

Abstract
Context
Collegiate student-athletes continue competing after experiencing symptoms of a concussion. Self-report of concussion symptoms is a critical element of the recovery process. Identifying factors related to concussion disclosure can aid in encouraging self-reporting.
Objective
To use latent profile analysis to categorize and describe athletes based on factors related to concussion disclosure.
Design
Cross-sectional study.
Setting
Web-based survey.
Patients or Other Participants
A total of 2 881 (52.4% female; 65.3% in-season; 40% collision sport) student-athletes from 16 National Collegiate Athletic Association member institutions.
Main Outcome Measure(s)
Student-athlete concussion expectations, attitudes, and norms were the profile variables and reporting intentions served as the distal outcome variable. We conducted latent profile analysis using select profile variables to determine the optimal number of classes. Differences in concussion-reporting intentions by profile assignment were then examined. Lastly, the extent to which a student-athlete's sex, season status, and level of contact predicted his or her intentions to report a concussion within each profile was investigated.
Results
Five unique student-athlete profiles emerged, including 1 profile that was most risky and another that was least risky. Females had significantly higher odds of being in the least risky profile. Those participating in collision sports had significantly higher odds of being in the top 2 most risky profiles. Contact-sport and in-season athletes were less likely to be in the least risky profile.
Conclusions
With a better understanding of student-athlete profiles, athletic trainers have an opportunity to encourage concussion disclosure. Prompt disclosure would allow student-athletes to begin the return-to-play protocol in a more timely manner.
Keywords: care seeking, reporting behavior, mild traumatic brain injuries
Key Points
Athletic trainers are in a unique position to affect the concussion-disclosure intentions of student-athletes.
Student-athletes in the greatest risk profile reported more erroneous normative perceptions related to playing through concussion symptoms.
Intervention developers should consider targeting attitudes, norms, and expectations using customized strategies to target males and females in unique ways.
Concussions from contact and collision sports are recognized as a significant public health problem.1 Whereas sport participation offers a range of health, developmental, and social benefits, nearly 4 million sport-related concussions (SRCs) are reported annually in the United States.2,3 Sport-related concussions may lead to negative physical, cognitive, and emotional consequences in the short and long term4 and consequent reductions in quality of life.5 A high prevalence of health problems during the first year after SRC and beyond was noted in the Polinder et al5 review. Over the long term and compared with population norms, patients with SRC showed persistently large deficits, specifically in the physical, emotional, and social functioning domains.
Sport-related concussions in adolescent athletes have generally been underreported.6–10 Alarmingly, the 4 million US SRCs reported each year likely represent only approximately half of the concussions that actually occur. Estimates8–11 suggest that in some student-athlete populations, up to 80% of suspected SRCs go unreported. Subsequently, a student-athlete who does not report symptoms soon after injury will likely enter a return-to-play protocol late or not at all. Preventive strategies include education for athletes, coaches, athletic trainers (ATs), and parents, as well as other tactics such as equipment improvements and modifications to sport rules.12 In addition to these preventive measures, the US Zackery Lystedt law requires the immediate removal from play of a student-athlete who has sustained a potentially concussive impact. However, this law is applied only when a collision or other event has been accurately observed or the symptoms have been reported by the student-athlete. If the event is not directly observed, the role of the student-athlete becomes that much more critical.
Researchers have cited a variety of factors associated with student-athletes' disclosure of concussion symptoms. These range from expectations of what will happen if they disclose the symptoms (such as losing their spot on the team, loss of playing time, or loss of scholarship13) to normative perceptions of what others expect them to do14 to factors related to the coach–athlete relationship.15 Athletic trainers are in a unique position because they interact with student-athletes regularly in and out of season, typically in a nonthreatening environment (eg, athletic training and practice facilities). For ATs, it would be beneficial to know whether different types or profiles of student-athletes exist are associated with important factors related to SRC disclosure. Therefore, the objective of our study was to use innovative analytic methods to categorize and describe student-athletes based on factors related to concussion disclosure so that effective strategies can be implemented to positively affect SRC-disclosure intentions. First, we hypothesized that, in fact, specific clusters of student-athletes would be associated with different SRC disclosure risk and protective factors. Second, we hypothesized that these student-athlete clusters would predict intentions to disclose SRCs to different degrees.
METHODS
Research Design
We conducted a cross-sectional survey of National Collegiate Athletic Association (NCAA) student-athletes from 16 member institutions representing 34 sports. Data for this study were collected during the fall of 2016 and were part of a larger 3-year study investigating the effectiveness of an online concussion-education program.
Sample and Participants
A total of 28 NCAA member institutions expressed interest in participating. Ultimately, 16 agreed to participate and provided data for the study. The inclusion criterion was current status as an NCAA student-athlete attending an NCAA member institution. As part of the consent process, student-athletes under the age of 18 bypassed the data-collection instruments but were still given access to any subsequent programming associated with the study. Of the 4 214 student-athletes invited to participate, 2 881 (68%) completed the baseline survey. Only data from participants with complete data for all profile indicators and the outcome were included in the final analysis; incomplete data from 299 participants were removed. An initial analysis produced a spurious profile (less than 2%), so we conducted multivariate outlier analysis using Mahalanobis distance. Responses with a Mahalanobis distance χ2 significance value of <.01 were excluded from the analysis, bringing the final analytic sample to 2 350. The final sample had slightly more females (52.4%) than males (47.6%), and nearly two-thirds competed in sports that were in season at the time of the study (65.3%). Most participants were white (70.4%); African Americans accounted for 13.7%. Nearly half of the sample consisted of Division I athletes (48.8%), and the remainder of the sample was evenly split between Divisions II and III. Forty percent of participants competed in collision sports, one-fourth in contact sports, and 35% in limited-contact sports. The sample demographics are summarized in Table 1.
Table 1.
Sample Characteristics (N = 2 350)
| Demographic |
n (%) |
| Sex | |
| Male | 1 118 (47.6) |
| Female | 1 232 (52.4) |
| Division | |
| I | 1 147 (48.8) |
| II | 607 (25.8) |
| III | 596 (25.4) |
| Sport category | |
| Collision | 952 (40.5) |
| Contact | 572 (24.3) |
| Limited contact | 826 (35.1) |
| Season | |
| In | 1 534 (65.3) |
| Out | 816 (34.7) |
| Race or ethnicity | |
| White | 1 654 (70.4) |
| African American | 322 (13.7) |
| Hispanic or Latino | 162 (6.9) |
| Other | 185 (7.9) |
| Unknown | 27 (1.1) |
Procedures
At the collegiate level, ATs commonly oversee the selection and delivery of educational programming related to SRCs. Therefore, we began recruitment via an email announcement to an athletic training and sports medicine listserv. Interested individuals reached out to a research team member to receive more information about the study. Once an institution agreed to participate, an AT at the school served as the study liaison to support implementation. Each AT worked with the athletics department to provide the research team with student-athlete contact information (eg, name and email address). Then we created a user account for each athlete that would provide access to the intervention content and Web-based surveys. Invitations were emailed to all student-athletes at each participating school. Each email provided details about the study, a link to the learning management system log-in screen, unique log-in information (username and password) that provided each student-athlete with access to the consent documents, data-collection instruments, and intervention. All participants provided informed consent, and the institutional review board of the host university approved the study.
Instrument
As part of the larger study, student-athletes were invited to answer a Web-based survey immediately before and after completing a Web-based educational intervention. Responses collected during the first survey served as the data for this study. In keeping with Expectancy Theory,16 which proposes that an individual's choice of behavior is motivated by what he or she expects the results of that behavior to be, we will use the term expectancy throughout.
Profile Variables
Using an adaptation of the State-Trait Anxiety Inventory and a modified version of the Rosenbaum and Arnett Concussion Attitudes Index, as well as guidance from social norms theory, we assessed student-athletes' concussion-disclosure attitudes and expectations (ie, positive expectations, negative expectations, and reporting expectations), and normative beliefs (ie, injunctive norms, subjective norms, and descriptive norms) pertaining to concussion disclosure. The profile variables are shown in Table 2.
Table 2.
Indicator Variables and Outcome Variable Scales and Measures
| Measure (α) |
No. of Items: Scale |
Item Stemsa |
Itemsa |
| Injunctive norms (.881) | 4 items: 1 = strongly disapprove to 5 = strongly approve | For each of the following individuals, select how much you believe they approve or disapprove of YOU reporting symptoms of a concussion to a coach, athletic trainer, or a sports medicine staff member | Your head coach Your assistant coach Athletic trainer Sports medicine staff member |
| Subjective norms (.783) | 4 items: 1 = strongly disagree to 5 = strongly agree | . . . expect me to tell a coach, athletic trainer, or a sports medicine staff member when I am experiencing symptoms of a concussion | Most of my teammates Most other nonteammate student-athletes My coach My athletic trainer |
| Descriptive norms | 1 item, 0% to 100% | What percentage (%) of all National Collegiate Athletic Association student-athletes do you think would tell a coach, athletic trainer, or a sports medicine staff member if they are experiencing symptoms of a concussion. | |
| Positive expectations (.847) | 4 items: 1 = extremely unlikely to 5 = extremely likely | How likely is it that playing through symptoms of a concussion will . . . | Help me continue performing at a high level Help me achieve what is important to me Help me achieve my athletic goals Help my team succeed |
| Negative expectations (.712) | 4 items: 1 = extremely unlikely to 5 = extremely likely | How likely is it that playing through symptoms of a concussion will . . . | Increase the chances of suffering another concussion Increase the chances of suffering an additional injury Prevent me from achieving my academic goals Prevent me from maintaining my long-term health |
| Reporting expectations (.569) | 5 items: 1 = extremely unlikely to 5 = extremely likely | How likely is it that telling your coach, athletic trainer, or a sports medicine staff member about symptoms of a concussion will . . . | Make my family proud Let my teammates down Cause me to miss out on team activities Cause me to permanently lose my position on the team Help my team succeed |
| Reporting attitudes (.817) | 5 items; 1 to 7 | If you were to experience symptoms of a concussion, telling a coach, athletic trainer, or a sports medicine staff member would be . . . | Harmful to beneficial Extremely difficult to extremely easy Bad to good Unimportant to important Worthless to valuable |
| Intentions to disclose concussion symptoms (.875) | 4 items; 1 = extremely unlikely to 5 = extremely likely | If you were to experience an impact to the body or a blow to the head after which you experienced any of the symptoms of a concussion, how likely are you to tell your coach in the following situations? | During a preseason practice During a regular-season practice During a regular-season game During a championship game |
Reproduced in their original format.
Outcome Variable
Intentions to disclose concussion symptoms have been established as a reliable measure for predicting future student-athlete reporting behavior.17 The scale reflecting intentions to disclose concussion symptoms to a coach measured how likely a student-athlete was to report concussion symptoms during various scenarios. The variable is described in Table 2.
Demographic Variables
Participants were asked to indicate their sex, whether they were in season or off season at the time of survey completion, and the level of contact in their sport. The contact level was defined as a limited-contact, contact, or collision sport according to the NCAA classification of impact (https://www.ncaa.org/sites/defalt/files/SMH_Guideline_21_20160217.pdf).
Statistical Analyses
All scales were z-score transformed to account for the variations in scale measures. Latent profile analysis using the 7 profile variables was conducted using Mplus software (version 8; Muthén & Muthén, Los Angeles, CA). Latent profile analysis is a statistical approach that attempts to define classes, or profiles, of people based on shared characteristics. Using select profile variables, a series of models with an additional class added iteratively are created to determine the best profile solution based on maximum likelihood estimation criteria. To obtain the optimal solution, we considered the Akaike information criterion, Bayesian information criterion, entropy, the Lo-Mendell-Rubin likelihood ratio test, and group sizes. The optimal number of classes was determined using the Lo-Mendell-Rubin test and proportions of the sample in each class. After the optimal solution was identified, we examined the extent to which the student-athlete's sex, whether he or she was currently participating in sport, and the sport level of contact predicted their profile assignment using logistic regression. We next explored differences in the distal outcome by profile assignment using linear regression. Lastly, we measured the extent to which a student-athlete's sex, whether he or she was currently participating in sport, and the sport level of contact predicted the intention to report a concussion within each profile. We also investigated whether significant differences existed across profiles in parameter estimates of a student-athlete's sex, whether he or she was currently participating in sport, and the sport level of contact in predicting the intention to report a concussion. A P value of less than .05 was statistically significant in all analyses.
RESULTS
The results of the latent profile analysis to determine the optimal profile solution are presented in Table 3. The Akaike information criterion and Bayesian information criterion decreased as the number of profiles increased, indicating a better fit for the models with more profiles. Greater entropy also indicated a stronger model fit. Entropy was highest for the 3-profile solution (0.957); however, the entropy was >0.8 for each solution. The P values for the Lo-Mendell-Rubin test indicated that a 5-profile solution fit as well as a 4-profile solution and that a 6-profile solution did not fit as well as a 5-profile solution; additionally, 2 profiles contained less than 4% each of the sample. Based on these criteria, a 5-profile solution was considered optimal (Figure).
Table 3.
Latent Profile Analysis Fit Statistics
| No. of Profiles |
Log Likelihood |
Akaike Information Criterion |
Bayesian Information Criterion |
Entropy |
Lo-Mendell-Rubin Test |
Profiles With <5% of Sample |
| 1 | −21 612.85 | 43 253.70 | 43 334.33 | |||
| 2 | −202 97.80 | 40 639.60 | 40 766.30 | 0.829 | 0.0000 | 0 |
| 3 | −19 550.33 | 39 160.66 | 39 333.44 | 0.957 | 0.0000 | 0 |
| 4 | −19 144.26 | 38 364.52 | 38 583.37 | 0.817 | 0.0040 | 0 |
| 5 | −18 456.82 | 37 005.65 | 37 271.58 | 0.872 | 0.0002 | 1 |
| 6 | −18 127.27 | 36 362.54 | 36 673.54 | 0.886 | 0.2181 | 2 |
Figure.
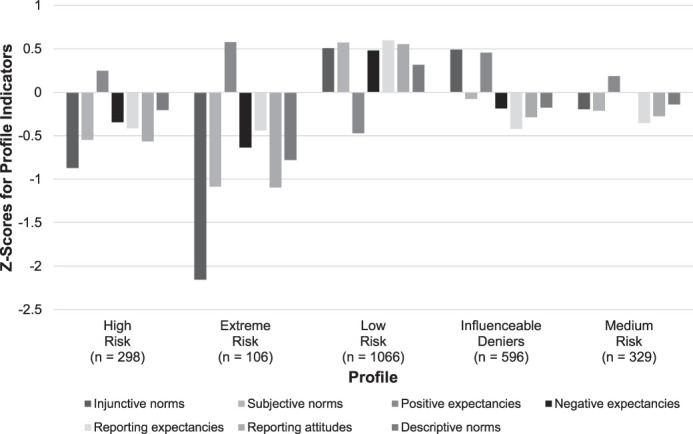
Characteristics of the latent profiles of concussion beliefs.
The z scores for each indicator within each class are supplied in Table 4. Profile 2 was the highest-risk group, with the lowest z score on all indicators and the highest score for positive expectations compared with all other profiles and was labeled the extreme-risk group. Profile 3 was the low-risk group, with the highest z scores on all indicators and the lowest score for positive expectations compared with all other profiles. Profile 1 had riskier z scores compared with profiles 3, 4, and 5 on all indicators except positive expectations. This group was labeled the high-risk group. Profile 5 displayed z scores between those of profiles 1 and 2 on all indicators and was labeled the medium-risk group. Profile 4 demonstrated characteristics similar to those of profiles 5 and 1 but had high injunctive norms that were comparable with those of the lowest-risk profile and substantially higher positive expectations than those of profiles 1, 3, and 5. This group was labeled the influenceable deniers. The mean intentions to report a concussion for each profile are provided in Table 4.
Table 4.
Indicator z Scores and Outcome Means for the 5 Profiles
| Indicator |
High Risk (n = 289) |
Extreme Risk (n = 106) |
Low Risk (n = 1 047) |
Influenceable Deniers (n = 583) |
Medium Risk (n = 325) |
| Injunctive norms | −0.871 | −2.155 | 0.508 | 0.491 | −0.197 |
| Subjective norms | −0.547 | −1.086 | 0.572 | −0.078 | −0.213 |
| Descriptive norms | −0.547 | −1.086 | 0.572 | −0.078 | −0.213 |
| Positive expectations | 0.247 | 0.577 | −0.47 | 0.455 | 0.186 |
| Negative expectations | −0.345 | −0.635 | 0.481 | −0.186 | −0.004 |
| Reporting expectations | −0.413 | −0.439 | 0.598 | −0.42 | −0.355 |
| Reporting attitudes | −0.871 | −2.155 | 0.508 | 0.491 | −0.197 |
| Outcome |
|||||
| Intention to report (standard error) | 3.46 (.05) | 3.15 (.06) | 4.34 (.03) | 3.33 (.05) | 3.43 (.05) |
Using the low-risk profile as the referent group, we added the covariates of sex, whether a sport was in season, and the level of contact to the model to assess how well these factors predicted profile membership. Females had significantly higher odds of being in the low-risk group compared with all other groups. Those participating in collision sports had significantly higher odds of being in the influenceable deniers or the medium-risk group compared with the low-risk group. Student-athletes who competed in contact sports and those whose sport was currently in season were as likely to be in the low-risk profile as any other profile. The logistic regression results predicting profile membership are given in Table 5.
Table 5.
Standardized Logistic Regression Estimates for Covariates Predicting Profile Membership Using Low Risk as the Referent Group
| Parameter |
Covariate |
Estimate |
Standard Error |
P Value |
| High risk | ||||
| Collision | −0.032 | 0.160 | .840 | |
| Contact | −0.198 | 0.192 | .302 | |
| Female | −0.643 | 0.142 | <.001 | |
| In-season | 0.028 | 0.155 | .858 | |
| Extreme risk | ||||
| Collision | −0.130 | 0.252 | .606 | |
| Contact | 0.279 | 0.278 | .315 | |
| Female | −0.885 | 0.210 | <.001 | |
| In-season | 0.118 | 0.247 | .632 | |
| Influenceable deniers | ||||
| Collision | 0.379 | 0.183 | .038 | |
| Contact | 0.266 | 0.200 | .184 | |
| Female | −0.979 | 0.157 | <.001 | |
| In-season | 0.081 | 0.160 | .615 | |
| Medium risk | ||||
| Collision | 0.533 | 0.160 | .001 | |
| Contact | 0.193 | 0.186 | .298 | |
| Female | −0.447 | 0.139 | .001 | |
| In-season | 0.044 | 0.147 | .763 |
The regression results for the covariates that predicted intention to report and the regression results within each profile appear in Table 6. The intercept for each model shows the average intention to report for males who participated in limited-contact sports and were currently out of season. In the overall regression model, sex and season were not significant predictors of intention to report concussion; however, the level of contact was a significant predictor, with those in collision sports (β = −.300, P < .001) and contact sports (β = −.162, P = .001) less likely to intend to report. Within the 5 profiles, playing a contact sport and the sport season were not significant predictors of intentions to report. Within the low-risk and influenceable deniers groups, those in collision sports (profile 3: β = −.228, P < .001; 4: β = −.369, P < .001) and females (profile 3: β = −.121, P =.017; 4: β = −.319, P = .001) were less likely to report a concussion.
Table 6.
Overall (Profile-Dependent) Linear Regression Results Predicting Intention to Report a Concussion
| Overall |
High Risk |
Extreme Risk |
Low Risk |
Influenceable Deniers |
Medium Risk |
|
| Intercept | 3.975 (0.05)a | 3.591 (0.12)a | 3.196 (0.13)a | 4.505 (0.07)a | 3.734 (0.11)a | 3.584 (0.14)a |
| Collision | −0.300 (0.04)a | −0.215 (0.13) | −0.016 (0.16) | −0.228 (0.06)a | −0.369 (0.10)a | −0.077 (0.13) |
| Contact | −0.162 (0.05)a | −0.027 (0.14) | −0.061 (0.13) | −0.101 (0.07) | −0.220 (0.12) | −0.042 (0.14) |
| Female | 0.057 (0.04) | −0.020 (0.11) | 0.139 (0.13) | −0.121 (0.05)a | −0.319 (0.10)a | 0.048 (0.10) |
| In-season | −0.076 (0.04) | −0.049 (0.11) | −0.124 (0.11) | 0.024 (0.05) | −0.076 (0.12) | −0.200 (0.11) |
P < .05.
The omnibus Wald test for each parameter estimate, using the low-risk profile as the referent group, is supplied in Table 7. A significant Wald test indicated that the parameter estimates predicting intention to report varied across profiles. The parameter estimates for sex differed significantly across profiles, indicating that the effect of sex on intention to report depended on profile assignment. Thus, the estimates of intention to report by sex within each profile were different.
Table 7.
Wald Tests of Parameter Constraints Predicting Intentions to Report Within Profiles
| Parameter |
Wald Test Value |
P Value |
| Collisiona | 4.880 | .300 |
| Contacta | 1.606 | .808 |
| Female | 10.94 | .027 |
| In-season | 4.331 | .363 |
Referent group = limited contact.
DISCUSSION
The objective of our study was to use innovative analytic methods to categorize and describe athletes based on risk and protective factors associated with concussion-disclosure intentions. This analysis allowed us to examine patterns of factors associated with concussion reporting. Identifying distinct clusters may reveal groups of student-athletes with higher-risk behavior profiles. In fact, we hypothesized that specific clusters of student-athletes would be characterized by different SRC-disclosure risks and protective factors and that these clusters would significantly predict the intention to disclose an SRC to varied degrees. Indeed, our hypotheses were confirmed: 5 clusters of student-athletes displayed different SRC-disclosure risks and protective factors, and these clusters predicted the intention to disclose an SRC to different degrees. Ultimately, this information could be used by ATs and others working closely with collegiate student-athletes to positively affect their SRC-disclosure intentions.
Higher-Risk Profiles
Based on the included factors, profile 2 was the highest-risk profile. More so than the other groups, these student-athletes reported more erroneous injunctive, subjective, and descriptive norms; fewer negative expectations related to playing through injury; and more negative reporting expectations and attitudes. Additionally, the extreme-risk profile displayed greater positive expectations for playing through a concussion. Stated more simply, student-athletes in the extreme-risk profile thought that playing through a concussion would not be too bad, others did not report concussions, and concussion reporting was neither expected nor supported by those around them. This profile was also the least likely to report a concussion in the future. Similarly, but to a lesser degree, profile 1 (high risk) was also identified as a risky profile, and the following can be applied to this group as well. These student-athletes should generate the most concern on the part of ATs. Regular and consistent communication will help to dispel erroneous norms related to concussion reporting; however, most ATs likely already provide same. It may be that ATs currently use concussion-education strategies (eg, behavioral interventions, team meetings) that specifically target student-athletes' norms and attitudes (eg, expectations of playing through injury and reporting expectations) in an effective way. Concussion-education strategies that directly target these risk and protective factors have a greater chance of shifting student-athletes' concussion-reporting intentions.17 Additionally, as the sport injury and concussion experts in their department, ATs should consider advocating for training coaches and other athletics staff on how to develop an athletic environment that supports student-athletes in seeking care for concussions and explicitly attempts to shift student-athlete normative perceptions and attitudes related to concussion reporting.
Like student-athletes in the riskiest profiles, those in profiles 4 (influenceable deniers) and 5 (medium risk) had several factors with negative z scores but to a lesser degree than athletes in profiles 1 (high risk) and 2 (extreme risk). Interestingly, the influenceable deniers had both high positive expectations of playing and high injunctive concussion norms. Essentially, student-athletes in this profile believed that playing through a concussion would have a positive outcome but that others (peers and coaches) approved of concussion reporting. It may be that when other factors do not favor concussion reporting, injunctive norms are less important. Furthermore, student-athletes may think others approve of their reporting a concussion, which based on social norms theory is a good thing; however, despite the approval of and support from others, their attitudes (expectations of playing through) ultimately drive their intention to report. Therefore, as noted previously, ATs should consider effective strategies to shift student-athletes' attitudes related to concussion reporting. Lastly, the latent profile analysis indicated that student-athletes who competed in collision sports had higher odds of being in the influenceable deniers and medium-risk groups than in the low-risk group. Considering that collision-sport athletes are at greatest risk for head injury18 and that 2 of the 4 risky profiles (influenceable deniers and medium risk) had greater proportions of collision-sport athletes, attempting to shift norms and attitudes among these athletes should be a priority for ATs. Yet collision-sport athletes were not more likely to be in the highest-risk profile, so the influenceable denier and medium-risk profiles may be unique to collision-sport athletes. Perhaps those in collision sports are more exposed to concussion safety guidelines and subsequently greater approval from and emphasis by coaches to report. This may also explain why profile 4 had high injunctive norms. Nonetheless, future researchers should consider ways to oversample this unique set of athletes.
Lower-Risk Profiles
Not only did we identify multiple risk profiles of NCAA student-athletes, but our findings also yielded a profile with significantly less risk than any of the others. With fewer erroneous norms about concussion reporting, more positive reporting attitudes, and the lowest positive expectations of playing through a concussion, profile 3 was most likely to report a future concussion. As previously noted, ATs should strongly contemplate working with the low-risk student-athletes to develop a culture that supports concussion reporting. Whereas several investigators19,20 have addressed the utility of student-athletes acting as supportive bystanders across a variety of topic areas, little attention has focused on the influence of athletes on their peers with respect to concussion reporting. Interestingly, even in the lowest-risk group, those in collision sports were still less likely to report a concussion, which indicates that something about playing a collision sport affected their intention to report a concussion. Rather than the collision sport alone, the identity or sport culture associated with the sport may affect concussion-reporting intentions. Kroshus et al21 discussed this idea of a sport ethos in terms of its relationship with biological sex and concussion reporting. Future authors may wish to take the role of sport ethos in concussion reporting into account and not rely solely on whether a sport involves collisions. Lastly, our results suggested no difference between males and females in intention to report, but in the 2 least risky profiles (profiles 3 and 4), females were significantly less likely to report than males. The intention of a male or female athlete to report appeared to depend on profile membership. Additionally, although females were much more likely to be in the lowest-risk profile than in any other profile, their attitudes, norms, and expectations seemed to have less effect on their intention to report when compared with males in similar lower-risk profiles. In other words, profiles of attitudes, norms, and expectations may affect male and female intentions to report in different ways. This is an important finding because many of the current concussion-reporting interventions that target attitudes, norms, and expectations do so in a universal manner. Instead, it may be beneficial for intervention developers to target these factors using strategies customized for target males and females in unique ways. More research is needed to further investigate this phenomenon.
Limitations
Although our unique analyses demonstrated important findings related to concussion reporting among collegiate student-athletes, they were not without limitations. First, despite the participation of more than 2 000 student-athletes, our sample was one of convenience. Institutional review board requirements (eg, protection of human participants) meant that student-athletes could opt out of the data-collection procedures that were part of a larger study investigating a behavioral intervention. Second, whereas we assessed factors internal to the student-athlete, external factors may affect concussion reporting. Future researchers, especially those using latent profile analyses, ought to consider evaluating external factors such as sport culture and coach or parental influence. Third, the self-report nature of the data is a potential limitation of this study; however, self-report remains a reliable and valid approach to concussion-related outcomes. Lastly, we surveyed concussion-reporting intentions, which have been used to predict future athlete-reporting behavior,17 yet future authors should measure both intentions and actual behaviors.
CONCLUSIONS
Athletic trainers are in a unique position to significantly affect the concussion-disclosure intentions of their student-athletes. As the health care professionals who often know their student-athletes best, ATs may be able to use relational strategies to encourage student-athletes to disclose symptoms of possible concussions so that they can be treated promptly and effectively.
ACKNOWLEDGMENTS
This study was funded by the National Collegiate Athletic Association and United States Department of Defense Mind Matters Challenge.
REFERENCES
- 1.Wiebe DJ, Comstock RD, Nance ML. Concussion research: a public health priority. Inj Prev. 2011;17(1):69–70. doi: 10.1136/ip.2010.031211. [DOI] [PubMed] [Google Scholar]
- 2.Institute of Medicine. Washington, DC: Institute of Medicine of the National Academies; 2014. Annual Report 2014. [Google Scholar]
- 3.Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375–378. doi: 10.1097/00001199-200609000-00001. [DOI] [PubMed] [Google Scholar]
- 4.Daneshvar DH, Riley DO, Nowinski CJ, Stern RA, Cantu RC. Long-term consequences: effects on normal development profile after concussion. Phys Med Rehabil Clin N Am. 2011;22(4):683–700. doi: 10.1016/j.pmr.2011.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Polinder S, Haagsma JA, van Klaveren D, Steyerberg EW, van Beeck EF. Health-related quality of life after TBI: a systematic review of study design, instruments, measurement properties, and outcome. Popul Health Metr. 2015;13:4. doi: 10.1186/s12963-015-0037-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Torres DM, Galetta KM, Phillips HW, et al. Sports-related concussion: anonymous survey of a collegiate cohort. Neurol Clin Pract. 2013;3(4):279–287. doi: 10.1212/CPJ.0b013e3182a1ba22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baugh CM, Kroshus E, Daneshvar DH, Stern RA. Perceived coach support and concussion symptom-reporting: differences between freshmen and non-freshmen college football players. J Law Med Ethics. 2014;42(3):314–322. doi: 10.1111/jlme.12148. [DOI] [PubMed] [Google Scholar]
- 8.Kroshus E, Garnett B, Hawrilenko M, Baugh CM, Calzo JP. Concussion under-reporting and pressure from coaches, teammates, fans, and parents. Soc Sci Med. 2015;134:66–75. doi: 10.1016/j.socscimed.2015.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Llewellyn T, Burdette GT, Joyner AB, Buckley TA. Concussion reporting rates at the conclusion of an intercollegiate athletic career. Clin J Sport Med. 2014;24(1):76–79. doi: 10.1097/01.jsm.0000432853.77520.3d. [DOI] [PubMed] [Google Scholar]
- 10.Kerr ZY, Register-Mihalik JK, Marshall SW, Evenson KR, Mihalik JP, Guskiewicz KM. Disclosure and non-disclosure of concussion and concussion symptoms in athletes: review and application of the socio-ecological framework. Brain Inj. 2014;28(8):1009–1021. doi: 10.3109/02699052.2014.904049. [DOI] [PubMed] [Google Scholar]
- 11.Williamson IJ, Goodman D. Converging evidence for the under-reporting of concussions in youth ice hockey. Br J Sports Med. 2006;40(2):128–132. doi: 10.1136/bjsm.2005.021832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Register-Mihalik J, Baugh C, Kroshus E, Kerr ZY. Valovich McLeod TC. A multifactorial approach to sport-related concussion prevention and education: application of the socioecological framework. J Athl Train. 2017;52(3):195–205. doi: 10.4085/1062-6050-51.12.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kerr ZY, Register-Mihalik JK, Kroshus E, Baugh CM, Marshall SW. Motivations associated with nondisclosure of self-reported concussions in former collegiate athletes. Am J Sports Med. 2016;44(1):220–225. doi: 10.1177/0363546515612082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kroshus E, Garnett BR, Baugh CM, Calzo JP. Social norms theory and concussion education. Health Educ Res. 2015;30(6):1004–1013. doi: 10.1093/her/cyv047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Milroy JJ, Hebard S, Kroshus E, Wyrick DL. Sport-related concussion reporting and coach-athlete attachment among collegiate student-athletes. J Clin Sport Psychol. 2018;12(2):268–281. [Google Scholar]
- 16.Oliver RL. Expectancy theory predictions of salesmen's performance. J Market Res. 1974;11(3):243–253. [Google Scholar]
- 17.Kroshus E, Baugh CM, Daneshvar DH, Nowinski CJ, Cantu RC. Concussion reporting intention: a valuable metric for predicting reporting behavior and evaluating concussion education. Clin J Sport Med. 2015;25(3):243–247. doi: 10.1097/JSM.0000000000000137. [DOI] [PubMed] [Google Scholar]
- 18.Baldwin GT, Breiding MJ, Comstock RD. Epidemiology of sports concussion in the United States. Handb Clin Neurol. 2018;158:63–74. doi: 10.1016/B978-0-444-63954-7.00007-0. [DOI] [PubMed] [Google Scholar]
- 19.Katz J, Moore J. Bystander education training for campus sexual assault prevention: an initial meta-analysis. Violence Vict. 2013;28(6):1054–1067. doi: 10.1891/0886-6708.vv-d-12-00113. [DOI] [PubMed] [Google Scholar]
- 20.Zinzow HM, Thompson MP, Goree J, Fulmer CB, Greene C, Watts CA. Evaluation of a college sexual violence prevention program focused on education, bystander intervention, and alcohol risk reduction. Coll Stud Aff J. 2018;36(2):110–125. [Google Scholar]
- 21.Kroshus E, Baugh CM, Stein CJ, Austin SB, Calzo JP. Concussion reporting, sex, and conformity to traditional gender norms in young adults. J Adolesc. 2017;54:110–119. doi: 10.1016/j.adolescence.2016.11.002. [DOI] [PubMed] [Google Scholar]