

Abstract
PURPOSE:
The study aims to evaluate and see if experiential learning theory for teaching cataract surgery can improve the ability of students to retain more knowledge compared to the classical or traditional way of teaching.
METHODS:
A pre and post control group design of 32 graduates was conducted in 2016 at King Saud University, Riyadh, Saudi Arabia to examine the effect of experiential learning as an applicable way for teaching cataract surgery. The total of graduates including males and females were divided into control and experimental groups to which the educational materials about cataract surgery were presented as a lecture and as wet lab session respectively. All the data collected were entered in SPSS version 22 for analysis and a P ≤ 0.05 was considered significant.
RESULTS:
Both control and experimental groups showed good retention rate of knowledge. However, the gain of knowledge was more in the Wet lab group. The scores mean increased more than 5 points in this group compared to 2.5 points only in the lecture groups.
CONCLUSION:
Both teaching modalities were effective in improving the knowledge rate of the students. However, in the experiential learning group (Wet lab group), the gain of knowledge was higher compared to that in the traditional group (lecture group).
Keywords: Cataract surgery, experiential learning, retention of knowledge, traditional learning
INTRODUCTION
Cataract surgery is one of the most common procedures performed in ophthalmology. In 2000, WHO anticipated that more than 32 million cataract surgeries will be performed by 2020.[1] In cataract surgery, the opaque natural lens will be removed and replaced by an artificial lens. Any ophthalmologist should be comfortable performing this kind of surgery. One of the milestones of ophthalmology residency programs is to teach cataract surgery and it is always a hot topic in ophthalmology meetings. One of the important aspects that residents look at when they try to choose a residency program is how it can teach cataract surgery.[1]
Most ophthalmology residency programs are using lectures in teaching the basic knowledge of cataract surgery. These lectures are about the concrete knowledge of cataract and cataract surgery; such as, causes of cataract, indications of cataract surgery, different surgical techniques and management of surgical complications. The amount of information absorbed by residents from these lectures is not too much as we already know from the literature on traditional teaching.[2]
Teaching surgery in general is not an easy task for being directly related to the patient's safety. There are many ways to teach surgery which include giving lectures, directly observing surgeries in the operating rooms, watching videos, attending courses, going to the wet lab and using simulation.[3] Each one of these methods has its own advantages and disadvantages. In talking about teaching surgery, academics in the medical field are keen on improving student′s or resident′s skill rather than improving the retention rate of knowledge.
Surgery is a skill which involves doing something by hands. From this aspect, researchers would like to propose a new way of teaching surgery by applying the experiential learning theory. This is mainly to improve the retention rate of knowledge rather than improving the skills which is a very important task too.
The study brings together two areas of importance: 1st is to probe the distribution of different learning and teaching modalities among graduates in the medical education and 2nd is to identify and tailor the most suitable strategies of instruction and learning. Understanding the vital role of experiential learning strategy will help to customize learning methods to students′ learning needs, which will contribute to students' satisfaction and result ultimately in the production of high quality medical educators. The purpose of this study is to assess the effective role of experiential learning as a teaching modality for medical graduates at King Saud University.
METHODS
The study is a pre and post control group design in which the sample was divided into two groups: intervention group and control group. It was conducted at King Saud University, Riyadh to compare the effectiveness of experiential learning versus traditional learning on students' retention of knowledge. The total of 32 graduates, equally and randomly divided into control and experimental groups, was included in the study. Educational materials about Cataract surgery were presented as a lecture to the graduates in the control group by a teacher during 50-min session. The content was simply presented through Power-Point slides. In the other group (experimental), educational materials were presented during 50 min as a Wet lab session. The educational content of both groups was similar and presented by the same instructor. Course content was about the causes and therapeutic surgical options of cataract as well as the complications and management of each surgical step. This study was approved by the Institutional Review Board, of King Saud University. Also, a written consent form was obtained from all participants. Data were secured and participants received a number to secure their identity.
The Medical Education Department introduced a multi-disciplinary block system in its traditional teaching method in order to improve clinical integration and problem solving. It is composed approximately of 200–250 students from both genders each year, divided into groups of around 70–80 students.
Sample size
The subject of the study included the medical graduates, both males and females during the academic year 2016. The total number of medical graduates is approximately 250 (both males and females) and they will be randomly divided into groups of around 80 graduates when they are about to start their internship. We took one group as a representative of the 2016 batch and according to our inclusion and exclusion criteria, we had 32 graduates divided randomly, on the basis of their GPA, in two groups: one control group and one intervention group. The total number of graduates includes both genders at ratio male:female 1.5:1 respectively. The inclusion criteria were about medical graduates of King Saud University who are about to start their internship. The exclusion criteria included any graduate who has applied for or thought to apply for Ophthalmology residency program and this was identified by a direct question to the graduates. Also, any graduate having an elective rotation in Ophthalmology was excluded as well. We didn't want to include a graduate who are interested in ophthalmology as this might vary the pre-exist knowledge on cataract and cataract surgery among the graduates. The study was an experimental, randomized pretest-posttest control group design. The sample was randomly divided into two groups: Group 1 (intervention group) which included medical graduates who will go to the Wet Lab to be taught cataract surgery, Group 2 (control group) which included medical graduates who will receive a traditional lecture on cataract surgery. The control group (n =16) will attend a traditional lecture of designed coursework while the experimental group (n =16) will participate in experiential learning of the same course.
Materials
Participation in the study was voluntary. A briefing session to provide students with the necessary information regarding their participation and to screen the graduates who have any experience in the Ophthalmology was done. Each group was given a pre-lecture quiz for 10 min followed by a teaching on cataract surgery (either in the Wet lab as experiential learning or in the classroom as a traditional learning) for 30 min. The same information were delivered to students in the both groups. Afterwards a post lecture quiz was conducted for 10 min in the form of a hard copy at the end of the teaching activity to assess the retention of knowledge with two methods of learning. The result score (total score out of 100) was collected by our research coordinator. The standard deviation (SD) of ten was estimated by dividing the difference between the expected maximum and minimum score by four. In addition a power of 80% and confidence level of 95% were used. The expected difference in scores to be determined as statistically significant was 5. As a result, the minimum calculated total sample size using Open-Epi website was thirty two graduates (sixteen in each group) which should be sufficient.
Data were collected pre- and post-intervention using a specific data collection sheet; they were then cleaned, managed, and coded using Microsoft Excel 2013®; Microsoft Corporation, Redmond, Washington, USA. The analysis was done using SPSS version 22 (IBM Inc., Chicago, Illinois, USA). Descriptive analysis was done, where variables were presented in the form of mean (±SD). Wilcoxon Signed Rank Test was used to investigate whether there was any significant difference between pre- and post- intervention measures. A confidence interval level was set to 95% where a corresponding P value threshold was identified as 0.05 and any output P below 0.05 would be interpreted as an indicator of statistical significance.
In order to assess the participants' retention of knowledge concerning teaching and learning strategies provided by the instructor, 12 multiple choice items are constructed and administered to the graduates in the lecture hall of ophthalmology department at KSU. Each student was given a number instead of a name and the quiz was corrected by an independent person to minimize any possible biases. The result score (the main outcome) was compiled by the research coordinator. All the data were entered in SPSS version 22 for analysis. The post teaching quiz and difference between pre and post teaching score were used to determine the effect of learning experiential theory on knowledge retention. Independent t-test was used to see the difference of scores of graduates' knowledge in the lecture and experiential groups before and after the lecture. A P ≤0.05 was considered significant.
RESULTS
A total of 32 interns were included in the analysis, with each group having 16: Lecture and Wet lab. Both groups showed good retention rate of knowledge. The pre-test (test before the intervention) mean±SD of the lecture group was 8.6±3.1, ranging from 3 to 15 scores with a post-test mean±SD was 11.1±1.9, range 8 to 15; this increase in knowledge was statistically significant (P =0.005). Also, the students in the Wet lab group showed improvement of their knowledge based on the pre- and post- tests result. The pre- test mean±SD of the Wet lab group was 6.7±2.7, 2 to 12 range and post- test mean±SD was 12.3±1.4 with a range of 10 to 14, the difference was statistically significant (P =0.001). However, the gain of knowledge was more in the Wet lab. The scores mean increased more than 5 points in the wet lab group compared to 2.5 points only in the lecture group [Table 1 and Figure 1].
Table 1.
The pre and post intervention test results for both groups
| Group | Pre-test Mean (SD) | Post-test Mean (SD) | P |
|---|---|---|---|
| Lecture | 8.6 (3.1) | 11.1 (1.9) | 0.005 |
| Wet lab | 6.7 (2.7) | 12.3 (1.4) | 0.001 |
Figure 1.
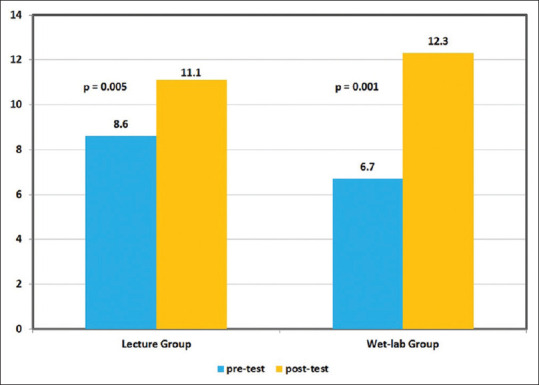
Pre and post tests comparisons between lecture and wet-lab groups (n = 32)
DISCUSSION
In 2003, Spencer suggested that we best learn from our experience.[3] In his theory, learner passes through a circle of four steps or phases: thinking (theory), applying (acting), experiencing and reflecting.[4,5] All of these steps allow the students integrate the new information with what already exists in his or her mind. By doing this, the student will be able to understand the new information and transfer it to the long-term memory as the deep encoding of the new information just occurred in the human mind. Understanding is very important in improving the retention rate.[5]
An example of using or applying this theory is to teach cooking. It is more responsive to take students to the kitchen and allow them to cook rather than having them sit in the classroom and giving a lecture.
Experiential learning has been used for long time in the different levels of education: kindergarten, elementary, as well as medical education.[2] However, there is not much evidence in using this theory in teaching surgery for improving retention of knowledge. From this point, this could be a novel approach in teaching surgery.[6]
The result of our study showed that both teaching modalities were effective in improving the knowledge rate of the students. However, in the experiential learning group (Wet lab group) the gain of knowledge was higher compared to that in the traditional group (lecture group). Also, the instructor who conducted both teaching modalities (lecture and Wet lab) noticed that students′ engagement was more in the experiential learning compared to the traditional learning.
CONCLUSION
In conclusion, we believe that medical curriculum approaches play a significant role in medical education. Presently, we do not have any study available locally on experiential learning styles of graduates at internship levels. This research is important because it may contribute to the theory of learning styles and, in addition to prior research findings, it may provide evidence about Saudi undergraduate level of education. Our study tries to explore the effective role of experiential learning style dimension to add to the current body of related educational knowledge.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. He does not mind to share the data with the journal.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Roodhooft JM. Leading causes of blindness worldwide. Bull Soc Belge Ophtalmol. 2002;35(238):19–25. [PubMed] [Google Scholar]
- 2.Kaufman D. Applying educational theory in practice. Br Med J. 2003;326(7382):213–6. doi: 10.1136/bmj.326.7382.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Spencer J. Learning and teaching in the clinical environment. Br Med J. 2003;326(7389):591–4. doi: 10.1136/bmj.326.7389.591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fowler J. Experiential learning and its facilitation. Nurse Educ Today. 2008;28(4):427–33. doi: 10.1016/j.nedt.2007.07.007. [DOI] [PubMed] [Google Scholar]
- 5.Kolb DA. Experiential Learning. New Jersy: Prentice Hall, Englewood Cliffs; 1984. [Google Scholar]
- 6.Taravella MJ, Davidson R, Erlanger M, Guiton G, Gregory D. Time and cost of teaching cataract surgery. J Cataract Refract Surg. 2014;40(2):212–6. doi: 10.1016/j.jcrs.2013.07.045. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. He does not mind to share the data with the journal.