

Supplemental Digital Content is available in the text.
Summary:
A 48-year-old man with a protruding tumor on the parietal region had undergone treatment of alopecia using artificial synthetic fibers 2 or 3 times a year for 10 years from 30 to 39 years old. Three months before the first consultation at our hospital, he noticed a small tumor that had gradually shown bleeding and discharge, with expansion of the affected area. A diagnosis of squamous cell carcinoma (SCC) was made based on a biopsy, and we resected the tumor with a 1-cm surgical margin from the reddened area around the protruding tumor (14 × 11 cm), including the periosteum membrane. No tight adhesion was found between the periosteum and skull, so we excised the outer table of the skull of the central part (diameter: 8 cm) for a pathological analysis. A pathological study showed moderately differentiated SCC with a negative surgical margin. The whole tumor was surrounded by scar tissue with buried artificial hair implants. The second surgery was performed on the 15th postoperative day. An anterolateral thigh flap was divided into 2 flaps to fit the circle-shaped wound. This is the second report of SCC developing after artificial hair implantation in the frontal-parietal scalp. The whole protruding tumor was surrounded by scar tissue with buried artificial hair implants. Proving the direct causal relationship between inflammation of scar tissue and SCC generation is difficult; however, our pathological findings support the possibility of the harmful effects of artificial hair implants.
In the 1970s, artificial synthetic fibers were implanted into the scalp for the surgical treatment of alopecia.1,2 These fibers had advantages of low cost and no donor invasion; however, several complications were reported, such as infection, scarring, pruritus, and hair loss.3,4 The US Food and Drug Administration subsequently banned the use of prosthetic hair fibers for implantation in 1983.5 The Ministry of Health, Labour, and Welfare in Japan also warned against implanting artificial hair,6 but production and uninsured implantation procedures are still performed on a small scale. Although the generation of malignant tumors may be a rare complication, surgeons should be aware of the pitfall and consider diagnostic biopsies. We herein report a case of squamous cell carcinoma (SCC) suspected of being associated with artificial hair implantation to highlight the risks.
Case Report
A 48-year-old man was referred to us for the treatment of a protruding tumor at the parietal region. He had no remarkable medical history, no allergy to drugs, and no family history. Artificial synthetic fibers had been implanted into the parietal region of his scalp as surgical treatment for alopecia. The procedures had been performed 2 or 3 times a year for 10 years between the age of 30 and 39 years. Three months before the first consultation at our hospital, he noticed a small tumor at the implantation site. The tumor gradually showed bleeding and discharge, with expansion of the affected area. He visited another clinic, resulting in a diagnosis of SCC by a dermal punch biopsy. Preoperative computed tomography showed no metastatic findings. Magnetic resonance imaging indicated contact of the tumor with the periosteum membrane. The protruding tumor was 8 cm in diameter, corresponding to the artificial hair implantation area (Fig. 1). Considering the needs of resecting the skull bone as a vertical margin, we planned the surgical procedures as follows: if the periosteum membrane adhered tightly to the skull, then we resected the whole layer of the skull bone. On the other hand, if there was no tight adhesion, then we simply obtained a portion of the outer table as a biopsy specimen. We did not apply any intraoperative pathological analyses using frozen sections because diagnosing bony tissue is often difficult and the findings are uncertain.
Fig. 1.

Preoperative image of a 48-year-old man with a protruding tumor in the parietal region. The tumor area matched the artificial-hair–implanted zone.
We resected the tumor with a 1-cm surgical margin from the reddened area around the protruding tumor (14 × 11 cm). The periosteum membrane was resected together. No tight adhesion was found between the periosteum and skull; so we excised the outer table of the skull of the central part (diameter: 8 cm) for a pathological analysis (Fig. 2). The opened wound was covered by a Pelnac Gplus bilayer wound matrix (Gunze Co., Ltd., Ayabe, Japan) until the second surgery.
Fig. 2.

Intraoperative findings. The periosteum layer was included in tumor resection. The outer table of the skull in the central area was removed to exclude bone invasion pathologically.
A pathological study revealed moderately differentiated SCC with negative surgical margin of 0.1 mm in the vertical direction and 14 mm in the horizontal direction (Fig. 3). The additionally excised outer table of the skull showed no invasion. Although the normal hair roots at the horizontal margin area existed around normal fat tissue, the base of the implanted fibers was surrounded by scar tissue in the deeper layer. (See figure 1, Supplemental Digital Content 1, which displays the (a) normal hair root and (b) the artificial hair; http://links.lww.com/PRSGO/B565.) Therefore, the protruding tumor was considered to originate from the scar tissue.
Fig. 3.
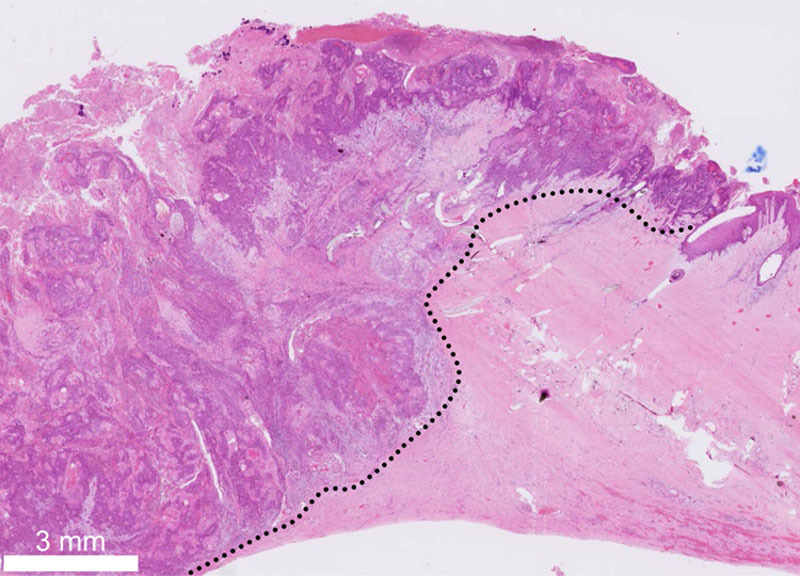
The pathological findings indicated a negative surgical margin. The black dotted line is the border of the malignant tumor. The moderately differentiated SCC was surrounded by scar tissue, including artificial hair implants.
The second surgery was performed on the 15th postoperative day. An anterolateral thigh (ALT) flap was elevated from his left thigh. The descending branch of the lateral femoral circumflex artery showed 2 main perforators; so 2 divided flaps were designed and rearranged in a circular pattern to facilitate the direct closure of the donor site. (See figure 2, Supplemental Digital Content 2, which displays the intraoperative findings; http://links.lww.com/PRSGO/B566.) The left superficial temporal artery and vein were microscopically anastomosed with the pedicle of the ALT flap. He was discharged on the 19th day after the second surgery. No recurrence or metastasis were found at 10 months after the surgeries (Fig. 4).
Fig. 4.

Postoperative findings at 10 months, with no recurrence and no metastasis. A 2-flap ALT flap was applied for scalp reconstruction.
DISCUSSION
Chiarelli et al. reported the first case of SCC developing after artificial hair implantation in the frontal-parietal scalp.7 They described multiple artificial hair implantation surgeries over 20 years that caused continuous inflammation and resulted in SCC, with histological findings of SCC infiltration to the skull and dura mater. The latency of the degeneration, affected area, and repetitive irritation history suggested Marjolin’s ulcer process, which is a rare malignancy that arises at sites of chronic non-healing wounds and scar wounds.8
Our case is the second such report and is very similar to the first in its clinical course and preoperative findings. The area around the artificial hair was filled with scar tissue. Peluso et al. performed a skin biopsy on 5 patients with severe skin complications after artificial hair transplantation, and the pathology showed the presence of hyperplastic epidermal proliferations around the artificial hair implants.9 Proving the direct causal relationship between scar tissue inflammation and SCC generation is difficult10; however, pathological findings showing that the whole protruding tumor was surrounded by scar tissue with buried artificial hair implants suggest potential harmful effects of artificial hair implants.
The patient had been worried about alopecia; so we selected an ALT flap with 2-flap design. As a secondary surgery, we are planning to replace the ALT flap with a tissue-expanded local flap after confirming the lack of long-term recurrence. Even if the central part is difficult to replace, we can select self-hair transplantation on the well-vascularized ALT flap.
CONCLUSIONS
We experienced SCC of the scalp after artificial hair implantation. The pathological findings showed that the tumor was surrounded by scar tissue with buried artificial hair implants.
Supplementary Material
Footnotes
Published online 26 January 2021.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com.
REFERENCES
- 1.Rauscher GE, DiGregorio VR. Surgical treatment of fiber-implanted scalps. Plast Reconstr Surg. 1981;67:449–452. [DOI] [PubMed] [Google Scholar]
- 2.Santiago M, Pérez-Rangel R, D’Ugo A, et al. Artificial hair fiber restoration in the treatment of scalp scars. Dermatol Surg. 2007;33:35–43; discussion 44. [DOI] [PubMed] [Google Scholar]
- 3.Lepaw MI. Complications of implantation of synthetic fibers into scalps for “hair” replacement: experience with fourteen cases. J Dermatol Surg Oncol. 1979;5:201–204. [DOI] [PubMed] [Google Scholar]
- 4.DiGregorio VR, Rauscher G. Experience with the complications of synthetic-hair implantations. Plast Reconstr Surg. 1981;68:498–504. [DOI] [PubMed] [Google Scholar]
- 5.Food and Drug Administration 21 C.F.R. Part 895, banned devices; proposal to make prosthetic hair fibers a banned device and declaration of a special effective date. Fed Regist. 1983;48:25126–25137. [Google Scholar]
- 6.Manabe M, Tsuboi R, Itami S, et al. ; Drafting Committee for the Guidelines for the Diagnosis and Treatment of Male- and Female-Pattern Hair Loss. Guidelines for the diagnosis and treatment of male-pattern and female-pattern hair loss, 2017 version. J Dermatol. 2018;45:1031–1043. [DOI] [PubMed] [Google Scholar]
- 7.Chiarelli A, Rotilio A, De Min V, et al. A case of squamous cell carcinoma of the scalp after several synthetic hair grafts. Aesthetic Plast Surg. 2012;36:649–652. [DOI] [PubMed] [Google Scholar]
- 8.Marjolin JN. Adelon NP, ed. Ulcer. In: Dictionnaire de Medicine. vol. 1828:21 Paris: Bechet; 31–50. [Google Scholar]
- 9.Peluso AM, Fanti PA, Monti M, et al. Cutaneous complications of artificial hair implantation: a pathological study. Dermatology. 1992;184:129–132. [DOI] [PubMed] [Google Scholar]
- 10.Sabin SR, Goldstein G, Rosenthal HG, et al. Aggressive squamous cell carcinoma originating as a Marjolin’s ulcer. Dermatol Surg. 2004;30(2 pt 1):229–230. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.