

Abstract
Background:
Sexual minority college students are at a higher risk for suicidal thoughts and self-injurious behaviors compared to heterosexual students. Minority stress theory proposes sexual minority individuals experience higher stress due to stigma. Using a sample of Mexican college students, this study tested perceived life stress as a mediator of suicide and self-injury outcomes across various sexual orientation groups.
Methods:
The sample of college students (N=7882) was recruited from nine Mexican universities as part of the WHO World Mental Health International College Student (WMH-ICS) initiative. Participants completed an online survey including demographic questions, measure of perceived life stress, suicide outcomes, and non-suicidal self-injury (NSSI) in the past 12 months.
Results:
Logistic regression analyses revealed identifying as a sexual minority significantly predicted a higher likelihood of suicide ideation (ORs 2.05–3.00), suicide attempts (ORs 2.48–8.73), and NSSI (ORs 2.92–4.18) compared to heterosexual students reporting no same-gender attraction. Significant indirect effects from mediation path analyses showed perceived life stress mediated the relationship between a sexual minority identity and suicide ideation (range of proportion mediated 10.48–31.48%), attempts (10.48–31.48%), and NSSI (7.69–20.09%) across each group except among asexual students.
Limitations:
The cross-sectional nature of the survey design precludes drawing causal inferences.
Conclusion:
Findings from this study contribute to minority stress theory by elucidating the role of perceived life stress as a mediator of suicide ideation and attempts and NSSI among sexual minority college students. Clinical interventions may benefit in focusing on experiences of stress across various life areas when supporting sexual minority college students.
Keywords: suicide, self-injury, sexual minority, college, Mexico
Introduction
Empirical evidence has shown that individuals identifying as a minority sexual identity (e.g., lesbian, gay, bisexual) are more likely to endorse suicide ideation, report a previous suicide attempt, and engage in non-suicidal self-injury (NSSI) compared to heterosexual individuals (Batejan et al., 2015; Haas et al., 2011; King et al., 2008; Marshal et al., 2011; Plöderl et al., 2014). Higher psychological distress has also been documented among individuals who identify as heterosexual yet report same-gender attraction (SGA), identify as asexual, and among people who are unsure of their sexuality (Greaves et al., 2017; Kuyper and Bos, 2016), but this evidence is scarce. Minority stress theory (Meyer, 2013, 2003) proposes that individuals from stigmatized social groups (e.g., sexual minority individuals) may be more likely to experience higher stress due to experiences of discrimination; subsequently, higher stress may lead to mental illness. Empirical evidence has supported perceived stress as a mediator between a sexual minority identity and depression (Krueger et al., 2018). Yet, these pathways have not been tested in predicting suicide ideation, attempts, and NSSI among sexual minority college students. Moreover, current research overemphasizes Eurocentric, White populations when studying sexual minority health (Plöderl and Tremblay, 2015).
Suicide is the second leading cause of death among college-age young adults worldwide (World Health Organization, 2016). College students may also be at a higher risk for non-suicidal self-injurious behaviors, defined as intentional damage or harm to one’s body without the intent of ending one’s life (Auerbach et al., 2018; Nock and Favazza, 2009). A meta-analysis of college student samples from around the world estimated that approximately 22.3% of students report lifetime suicide ideation, plans, or attempts. For 12-month prevalence, estimates were 10.6% for suicide ideation, 3.0% for suicide plans, and 1.2% for suicide attempts (Mortier et al., 2018). Another meta-analysis estimated a 13.4% lifetime prevalence of NSSI among young adults (Swannell et al., 2014) while a prospective assessment of NSSI in a sample of Belgian college students reported 10.3% incidence within the first year of college (Kiekens et al., 2019). A previous publication using a subset of data from the current study showed that among the sample of Mexican university students 9.7% reported suicide ideation in the previous 12 months (12M), 0.7% reported a suicide attempt, and 5.3% reported having engaged in NSSI (Benjet et al., 2019). Researchers have underscored the importance of studying suicide ideation, previous attempts, and self-injurious behaviors as markers of severe psychological distress (Auerbach et al., 2018) and as predictors (albeit a weak association; Ribeiro et al., 2016) of suicide death (Wetherall et al., 2018; Whitlock et al., 2013). However, little research has examined suicide and self-injurious behaviors among sexual minority college students, especially from developing nations.
Minority stress theory (Meyer, 2013, 2003, 1995) postulates that members of socially stigmatized groups (e.g., sexual minority identities) may experience heightened stress due to distal (e.g., overt discrimination, violence, rejection) and/or proximal stressors (e.g., expectations of rejection, concealment of identity, internalized homophobia). This theory then proposes that this heightened stress accounts for mental illness documented among sexual minority individuals. For example, Krueger, Meyer, & Upchurch (2018) found higher perceived stress mediated the association between a sexual minority identity and depression in an adult sample from the United States. Similar for suicide-related outcomes, Bränström et al. (2020) identified various psychological factors (e.g., depression), interpersonal risk factors (e.g., discrimination), and barriers to societal integration (e.g., being unemployed) as mediators. Yet, despite evidence supporting heightened stress is pervasive across various areas of life among sexual minority populations (e.g., stress related to one’s financial situation, health, love life, family relations, health of family members; Frost et al., 2015; Hatzenbuehler, 2011; McGarrity, 2014; Rostosky et al., 2007), little research has tested perceived life stress as a predictor of suicide-related outcomes and NSSI behaviors or how these associations may differ among specific sexual orientation groups (i.e., heterosexual students reporting SGA, asexual, and unsure). This research is especially critical among Mexican college students given the heteronormative sociopolitical context. Despite existing federal anti-discrimination laws (Alterio and Ortega, 2017; Corrales, 2015), sexual minority communities in Mexico continue to experience aggressive anti-LGBTQ sentiment (Corrales, 2020), homophobic victimization (Baruch-Dominguez et al., 2016), and health disparities (Mendoza et al., 2015).
Sexual orientation has been conceptualized as a multidimensional construct comprised of sexual identity, sexual attractions, and sexual behaviors (Korchmaros et al., 2013). Sexual identity refers to one’s self-identification within a group (i.e., heterosexual, gay/lesbian, etc.) while sexual attraction refers to the “direction” towards the gender to which someone experiences sexual arousal (e.g., women, men, non-binary, or neither). For example, evidence has demonstrated that heterosexual-identified individuals may report same-gender attraction (SGA) or even identify as “mostly heterosexual” (Igartua et al., 2009; Savin-Williams and Vrangalova, 2013). Research often also includes sexual behaviors when measuring sexual orientation, yet this is typically utilized to predict risky sexual outcomes (e.g., HIV infection risk; (Beyrer et al., 2016). The present study was specifically interested in intrapersonal markers of sexual orientation such as self-identification and perceived sexual attraction, therefore sexual behaviors were not used to identify sexual orientation groups.
Empirical evidence has supported that conceptualizing sexual orientation in this manner (i.e., sexual identity and sexual attraction) has revealed health disparities among heterosexual individuals with SGA that otherwise may have been ignored (Gattis et al., 2012; Vrangalova and Savin-Williams, 2014). Furthermore, scarce research examines asexuality or those “not sure” of their identity, typically collapsing these identities with the overall sexual minority sample (Harris, 2013; Lytle et al., 2015). This is problematic given some evidence indicating higher psychological distress among those identifying as “questioning” (Sornberger et al., 2013). On the other hand, research on asexual mental health has been mixed. Although one study found asexual individuals were more likely to endorse a mood disorder compared to heterosexual men (Yule et al., 2013), another study found no mental or physical health differences between asexual and heterosexual individuals (Greaves et al., 2017).
The current study sought to advance minority stress theory (Meyer, 2013) by testing perceived life stress as a mediator of suicide ideation, attempts, and NSSI among sexual minority college students from Mexican universities. The primary aims were to test a) sexual orientation differences in 12-month suicide ideation, attempt, and NSSI, b) sexual orientation differences in reported perceived life stress, and c) perceived life stress as a mediator between sexual minority identity and relevant outcomes. To this end, mediation path models were estimated for each sexual orientation group (i.e., heterosexual with SGA, gay/lesbian, bisexual, asexual, and not sure) testing perceived life stress as a mediator between a sexual minority identity (vs identifying as heterosexual with no SGA) and suicide ideation, suicide attempt, and NSSI in the previous 12 months. It was expected that perceived life stress would partially mediate suicide ideation, attempts, and NSSI and that the indirect effect would vary across sexual orientation groups.
Method
Procedures
Participants were first-year university students from the first two cohorts of PUERTAS (University Project for Healthy Students; Benjet et al., 2019), a web-based, self-report survey conducted in nine Mexican universities as part of the World Health Organization World Mental Health International College Student initiative (WMH-ICS; Cuijpers et al., 2019). Universities were chosen based on their interest to participate and included four public and five private universities of varying sizes and geographical locations. All first-year students aged 18 or older from every university were eligible for the survey (i.e., census sampling), and were recruited through events that all first-year students attend (e.g., “health week” part of new student orientation, courses that all first-year students attend, and teacher evaluations at the end of the semester). In total, 8,076 first-year students completed the survey, representing an overall response rate (RR) of 79.3% (i.e., number of completed surveys divided by total number incoming first year students aged 18 or above). RR varied between 44.2% and 90.8% across universities. All participation was confidential and voluntary, and required informed consent. The recruitment, consent, and data collection procedures were approved by the Research Ethics Committee of the National Institute of Psychiatry in Mexico City, Mexico.
Measures
The web-based, self-report survey was developed for the WMH-ICS initiative (Cuijpers et al., 2019) and contains well-validated screeners measuring a wide range of mental health outcomes. The included areas of assessment are reviewed in the sections below.
Sociodemographic variables.
Included in this study were questions on gender (i.e., “Woman” “Man” or “Other”, however, the 21 participants who endorsed other were not included in analyses due to small sample size), age (categorized into “18–19” and “≥ 20 years” to reflect students who begin university at the normative age versus students who postpone enrollment and begin at older ages), highest parental level of education (categorized as “Secondary or less”, “High school or equivalent”, “4-year College or more”), religious affiliation (categorized as “Catholic/Christian”, “Another religion”, and “No religion”), and type of institution (i.e., private vs public).
Sexual orientation.
All participants were asked to identify their sexual identity given the options “Heterosexual”, “Gay or lesbian”, “Bisexual”, “Asexual”, “Not sure”, or “Other”. Respondents who selected “Other” (n = 86) had the chance to write in a response, yet were marked as missing and excluded from the analysis as respondents either did not seem to understand the original question or did not provide a serious answer (e.g., provided gender identity, provided a qualitative adjective instead of identity). To measure sexual attraction, participants rated their level of sexual attraction towards women and men separately, using a 5-point Likert scale ranging from “Not at All Sexually Attracted” to “Very Sexually Attracted”. Using the two sexual attraction items and self-identified gender, participants who self-identified as heterosexual (n =7,287) were categorized into “Heterosexual with no same-gender attraction (SGA)” for those who indicated no SGA and “Heterosexual with SGA” for those who indicated any level of SGA. Similar approaches to identifying heterosexual individuals with SGA have been used previously in research (see Gattis et al., 2012; Krueger et al., 2018).
Perceived life stress.
The MIDUS self-report scale of perceived stress was used to measure perceived life stress (Kessler et al., 2004), in which participants were asked to answer the question “How much stress do you currently have in each of the following areas of your life?” Students responded to this question to 8 different life areas: financial situation, own health, love life, family relationships, getting along with people, health of loved ones, other problems of loved ones, life overall. Students rated perceived stress using a 5-point Likert scale ranging from 1 (“none”) to 5 (“very severe”). The overall mean across 8 items was utilized to measure perceived life stress. The measure demonstrated an acceptable internal consistency for this sample (Cronbach’s α = .89). A factor analysis on the 8 items supported a one-factor structure with factor loadings ranging from .57 to .82.
Suicide ideation, suicide attempts, and NSSI.
A modified version of the Columbia-Suicide Severity Rating Scale (Posner et al., 2011) was used to assess suicide ideation and history of suicide attempts. This included inquiring about suicide ideation (reporting “yes” on either question “Did you ever wish you were dead or would go to sleep and never wake up?” and/or “Did you ever have thoughts of killing yourself?”) and suicide attempts (“Have you ever made a suicide attempt?”) in the past 12 months. This version of the scale has demonstrated adequate predictive validity (Ballester et al., 2019). Non-suicidal self-injurious behaviors were measured via self-report using items taken from the Self-Injurious Thoughts and Behaviors Interview (Nock et al., 2007). To measure NSSI, participants were asked if they have ever engaged in self-injury without suicidal intention during the past year (“Did you ever do something to hurt yourself on purpose, without wanting to die [e.g., cutting yourself, hitting yourself, or burning yourself]?”). This measure has shown strong psychometric properties (Nock et al., 2007).
Statistical Analysis
First, differences across sexual orientation groups were tested for all demographic and relevant variables. Then, MPLUS 8 (Muthén and Muthén, 2012) was utilized to carry out mediation path analyses testing perceived life stress as a mediator between sexual minority identity and each of the study outcomes using code provided by Stride et al. (2015). Mediations were carried out using heterosexual students reporting no SGA as the reference group, thus each sexual minority group was dummy coded where sexual minority identity = 1 and heterosexual with no SGA = 0 (e.g., bisexual = 1 and heterosexual no SGA = 0). Mediations were carried out across each sexual orientation group (i.e., heterosexual with SGA, lesbian/gay, bisexual, asexual, not sure) for each outcome (i.e., suicide ideation, suicide attempts, and NSSI) for a total of 15 mediation models. Total, direct, and indirect effects were calculated controlling for gender, age, religious preference, parental education, and type of institution (private vs. public). The significance of indirect effects was evaluated to determine whether life stress mediated the associations, while significance of direct effects was evaluated to determine the association between sexual orientation and suicide ideation, suicide attempt, and NSSI after accounting for the mediator. All mediation analyses were carried out with sampling weights based on demographic information made available by university officials to increase the representativeness of the sample.
Results
Descriptive results
Among the original sample (N = 8076), participants who selected the “Other” option for either sexual orientation (n = 86) or gender (n = 21) were excluded from the analyses (the reasons for this explained previously). Participants who did not respond to the questions on sexual attraction (utilized to construct the heterosexual students with SGA group) were also excluded, resulting in a sample of N = 7882. Among this sample, 1.8% self-identified as lesbian/gay, 3.3% as bisexual, 1.0% as asexual, and 1.4% stated not being sure of their sexual identity. Of the 92.5% that self-identified as heterosexual, 8.7% (8.0% of overall sample) reported any level of same-gender attraction. In the overall sample, 53.1% identified as a woman, the majority were ages 18–19 (79.2%), identified as Catholic/Christian (82.7%), and were attending a public university (64.0%). Chi square tests demonstrated significant differences across sexual orientation groups for each demographic variable (see Table 1). There was also a significant difference in proportions of students reporting above the 50th percentile on perceived life stress, where students identifying as “not sure” had the highest proportion and heterosexual students with no SGA with the lowest. Compared to heterosexual students with no SGA, each sexual minority group had a higher proportion of suicide ideation (range 19.4–26.1% vs 9.0%), although asexual students had only a slightly higher proportion (9.2%). Suicide attempts (range 0.9–4.0% vs 0.5%) were also higher among sexual minority groups except for asexual students (0.0%). And last, NSSI (range 5.3–18.0% vs 4.2%) were consistently higher among sexual minority groups.
Table 1.
Demographic information & differences across sexual orientation groups
| Total | Heterosexual with No SGA | Heterosexual with SGA | Gay/Lesbian | Bisexual | Asexual | Not sure | χ2 | |
|---|---|---|---|---|---|---|---|---|
| n | 7882 | 6653 | 634 | 144 | 266 | 77 | 108 | |
| Gender (%) | ||||||||
| Women | 53.1 | 52.3 | 61.3 | 35.8 | 65.8 | 42.7 | 57.7 | 58.26*** |
| Age (%) | ||||||||
| 18–19 | 79.2 | 79.6 | 78.4 | 66.7 | 76.9 | 82.7 | 79.6 | 16.76** |
| 20+ | 20.8 | 20.4 | 21.6 | 33.3 | 23.1 | 17.3 | 20.4 | |
| Religious Preference (%) | ||||||||
| Catholic/Christian | 82.7 | 85.0 | 76.1 | 69.6 | 59.2 | 73.7 | 62.3 | 208.68*** |
| Another Religion | 2.7 | 2.3 | 3.0 | 4.7 | 8.1 | 5.3 | 4.7 | |
| No Religion | 14.6 | 12.6 | 21.0 | 25.7 | 32.7 | 21.1 | 33.0 | |
| Parental Education (%) | ||||||||
| Secondary or less | 41.6 | 41.2 | 39.1 | 54.1 | 46.1 | 45.9 | 47.2 | 25.04** |
| High school or equivalent | 30.8 | 31.5 | 28.2 | 24.3 | 25.5 | 28.4 | 26.4 | |
| 4-year college or more | 27.6 | 27.3 | 32.6 | 21.6 | 28.4 | 25.7 | 26.4 | |
| Type of Institution (%) | ||||||||
| Private | 36.0 | 36.0 | 41.9 | 28.2 | 32.7 | 26.7 | 28.0 | 20.59** |
| Public | 64.0 | 64.0 | 58.1 | 71.8 | 67.3 | 73.3 | 72.0 | |
| 12M Suicide Ideation (%) | 10.8 | 9.0 | 20.1 | 20.0 | 26.1 | 9.2 | 19.4 | 168.66*** |
| 12M Suicide Attempt (%) | 0.8 | 0.5 | 1.4 | 4.0 | 4.0 | 0.0 | 0.9 | 66.33*** |
| 12M NSSI (%) | 4.2 | 11.7 | 14.8 | 18.0 | 5.3 | 9.3 | 175.62*** | |
| Perceived Life Stress (% above 50th percentile) | -- | 46.8 | 64.2 | 57.3 | 57.5 | 51.9 | 65.4 | 95.37*** |
Note.
p <.05;
p < .01;
p < .001.
SGA= Same-gender attraction; 12M = Previous twelve months; NSSI = non-suicidal self-injury. Raw sample sizes shown, all frequencies are weighted.
Mediation models: Total, Direct, and Indirect Effects
Mediation analyses were carried out for each sexual orientation group with heterosexual students with no SGA as the reference group. Table 2 shows the total, direct, and indirect effects for each mediation model across each outcome. Each sexual minority identity (except asexual) predicted increased risk for 12M suicide ideation (ORs range 2.05–3.00). Sexual minority identity also predicted increased risk for 12M suicide attempts (ORs range 2.48–8.73), and 12M NSSI (ORs range 2.92–4.18), except for asexual and students not sure of their sexual identity. In fact, no asexual students endorsed a 12M suicide attempt, and therefore no estimations were provided. Individual ORs were included in Table 2 for interpretability purposes. Perceived life stress partially mediated the association between sexual minority identity and 12M suicide ideation (range of proportion mediated 10.48% – 31.48%), 12M suicide attempts (10.48% – 31.48%), and 12M NSSI (7.69%–20.09) across each sexual orientation group except asexual students based on significant indirect effects. It is worth noting that among students not sure of their sexual identity, indirect effects were significant for 12M suicide attempts and 12M NSSI, yet the total effects were not significant. As shown in Figures 1–3, each sexual orientation group (except asexual students) reported significantly higher perceived life stress than heterosexual students with no SGA; stress then predicted suicide ideation, suicide attempt, and NSSI.
Table 2.
Total, direct, and indirect effects of sexual minority identity on suicide and self-injury outcomes mediated by perceived life stress
| 12M Suicide Ideation | Hetero SGA | Gay/Lesbian | Bisexual | Asexual | Not Sure | |
|---|---|---|---|---|---|---|
| Total Effect | B (SE) | 0.89 (0.12)*** | 0.97 (0.23)*** | 1.10 (0.17)*** | −0.05 (0.44) | 0.72 (0.28)** |
| OR (95% CI) | 2.42 (1.91, 3.07) | 2.64 (1.67, 4.17) | 3.00 (2.15, 4.17) | 0.96 (0.40, 2.27) | 2.05 (1.20, 3.51) | |
| Direct Effect | B (SE) | 0.67 (0.12)*** | 0.77 (0.22)** | 0.98 (0.16)*** | −0.10 (0.45) | 0.49 (0.27) |
| OR (95% CI) | 1.95 (1.55, 2.46) | 2.16 (1.40, 3.34) | 2.67 (1.94, 3.68) | 0.91 (0.38, 2.18) | 1.64 (0.97, 2.77) | |
| Indirect Effect | B (SE) | 0.22 (0.03)*** | 0.20 (0.06)** | 0.12 (0.04)** | 0.05 (0.08) | 0.23 (0.07)** |
| OR (95% CI | 1.24 (1.17, 1.32) | 1.22 (1.08, 1.38) | 1.12 (1.03, 1.22) | 1.05 (0.90, 1.23) | 1.25 (1.10, 1.43) | |
| 12M Suicide Attempt | Hetero SGA | Gay/Lesbian | Bisexual | Asexual | Not Sure | |
| Total Effect | B (SE) | 0.91 (0.35)** | 2.17 (0.46)*** | 1.95 (0.40)*** | +++ | 0.05 (1.04) |
| OR (95% CI) | 2.48 (1.25, 4.92) | 8.73 (3.55, 21.52) | 7.01 (3.20, 15.33) | 0.05 (0.14, 8.03) | ||
| Direct Effect | B (SE) | 0.65 (0.35) | 1.89 (0.44)*** | 1.82 (0.40)*** | +++ | −0.24 (1.04) |
| OR (95% CI) | 1.92 (0.96, 3.83) | 6.59 (2.79, 15.56) | 6.17 (2.80, 13.56) | 0.79 (0.10, 6.04) | ||
| Indirect Effect B (SE) | B (SE) | 0.26 (0.05)*** | 0.28 (0.10)** | 0.13 (0.05)* | +++ | 0.29 (0.09)** |
| OR (95% CI) | 1.29 (1.17, 1.43) | 1.33 (1.10, 1.60) | 1.14 (1.03, 1.26) | 1.34 (1.12, 1.60) | ||
| 12M NSSI | Hetero SGA | Gay/Lesbian | Bisexual | Asexual | Not Sure | |
| Total Effect | B (SE) | 1.07 (0.15)*** | 1.41 (0.26)*** | 1.43 (0.19)*** | 0.26 (0.53) | 0.63 (0.38) |
| OR (95% CI) | 2.92 (2.17, 3.92) | 4.08 (2.45, 6.77) | 4.18 (2.87, 6.08) | 1.30 (0.46, 3.64) | 1.89 (0.89, 3.99) | |
| Direct Effect | B (SE) | 0.86 (0.15)*** | 1.20 (0.25)*** | 1.32 (0.19)*** | 0.21 (0.54) | 0.40 (0.39) |
| OR (95% CI) | 2.35 (1.76, 3.15) | 3.32 (2.03, 5.42) | 3.74 (2.57, 5.45) | 1.23 (0.43, 3.56) | 1.49 (0.70, 3.19) | |
| Indirect Effect | B (SE) | 0.22 (0.03)*** | 0.21 (0.07)** | 0.11 (0.04)** | 0.05 (0.08) | 0.23 (0.07)** |
| OR (95% CI) | 1.24 (1.16, 1.32) | 1.23 (1.08, 1.40) | 1.12 (1.03, 1.21) | 1.05 (0.89, 1.23) | 1.26 (1.11, 1.44) | |
Note.
p < .05,
p < .01,
p < .001;
= Unable to estimate due to zero occurrences.
12M = 12 months; NSSI = non-suicidal self-injury; SGA = same-gender attraction; SE = standard errors; CI = confidence intervals; OR = odds ratios. Total, Direct, and Indirect Effects are unstandardized logistic coefficients from mediation path analyses where reference group was heterosexual students with no same-gender attraction; odds ratios are also shown for interpretability. Coefficients adjusted for gender, parental education, age, type of institution, religious preference. All estimations are weighted. Significant indirect effects show in bold type.
Figure 1.
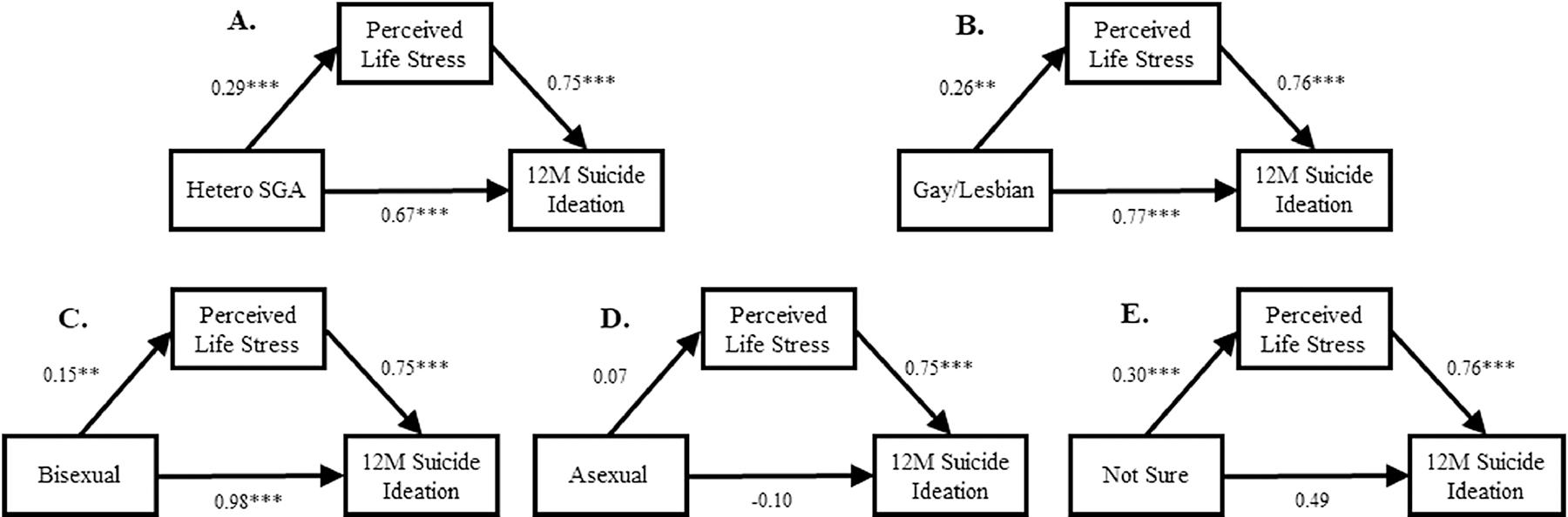
Mediation path analyses between sexual minority identity, perceived life stress, and 12M suicide ideation: coefficients from path analyses shown where reference group was heterosexual students with no same-sex attraction. Coefficient between sexual identity and 12M suicide ideation is adjusted for perceived life stress (c’). Coefficients are unstandardized and adjusted for gender, parental education, age, type of institution, religious preference. All estimations are weighted. Hetero SGA = Heterosexual with same-gender attraction; 12M = 12 months. Note. *p < .05, **p < .01, *** p < .001.
Figure 3.
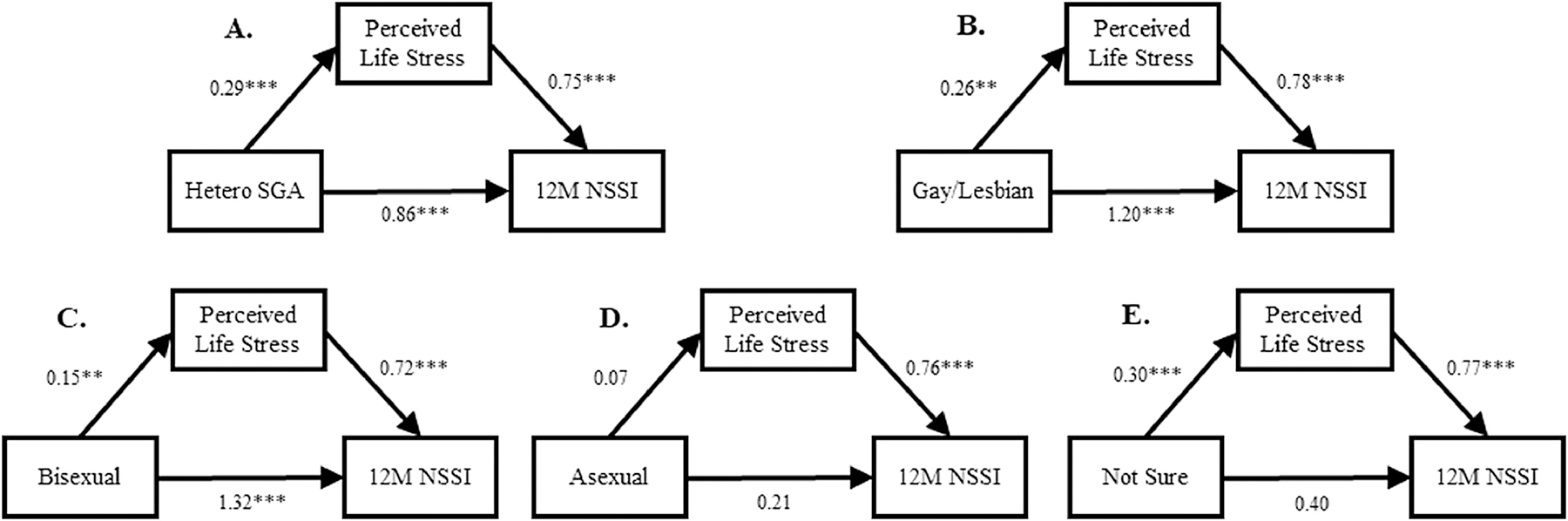
Mediation path analyses between sexual minority identity, perceived life stress, and 12M NSSI: coefficients from path analyses shown where reference group was heterosexual students with no same-sex attraction. Coefficient between sexual identity and 12M NSSI is adjusted for perceived life stress (c’). Coefficients are unstandardized and adjusted for gender, parental education, age, type of institution, religious preference. All estimations are weighted. Hetero SGA = Heterosexual with same-gender attraction; 12M = 12 months; NSSI = non-suicidal self-injury. Note. *p < .05, **p < .01, *** p < .001.
Discussion
The findings from this study advance minority stress theory (Meyer, 2013) by documenting evidence for perceived life stress as a mediator between a sexual minority identity and suicidal thoughts and behaviors and NSSI among sexual minority college students. Furthermore, it is one of the few studies documenting suicidal thoughts and behaviors and NSSI sexual minority disparities in a Latin American sample. As expected, sexual minority students reported higher perceived life stress and were at an increased risk of endorsing 12M suicide ideation, 12M suicide attempts, and 12M NSSI compared to heterosexual students reporting no SGA. Students not sure of their sexual orientation reported higher perceived life stress yet were only at increased risk of endorsing 12M suicide ideation. Asexual students were the only consistent exception, where no differences were found.
The findings corroborate previous empirical evidence among sexual minority populations (King et al., 2008; Manalastas, 2013). Consistent with the minority stress theory (Meyer, 2013, 2003), perceived life stress mediated the associations between a sexual minority identity and suicide ideation, suicide attempts, and NSSI. Although growing empirical evidence has supported disparities in suicide and self-harm outcomes among sexual minority communities, no study of which we are aware has yet tested perceived life stress as a mediator. These findings indicate that sexual minority college students experience higher stress across various life domains as compared to heterosexual students with no SGA. This suggests that minority stressors (e.g., discrimination and rejection) are not only pervasive across various life domains, but that the severity of heightened stress seems to at least partially account for suicide-related outcomes and self-injurious behaviors.
Furthermore, this study tested such mediations across various sexual identities, contributing empirical evidence for often less investigated sexual identities such as heterosexual individuals reporting SGA, asexual individuals, and those not sure of their sexual identity. This addition to the literature emphasizes the importance of scientific and clinical focus on the heterogeneity within the overall sexual minority community as different sexual orientation groups may vary in perceived stress and mental health. In terms of variations in the mediation pathways, perceived life stress was a significant mediator across each sexual orientation except among asexual students. In fact, asexual students did not differ in reports of stress, suicide outcomes, nor NSSI when compared to heterosexual students with no SGA. This finding is consistent with a previous study from New Zealand examining psychological and health differences between asexual and heterosexual individuals that also found no differences (Greaves et al., 2017). The latter study utilized a sample with 0.4% (n = 44) identifying as asexual; our study adds to the empirical body on asexual mental health utilizing a Mexican college student sample with 1.0% (n = 77) identifying as asexual. These findings may suggest that asexual students may not experience the same heightened stress reported by other sexual minority groups. In the context of minority stress theory, asexual individuals may not share the same experiences of distal and proximal stressors as other sexual minority groups. However, further conclusions about the well-being and experience of asexual individuals cannot be made as the variables in this study are not exhaustive of overall health. That is, asexual individuals may not necessarily benefit from heterosexual privilege and may experience challenges and stigma not fully explained by the minority stress theory (Chasin, 2015).
With the exception of asexual students, perceived life stress partially mediated suicide ideation, suicide attempt, and NSSI across all sexual orientation groups. These findings are congruent with extant literature indicating sexual minority individuals report higher perceived stress (Bränström, 2017; Bruce et al., 2015; Krueger et al., 2018). Our findings contribute further to the literature by testing mediation pathways of perceived stress as a contributor to increased suicide and self-injury risk. Furthermore while other research has operationalized perceived stress as cognitive/affective symptoms (Krueger et al., 2018), this study found that life stress (i.e., stress reported across various life areas) is also a predictor of suicide thoughts and behaviors and self-injury.
Limitations
The findings from this study should be interpreted considering certain limitations. Primarily, given the cross-sectional nature of the analyses, causality cannot be assumed in the mediation pathways. That is, while our analyses support that a sexual minority identity influences perceived life stress and this in turn influences suicidal and NSSI behaviors, we cannot conclude this is the causal direction between these variables (Hayes, 2018). Nonetheless, the findings align with previous theory and empirical evidence. Longitudinal research on these associations may contribute further evidence of causality. Furthermore, the self-report nature of suicidal ideation, attempt and NSSI may be biased, but Ballester et al. (2019) found good sensitivity and specificity (75.9% and 94.8% respectively) for 12M suicidal thoughts and behaviors comparing this online measure in Spanish students with clinician interviews. Another limitation of this study is that experiences of stigma and discrimination are not directly measured and tested in the mediation pathways, and life stress is likely to encompass those sources of stress as well as others. Specifically, minority stress theory identifies distal (e.g., overt discrimination) and proximal stressors (e.g., expectations of rejection), yet the perceived life stress measure was unable to distinguish minority stress from general stress. Nonetheless, this study suggests that measurement of distal and proximal stressors among sexual minority college students should encompass various life areas to better measure sexual minority stress.
Conclusions
Given the pervasiveness of stress experienced by sexual minority college students and its mediational role on suicide and self-injury, endeavors to assess and prevent suicide and NSSI among sexual minority college students might benefit from taking into consideration perceived stress across various life domains. Research on Mexican sexual minority communities may also benefit from the application of an intersectional approach (Agénor, 2020) by examining systemic inequalities related to structural (e.g., discriminatory laws, access to health services) and sociocultural factors (e.g., race/ethnicity, indigenous affiliation). Finally, future research endeavors should also examine longitudinal pathways and measure life domain-specific stigma and discrimination (e.g., family, work, relationships).
Figure 2.
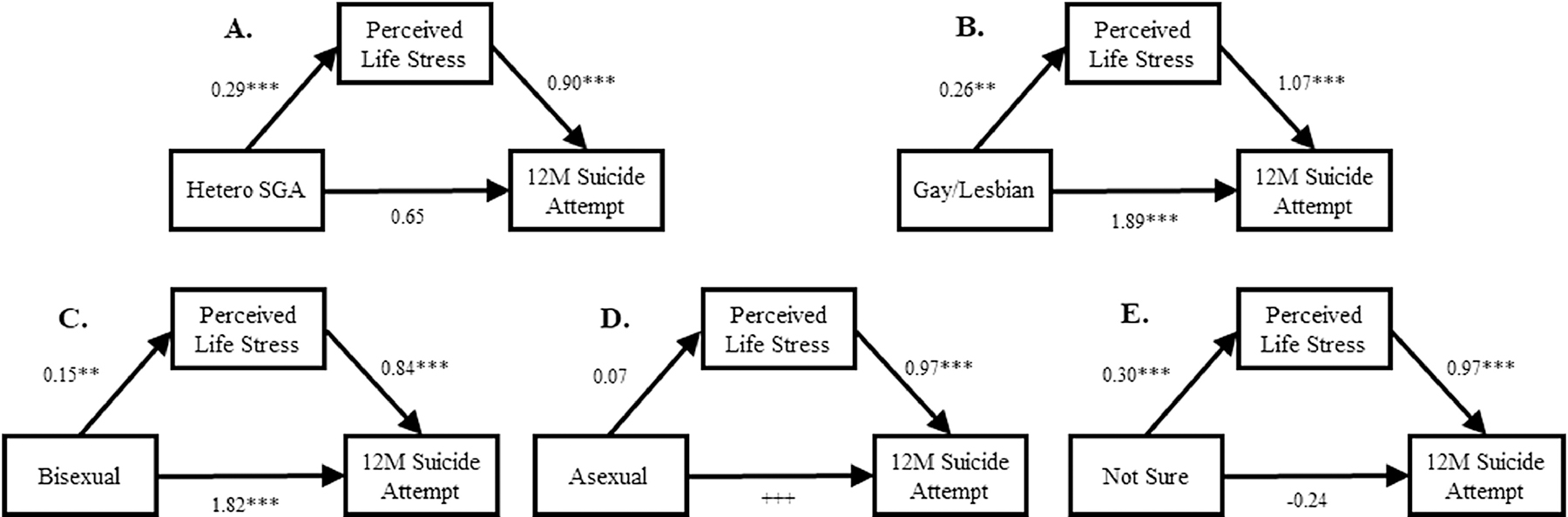
Mediation path analyses between sexual minority identity, perceived life stress, and 12M suicide attempt: coefficients from path analyses shown where reference group was heterosexual students with no same-sex attraction. Coefficient between sexual identity and 12M suicide attempt is adjusted for perceived life stress (c’). Coefficients are unstandardized and adjusted for gender, parental education, age, type of institution, religious preference. All estimations are weighted. Hetero SGA = Heterosexual with same-gender attraction; 12M = 12 months.
Note. *p < .05, **p < .01, *** p < .001.; +++ = Unable to estimate due to zero occurrences.
Highlights.
Sexual minority college students are at higher risk for suicide and self-harm.
Heterosexual students with same-gender attraction are also at a higher risk.
Perceived life stress partially mediated suicide and self-injurious behaviors.
Asexual students did not differ from heterosexuals with no same-sex attraction.
Acknowledgements
The survey was carried out in conjunction with the WHO World Mental Health International College Surveys Initiative (WHO WMH-ICS). The authors thank the WHO WMH-ICS collaborators and staff for assistance with instrumentation.
Role of the Funding Sources
Dr. Benjet received support from the (Mexican) National Council of Science and Technology (CONACyT; CB-2016-01-285548) with supplemental support from the Fundación Miguel Alemán A.C. Writing of the manuscript was supported in part by a grant from the National Institute on Minority Health and Health Disparities, T37 MD003405. The funding sources had no role in the design and conduct of the study; collection, management, analysis, interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest
Authors report no conflicts of interest.
References
- Agénor M, 2020. Future Directions for Incorporating Intersectionality Into Quantitative Population Health Research. Am. J. Public Health 110, 803–806. 10.2105/AJPH.2020.305610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alterio AM, Ortega RN, 2017. La Suprema Corte y el matrimonio igualitario en México.
- Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, Demyttenaere K, Ebert DD, Green JG, Hasking P, Lee S, Lochner C, McLafferty M, Nock MK, Petukhova MV, Pinder-Amaker S, Rosellini AJ, Sampson NA, Vilagut G, Zaslavsky AM, Kessler RC, 2018. Mental disorder comorbidity and suicidal thoughts and behaviors in the World Health Organization World Mental Health Surveys International College Student initiative. Int. J. Methods Psychiatr. Res 1–16. 10.1002/mpr.1752 [DOI] [PMC free article] [PubMed]
- Ballester L, Alayo I, Vilagut G, Almenara J, Cebrià AI, Echeburúa E, Gabilondo A, Gili M, Lagares C, Piqueras JA, Roca M, Soto-Sanz V, Blasco MJ, Castellví P, Forero CG, Bruffaerts R, Mortier P, Auerbach RP, Nock MK, Sampson N, Kessler RC, Alonso J, 2019. Accuracy of online survey assessment of mental disorders and suicidal thoughts and behaviors in Spanish university students. Results of the WHO World Mental Health-International College Student initiative. PLoS One 14, 1–21. 10.1371/journal.pone.0221529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baruch-Dominguez R, Infante-Xibille C, Saloma-Zuñiga CE, 2016. Homophobic bullying in Mexico: Results of a national survey. J. LGBT Youth 13, 18–27. 10.1080/19361653.2015.1099498 [DOI] [Google Scholar]
- Batejan KL, Jarvi SM, Swenson LP, 2015. Sexual orientation and non-suicidal self-injury: a meta-analytic review. Arch. Suicide Res 19, 131–50. 10.1080/13811118.2014.957450 [DOI] [PubMed] [Google Scholar]
- Benjet C, Gutiérrez-García RA, Abrego-Ramírez A, Borges G, Covarrubias-Díaz A, Durán MDS, González-González R, Hermosillo-de la Torre AE, Martínez-Martínez KI, Medina-Mora ME, Mejía-Zarazúa H, Pérez-Tarango G, Zavala-Berbena MA, Mortier P, 2019. Psychopathology and self-harm among incoming first-year students in six Mexican universities. Salud Publica Mex 61, 16–26. 10.21149/9158 [DOI] [PubMed] [Google Scholar]
- Beyrer C, Baral SD, Collins C, Richardson ET, Sullivan PS, Sanchez J, Trapence G, Katabira E, Kazatchkine M, Ryan O, Wirtz AL, Mayer KH, 2016. The global response to HIV in men who have sex with men. Lancet 388, 198–206. 10.1016/S0140-6736(16)30781-4 [DOI] [PubMed] [Google Scholar]
- Bränström R, 2017. Minority stress factors as mediators of sexual orientation disparities in mental health treatment: A longitudinal population-based study. J. Epidemiol. Community Health 71, 446–452. 10.1136/jech-2016-207943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bränström R, van der Star A, Pachankis JE, 2020. Untethered lives: barriers to societal integration as predictors of the sexual orientation disparity in suicidality. Soc. Psychiatry Psychiatr. Epidemiol 55, 89–99. 10.1007/s00127-019-01742-6 [DOI] [PubMed] [Google Scholar]
- Bruce D, Harper GW, Bauermeister JA, 2015. Minority stress, positive identity development, and depressive symptoms: Implications for resilience among sexual minority male youth. Psychol. Sex. Orientat. Gend. Divers 2, 287–296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chasin DC, 2015. Making Sense in and of the Asexual Community: Navigating Relationships and Identities in a Context of Resistance CJ. J. Community Appl. Soc. Psychol 25, 167–180. 10.1002/casp [DOI] [Google Scholar]
- Corrales J, 2020. The Expansion of LGBT Rights in Latin America and the Backlash. Oxford Handb. Glob. LGBT Sex. Divers. Polit 184–200. 10.1093/oxfordhb/9780190673741.013.14 [DOI]
- Corrales J, 2015. The politics of LGBT rights in Latin America and the caribbean: Research agendas. Eur. Rev. Lat. Am. Caribb. Stud 100, 53–62. 10.18352/erlacs.10126 [DOI] [Google Scholar]
- Cuijpers P, Auerbach RP, Benjet C, Bruffaerts R, Ebert D, Karyotaki E, Kessler RC, 2019. Introduction to the special issue: The WHO World Mental Health International College Student (WMH-ICS) initiative. Int. J. Methods Psychiatr. Res e1762 10.1002/mpr.1762 [DOI] [PMC free article] [PubMed]
- Frost DM, Lehavot K, Meyer IH, 2015. Minority stress and physical health among sexual minority individuals. J. Behav. Med 38, 1–8. 10.1007/s10865-013-9523-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gattis MN, Sacco P, Cunningham-Williams RM, 2012. Substance use and mental health disorders among heterosexual identified men and women who have same-sex partners or same-sex attraction: Results from the national epidemiological survey on alcohol and related conditions. Arch. Sex. Behav 41, 1185–1197. 10.1007/s10508-012-9910-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greaves LM, Barlow FK, Huang Y, Stronge S, Fraser G, Sibley CG, 2017. Asexual identity in a New Zealand national sample: Demographics, well-being, and health. Arch. Sex. Behav 46, 2417–2427. 10.1007/s10508-017-0977-6 [DOI] [PubMed] [Google Scholar]
- Haas AP, Eliason M, Mays VM, Mathy RM, Cochran SD, D’Augelli AR, Silverman MM, Fisher PW, Hughes T, Rosario M, Russell ST, Malley E, Reed J, Litts DA, Haller E, Sell RL, Remafedi G, Bradford J, Beautrais AL, Brown GK, Diamond GM, Friedman MS, Garofalo R, Turner MS, Hollibaugh A, Clayton PJ, 2011. Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations. J. Homosex 58, 10–51. 10.1080/00918369.2011.534038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris KM, 2013. Sexuality and suicidality: Matched-pairs analyses reveal unique characteristics in non-heterosexual suicidal behaviors. Arch. Sex. Behav 42, 729–737. 10.1007/s10508-013-0112-2 [DOI] [PubMed] [Google Scholar]
- Hatzenbuehler ML, 2011. The social environment and suicide attempts in lesbian, gay, and bisexual youth. Pediatrics 127, 896–903. 10.1542/peds.2010-3020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes AF, 2018. Introduction to mediation, moderation, and conditional process analysis, 2nd ed. The Guildfor Press, New York. [Google Scholar]
- Igartua K, Thombs BD, Burgos G, Montoro R, 2009. Concordance and Discrepancy in Sexual Identity, Attraction, and Behavior Among Adolescents. J. Adolesc. Heal 45, 602–608. 10.1016/j.jadohealth.2009.03.019 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Mickelson KD, Walters EE, Zhao S, Hamilton L, 2004. Age and Depression in the MIDUS Survey, in: Brim OG, Ryff CD, Kessler RC (Eds.), The John D. and Catherine T. MacArthur Foundation Series on Mental Health and Development. Studies on Successful Midlife Development. How Healthy Are We?: A National Study of Well-Being at Midlife. University of Chicago Press, pp. 227–251. [Google Scholar]
- Kiekens G, Hasking P, Claes L, Boyes M, Mortier P, Auerbach RP, Cuijpers P, Demyttenaere K, Green JG, Kessler RC, Myin-Germeys I, Nock MK, Bruffaerts R, 2019. Predicting the incidence of non-suicidal self-injury in college students. Eur. Psychiatry 59, 44–51. 10.1016/j.eurpsy.2019.04.002 [DOI] [PubMed] [Google Scholar]
- King M, Semlyen J, Tai SS, Killaspy H, Osborn D, Popelyuk D, Nazareth I, 2008. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 8, 70 10.1186/1471-244X-8-70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korchmaros JD, Powell C, Stevens S, 2013. Chasing sexual orientation: A comparison of commonly used single-indicator measures of sexual orientation. J. Homosex. 60, 596–614. 10.1080/00918369.2013.760324 [DOI] [PubMed] [Google Scholar]
- Krueger EA, Meyer IH, Upchurch DM, 2018. Sexual Orientation Group Differences in Perceived Stress and Depressive Symptoms Among Young Adults in the United States. LGBT Heal 5, 242–249. 10.1089/lgbt.2017.0228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuyper L, Bos H, 2016. Mostly Heterosexual and Lesbian / Gay Young Adults: Differences in Mental Health and Substance Use and the Role of Minority Stress. J. Sex Res 53, 731–741. 10.1080/00224499.2015.1071310 [DOI] [PubMed] [Google Scholar]
- Lytle MC, De Luca SM, Blosnich JR, Brownson C, 2015. Associations of racial/ethnic identities and religious affiliation with suicidal ideation among lesbian, gay, bisexual, and questioning individuals. J. Affect. Disord 178, 39–45. 10.1016/j.jad.2014.07.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manalastas EJ, 2013. Sexual orientation and suicide risk in the Philippines: evidence from a nationally representative sample of young Filipino men. Philipp. J. Psychol 46, 1–13. [Google Scholar]
- Marshal MP, Dietz LJ, Friedman MS, Stall R, Smith HA, McGinley J, Thoma BC, Murray PJ, D’Augelli AR, Brent DA, 2011. Suicidality and depression disparities between sexual minority and heterosexual youth: A meta-analytic review. J. Adolesc. Heal 49, 115–123. 10.1016/j.jadohealth.2011.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGarrity LA, 2014. Socioeconomic status as context for minority stress and health disparities …: EBSCOhost. Psychol. Sex. Orientaty Gend. Divers 1, Vol.1, No.4, 383–397. [Google Scholar]
- Mendoza JC, Ortiz Hernández L, Román R, Rojas A, 2015. Principales Resultados del Diagnóstico situacional de personas lesbianas, gays, bisexuales, transgénero, travestis, transexuales, intersexuales y queers (LGBTIQ) de México 2015 [Principal results of the situational diagnosis of lesbian, gay, bisexual, tra. Mexico City. [Google Scholar]
- Meyer IH, 2013. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Sex. Orientat. Gend. Divers 1, 3–26. 10.1037/2329-0382.1.S.3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH, 2003. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol. Bull 129, 674–697. 10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH, 1995. Minority Stress and Mental Health in Gay Men Author (s): Ilan H. Meyer Source: Journal of Health and Social Behavior, Mar., 1995, Vol. 36, No. 1 (Mar., 1995), Published by: American Sociological Association Stable; URL: http://www.jstor.com/ 36, 38–56. [PubMed] [Google Scholar]
- Mortier P, Auerbach RP, Alonso J, Bantjes J, Benjet C, Cuijpers P, Ebert DD, Green JG, Hasking P, Nock MK, O’Neill S, Pinder-Amaker S, Sampson NA, Vilagut G, Zaslavsky AM, Bruffaerts R, Kessler RC, Boyes M, Kiekens G, Baumeister H, Kaehlke F, Berking M, Ramírez AA, Borges G, Díaz AC, Durán MS, González RG, Gutiérrez-García RA, de la Torre AEH, Martinez Martínez KI, Medina-Mora ME, Zarazúa HM, Tarango GP, Zavala Berbena MA, O’Neill S, Bjourson T, Lochner C, Roos J, Cur HB, Taljaard L, Saal W, Stein D, Alayo I, Almenara J, Ballester L, Barbaglia G, Blasco MJ, Castellví P, Cebrià AI, Echeburúa E, Gabilondo A, García-Forero C, Iruin Á, Lagares C, Miranda-Mendizábal A, Parès-Badell O, Pérez-Vázquez MT, Piqueras JA, Roca M, Rodríguez-Marín J, Gili M, Soto-Sanz V, Vives M, 2018. Suicidal thoughts and behaviors among first-year college students: Results From the WMH-ICS project. J. Am. Acad. Child Adolesc. Psychiatry 57, 263–273.e1. 10.1016/j.jaac.2018.01.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén L, Muthén B, 2012. Mplus user’s guide (version 7.0). Mplus user’s Guid (seventh Ed. 1–850. 10.1111/j.1600-0447.2011.01711.x [DOI]
- Nock MK, Favazza AR, 2009. Understanding nonsuicidal self-injury: Origins, assessment, and treatment. American Psychological Association, Washington: 10.1037/11875-000 [DOI] [Google Scholar]
- Nock MK, Holmberg EB, Photos VI, Michel BD, 2007. Self-Injurious Thoughts and Behaviors Interview: Development, Reliability, and Validity in an Adolescent Sample. Psychol. Assess 19, 309–317. 10.1037/1040-3590.19.3.309 [DOI] [PubMed] [Google Scholar]
- Plöderl M, Sellmeier M, Fartacek C, Pichler EM, Fartacek R, Kralovec K, 2014. Explaining the Suicide Risk of Sexual Minority Individuals by Contrasting the Minority Stress Model with Suicide Models. Arch. Sex. Behav 43, 1559–1570. 10.1007/s10508-014-0268-4 [DOI] [PubMed] [Google Scholar]
- Plöderl M, Tremblay P, 2015. Mental health of sexual minorities. A systematic review. Int. Rev. Psychiatry 27, 367–385. 10.3109/09540261.2015.1083949 [DOI] [PubMed] [Google Scholar]
- Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, Currier GW, Melvin GA, Greenhill L, Shen S, Mann JJ, 2011. The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings From Three Multisite Studies With Adolescents and Adults. Am. J. Psychiatry 168, 1266–1277. 10.1176/appi.ajp.2011.10111704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ribeiro JD, Franklin JC, Fox KR, Bentley KH, Kleiman EM, Chang BP, Nock MK, 2016. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol. Med 46, 225–236. 10.1017/S0033291715001804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rostosky SS, Riggle EDB, Gray BE, Hatton RL, 2007. Minority Stress Experiences in Committed Same-Sex Couple Relationships. Prof. Psychol. Res. Pract 38, 392–400. 10.1037/0735-7028.38.4.392 [DOI] [Google Scholar]
- Savin-Williams RC, Vrangalova Z, 2013. Mostly heterosexual as a distinct sexual orientation group: A systematic review of the empirical evidence. Dev. Rev 33, 58–88. 10.1016/j.dr.2013.01.001 [DOI] [Google Scholar]
- Sornberger MJ, Smith NG, Toste JR, Heath NL, 2013. Nonsuicidal Self-Injury, Coping Strategies, and Sexual Orientation. J. Clin. Psychol 69, 571–583. 10.1002/jclp.21947 [DOI] [PubMed] [Google Scholar]
- Stride CB, Gardner S, Catley N, Thomas F, 2015. Mplus code for mediation, moderation, and moderated mediation models [WWW Document]. URL http://www.offbeat.group.shef.ac.uk/FIO/mplusmedmod.htm
- Swannell SV, Martin GE, Page A, Hasking P, St John NJ, 2014. Prevalence of nonsuicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide Life-Threatening Behav 44, 273–303. 10.1111/sltb.12070 [DOI] [PubMed] [Google Scholar]
- Vrangalova Z, Savin-Williams RC, 2014. Psychological and physical health of mostly heterosexuals: A systematic review. J. Sex Res 51, 410–445. 10.1080/00224499.2014.883589 [DOI] [PubMed] [Google Scholar]
- Wetherall K, Cleare S, Eschle S, Ferguson E, O’Connor DB, O’Carroll RE, O’Connor RC, 2018. From ideation to action: Differentiating between those who think about suicide and those who attempt suicide in a national study of young adults. J. Affect. Disord 241, 475–483. 10.1016/j.jad.2018.07.074 [DOI] [PubMed] [Google Scholar]
- Whitlock J, Muehlenkamp J, Eckenrode J, Purington A, Baral Abrams G, Barreira P, Kress V, 2013. Nonsuicidal self-injury as a gateway to suicide in young adults. J. Adolesc. Heal 52, 486–492. 10.1016/j.jadohealth.2012.09.010 [DOI] [PubMed] [Google Scholar]
- Yule MA, Brotto LA, Gorzalka BB, 2013. Mental health and interpersonal functioning in self-identified asexual men and women. Psychol. Sex 4, 136–151. 10.1080/19419899.2013.774162 [DOI] [Google Scholar]