a quantitative (LIWC) measure in the analysis of childbirth narratives. On the BirthMARQ questionnaire, women with probable CB-PTSD reported to involuntarily recall their childbirth experience more frequently and the memory of childbirth to be characterized by more emotional and sensory details. They also indicated the childbirth memory to be more incoherent, as well as more central to their identity. Written childbirth narratives in CB-PTSD were characterized by fewer affective details and positive emotions, and more cognitive processes.
Our findings regarding self-reported childbirth memory characteristics in CB-PTSD are consistent with the general PTSD literature. Following traumatic childbirth experiences, deficits in encoding the childbirth experience into autobiographical memory may facilitate involuntary recollections with a sense of “nowness” and heightened emotional and sensory detail. Neural abnormalities in the amygdala seen in PTSD patients may explain incoherence and involuntary recall and reliving with high emotional and perceptual arousal. The single previous study that examined reliving in childbirth memories did not report a relationship with CB-PTSD (Foley et al., 2014), and this in part may be due to not controlling for depression symptoms (Foley et al., 2014).
We further found the childbirth experience to be more central to women’s identity in CB-PTSD. Although for most women, childbirth may be integrated into identity as a central event, if experienced as negative, it may threaten women’s perception of the self in their newly acquired maternal role. The childbirth experience being more central to identity in CB-PTSD is in line with a landmark hypothesis (Berntsen et al., 2003), according to which highly emotional events act as landmarks within the memory network.
The apparent conflict between less affective references in narratives and more self-reported emotional memory may be explained by PTSD status itself. In seminal models of PTSD, unique encoding of trauma memories into autobiographical memory is hypothesized to result in involuntary deficits in verbal recall (Brewin, 1996; Ehlers and Clark, 2000). Thus, those with PTSD may be readily able to self-report high emotional content of the trauma memory in response to direct questions, while having difficulties describing specific emotional reactions in a free recall paradigm.
Increased cognitive processes in PTSD have been documented in some prior studies (e.g., Dekel and Bonanno, 2013). In the case of traumatic childbirth narratives, they may represent women trying to make sense of the event while being “haunted” by the memory and simultaneously attempting to establish a socially acceptable narrative.
Influenced by cultural factors such as expectations of childbirth being a positive event, childbirth constitutes a unique traumatic event in that, in contrast to other traumatic events, it is commonly talked about. Talking or writing about a highly stressful event may encourage natural recovery (Alisic et al., 2016). Narratives may help to create meaning and recruit social support (Harber and Cohen, 2005), and they are a crucial component of therapeutic interventions such as Prolonged Exposure Therapy (Alisic et al., 2016). We found BirthMARQ responders with CB-PTSD to present lower endorsement of DSM-5 cluster C, i.e., avoidance, than BirthMARQ non-responders with CB-PTSD, but we did not find such a difference regarding narrative responders vs. narrative non-responders. Following the aforementioned reasoning, women may have already had the opportunity to rehearse a coherent narrative of their childbirth experience, reducing their motivation to avoid writing a narrative and offering another explanation for our finding of no evidence for incoherent narratives in those with CB-PTSD. Nonetheless, childbirth narratives may also have been rehearsed to comply with culturally acceptable perceptions of childbirth and may therefore diverge from actuality. Although women with CB-PTSD may be less likely than women with PTSD from other events to avoid recalling a narrative of their childbirth experience, they may provide “socially acceptable” versions.
Several limitations should be considered. First, our sample stems from an anonymous online survey, raising the possibility of selection and severity-related reporting biases. It should further be acknowledged that not all women who initiated the survey completed all measures. Because the outcome measures included in the current report (i.e., BirthMARQ, written narratives) were included towards the end of the survey, the current analysis sample was reduced by women terminating the survey before completion of all questionnaires. In addition, information pertaining to current medication use or treatment status was no collected and could thus not be controlled for in the present analyses. Second, although we assessed CB-PTSD and depression with well-validated measures, we did not utilize clinical assessments. Third, the survey was in English and thus, the current sample may over-represent native English speakers. Although most participants resided in North America, the sample includes women from other regions. There may be undetected cultural influences in coping with trauma and postpartum adaptation. Despite these methodological limitations, this study is pioneering in examining traumatic childbirth memories in a large sample, using a multi-method approach.
In summary, we conclude that childbirth memories in women who endorse symptoms of childbirth-related posttraumatic stress in the early postpartum period resemble those described in the general PTSD literature, with regard to greater traumatic memory centrality, more involuntary recall, greater self-reported emotional and sensory detail, and greater self-reported incoherence, as well as fewer positive words, and more cognitive processing words, in trauma narratives. Our findings indicate that childbirth can trigger a traumatic response possibly resulting in distinct encoding of the traumatic childbirth memory, ultimately creating a path toward the development and maintenance of CB-PTSD. Given the detrimental impact of CB-PTSD on mother, child, and the entire family, our findings highlight the need to develop interventions that modify traumatic memories of childbirth in women at risk for CB-PTSD. In light of the complex experience of childbirth, future research investigating characteristics of traumatic childbirth memories is needed to advance our understanding of this overlooked postpartum condition.
Supplementary Material
{kind=link}
Highlights.
The role of trauma memories in childbirth-related (CB-)PTSD requires explication
CB-PTSD relates to incoherence and more emotional and sensory details
CB-PTSD relates to more involuntary recall, reliving, centrality to identity
Narratives in CB-PTSD characterized by less affective, and more cognitive processes
Trauma memories in CB-PTSD resemble those described in the general PTSD literature
Funding:
Sharon Dekel received the Mass General Executive Committee on Research (ISF) award.
The authors would like to thank Prof. James W. Pennebaker for his generous contributions regarding the narrative analysis software, as well as Ms. Shannon Henning for her generous support in initiating this research project.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interest: none
References
- Alisic E, Krishna RN, Robbins ML, Mehl MR, 2016. A Comparison of Parent and Child Narratives of Children’s Recovery From Trauma. J. Lang. Soc. Psychol 35, 224–235. 10.1177/0261927X15599557 [DOI] [Google Scholar]
- American Psychiatric Association, 2013. Diagnostic and Statistical Manual of Mental Disorders: DSM-V 10.1176/appi.books.9780890425596.744053 [DOI]
- Ayers S, 2007. Thoughts and emotions during traumatic birth: A qualitative study. Birth 34, 253–263. 10.1111/j.1523-536X.2007.00178.x [DOI] [PubMed] [Google Scholar]
- Ayers S, Radoš SN, Balouch S, 2015. Narratives of traumatic birth: Quality and changes over time. Psychol. Trauma Theory, Res. Pract. Policy 7, 234–242. 10.1037/a0039044 [DOI] [PubMed] [Google Scholar]
- Berman Z, Thiel F, Dishy GA, Chan SJ, Dekel S, 2020. Maternal psychological growth following childbirth. Arch. Womens. Ment. Health 10.1007/s00737-020-01053-9 [DOI] [PubMed]
- Berntsen D, Rubin DC, 2007. When a trauma becomes a key to identity. Enhanc. Integr. trauma memories Predict. posttraumatic Stress Disord. symptoms 21, 417–431. [Google Scholar]
- Berntsen D, Rubin DC, 2006. The centrality of event scale: A measure of integrating a trauma into one’s identity and its relation to post-traumatic stress disorder symptoms. Behav. Res. Ther 10.1016/j.brat.2005.01.009 [DOI] [PMC free article] [PubMed]
- Berntsen D, Willert M, Rubin C, D., 2003. Splintered memories or vivid landmarks? Qual. Organ. Trauma. memories with without PTSD 17, 675. [Google Scholar]
- Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL, 2015. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 28, 489–498. 10.1002/jts.22059 [DOI] [PubMed] [Google Scholar]
- Bovin MJ, Marx BP, Weathers FW, Gallagher MW, Rodriguez P, Schnurr PP, Keane TM, 2016. Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders-fifth edition (PCL-5) in veterans. Psychol. Assess 28, 1379–1391. 10.1037/pas0000254 [DOI] [PubMed] [Google Scholar]
- Brewin CR, 2014. Episodic memory, perceptual memory, and their interaction: Foundations for a theory of posttraumatic stress disorder. Psychol. Bull 140, 69–97. 10.1037/a0033722 [DOI] [PubMed] [Google Scholar]
- Brewin CR, 2011. The Nature and Significance of Memory Disturbance in Posttraumatic Stress Disorder. Annu. Rev. Clin. Psychol 7, 203–227. 10.1146/annurev-clinpsy-032210-104544 [DOI] [PubMed] [Google Scholar]
- Brewin CR, 2001. Memory processes in post-traumatic stress disorder. Int. Rev. Psychiatry 10.1080/09540260120074019 [DOI]
- Brewin CR, 1996. Cognitive processing of adverse experiences. Int. Rev. Psychiatry 10.3109/09540269609051548 [DOI]
- Briddon E, Slade P, Isaac C, Wrench I, 2011. How do memory processes relate to the development of posttraumatic stress symptoms following childbirth? J. Anxiety Disord 25, 1001–1007. 10.1016/j.janxdis.2011.06.008 [DOI] [PubMed] [Google Scholar]
- Brown AD, Antonius D, Kramer M, Root JC, Hirst W, 2010. Trauma centrality and PTSD in veterans returning from Iraq and Afghanistan. J. Trauma. Stress 10.1002/jts.20547 [DOI] [PubMed]
- Crespo M, Fernandez-Lansac V, 2016. Memory and Narrative of Traumatic Events: A Literature Review. Psychol. Trauma Theory, Res. Pract. Policy 8, 149–156. 10.1037/tra0000041 [DOI] [PubMed] [Google Scholar]
- Czarnocka J, Slade P, 2000. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br. J. Clin. Psychol 39, 35–51. 10.1348/014466500163095 [DOI] [PubMed] [Google Scholar]
- Dekel S, Bonanno GA, 2013. Changes in trauma memory and patterns of posttraumatic stress. Psychol. Trauma Theory, Res. Pract. Policy 10.1037/a0022750 [DOI]
- Dekel S, Ein-Dor T, Berman Z, Barsoumian IS, Agarwal S, Pitman RK, 2019a. Delivery mode is associated with maternal mental health following childbirth. Arch. Womens. Ment. Health 22, 817–824. 10.1007/s00737-019-00968-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dekel S, Ein-Dor T, Dishy GA, Mayopoulos PA, 2019b. Beyond postpartum depression: posttraumatic stress-depressive response following childbirth. Arch. Womens. Ment. Health 23, 557–564. 10.1007/s00737-019-01006-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dekel S, Hankin IT, Pratt JA, Hackler DR, Lanman ON, 2016a. Posttraumatic Growth in Trauma Recollections of 9/11 Survivors: A Narrative Approach. J. Loss Trauma 10.1080/15325024.2015.1108791 [DOI]
- Dekel S, Solomon Z, Ein-Dor T, 2016b. PTSD symptoms lead to modification in the memory of the trauma: A prospective study of former prisoners of war. J. Clin. Psychiatry 10.4088/JCP.14m09114 [DOI] [PubMed]
- Dekel S, Stuebe C, Dishy G, 2017. Childbirth induced posttraumatic stress syndrome: A systematic review of prevalence and risk factors. Front. Psychol 10.3389/fpsyg.2017.00560 [DOI] [PMC free article] [PubMed]
- Dekel S, Thiel F, Dishy G, Ashenfarb AL, 2019c. Is childbirth-induced PTSD associated with low maternal attachment? Arch. Womens. Ment. Health 22, 119–122. 10.1007/s00737-018-0853-y [DOI] [PubMed] [Google Scholar]
- Derogatis LR, 1993. BSI: brief symptom inventory. Minneap. Natl. Comput. Syst 32–40. 10.1037/t00789-000 [DOI]
- Ehlers A, Clark DM, 2000. A cognitive model of posttraumatic stress disorder. Behav. Res. Ther 38, 319–345. 10.1016/S0005-7967(99)00123-0 [DOI] [PubMed] [Google Scholar]
- Farrar MJ, Goodman GS, 1992. Developmental Changes in Event Memory. Child Dev 10.1111/j.1467-8624.1992.tb03605.x [DOI] [PubMed]
- Foa EB, Molnar C, Cashman L, 1995. Change in rape narratives during exposure therapy for posttraumatic stress disorder. J. Trauma. Stress 8, 675–690. 10.1007/BF02102894 [DOI] [PubMed] [Google Scholar]
- Foley S, Crawley R, Wilkie S, Ayers S, 2014. The Birth Memories and Recall Questionnaire (BirthMARQ): Development and evaluation. BMC Pregnancy Childbirth 14 10.1186/1471-2393-14-211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garthus-Niegel S, Ayers S, Martini J, Von Soest T, Eberhard-Gran M, 2017. The impact of postpartum post-traumatic stress disorder symptoms on child development: A population-based, 2-year follow-up study. Psychol. Med 47, 161–170. 10.1017/S003329171600235X [DOI] [PubMed] [Google Scholar]
- Garthus-Niegel S, Horsch A, Handtke E, von Soest T, Ayers S, Weidner K, Eberhard-Gran M, 2018. The impact of postpartum posttraumatic stress and depression symptoms on couples’ relationship satisfaction: A population-based prospective study. Front. Psychol 9 10.3389/fpsyg.2018.01728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halligan SL, Michael T, Clark DM, Ehlers A, 2003. Posttraumatic stress disorder following assault: The role of cognitive processing, trauma memory, and appraisals. J. Consult. Clin. Psychol 71, 419–431. 10.1037/0022-006X.71.3.419 [DOI] [PubMed] [Google Scholar]
- Harber KD, Cohen DJ, 2005. The emotional broadcaster theory of social sharing. J. Lang. Soc. Psychol 24, 382–400. 10.1177/0261927X05281426 [DOI] [Google Scholar]
- Jones C, Harvey AG, Brewin CR, 2007. The organisation and content of trauma memories in survivors of road traffic accidents. Behav. Res. Ther 45, 151–162. 10.1016/j.brat.2006.02.004 [DOI] [PubMed] [Google Scholar]
- LaBar KS, Cabeza R, 2006. Cognitive neuroscience of emotional memory. Nat. Rev. Neurosci 10.1038/nrn1825 [DOI] [PubMed]
- Lipton JP, 1976. On the psychology of eyewitness testimony. J. Appl. Psychol 10.1037/0021-9010.62.1.90 [DOI]
- Michael T, Ehlers A, Halligan SL, Clark DM, 2005. Unwanted memories of assault: What intrusion characteristics are associated with PTSD? Behav. Res. Ther 43, 613–628. 10.1016/j.brat.2004.04.006 [DOI] [PubMed] [Google Scholar]
- Murray J, Ehlers A, Mayou RA, 2002. Dissociation and post-traumatic stress disorder: Two prospective studies of road traffic accident survivors. Br. J. Psychiatry 180, 363–368. 10.1192/bjp.180.4.363 [DOI] [PubMed] [Google Scholar]
- O’Kearney R, Perrott K, 2006. Trauma narratives in posttraumatic stress disorder: A review. J. Trauma. Stress 10.1002/jts.20099 [DOI] [PubMed]
- Ogle CM, Rubin DC, Siegler IC, 2016. Accounting for posttraumatic stress disorder symptom severity with pre-and posttrauma measures: A longitudinal study of older adults. Clin. Psychol. Sci 4, 272–286. 10.1177/2167702615583227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pennebaker JW, Boyd RL, Jordan K, Blackburn K, 2015. The development and psychometric properties of LIWC2015 University of Texas at Austin, Austin, TX. [Google Scholar]
- Pennebaker JW, Chung CK, Ireland M, Gonzales A, Booth RJ, 2007. The Development and Psychometric Properties of LIWC2007 The University of Texas at Austin. Development 10.1068/d010163 [DOI]
- Pennebaker JW, King LA, 1999. Linguistic styles: Language use as an individual difference. J. Pers. Soc. Psychol 10.1037/0022-3514.77.6.1296 [DOI] [PubMed]
- Pitman RK, 1989. Post-traumatic stress disorder, hormones, and memory. Biol. Psychiatry 10.1016/0006-3223(89)90033-4 [DOI] [PubMed]
- Pitman RK, Orr SP, 2012. Psychophysiology of Emotional Memory Networks in Posttraumatic Stress Disorder, in: Brain and Memory: Modulation and Mediation of Neuroplasticity 10.1093/acprof:oso/9780195082944.003.0003 [DOI]
- Robinaugh DJ, McNally RJ, 2011. Trauma centrality and PTSD symptom severity in adult survivors of childhood sexual abuse. J. Trauma. Stress 10.1002/jts.20656 [DOI] [PubMed]
- Ross LE, Evans SEG, Sellers EM, Romach MK, 2003. Measurement issues in postpartum depression part 1: Anxiety as a feature of postpartum depression. Arch. Womens. Ment. Health 6, 51–57. 10.1007/s00737-002-0155-1 [DOI] [PubMed] [Google Scholar]
- Rubin DB, 2009. Multiple imputation for nonresponse in surveys (Vol. 307). Wiley, Hoboken, NJ. [Google Scholar]
- Rubin DC, Dennis MF, Beckham JC, 2011. Autobiographical memory for stressful events: The role of autobiographical memory in posttraumatic stress disorder. Conscious. Cogn 20, 840–856. 10.1016/j.concog.2011.03.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin DC, Feldman ME, Beckham JC, 2004. Reliving, emotions, and fragmentation in the autobiographical memories of veterans diagnosed with PTSD. Appl. Cogn. Psychol 18, 17–35. 10.1002/acp.950 [DOI] [Google Scholar]
- Say L, Chou D, Gemmill A, Tunçalp Ö, Moller A-B, Daniels J, Gülmezoglu AM, Temmerman M, Alkema L, 2014. Global causes of maternal death: a WHO systematic analysis. Lancet. Glob. Heal 2, e323–33. 10.1016/S2214-109X(14)70227-X [DOI] [PubMed] [Google Scholar]
- Scheepstra KWF, van Steijn ME, Dijksman LM, van Pampus MG, 2017. Post-traumatic stress disorder in women and their partners, following severe post-partum hemorrhage: A study protocol for a prospective cohort study. Cogent Med 4 10.1080/2331205x.2017.1278840 [DOI] [Google Scholar]
- Slade P, MacPherson SA, Hume A, Maresh M, 1993. Expectations, experiences and satisfaction with labour. Br. J. Clin. Psychol 32, 469–483. 10.1111/j.2044-8260.1993.tb01083.x [DOI] [PubMed] [Google Scholar]
- Speckens AEM, Ehlers A, Hackmann A, Clark DM, 2006. Changes in intrusive memories associated with imaginal reliving in posttraumatic stress disorder. J. Anxiety Disord 20, 328–341. 10.1016/j.janxdis.2005.02.004 [DOI] [PubMed] [Google Scholar]
- Taylor SE, 1983. Adjustment to threatening events: A theory of cognitive adaptation. Am. Psychol 10.1037/0003-066X.38.11.1161 [DOI]
- Thiel F, Dekel S, 2020. Peritraumatic dissociation in childbirth-evoked posttraumatic stress and postpartum mental health. Arch. Womens. Ment. Health 23, 189–197. 10.1007/s00737-019-00978-0 [DOI] [PubMed] [Google Scholar]
- Thiel F, Ein-Dor T, Dishy G, King A, Dekel S, 2018. Examining Symptom Clusters of Childbirth-Related Posttraumatic Stress Disorder. Prim. Care Companion CNS Disord 20 10.4088/pcc.18m02322 [DOI] [PubMed] [Google Scholar]
- Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP, 2013. The PTSD Checklist for DSM-5 (PCL-5). Natl. Cent. PTSD 5, 2002 10.1037/t02622-000 [DOI] [Google Scholar]
- Yehuda R, 2002. Post-traumatic stress disorder. N. Engl. J. Med 10.1056/NEJMra012941 [DOI] [PubMed]
- Yildiz PD, Ayers S, Phillips L, 2017. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord 208, 634–645. 10.1016/j.jad.2016.10.009 [DOI] [PubMed] [Google Scholar]
- Zaragoza MS, Mitchell KJ, 1996. Repeated exposure to suggestion and the creation of false memories. Psychol. Sci 10.1111/j.1467-9280.1996.tb00377.x [DOI]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.