

Abstract
Objectives
Our study aimed to investigate the association between comprehensive workstations and neck and upper‐limb pain (NUP) among office workers.
Methods
This cross‐sectional study included 307 office workers (median age, 39 years; 88% men). Workstations (presence of armrest, armrest position, number of monitors used, mouse position, mouse usage, keyboard usage, and keyboard position) were investigated in terms of 17 items and judged as “adequate” or “inadequate.” NUP was assessed using a numerical rating scale. NUP locations included the neck, shoulder, elbow, and wrist. In the statistical analysis, outcome variables were the presence of pain in each part, while explanatory variables were the number of inadequate workstations. Logistic regression analyses were conducted with adjustment for age, gender, working duration, and exercise habit.
Results
The prevalence of neck pain was 47% (n = 143), shoulder pain was 50% (n = 153), elbow pain was 7.2% (n = 22), and wrist pain was 13% (n = 40). In the adjusted model, the number of inadequate workstations had significant positive associations with elbow pain (odds ratio [OR], 1.39; 95% confidence interval [CI], 1.06.1.81) and wrist pain (OR, 1.80; 95% CI, 1.17.2.26). However, the number of inadequate workstations was not significantly associated with neck pain or shoulder pain.
Conclusions
Workstation‐related factors (presence of armrest, armrest position, mouse usage, and keyboard usage) were significantly associated with elbow and wrist pain. Our findings suggest that workstations can contribute to elbow and wrist pain in office workers.
Keywords: epidemiology, office worker, pain, workstation
1. INTRODUCTION
Computer work has recently increased due to technological developments. In developed countries, office work is among the most rapidly growing occupations; in Japan, more than 60% of the workforce are office workers. 1 Among office workers, neck and upper‐limb pain (NUP) is a prevalent health problem. The pain prevalence in the last 12 months in a population of office workers was 55% in the neck, 38% in the shoulder, 15% in the elbow, and 21% in the wrist. 2 Pain is not simply a physical problem; it increases medical costs and diminishes work productivity. 3 Therefore, it is essential to detect factors related to NUP among office workers.
With increasing computer work, the impact of workstation‐related factors (place or usage of monitor, armrest, mouse, and keyboard) on musculoskeletal problems has attracted attention. Workstations can influence muscle activities. 4 Excessive muscle activity can lead to pain. In some experimental studies, factors such as workstations had a significant impact on NUP. 5 , 6 , 7 , 8 , 9 , 10 However, these experimental studies were not conducted in real work environments. Therefore, it is difficult to conclude whether workstation‐related factors have an actual impact on NUP among office workers in the real world. In other words, a gap remains between experimental and epidemiological studies. A few epidemiological studies have investigated the relationship between individual workstations (eg, monitor and keyboard position) and NUP. 11 , 12 , 13 Nevertheless, in the real world, the workstation consists of a number of factors, for example, armrest position, distance from monitor, mouse position, and keyboard and mouse usage. Thus, we hypothesized that the greater the number of inadequate workstations, the higher the risk of NUP. In previous studies, however, the relationship between comprehensive workstations and NUP was not investigated. (“Comprehensive workstation” refers to the concept of assessing a keyboard, a mouse, a monitor, and an armrest comprehensively rather than separately.)
Therefore, in this study, we aimed to investigate the relationship between comprehensive workstations (armrest, monitor, mouse, and keyboard) and the current prevalence of NUP among office workers.
2. METHODS
2.1. Design and participants
In this cross‐sectional study, data collection was conducted at two companies from June to September 2018. The data were collected using a self‐reported questionnaire (web‐based and paper) at annual health check‐ups. One of the two companies was an electric company, while the other was the laboratories of a steel company. A total of 915 workers completed an annual health check‐up. The inclusion criteria were as follows: (i) written consent and (ii) office worker. The exclusion criteria were as follows: (i) working less than 1 year (because workers working for less than 1 year may be exposed to their workstation for an insufficient amount of time), and (ii) trauma or disease related to NUP (sprain of neck or upper limb in the past month, fracture under treatment, medial epicondylitis, bruise, whiplash injury, osteoarthritis, and other cervical spine injuries). Among the 620 participants who provided consent, the following individuals were excluded: 130 who were not office workers, 31 who worked less than a year, and 12 with trauma or disease in the neck or upper limb. After the exclusion of workers for whom data were missing on the workstation questionnaire (n = 115) or the annual health check‐up (n = 8), a total of 307 workers were included in the final analysis (response rate: 70%).
This study was approved by the ethics committee of the Kobe University School of Medicine Faculty of Health Science and conformed to the Declaration of Helsinki.
2.2. Measurement
2.2.1. Workstation
Workstations were assessed using a web‐based questionnaire distributed by e‐mail. We developed all items of the questionnaire based on the findings of previous studies that identified the relationships between workstations and muscle activities or NUP. 5 , 6 , 7 , 19 The questionnaire consisted of 17 items (5 about armrest, 5 about monitor, 3 about mouse, and 4 about keyboard). For example, the first question was “Are there armrests on your work chair?” and the answer was “Yes” or “No.” Detailed information about the workstation questionnaire is provided in Appendix 1. The workstation questionnaire was self‐rated by the participants. In order to reduce recall bias, we instructed the participants to answer the workstation questionnaire when they were in front of their own workstation.
Of the 17 items, 11 were included in the analysis that revealed the association between workstation and neck pain (neck model): 4 items about the armrest (presence, height, adjustability, and width), 5 items about the monitor (number, desktop or laptop, vertical and horizontal position, and distance from eye to monitor), 1 item about the mouse (position height), and 1 item about the keyboard (distance from near side of desk edge). In Appendix 1, these items were nos. 1, 2, 4‐11, and 17. Seven items were included in the shoulder model: 5 about the armrest (presence, height, distance from body, adjustability, and width) and 2 about the mouse (position height and distance from body). In Appendix 1, these items were nos.1‐5, 11, and 12. Six items were included in the elbow model: 4 about the armrest (presence, height, adjustability, and width), 1 about the mouse (position height), and 1 about the keyboard (position height). In Appendix 1, these items were nos. 1, 2, 4, 5, 11, and 14. Three items were included in the wrist model: 1 about the mouse (usage) and 2 about the keyboard (wrist extension and ulnar flexion). In Appendix 1, these items were nos. 13, 15, and 16.
Next, the number of inadequate workstations in each body part was counted. The score range was 0‐11 for the neck, 0‐7 for the shoulder, 0‐6 for the elbow, and 0‐3 for the wrist. A higher score indicates more inadequate workstations.
2.2.2. Neck and upper‐limb pain
NUP was measured using a numerical rating scale (NRS) 20 ranking of 0‐10. On this scale, 0 means “no pain” and 10 means “’ worst imaginable pain.” In this study, the current pain intensity in the neck, shoulder, elbow, and wrist was measured using NRS. Zero indicated “no pain” and answers 1‐10 indicated “having pain.” To indicate pain location, we used a picture of the human body (Appendix 2).
2.2.3. Other data
We collected data regarding age, gender, work duration, and trauma or disease in the neck and upper limbs from the paper‐based questionnaire. The working duration questions consisted of 3 items: “<1 year,” “>1 year but < 5 years,” and “≥5 years.” The trauma and disease questions consisted of 6 items: “no trauma or disease,” “twisted in a month,” “broken a bone and under treated,” “rheumatoid arthritis,” “fibromyalgia,” and “others.” If they answered “others,” specific names of the trauma or disease were provided.
From the annual health check‐up data, we extracted data regarding height, weight, and exercise habits. Exercise habits were measured differently between the two facilities. Therefore, regardless of the measurement method, exercising at least twice per week was defined as “active,” while exercising once or not at all per week was defined as “non‐active”. 21
2.3. Statistical analysis
Categorical variables (eg, gender, exercise habit, and working duration) are described as number and percentage. Normally distributed continuous variables are described as means and standard deviations (SDs). Non‐normally distributed continuous variables are described as medians and interquartile ranges (Table 1).
TABLE 1.
Characteristics of participants
| Age, (y) | 39 [30‐49] a |
|---|---|
| Male, n (%) | 270 (88) |
| Married n (%) | 195 (64) |
| Height, (cm) | 170.7 ± 7.2 b |
| Weight, (kg) | 65.9 ± 11.4 b |
| Work duration, n (%) | |
| 1‐5 y | 72 (23) |
| >5 y | 235 (77) |
| Exercise habit (> twice per a wk), n (%) | 146 (48) |
| Presence of pain, n (%) | |
| Neck | 143 (47) |
| Shoulder | 153 (50) |
| Elbow | 22 (7.2) |
| Wrist | 40 (13) |
Median [Interquartile range].
Mean ± Standard deviation.
The reliability of the workstation questionnaire was inspected using the test‐retest method. For the reliability test, we recruited 25 office workers from a company other than the two companies included in the main analysis. Two weeks after the first test, these workers answered the same questionnaire in the retest. Four workers were excluded because of missing data. Finally, the data of 21 workers were analyzed. Cohen's kappa (κ) between the first and second tests was calculated for each question. In a previous study, 0 < κ ≤ 0.4 indicated “low reliability,” 0.4 < κ ≤ 0.6 indicated “moderate reliability,” 0.6 < κ ≤ 0.8 indicated “high reliability,” and 0.8 ≤ κ indicated “very high reliability”. 22
Simple and multiple logistic regression was used to determine the association between workstations and NUP. The outcome variables were “no pain” or “having pain” for NUP. In the analysis, four models were performed for each of the four NUP parts (neck, shoulder, elbow, and wrist). The explanatory variables were the number of inadequate workstations. Based on previous studies, 2 , 8 , 13 confounding factors were selected (age, gender, working duration, and exercise habit). Two sensitivity analyses were performed: the first analysis to compare the characteristics of the group that answered (n = 307) and the group that did not answer (n = 115) the workstation questionnaire and another analysis after excluding questions with low reliability (Q5 and Q11). Odds ratios (OR) and 95% confidence intervals (95% CI) were calculated and the statistical significance set at P < .05. EZR ver. 1.37 was used for all statistical analyses. 23
3. RESULTS
The characteristics are listed in Table 1. The median [interquartile range] age was 39 [30‐49] years. Male participants comprised 88% (n = 270). The prevalence of neck pain was 47% (n = 143), shoulder pain in 50% (n = 153), elbow pain in 7.2% (n = 22), and wrist pain in 13% (n = 40). The number of inadequate workstations is shown in Figure 1. Of the participants, 92 (30.0%) had no pain, 125 (40.7%) had one painful site, and 90 (29.3%) had multiple painful sites, with a mean number of painful sites per person of 1.08 ± 0.94.
FIGURE 1.
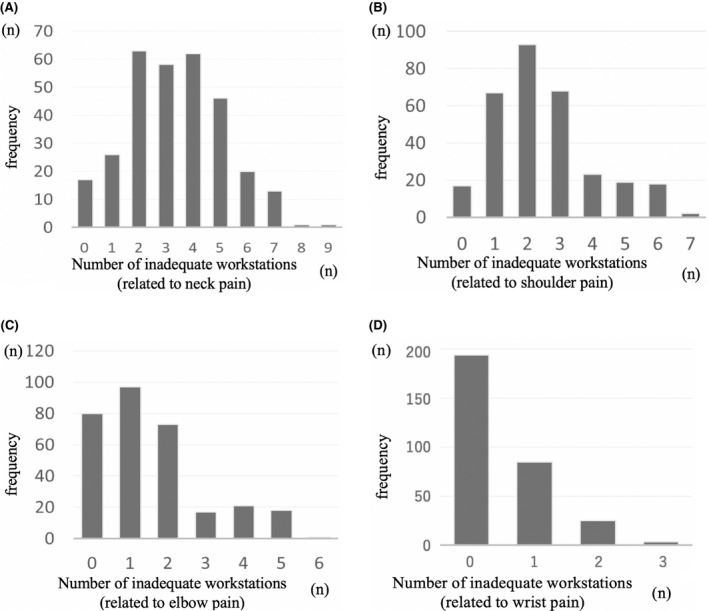
The frequency of the number of inadequate workstations
The reliabilities for most questions were medium (0.4 < κ≤ 0.6), high (0.6 < κ≤ 0.8), or very high (0.8 < κ) reliability. However, “Question 5” and “Question 11” had low reliability (κ ≤ 0.4).
Table 2 shows the associations between workstations and NUP. In the simple logistic regression models, the number of inadequate workstations had significant positive associations with shoulder pain (OR, 1.24; 95% CI, 1.07‐1.44; P = .005), elbow pain (OR, 1.39; 95% CI, 1.06.1.81; P < .001), and wrist pain (OR, 1.80; 95% CI, 1.17.2.26; P < .001). However, neck pain was not significantly associated with workstations.
TABLE 2.
The relationships between the number of inadequate workstations and NUP
| Crude model | Adjusted model | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | P | OR | 95%CI | P | |
| Neck pain | 1.09 | 0.96‐1.24 | 0.16 | 1.05 | 0.92‐1.20 | 0.45 |
| Shoulder pain | 1.24 | 1.07‐1.44 | 0.005 | 1.13 | 0.96‐1.34 | 0.13 |
| Elbow pain | 1.39 | 1.06‐1.81 | <0.001 | 1.36 | 1.01‐1.83 | 0.043 |
| Wrist pain | 1.80 | 1.17‐2.76 | <0.001 | 1.87 | 1.21‐2.88 | 0.004 |
In adjusted model, confounding factors (age, gender, working duration, and exercise habit) were adjusted.
Abbreviations: NUP, neck and upper‐limb pain, OR, odds ratio, 95%CI, 95% confidence intervals.
In the multiple logistic regression models, the number of inadequate workstations had significant positive associations with elbow pain (OR, 1.36; 95% CI, 1.01.1.83; P = .043) and wrist pain (OR, 1.87; 95% CI, 1.21.2.88; P = .004), even after adjusting for age, gender, working duration, and exercise habit. However, the number of inadequate workstations did not have significant associations with neck or shoulder pain.
Two sensitivity analyses were performed. One analysis to compare the characteristics of the group that answered (n = 307) and the group that did not answer (n = 115) the workstation questionnaire. There was no significant difference in the characteristics between both groups (data not shown). Another analysis was performed after excluding Q5 and Q11. The results of the neck and shoulder models were unchanged (non‐significant association). Moreover, the results of the elbow model were also unchanged (OR, 1,44; 95% CI, 1.07‐1.93; P = .014). Q5 and Q11 were not included in the wrist model.
4. DISCUSSION
We investigated the association between comprehensive workstations and NUP among office workers in this epidemiological study. In the adjusted model, the number of inadequate workstations was significantly associated with elbow and wrist pain but not with neck and shoulder pain.
This study found a significant association between workstations and elbow/wrist pain. Previous studies indicated that an adequate environment for armrests (having armrest, height at elbow level, adjustable, width of 5‐10 cm) [6,7,14,15], desk height (more than 5 cm from the elbow), 14 , 16 keyboard use (using neutral wrist position), 14 , 18 , 19 and mouse (not gripping) 8 affected muscle activities of the forearm. Thus, the results of this study support those of previous experimental studies. However, this is the first epidemiological study to indicate the association between workstations and elbow and wrist pain among office workers.
In addition, this study showed that workstations were not significantly associated with neck and shoulder pain. However, a previous study suggested that workstations affected neck and shoulder pain. In other words, the results of our study differed from those of previous studies, which revealed the associations between individual workstations and neck or shoulder pain (eg, horizontal monitor position and distance from keyboard to near side of desk edge were significantly associated with neck pain). 11 , 12 , 13 This may be due to other factors, including psychological factors and working time. For example, emotional exhaustion was reported to be associated with neck and shoulder pain, but not with elbow and wrist pain in office workers. 24 , 25 Conversely, mechanical factors such as wrist posture might be associated with elbow and wrist pain rather than psychological factors or working time. Therefore, these factors might explain why the workstations were significantly associated with elbow and wrist pain but not with neck and shoulder pain in this study.
This study found that several workstations (armrests, desk height, keyboard usage, and mouse) were associated with elbow and wrist pain. Some workstations can be modified more easily and rapidly (eg, wrist extension during keyboard use is modified by lean adjustment only) than other factors such as office environment (noise or light) or psychosocial factors (job demands, job control, and social support). Furthermore, once workstations are corrected, adequate environments will be sustained over the long term. On the other hand, several workstations are difficult to modify with individual effort. For example, without armrests, a chair must be replaced to create an adequate workstation. Therefore, we suggest that an individual adjusts workstations that are easy to modify, whereas an organization prepares those that are difficult to modify.
Some limitations should be considered regarding the interpretation of results. First, this was a cross‐sectional study, so it could not reveal the causal association between workstations and NUP; thus, a longitudinal study is needed in the future. Second, most of the participants were men; only 12.1% (n = 37) were women. Women generally have lower muscle strength than men. In a previous study, female muscle activities were larger than male muscle activities during computer work 5 because of the lower strength. Moreover, women are more sensitive to pain than men. 10 Therefore, the relationships between workstations and NUP might differ between men and women. To increase the generalizability of the results, future studies should investigate these associations among female office workers. Third, the workstation questionnaire was original. In Japan, there is no validated tool for assessing workstations. Hence, the validity of this workstation questionnaire is uncertain. However, all questions were based on the results of previous studies, which showed significant associations between workstations and muscle activities or NUP. Furthermore, the workstation questionnaire consisted of pictures and text, which can reduce misunderstanding. In the future, objective measurements of workstations are necessary to reduce measurement bias. Fourth, the results showed an association between workstation and presence of current pain rather than long‐term pain and pain intensity. To reduce recall bias, we measured the current pain. Moreover, the distributions of pain intensity were not normal. The NRS score of most participants was 0, and the participants decreased as the NRS scores increased. Thus, the analyses were performed in the presence of current pain. Additionally, the participants could work full‐time; therefore, the participants had a little disability despite having pain. For this reason, the disabilities were not measured.
In conclusion, this study was the first to investigate the association between several workstations and NUP among office workers. The results showed that the greater the number of inadequate workstations (armrest and keyboard and mouse usage), the higher the risk of elbow and wrist pain but not neck and shoulder pain. In the future, longitudinal studies including an adequate number of female office workers are necessary to reveal causal relationships between workstations and NUP.
DISCLOSURE
Approval of the research protocol: The study protocol was approved by the ethics committee of Kobe University School of Medicine Faculty of Health Science and conformed to the Declaration of Helsinki. Informed consent: All participants of this study gave informed consent. Registry and the Registration No. of the study/Trial: N/A. Animal studies: N/A. Conflict of interest: The authors declare no potential competing interests with respect to the study and authorship and/or publication of this article.
AUTHOR CONTRIBUTIONS
K Nakatsuka made substantial contributions to the study design, data collection, analysis, and interpretation of the results and was involved in drafting the article. Y. Tsuboi and M. Okumura made substantial contributions to the study design, data collection, analysis, and interpretation of the results and was involved in critically revising it for important intellectual content. Murata S, Isa T, Matsuda N, Kawaharada R, Uchida K, Horibe K, and Kogaki made substantial contributions to the data collection and were involved in critically revising the text for important intellectual content. Ono made substantial contributions to the study concept and design, data collection, analysis, and interpretation, and was involved in critically revising the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Supporting information
Supplementary Material
ACKNOWLEDGMENTS
We thank our participants for their time and responses to our questionnaires. We also thank the staff members, especially all authors and occupational health nurses employed by the two facilities involved in this study. Financial and material support did not exist in this study.
Nakatsuka K, Tsuboi Y, Okumura M, et al. Association between comprehensive workstation and neck and upper‐limb pain among office worker. J Occup Health. 2021;63:e12194 10.1002/1348-9585.12194
REFERENCES
- 1. Statistical Bureau of Japan / the data of national population census in 2010 / working section (p. 14) http://www.stat.go.jp/data/kokusei/2015/kekka/kihon2/pdf/gaiyou.pdf. Accessed April 28, 2019
- 2. Klussmann A, Gebhardt H, Liebers F, Rieger MA. Musculoskeletal symptoms of the upper extremities and the neck: a cross‐sectional study on prevalence and symptom‐predicting factors at visual display terminal (VDT) workstations. BMC Musculoskelet Disord. 2008;9:96 10.1186/1471-2474-9-96 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pereira MJ, Johnston V, Straker LM, et al. An investigation of self‐reported health‐related productivity loss in office workers and associations with individual and work‐related factors using an employer’s perspective. J Occup Environ Med. 2017;59(7):e138‐e144. 10.1097/JOM.0000000000001043 [DOI] [PubMed] [Google Scholar]
- 4. Szeto GPY, Straker LM, O’Sullivan PB. A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work–2: neck and shoulder kinematics. Man Ther. 2005;10(4):281‐291. 10.1016/j.math.2005.01.005 [DOI] [PubMed] [Google Scholar]
- 5. Farias Zuniga AM, Côté JN. Effects of dual monitor computer work versus laptop work on cervical muscular and proprioceptive characteristics of males and females. Hum Factors. 2017;59(4):546‐563. 10.1177/0018720816684690 [DOI] [PubMed] [Google Scholar]
- 6. Feng Y, Grooten W, Wretenberg P, Arborelius UP. Effects of arm support on shoulder and arm muscle activity during sedentary work. Ergonomics. 1997;40(8):834‐848. 10.1080/001401397187829 [DOI] [PubMed] [Google Scholar]
- 7. Hasegawa T, Kumashiro M. Effects of armrests on workload with ten‐key operation. Appl Hum Sci J Physiol Anthropol. 1998;17(4):123‐129. [DOI] [PubMed] [Google Scholar]
- 8. Huysmans MA, Eijckelhof BHW, Garza JLB, et al. Predicting forearm physical exposures during computer work using self‐reports, software‐recorded computer usage patterns, and anthropometric and workstation measurements. Ann Work Expo Health. 2017;62(1):124‐137. 10.1093/annweh/wxx092 [DOI] [PubMed] [Google Scholar]
- 9. Szeto GPY, Chan CCY, Chan SKM, Lai HY, Lau EPY. The effects of using a single display screen versus dual screens on neck‐shoulder muscle activity during computer tasks. Int J Ind Ergon. 2014;44(3):460‐465. 10.1016/j.ergon.2014.01.003 [DOI] [Google Scholar]
- 10. Taib MFM, Bahn S, Yun MH. The effect of psychosocial stress on muscle activity during computer work: comparative study between desktop computer and mobile computing products. Work Read Mass. 2016;54(3):543‐555. 10.3233/WOR-162334 [DOI] [PubMed] [Google Scholar]
- 11. Paksaichol A, Lawsirirat C, Janwantanakul P. Contribution of biopsychosocial risk factors to nonspecific neck pain in office workers: a path analysis model. J Occup Health. 2015;57(2):100‐109. 10.1539/joh.14-0124-OA [DOI] [PubMed] [Google Scholar]
- 12. Rempel DM, Krause N, Goldberg R, Benner D, Hudes M, Goldner GU. A randomised controlled trial evaluating the effects of two workstation interventions on upper body pain and incident musculoskeletal disorders among computer operators. Occup Environ Med. 2006;63(5):300‐306. 10.1136/oem.2005.022285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ye S, Jing Q, Wei C, Lu J. Risk factors of non‐specific neck pain and low back pain in computer‐using office workers in China: a cross‐sectional study. BMJ Open. 2017;7(4):e014914 10.1136/bmjopen-2016-014914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Woo EHC, White P, Lai CWK. Ergonomics standards and guidelines for computer workstation design and the impact on users’ health ‐ a review. Ergonomics. 2016;59(3):464‐475. 10.1080/00140139.2015.1076528 [DOI] [PubMed] [Google Scholar]
- 15. Jun D, Zoe M, Johnston V, O’Leary S. Physical risk factors for developing non‐specific neck pain in office workers: a systematic review and meta‐analysis. Int Arch Occup Environ Health. 2017;90(5):373‐410. 10.1007/s00420-017-1205-3 [DOI] [PubMed] [Google Scholar]
- 16. Dennerlein JT, Johnson PW. Changes in upper extremity biomechanics across different mouse positions in a computer workstation. Ergonomics. 2006;49(14):1456‐1469. 10.1080/00140130600811620 [DOI] [PubMed] [Google Scholar]
- 17. Cook CJ, Kothiyal K. Influence of mouse position on muscular activity in the neck, shoulder and arm in computer users. Appl Ergon. 1998;29(6):439‐443. [DOI] [PubMed] [Google Scholar]
- 18. Lai WKC, Chiu YT, Law WS. The deformation and longitudinal excursion of median nerve during digits movement and wrist extension. Man Ther. 2014;19(6):608‐613. 10.1016/j.math.2014.06.005 [DOI] [PubMed] [Google Scholar]
- 19. Simoneau GG, Marklin RW. Effect of computer keyboard slope and height on wrist extension angle. Hum Factors. 2001;43(2):287‐298. 10.1518/001872001775900940 [DOI] [PubMed] [Google Scholar]
- 20. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073‐1093. 10.1016/j.jpainsymman.2010.08.016 [DOI] [PubMed] [Google Scholar]
- 21. Ministry of Health, Labour, and Welfare in Japan . 2018.
- 22. Kundel HL, Polansky M. Measurement of observer agreement. Radiology. 2003;228(2):303‐308. 10.1148/radiol.2282011860 [DOI] [PubMed] [Google Scholar]
- 23. Kanda Y. Investigation of the freely available easy‐to‐use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452‐458. 10.1038/bmt.2012.244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Sadeghian F, Raei M, Ntani G, et al. Predictors of incident and persistent neck/shoulder pain in Iranian workers: a cohort study. PLoS One. 2013;8(2):e57544 10.1371/journal.pone.0057544 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Oha K, Animägi L, Pääsuke M, et al. Individual and work‐related risk factors for musculoskeletal pain: a cross‐sectional study among Estonian computer users. BMC Musculoskelet Disord. 2014;15:181 10.1186/1471-2474-15-181 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material