

Abstract
Context
Concussions are a global public health concern, and education on the importance of self-reporting may not reach all athletes to the same degree around the world.
Objective
To determine if differences were present in the concussion awareness, understanding, and -reporting behaviors of collegiate athletes' in 3 countries with varied degrees of concussion publicity.
Design
Cross-sectional survey.
Setting
Collegiate sports medicine clinics.
Patients or Other Participants
Collegiate athletes in the United States (n = 964; high publicity), Ireland (n = 302; moderate publicity), and Jordan (n = 129; low publicity). The degree of concussion publicity was categorized based on the extent of national public health awareness initiatives, care guidelines, research publications, and mass media coverage.
Main Outcome Measure(s)
Participants completed a 10- to 15-minute survey on concussion awareness, understanding, and -reporting behaviors. The main outcome measures were concussion education (awareness; 21 options; select all sources of concussion information), concussion knowledge (understanding; maximum score of 49), and diagnosed/nondisclosed concussion history (reporting behaviors; self-report yes/no items).
Results
A higher proportion of Jordanian athletes reported never having received concussion information previously (73.6%) than Irish (24.2%) or US athletes (9.4%). Knowledge differed among countries (P < .0001, η2 = .28), with US athletes displaying higher total knowledge scores (40.9 ± 4.5) than Jordanian (35.1 ± 5.6) and Irish (32.1 ± 3.5) athletes. Greater percentages of Irish and US athletes reported a history of a diagnosed concussion (31.8% and 29.6%, respectively) and history of concussion nondisclosure (25.2% and 15.5%, respectively) than Jordanian athletes (2.3% and 0.0% for history of a diagnosed concussion and history of concussion nondisclosure, respectively).
Conclusions
In the United States, where concussion publicity is high, formal legislation exists, and sports medicine resources and concussion awareness and understanding were increased. More culturally appropriate concussion initiatives are needed globally to ensure that athletes around the world can identify concussive injuries and understand the dangers of continued sport participation while concussed.
Keywords: head injuries, traumatic brain injuries, global health
Key Points
Concussion awareness, understanding, and -reporting behaviors varied among collegiate athletes in different countries.
Concussion awareness and understanding was greatest in the United States, where sports medicine resources are readily available, concussion publicity is high, and formal legislation exists.
More global initiatives are needed to ensure that all athletes, regardless of competition level or geographic location, are provided with evidence-based concussion education and sports medicine health care resources.
Concussion is a sport injury that may affect any athlete at any level. At the 5th International Conference on Concussion in Sport, sport-related concussion was defined as a traumatic brain injury caused by biomechanical forces to the head or body that results in functional, short-lived neurologic impairments.1 Concussion knowledge, perceptions, and external psychosocial factors converge to form concussion awareness, understanding, and -reporting behaviors (C-AUB). The C-AUB may vary by geographic location and be influenced by multiple levels of the socioecological framework. Researchers who use the socioecological framework2 seek to understand the interactions among intrapersonal beliefs, interpersonal relationships, community responses, and societal policy development and enforcement to identify areas in need of intervention in order to positively influence C-AUB.3 Some key socioecological aspects to consider include access to sports medicine health care providers, sport values, team camaraderie, socioeconomic status, and racial or ethnic identity. Ultimately, how athletes view and respond to concussive injuries may affect their choice to disclose the injury and adhere to a management plan,4 which can be further explained by the theory of planned behavior.5 To date, little is known about how these factors differ globally, and an assessment of C-AUB from this perspective is needed to develop successful education and prevention initiatives that meet the needs of different sport populations.
It is important to consider how C-AUB translate and adapt as concussion initiatives continue to increase worldwide. Three countries with different degrees of concussion publicity are the United States (high), Ireland (moderate), and Jordan (low). In the United States, 70% of public secondary schools have access to a sports medicine health care professional,6 and annual concussion education for secondary school athletes has been mandatory across the United States since 2014 due to state concussion legislation.7 Ireland has no streamlined concussion education for collegiate athletes, and guidelines vary by sport. Additionally, Irish collegiate athletes do not typically have sports medicine coverage at all events, as is the case in the United States, but they may have access to a certified athletic therapist or physiotherapist for concussion management. In Jordan and the Middle East, however, mandatory education for athletes and legal mandates on education regarding concussion in sport are absent, and the availability of sports medicine health care providers is limited. In addition, Jordan has not developed any concussion guidelines for collegiate sports. The variations in concussion awareness and access to sports medicine health care from country to country may result in cultural C-AUB differences.
Differences in sport culture from country to country may also be noteworthy when considering C-AUB. In the United States, approximately 5.7% of the 8 million students who play sports in high school go on to compete in college.8 In recent years, sport specialization with high-volume training has become more prevalent in the United States as adolescent athletes competed for collegiate sport scholarships.9,10 This has resulted in overuse injuries and psychological stress.9–12 Although such scholarships are available in Ireland and Jordan, participation in collegiate sports may not be as financially driven as it is in the United States, as fees to attend higher education institutions in Ireland and Jordan are far less. With smaller populations, Ireland and Jordan have fewer collegiate athletes, and in Ireland, many participate on a more recreational level.13 Youth sport development in these countries may not be at the same level as in the United States, and although sport opportunities are available to both sexes equally in Jordan, girls and women do not participate in sport as frequently as do boys and men.
Injury self-reporting decisions may be affected by C-AUB. In most instances, concussion identification depends on athletes' willingness to immediately remove themselves from activity and report their injury, as many common concussion symptoms are subjective in nature (eg, headache, dizziness, confusion). Despite the tremendous increase in concussion awareness and resources, numerous researchers14–16 have concluded that approximately 50% of collegiate athletes in North America did not report a suspected concussion. Although not specific to collegiate athletics, previous authors have shown that between 18.5% and 25% of Irish adults reported not disclosing a suspected concussion in club rugby,17,18 Gaelic Games,19,20 and horse racing.21 Little is known about concussion-disclosure rates in Jordan and the Middle East, but in 1 study, investigators22 found that the concussion incidence was lower in the Qatari professional football (soccer) league than in European football leagues. They concluded that this lower incidence of concussion might be attributed to Qatari athletes failing to recognize the significance of their symptoms or purposely concealing a concussion to avoid missing a match.22 More information is needed to determine the degree of variance in and rationale for concussion nondisclosure among countries in order to identify potential C-AUB differences.
Concussions occur in all arenas of sport, but concussion awareness may not reach all athletes to the same degree globally. At a minimum, athletes must be able to identify when a possible concussive injury has occurred and understand the dangers associated with continued sport participation while concussed. Barriers to the dissemination of concussion information and postinjury management may exist in some geographic locations that lack health care resources. Although international initiatives and consensus documents have established universal core concussion-care guidelines, no researchers have compared how this information has translated across different countries. From a global perspective, more evidence-based concussion awareness is needed to identify potential health disparities and cultural differences among countries. This information is pertinent to developing ways to close the gaps in health care access and tailoring concussion initiatives to meet the needs of athletes from diverse backgrounds. Therefore, the purpose of our study was to determine if difference existed in collegiate athletes' C-AUB among countries with varying degrees of concussion publicity (United States [high], Ireland [moderate], Jordan [low]). We also aimed to examine how sex and type of sport risk affected C-AUB.
METHODS
Research Design
We conducted a cross-sectional survey to determine differences in C-AUB among collegiate athletes in the United States, Ireland, and Jordan. The independent variable was country of sport participation categorized as having high, moderate, or low concussion publicity. We classified the degree of concussion publicity based on the extent of national public health awareness initiatives, care guidelines, research publications, and mass media coverage in each country. The dependent variables that represented C-AUB were sources of concussion information, concussion knowledge, external pressure to participate after a head impact, and concussion-reporting behaviors. We collected data from September 2017 to May 2018.
Participants
Study participants were a convenience sample of male and female collegiate athletes over the age of 18 years from the United States (high concussion publicity), Ireland (moderate concussion publicity), and Jordan (low concussion publicity). We defined a collegiate athlete as an individual who competed in a sport directly affiliated with and supported by his or her institution. This investigation included sports with both high (eg, American football, rugby, soccer) and low (eg, tennis, track and field) risks of concussion. A full list of included sports from each country appears in Table 1. To decrease response bias, we excluded participants who had sustained a concussive injury within the previous 3 months (United States = 28, Ireland = 4, Jordan = 1), experienced lingering concussion symptoms, or were undergoing treatment for a concussion they had incurred more than 3 months previously (United States = 17, Ireland = 3, Jordan = 0). The resulting study sample comprised 1395 collegiate athletes (United States = 964, Ireland = 302, Jordan = 129).
Table 1.
Included Collegiate Sports by Country
| Country | ||
| United States |
Ireland |
Jordan |
| American football Baseball and softball Basketball Cross-country Field hockey Golf Ice hockey Lacrosse Rowing Soccer Swimming and diving Tennis Track and field Volleyball Water polo Wrestling | Basketball Boxing Camogie Canoeing Cycling Field hockey Gaelic football Ladies' Gaelic football Gaelic handball Hurling Mixed martial arts Rowing Rugby Soccer Swimming and diving Tae kwon do Track and field Ultimate Frisbee Volleyball | Basketball Field hockey Golf Ice hockey Soccer Swimming and diving Tennis Volleyball Water polo Wrestling |
Measures
To assess elements of C-AUB, we used a 1-time, 70-item survey that took approximately 10 to 15 minutes to complete (Supplementary Materials 1, 2, and 3 [see Supplemental Materials 1–3, available online at http://dx.doi.org/10.4085/1062-6050-0575-19.S1]). Multiple sections captured information related to participant demographics, collegiate sport participation, a history of diagnosed concussion, emotional perception of injury, concussion knowledge, external pressure to participate after a head impact, concussion nondisclosure and -reporting behaviors, and concussion education. Multiple concussion researchers and clinicians assessed the US (n = 3), Irish (n = 2), and Jordanian (n = 5) surveys for content validity. The US survey was pilot tested on 9 healthy undergraduate college students to determine readability and comprehensibility; no resultant changes were made. The Irish and Jordanian surveys were then adapted from the US survey. The Irish survey was pilot tested on 10 healthy college students. For the Jordanian athletes, the survey was translated into Arabic based on the World Health Organization guidelines23 for forward and backward translation and pilot tested on 10 bilingual athletes and therapists. Pilot testing indicated that the survey was clear and the questions were easy to understand and follow.
Sources of concussion information were determined by asking participants to select from a list all sources from which they had ever acquired concussion information. Five concussion researchers from the United States compiled the list of 20 potential sources of concussion information. Level of concussion knowledge (maximum score = 49) was determined using a previously established questionnaire that included items on symptom recognition, complications related to multiple concussions, and potential repercussions of continuing to participate in sport while concussed.24 We made minor adaptations to the original instrument by adding pertinent concussion symptoms (eg, fogginess) found on the Post-Concussion Symptom Scale.25 We also calculated a separate symptom-knowledge score (maximum score = 34; 20 true concussion symptoms, 14 distractor symptoms) using the symptom items from the knowledge scale as symptom recognition is a key element of concussion identification. For the concussion total-knowledge and symptom-knowledge scores, higher scores indicated greater knowledge. The level of external pressure from coaches, teammates, family, and fans to continue participating in sport after a head impact during collegiate or high school sport participation was measured using four 7-point Likert-scale (1 = strongly disagree to 7 = strongly agree) items.14 A history of diagnosed concussion was assessed by asking participants if they had ever been diagnosed with (a) concussion(s) by a health care professional, and, if so, how many. Lastly, concussion nondisclosure and -reporting behaviors were assessed by asking participants if they had ever sustained a possible concussion that they did not report to anyone, and, if so, to select all the reasons for not disclosing from a list of 17 possible options (eg, not wanting to miss playing time, not wanting to appear weak to teammates or coaches).26,27
Data Collection
Before data collection, we obtained research ethics approval at each participating institution in the United States, Ireland, and Jordan. In the United States, the research team recruited 6 National Collegiate Athletic Association (NCAA) institutions (Division I = 4, Division II = 2) to participate by contacting their head athletic trainers. The athletic trainers then worked with each institution's sports medicine staff to coordinate data-collection sessions during which the participants voluntarily completed the study survey via paper and pencil or on a smart device using Qualtrics software (Provo, UT). We collected data in Ireland using SurveyMonkey (San Mateo, CA) links distributed via social media, emails to Irish third-level education institution sports officers, and word of mouth. The survey was also available in a paper format on request. We collected data in Jordan using a paper format and recruited participants via the athletic departments of universities. A researcher attended practices to distribute and collect the surveys. Trained research assistants entered the US data into Qualtrics and the Irish data into SurveyMonkey, which we then exported to SPSS (version 25.0; IBM Corp, Armonk, NY) for the statistical analyses. We entered the Jordanian data directly into an SPSS file.
Statistical Analyses
We computed frequencies and proportions for participant demographics, history of previous diagnosed concussion and suspected concussion nondisclosure, concussion education sources, previous pressure to play after a head impact, and reasons for not reporting a suspected concussion. We used 3-way analysis of variance to examine the differences between (1) country (United States versus Ireland versus Jordan), (2) sex (male versus female), and (3) concussion risk in sport (high versus low) for the total-knowledge score, symptom-knowledge score, and pressure-to-play items. Because the Jordanian athletes did not complete the pressure-to-play items, we excluded this sample from the 3-way analysis of variance. All analyses were carried out using SPSS, and P < .05 was considered statistically significant. Effect sizes were calculated using partial ηp2 and classified as small (0.01), medium (0.06), or large (0.138).28
RESULTS
Participants
The classification of participants with respect to the country, sex, and high or low sporting concussion risk is displayed in Table 2. A greater percentage of Irish and US athletes reported a previously diagnosed concussion (31.8%, n = 96; 29.6%, n = 285, respectively) and a history of nondisclosure after a suspected concussion (25.2%, n = 76; 15.5%, n = 149, respectively), than Jordanian athletes (previously diagnosed concussion: 2.3%, n = 3; nondisclosure after a suspected concussion: 0.0%, n = 0/129; Figure).
Table 2.
Participant Demographics
| Country |
Participants, No. |
% (No.) |
|||
| Sex |
Concussion Risk of Sport Participationa |
||||
| Males |
Females |
High |
Low |
||
| United States | 964 | 62.3 (601) | 37.7 (363) | 74.7 (717) | 25.3 (243) |
| Ireland | 302 | 48.0 (145) | 52.0 (157) | 88.7 (268) | 11.3 (34) |
| Jordan | 129 | 73.6 (95) | 26.4 (34) | 64.3 (83) | 35.7 (46) |
Four participants did not answer this question.
Figure.
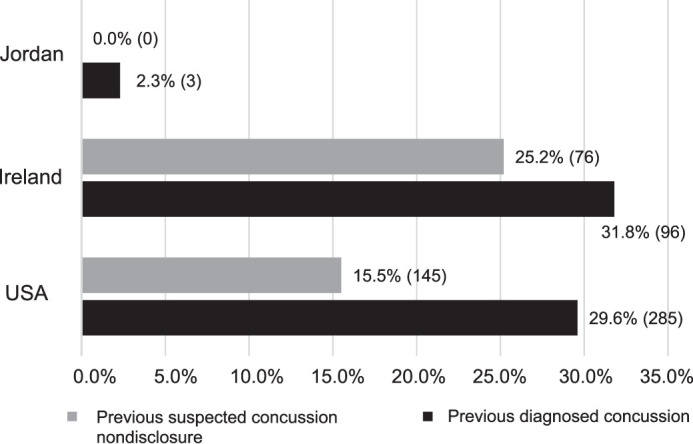
History of previously diagnosed concussion and concussion nondisclosure by country.
Concussion Sources of Information and Knowledge (Awareness and Understanding)
Jordanian athletes predominantly reported never having received concussion information from any source (73.6%, n = 95), a far higher value than reported by Irish (24.2%, n = 73) or US athletes (9.4%, n = 91). In contrast, more US athletes received concussion information from an allied health care professional (73.2%, n = 706) than Irish (34.8%, n = 105) and Jordanian (0.8%, n = 10) athletes. Irish athletes most frequently received concussion information from movies and books (36.1%, n = 109), and 18.5% (n = 56) received concussion information from a university lecturer (eg, leaflets, flyers, or educational talks). The full list of concussion sources of information is available in Table 3.
Table 3.
Concussion Information Sources in US, Irish, and Jordanian Collegiate Athletes
| Concussion Information Sources |
Country, % (No.) |
||
| United States (n = 700) |
Ireland (n = 302) |
Jordan (n = 129) |
|
| Never received concussion information from any source | 9.4 (91) | 24.2 (73) | 73.6 (95) |
| Family member | 41.1 (396) | 9.3 (28) | 1.6 (2) |
| School-based professional (eg, school nurse, teacher) | 68.4 (659) | 8.3 (25) | 1.6 (2) |
| Coach or manager | 56.3 (543) | 29.1 (88) | 2.3 (3) |
| Referee | 4.6 (44) | 4.0 (12) | 0.8 (1) |
| Recreational league officials or mandated paperwork | 9.3 (90) | NA | NA |
| Recreational sporting association concussion education | NA | 21.5 (65) | 0.0 |
| High school sport associations | 28.0 (270) | NA | 0.8 (1) |
| Collegiate sport associations (eg, National Collegiate Athletic Association) | 46.2 (445) | NA | 0.0 |
| Youth sport state concussion laws | 5.7 (55) | NA | NA |
| Allied or other health care professional | 73.2 (706) | 34.8 (105) | 0.8 (1) |
| Physician | 44.7 (431) | 25.5 (77) | 2.3 (3) |
| Neuropsychologist or psychologist | 5.6 (54) | 0.7 (2) | 0.0 |
| Nurse | 12.3 (119) | 3.3 (10) | 0.0 |
| Movies or books | 34.0 (328) | 36.1 (109) | 8.5 (11) |
| Social media | 33.8 (326) | 31.5 (95) | 19.4 (25) |
| Sports news outlets (eg, online, TV, radio, newspaper) | 31.8 (307) | 19.9 (65) | 12.4 (16) |
| General news outlets (eg, online, TV, radio, newspaper) | 19.4 (187) | 11.9 (36) | 3.1 (4) |
| Online medical sources | 21.4 (206) | 14.9 (45) | 2.3 (3) |
| Other online sources (eg, Wikipedia or Google searches, blogs) | 14.6 (141) | 11.9 (36) | 0.0 |
Abbreviation: NA, not applicable for this sample.
We did not identify interactions or main effects for sport risk on the total-knowledge score and symptom-knowledge score. A main effect was present for country (P < .001) with a large effect size (ηp2 = 0.28). Post hoc analysis demonstrated that US athletes had significantly higher total-knowledge scores (40.9 ± 4.5) and symptom-knowledge scores (27.3 ± 3.9) than Jordanian (35.1 ± 5.6 and 25.2 ± 3.4, respectively) and Irish (32.1 ± 3.5 and 20.1 ± 2.5, respectively) athletes. Irish athletes displayed lower scores than both US and Jordanian athletes (P < .001). Across the sample, women demonstrated higher total-knowledge (39.2 ± 5.7) and symptom-knowledge (26.1 ± 4.7) scores than men (37.6 ± 5.8 and 25.1 ± 4.6, respectively), with small effect sizes (P < .001, ηp2 = 0.02; P < .001, ηp2 = 0.01, respectively).
Pressure to Play After a Head Impact (Behaviors)
We found no interaction effects or main effects for sex or concussion sport risk for pressure to play in college or high school. However, Irish athletes reported greater perceived pressure to return to sport after a head injury in college (3.5 ± 1.9, 59.3%, n = 179) and high school (3.5 ± 1.7, 54.0%, n = 163, P < .001) than US athletes (2.4 ± 1.5, 29.9%, n = 295; 2.6 ± 1.5, 23.9%, n = 187, respectively); effect sizes were small (ηp2 = 0.05 and ηp2 = 0.03, respectively) for both.
Concussion Nondisclosure (Behaviors)
The US athletes primarily did not report a suspected concussion because they did not want to miss a game (20.0%, n = 193) or lose playing time (19.7%, n = 190) or, at the time, did not think it was a concussion (15.7%, n = 151; Table 4). Similarly, most Irish athletes did not report because they did not think it was a concussion (19.9%, n = 60), did not want to miss a game (14.6%, n = 44), or did not want to lose playing time (13.9%, n = 42). Jordanian athletes did not complete this section as none reported that they did not disclose a suspected concussion.
Table 4.
Reasons for Not Reporting a Suspected Concussion Among US and Irish Collegiate Athletes
| Reasons for Not Reporting a Suspected Concussion |
Country, % (No.) |
|
| United States (n = 964) |
Ireland (n = 302) |
|
| Did not want to miss a game | 20.0 (193) | 14.6 (44) |
| Did not want to lose playing time | 19.7 (190) | 13.9 (42) |
| Did not think it was a concussion at the time | 15.7 (151) | 19.9 (60) |
| Did not want to let the team down | 14.8 (143) | 1.3 (4) |
| Did not think it was a serious injury | 12.3 (119) | 13.6 (41) |
| Did not want to go to the doctor | 12.0 (116) | 6.0 (18) |
| Worried about missing school and getting behind on schoolwork | 7.8 (75) | 3.0 (9) |
| Thought my teammates would think I am weak | 7.7 (74) | 3.3 (10) |
| Thought my coach would think I am weak | 7.2 (69) | 3.6 (11) |
| Thought my coach would get mad | 7.1 (68) | 1.7 (5) |
| My team was going to playoffs when it happened | 4.8 (46) | 10.6 (32) |
| Thought my parents would be upset | 3.4 (33) | 1.0 (3) |
| Concerned it would affect my chances of playing professional sports | 2.8 (27) | 3.3 (10) |
| Had an examination or project due at school that I did not want to make up | 2.0 (19) | 1.0 (3) |
| Did not have health insurance and could not go to the doctor | 1.0 (10) | 10.6 (32) |
DISCUSSION
Our study was the first that sought to understand C-AUB from a global perspective. The purpose was to determine if there were differences in sources of concussion information, knowledge, and disclosure among 3 countries with varying degrees of concussion publicity. Inconsistencies were present in the level of C-AUB by geographic location, and more global concussion initiatives are needed.
Sources of Concussion Information and Knowledge (Awareness and Understanding)
When investigating sources of concussion information, we found measurable discrepancies among collegiate athletes in the 3 countries. Those in the United States largely received concussion information from allied health care professionals, such as athletic trainers, versus only one-third of Irish athletes and virtually no Jordanian athletes. Aside from the concerning fact that 73.6% of Jordanian athletes reported never having received concussion information from any source, of those who had received such information, social media and sports news were the primary sources. Irish athletes cited movies and books as the most frequent sources of concussion information. These results demonstrate inconsistencies in how collegiate athletes received concussion information from country to country. Within the United States, all active NCAA member institutions are required to have a concussion-management plan on file and provide athletes with educational materials.29 These required concussion-education materials are most often distributed and explained by certified sports medicine health care providers (ie, athletic trainers) working at the institution. Similar regulatory directives are not mandated in collegiate sports in Ireland and Jordan. Furthermore, contrary to collegiate athletics in the United States, where athletic trainers are required to be present for sanctioned athletic competitions, nearly 41% of Gaelic Games athletes in Ireland lacked regular access to medical personnel at matches.19 The differences in access to health care professionals likely account for the vast discrepancies found among countries and the larger variance in nonreputable sources from which Irish and Jordanian athletes obtained concussion information.
Considering the differences in concussion publicity among countries, the differences in overall concussion-knowledge scores among US, Irish, and Jordanian athletes were to be expected. Total concussion-knowledge scores of US collegiate athletes were nearly 12% higher than those of Jordanian athletes and almost 18% higher than those of Irish athletes. We also observed this finding for simple concussion-symptom recognition. Again, these results are most likely due to heightened requirements for concussion education by US legislation and sport organizations. Concussion knowledge has been heavily studied and surveyed in the United States, and much of the literature pertaining to collegiate athletes suggested that their concussion knowledge and ability to identify true symptoms of concussion, such as headache, sensitivity to light or noise, feeling dizzy, and balance difficulty, were moderate.30 Comparatively, the Irish collegiate athletes in our study had the poorest scores in total concussion knowledge and symptom recognition. These results parallel the findings of previous researchers19,21 who observed that Gaelic Games athletes and Irish jockeys possessed a good overall understanding of concussion but had misconceptions about false signs and symptoms of concussion. It is also important to note that Irish athletes had the poorest scores of all countries, so there could be a connection between the misconceptions and the higher percentage of Irish athletes seeking concussion information from nonreputable versus reputable sources or from a health care professional. Additionally, Jordanian athletes in this study had moderate knowledge. This result is somewhat surprising considering that Jordanian athletes were rarely exposed to concussion information and reported a higher dependence on information from nonreputable sources. These concussion-knowledge outcomes support the need to provide Irish and Jordanian athletes with a clearer, more uniform message to negate the mixed messaging from nonreputable sources.
Pressure to Play After a Head Impact (Behaviors)
Neither sex nor sport type influenced whether US or Irish athletes described being pressured to continue participating after a head impact while playing high school or collegiate sports. However, Irish athletes were twice as likely to report a previous experience of pressure to play than US athletes in both high school and collegiate sports. Additionally, US athletes were pressured 30% less frequently by their teammates, coaches, and fans than were Irish athletes. Thus, Irish athletes are at high risk for being pressured to play by their peers and team leaders despite having sustained a potential head injury.
The percentage of US collegiate athletes who indicated they had experienced pressure to play after a head injury was similar to that of Kroshus et al14 in their 2015 study. Less pressure in the US sample versus the Irish athletes may be explained by the increase in concussion publicity and educational initiatives that targeted athletes, parents, and coaches. A primary component of the youth concussion laws in the United States is the mandated concussion education coaches receive before engaging in coaching activities.7 This approach has also been adopted by the NCAA for collegiate sport coaches.29 Additionally, numerous high-profile media reports and lawsuits in recent years in the United States have addressed coach misconduct surrounding concussion identification and reporting at high schools and prominent colleges across the country. Increased understanding and fear related to legal liability if a catastrophic event or complication occurs after a concussion may act as deterrents to bystanders and reduce their likelihood of pressuring an athlete to continue playing or negatively influencing injury identification and management.
Concussion-Reporting Behaviors
Approximately one-third of US and Irish collegiate athletes had a history of at least 1 diagnosed concussion. Although these groups had similar rates of concussion diagnosis, the percentage of Irish athletes who did not disclose a potential concussive injury was double that of US athletes (29.6% versus 15.5%). The higher prevalence of concussions in Irish athletes may be related to the greater percentage of athletes who participated in high-risk sports. The percentage of concussion nondisclosure in US collegiate athletes in this study was less than the 33.2% previously reported31 and may be attributed to the recent increase in concussion publicity in the United States. Furthermore, more nondisclosure behaviors may indicate that concussion awareness is not as advanced in Ireland as it is in the United States. This could be due to the lack of onsite sports medicine health care professionals during sport participation. The lower concussion-knowledge scores for the Irish sample could also make it more challenging for them to identify a concussion when it occurs. Regardless of the percentage differences in concussion nondisclosure, collegiate athletes from Ireland and the United States did not report suspected concussions for the same reasons; they did not want to be removed from athletic participation and did not initially identify their injury as a concussion. These findings are consistent with previous research on various athletic populations.24,31–33
As noted previously, a small percentage (2.3%) of the Jordanian college athletes reported being diagnosed with a concussion by a health care provider. Moreover, none of the participants from this group indicated having sustained a possible concussion that went unreported. The sport participation reported by the Jordanian sample included activities that have been established as having higher concussion incidence rates in collegiate athletics in the United States.34 Therefore, these low values for concussion reporting may be a byproduct of decreased concussion publicity and health care resources rather than a true lack of injury occurrence. The athletic structure in Jordan currently lacks key elements of the socioecological frameworks that have been outlined to help facilitate concussion awareness and prevention strategies in the United States.3 Presently, no mandates are focused on improving C-AUB in athletes (intrapersonal level) or additional stakeholders, such as coaches, teammates, and parents (interpersonal level). Additionally, sports medicine health care providers are not available in most athletic environments (community level), and concussion policies are lacking at all levels of sport (society and policy level). Because the Jordanian athletes did not receive formal concussion education, their awareness of concussions in themselves or their teammates may have been deficient. Furthermore, even if they identified a possible concussion, health care resources to which they can report an injury are few. Due to these deficiencies, concussion reporting or nondisclosure is not part of the culture in Jordan, which could explain the lack of or low response to these items.
Limitations
Although this study is one of the first to provide cross-cultural comparisons, it was not without limitations. First, we relied on convenience sampling. Thus, implicit bias may have been present in the athletes who completed the questionnaire. In addition, we collected data via self-reported questionnaires and assumed that participants answered honestly, but that is not a guarantee. Further, the numbers of men and women from Jordan and the United States were unbalanced. The smaller number of Jordanian female collegiate athletes may reflect the fact that fewer women participate in competitive sports in Jordan, though this number is increasing. Finally, although the surveys were culturally adapted and translated for each group, the questions may have been interpreted inconsistently by US, Irish, and Jordanian athletes. Future researchers should address C-AUB differences in athletes from African, Asian, and South American nations at various levels of competition. This work advances a global understanding of how concussion awareness is disseminated globally and how information sources are reflected in knowledge, awareness, perceptions, understanding, and reporting behaviors across cultures. Therefore, it is important that future investigations include representation from other nations with a heavy sport presence. Also, nations in which athletes obtain most of their concussion knowledge from nonreputable sources should be examined with a focus on knowledge changes after education initiatives delivered by health care professionals or reputable sources.
CONCLUSIONS
We identified significant cross-cultural differences in C-AUB among countries with various levels of concussion publicity, which may be used to help inform global concussion initiatives. In the United States, where concussion publicity is high, formal legislation exists, and increased access to sports medicine resources is available, awareness and understanding were highest. Tackling the existing global inconsistencies relative to concussion to ensure that every athlete has access to culturally applicable education resources and sports medicine health care resources is an important step in “leveling the playing field.” A large percentage of the sport-related concussion literature on concussion knowledge and reporting has been produced in the United States; however, concussion is an injury that affects athletes all over the world. As such, each geographic location presents its own unique set of needs and challenges; therefore, those tasked with developing concussion-awareness and -management plans should consider the current C-AUB of the sport culture they are serving. The public health messages used to address C-AUB in the United States may not be culturally appropriate in other regions of the world. Sports medicine professionals and researchers within each cultural context should seek out stakeholders in diverse sport communities to obtain a deeper understanding of the current resources and barriers to help inform concussion messaging to address the specific needs of that population. Efforts must be made to ensure that all athletes, across all levels of competition and all borders, are provided with consistent, evidence-based concussion education and management; yet that will likely look different in each country, depending on specific cultural needs.
Supplementary Material
REFERENCES
- 1.McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport—the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017;51(110):838–847. doi: 10.1136/bjsports-2017-097699. [DOI] [PubMed] [Google Scholar]
- 2.Stokols D. Establishing and maintaining healthy environments: toward a social ecology of health promotion. Am Psychol. 1992;47(1):6–22. doi: 10.1037//0003-066x.47.1.6. [DOI] [PubMed] [Google Scholar]
- 3.Register-Mihalik J, Baugh C, Kroshus E, Kerr ZY, Valovich McLeod TC. A multifactorial approach to sport-related concussion prevention and education: application of the socioecological framework. J Athl Train. 2017;52(3):195–205. doi: 10.4085/1062-6050-51.12.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sarmiento K, Donnell Z, Hoffman R. A scoping review to address the culture of concussion in youth and high school sports. J Sch Health. 2017;87(10):790–804. doi: 10.1111/josh.12552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi: 10.1016/0749-5978(91)90020-T. [DOI] [Google Scholar]
- 6.Pryor RR, Casa DJ, Vandermark LW, et al. Athletic training services in public secondary schools: a benchmark study. J Athl Train. 2015;50(2):156–162. doi: 10.4085/1062-6050-50.2.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gibson TB, Herring SA, Kutcher JS, Broglio SP. Analyzing the effect of state legislation on health care utilization for children with concussion. JAMA Pediatr. 2015;169(2):163–168. doi: 10.1001/jamapediatrics.2014.2320. [DOI] [PubMed] [Google Scholar]
- 8.Estimated probability of competing in college athletics. National Collegiate Athletic Association Web site. 20192019 http://www.ncaa.org/about/resources/research/estimated-probability-competing-college-athletics Accessed October 4.
- 9.Jayanthi NA, LaBella CR, Fischer D, Pasulka J, Dugas LR. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med. 2015;43(4):794–801. doi: 10.1177/0363546514567298. [DOI] [PubMed] [Google Scholar]
- 10.Myer GD, Jayanthi N, Difiori JP, et al. Sport specialization, part I: does early sports specialization increase negative outcomes and reduce the opportunity for success in young athletes? Sports Health. 2015;7(5):437–442. doi: 10.1177/1941738115598747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Post EG, Trigsted SM, Riekena JW, et al. The association of sport specialization and training volume with injury history in youth athletes. Am J Sports Med. 2017;45(6):1405–1412. doi: 10.1177/0363546517690848. [DOI] [PubMed] [Google Scholar]
- 12.Bell DR, Post EG, Trigsted SM, Hetzel S, McGuine TA, Brooks MA. Prevalence of sport specialization in high school athletics: a 1-year observational study. Am J Sports Med. 2016;44(6):1469–1474. doi: 10.1177/0363546516629943. [DOI] [PubMed] [Google Scholar]
- 13.Murphy MH, Murphy N, MacDonncha C, et al. Student activity and sports study Ireland. Student Sport Ireland Web site. 20152019 http://www.studentsport.ie/wp-content/uploads/2016/02/SASSI-Full-Report-Without-Appendices..pdf Accessed September 26.
- 14.Kroshus E, Garnett B, Hawrilenko M, Baugh CM, Calzo JP. Concussion under-reporting and pressure from coaches, teammates, fans, and parents. Soc Sci Med. 2015;134:66–75. doi: 10.1016/j.socscimed.2015.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Delaney JS, Lamfookon C, Bloom GA, Al-Kashmiri A, Correa JA. Why university athletes choose not to reveal their concussion symptoms during a practice or game. Clin J Sport Med. 2015;25(2):113–125. doi: 10.1097/JSM.0000000000000112. [DOI] [PubMed] [Google Scholar]
- 16.Llewellyn T, Burdette GT, Joyner AB, Buckley TA. Concussion reporting rates at the conclusion of an intercollegiate athletic career. Clin J Sport Med. 2014;24(1):76–79. doi: 10.1097/01.jsm.0000432853.77520.3d. [DOI] [PubMed] [Google Scholar]
- 17.O'Connell E, Molloy MG. Concussion in rugby: knowledge and attitudes of players. Ir J Med Sci. 2016;185(2):521–528. doi: 10.1007/s11845-015-1313-6. [DOI] [PubMed] [Google Scholar]
- 18.Baker JF, Devitt BM, Green J, McCarthy C. Concussion among under 20 rugby union players in Ireland: incidence, attitudes and knowledge. Ir J Med Sci. 2013;182(1):121–125. doi: 10.1007/s11845-012-0846-1. [DOI] [PubMed] [Google Scholar]
- 19.Leahy R, Farrington S, Whyte E, O'Connor S. Concussion reporting, knowledge and attitudes in Irish amateur Gaelic games athletes. Phys Ther Sport. 2020;43:236–243. doi: 10.1016/j.ptsp.2019.06.004. [DOI] [PubMed] [Google Scholar]
- 20.Sullivan L, Thomas AA, Molcho M. An evaluation of Gaelic Athletic Association (GAA) athletes' self-reported practice of playing while concussed, knowledge about and attitudes towards sports-related concussion. Int J Adolesc Med Health. 2016;29(3) doi: 10.1515/ijamh-2015-0084. /j/ijamh.2017.29.issue-3/ijamh-2015-0084/ijamh-2015-0084.xml. [DOI] [PubMed] [Google Scholar]
- 21.O'Connor S, Warrington G, Whelan G, McGoldrick A, Cullen S. Concussion history, reporting behaviors, attitudes, and knowledge in jockeys. Clin J Sport Med. 2018 doi: 10.1097/JSM.0000000000000658. [epub ahead of print] August 30. [DOI] [PubMed]
- 22.Eirale C, Tol JL, Targett S, Holmich P, Chalabi H. Concussion surveillance: do low concussion rates in the Qatar Professional Football League reflect a true difference or emphasize challenges in knowledge translation? Clin J Sport Med. 2015;25(1):73–74. doi: 10.1097/JSM.0000000000000066. [DOI] [PubMed] [Google Scholar]
- 23.Process of translation and adaptation of instruments. World Health Organization Web site. 2019 https://www.who.int/substance_abuse/research_tools/translation/en/ Accessed September 12.
- 24.Register-Mihalik JK, Guskiewicz KM, Valovich McLeod TC, Linnan LA, Mueller FO, Marshall SW. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Athl Train. 2013;48(5):645–653. doi: 10.4085/1062-6050-48.3.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kontos AP, Elbin R, Schatz P, et al. A revised factor structure for the post-concussion symptom scale: baseline and postconcussion factors. Am J Sports Med. 2012;40(10):2375–2384. doi: 10.1177/0363546512455400. [DOI] [PubMed] [Google Scholar]
- 26.McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004;14(1):13–17. doi: 10.1097/00042752-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 27.Wallace J, Covassin T, Nogle S, Gould D, Kovan J. Knowledge of concussion and reporting behaviors in high school athletes with or without access to an athletic trainer. J Athl Train. 2017;52(3):228–235. doi: 10.4085/1062-6050-52.1.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cohen J. Statistical Power Analysis for the Behavioural Sciences 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates;; 1988. [Google Scholar]
- 29.Parsons JT. 2014-15 NCAA Sports Medicine Handbook. National Collegiate Athletic AssociationWeb site. 2019 http://www.ncaapublications.com/productdownloads/MD15.pdf Published 2014. Accessed October 4.
- 30.Bernstein JP, Calamia M, Mullenix S. Predictors of collegiate student-athletes' concussion-related knowledge and behaviors. Can J Neurol Sci. 2019;46(5):575–584. doi: 10.1017/cjn.2019.76. [DOI] [PubMed] [Google Scholar]
- 31.Kerr ZY, Register-Mihalik JK, Kroshus E, Baugh CM, Marshall SW. Motivations associated with nondisclosure of self-reported concussions in former collegiate athletes. Am J Sports Med. 2016;44(1):220–225. doi: 10.1177/0363546515612082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wallace J, Covassin T, Beidler E. Sex differences in high school athletes' knowledge of sport-related concussion symptoms and reporting behaviors. J Athl Train. 2017;52(7):682–688. doi: 10.4085/1062-6050-52.3.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Beidler E, Bretzin AC, Hanock C, Covassin T. Sport-related concussion: knowledge and reporting behaviors among collegiate club-sport athletes. J Athl Train. 2018;53(9):866–872. doi: 10.4085/1062-6050-266-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zuckerman SL, Kerr ZY, Yengo-Kahn A, Wasserman E, Covassin T, Solomon GS. Epidemiology of sports-related concussion in NCAA athletes from 2009-2010 to 2013-2014: incidence, recurrence, and mechanisms. Am J Sports Med 2015; 43(11):2654–2662. doi: 10.1177/0363546515623241. doi: 10.1177/0363546515623241. [published correction appears in Am J Sports Med 2016;44(1):NP5. doi: ] [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.