

Abstract
Purpose:
To compare (1) rates of complication and reoperation, (2) rate of anterior cruciate ligament (ACL) graft failure, and (3) patient reported outcomes (PRO) among patients following hamstring autograft ACL reconstruction (ACLR) with and without independent suture tape reinforcement at a minimum 2-year clinical follow-up
Methods:
A 1:2 matched cohort comparison was performed on patients who underwent hamstring autograft ACLR with and without independent suture tape reinforcement between July 2011 and July 2017. Patients were matched according to age, sex, BMI, pre-injury Tegner score, and concomitant meniscus injury. Medical records were reviewed for demographics, additional injuries, and concomitant procedures. PRO scores (including the Tegner activity, Lysholm, and International Knee Documentation Committee (IKDC) scores) and physical exam findings were collected both preoperatively and at a minimum of 2 years postoperatively.
Results:
Overall, 108 patients were included, with 36 patients (mean age 25.3 years, range 13–44) who underwent ACLR with independent suture tape reinforcement and 72 patients (mean age 24.9 years, range 13–54) without suture tape reinforcement. Overall, 5/36 (14%) suture tape patients and 10/72 (14%) control patients underwent reoperation. At an average follow-up of 26.1 months in the suture tape cohort and 31.3 months in the control cohort, one patient in the suture tape and four patients in the control cohort experienced graft failure. There were no statistically significant differences between the suture tape and control groups in regard to return to sport (89% and 88%), postoperative IKDC scores (94.4 and 93.8), and Lysholm scores (95.6 and 94). There was a statistically significant difference between the suture tape and control groups in post-operative Tegner activity score at 7.1 (95% CI: 6.5–7.6) and 6.4 (95% CI: 6.2–6.6) (p = 0.026), respectively.
Conclusions:
ACLR with hamstring autograft and independent suture tape reinforcement was performed safely with a low rate of complications, graft failure, and reoperation with similar patient reported outcomes, function, and return to sport when compared to hamstring autograft ACLR without suture tape reinforcement at minimum 2-year follow-up.
Level of Evidence:
Level III, retrospective comparative study
INTRODUCTION
Over the last decade, there have been a multitude of changes in ACLR surgical technique– femoral tunnel drilling technique and positioning, method of graft fixation, and graft augmentation) in an effort to decrease the rate of graft failure. However, little variation has been observed in graft-type preference, with a continued high utilization of hamstring autograft.1, 2 A recent meta-analysis reported the incidence of graft failure in hamstring autograft ACLR at 2.84%,3 with higher rates of failure reported in younger patients with high activity levels.4 Additionally, studies have attempted to elucidate predictors of failure in patients undergoing ACLR with hamstring autograft, such as reporting failure rates as a function of graft diameter, with decreased rates of failure in grafts equal to or greater than 8 millimeters (mm) in diameter.5
With the high variability of autograft diameter in ACLR patients, various methods have been utilized for graft augmentation. The utilization of ligament augmentation devices was first employed in 1980, with the purpose of increasing the tensile strength of the soft tissue graft and promoting optimal healing following ACLR.6 Use of these early devices has since diminished due to high rates of failure and noninfectious knee synovitis/effusion.7 More recently, the use of suture tape – a braided ultra-high-molecular-weight polyethylene material – reinforcement has been described in effort to provide biomechanical support during the proliferation, maturation, and ligamentization graft healing phases.8, 9 To date suture tape reinforcement has been successfully incorporated into various knee ligament repairs, including medial collateral ligament repair,10 posterolateral corner repair,11 posterior cruciate ligament repair,12 and ACL repair.13, 14 Only one recent study has compared the clinical results of ACLR with and without suture reinforcement;15 therefore, additional research is necessary to evaluate outcomes when utilizing this technique. The purposes of this study were to compare (1) rates of complication and reoperation, (2) rate of ACL graft failure, and (3) patient reported outcomes (PRO) among patients following hamstring autograft ACLR with and without independent suture tape reinforcement at a minimum 2-year clinical follow-up. We hypothesized that ACLR with suture tape reinforcement will result in a lower rate of ACL graft failure with a similar rate of complications and reoperations and comparable clinical outcomes to ACLR without suture tape reinforcement.
MATERIALS AND METHODS
This retrospective case-control study was performed at a single academic sports medicine center from 2011–2017. Following approval of the institutional review board (IRB#: 15–000601) subjects who underwent primary ACLR with semitendinosus or semitendinosus/gracilis autograft from July 2011 to July 2017 by three of the senior authors (BAL, MJS, and AJK) were identified. Inclusion criteria consisted of patients who (1) underwent ACLR with or without independent suture tape reinforcement, (2) had a minimum 2-year follow-up, and (3) were available for contact follow-up regarding confirmation of any complications, reoperations, and patient reported outcomes. Exclusion criteria consisted of (1) revision ACLR, (2) utilization of allograft or patellar tendon autograft, (3) concomitant posterior cruciate or collateral ligament surgery, and (4) a lack of minimum 2-year follow-up.
Patient charts were individually reviewed to obtain patient demographics, physical examination findings, operative details (including graft type, graft construct, graft reinforcement, fixation technique, concomitant procedures, etc.), concomitant injuries, reoperations, complications, return-to-sport timeline, PRO (Tegner activity score, Lysholm scores, and International Knee Documentation Committee (IKDC) scores)16, 17 and clinical outcomes (range of motion, presence of effusion, Lachman exam, pivot shift exam). Patients were contacted via telephone when necessary. All patients were assessed by physical exam performed by the operating surgeon (BAL, MJS, and AJK) during clinical follow-up. ACLR failure was defined as graft rupture and/or revision reconstruction procedures. Patients were assigned to one of two groups: hamstring autograft ACLR or hamstring autograft ACLR with suture tape reinforcement. The three authors (BAL, MJS, and AJK) performing ACLR in this study began incorporating suture tape augmentation in hamstring autograft constructs in 2017 as a standard of care.All patients meeting inclusion criteria in the suture tape cohort were matched 1:2 with patients in the control group of ACLR without suture tape reinforcement. Matching was performed according to age at time of ACLR (within 2 years), sex, BMI (within 5 kg/m2), pre-injury Tegner (within 1 point), initial visit VAS both at rest and with use (within 1 point), medial meniscus injury, and lateral meniscus injury.
Surgical Technique
Patients included in this study underwent primary ACLR utilizing an all-inside technique with semitendinosus or semitendinosus/gracilis autograft, with or without the addition of independent suture tape reinforcement. Autograft constructs consisted of quadrupled semitendinosus tendon or combined quadrupled semitendinosus and gracilis tendons. All grafts were constructed using the GraftLink® (Arthrex, Naples, FL) technique with suspensory fixation (Tightrope®, Arthrex) on both femoral and tibial sides. For the suture tape reinforced grafts, one FiberTape® (Arthrex) suture – ultra-high molecular weight polyethylene core with a braided polyester jacket – was passed through the femoral Tightrope® (Arthrex) button creating a doubled FiberTape® (Arthrex) augment (Figure 1).
Figure 1.
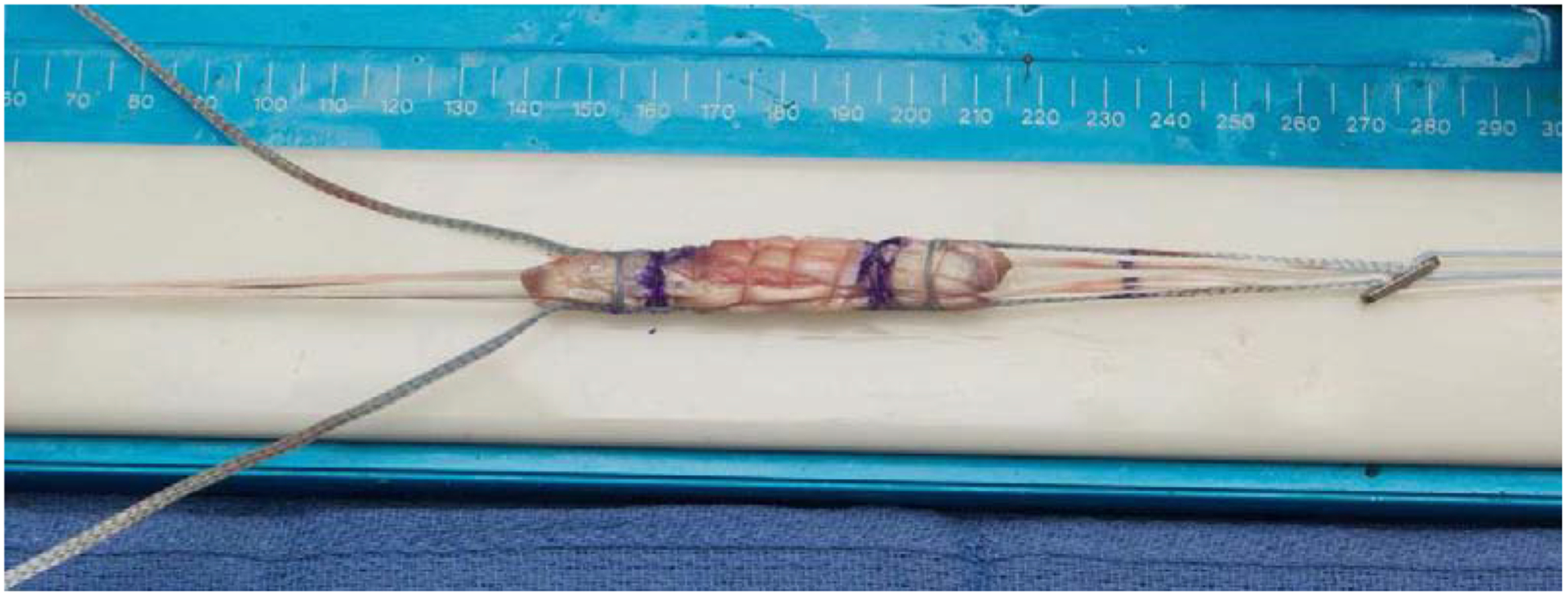
Prepared quadrupled hamstring ACL autograft with suspensory fixation devices and suture tape augmentation.
Independent femoral and tibial sockets were created in all patients. The femoral socket was prepared by anterograde drilling through a low anteromedial portal, and drilled to an osseous depth of at least 20 millimeters (mm). The tibial socket was then created drilling in a retrograde fashion utilizing a FlipCutter® (Arthrex) to an osseous depth of at least 30 mm. The graft was then passed into the knee first proximally, obtaining fixation with the TightRope® button on the lateral femoral cortex. Next, a passing suture was used to pass the tibial TightRope® into the knee joint and through the tibial socket. Suspensory sutures were then passed through the external attachable button system (ABS, Arthrex) on the outer tibial cortex at the aperture of the socket. For the suture reinforced constructs, the FiberTape® sutures were passed independently through the ABS button. The knee was cycled through flexion and extension multiple times while the tibial side of the graft was pretensioned. Final proximal and distal tensioning was performed with the knee in full extension. For the suture reinforced constructs, the FiberTape® sutures were tensioned independently of the graft to avoid over-tensioning, then fixed to the tibia with a SwiveLock® (Arthrex) anchor. An arthroscopic image of a tensioned hamstring autograft with suture tape reinforcement following fixation is shown in Figure 2.
Figure 2.
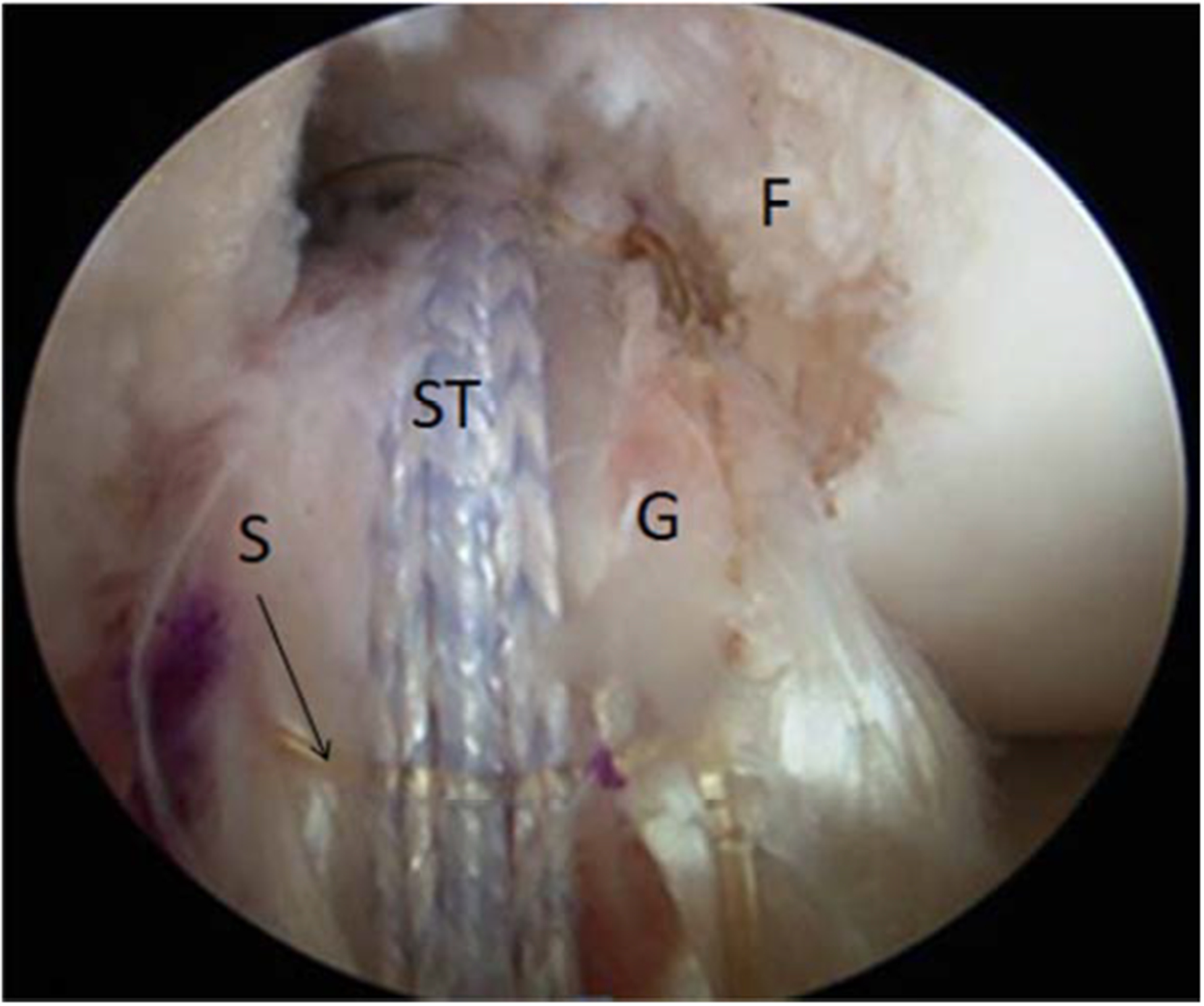
Viewing the left knee in 90 degrees of flexion with the 30° arthroscope from the anteromedial portal, demonstrating tensioned hamstring autograft with suture tape reinforcement following fixation of the graft. F, femur; G, quadrupled hamstring ACL autograft; S, running absorbable suture; ST, suture tape
All patients followed a standardized rehabilitation protocol with immediate weight-bearing and range of motion as tolerated with a hinged knee brace and crutches. Patients were allowed to return to running at 3–4 months and cutting and pivoting sports at 9–12 months as determined by satisfactory progress with the physical therapist and orthopedic surgeon.
STATISICAL ANALYSIS
Collected data was stored in Microsoft Excel (2010; Microsoft Corp) and analyzed with JMP Pro (v. 14.1.0; SAS Institute). After analyzing data for parametric/nonparametric assumptions, the demographics, PROs, complications, reoperations, and failure rates of the control and suture tape reinforcement ACLR cohorts were compared utilizing Student t tests or Wilcoxon rank-sum tests for continuous variables (age, PRO scores, etc.) and chi-square analysis or Fisher exact tests for categorical variables (injury characteristics, reoperations, etc.). P values < .05 were considered statistically significant.
A post-hoc power analysis for the chi-square test was performed to determine the sample size by use of a 2-tailed hypothesis test at an alpha level of 0.05, a power of 0.8, and a sample proportion of 1:2 in the cohorts. The graft failure rates of 4% in the suture tape group and 8% in the control group based on a previous study prospectively analyzing greater than 2,400 ACL reconstructions.4 This revealed the total sample size needed to detect a difference to be 1,290 patients with 430 in the suture tape group.
RESULTS
A total of 67 patients underwent ACLR with hamstring autograft and independent suture tape reinforcement between July 2011 and July 2017 at our institution. Of these patients 16 were excluded; 9 due to multiligament knee surgery and 7 were revision ACLR cases. As a result, 51 patients were eligible for 2-year follow-up. Fifteen of these patients were lost to follow-up resulting in 36 patients who were included and analyzed in the study (Figure 3). All 36 patients in the suture tape cohort were matched to a cohort of 72 control patients (ACLR without suture tape reinforcement) in a 1:2 fashion. The average clinical follow-up time was 26.1 (24.0–31.3) months in the suture tape cohort versus 31.3 (24.0–69.3) months in the control cohort (p = 0.898). Demographic characteristics of the two cohorts are reported in Table 1. There were no significant differences between the two cohorts in regards to patient demographics, including to age, sex, BMI, visual analog pain score (VAS) at presentation, pre-injury Tegner activity score, and time from injury to reconstruction.
Figure 3.
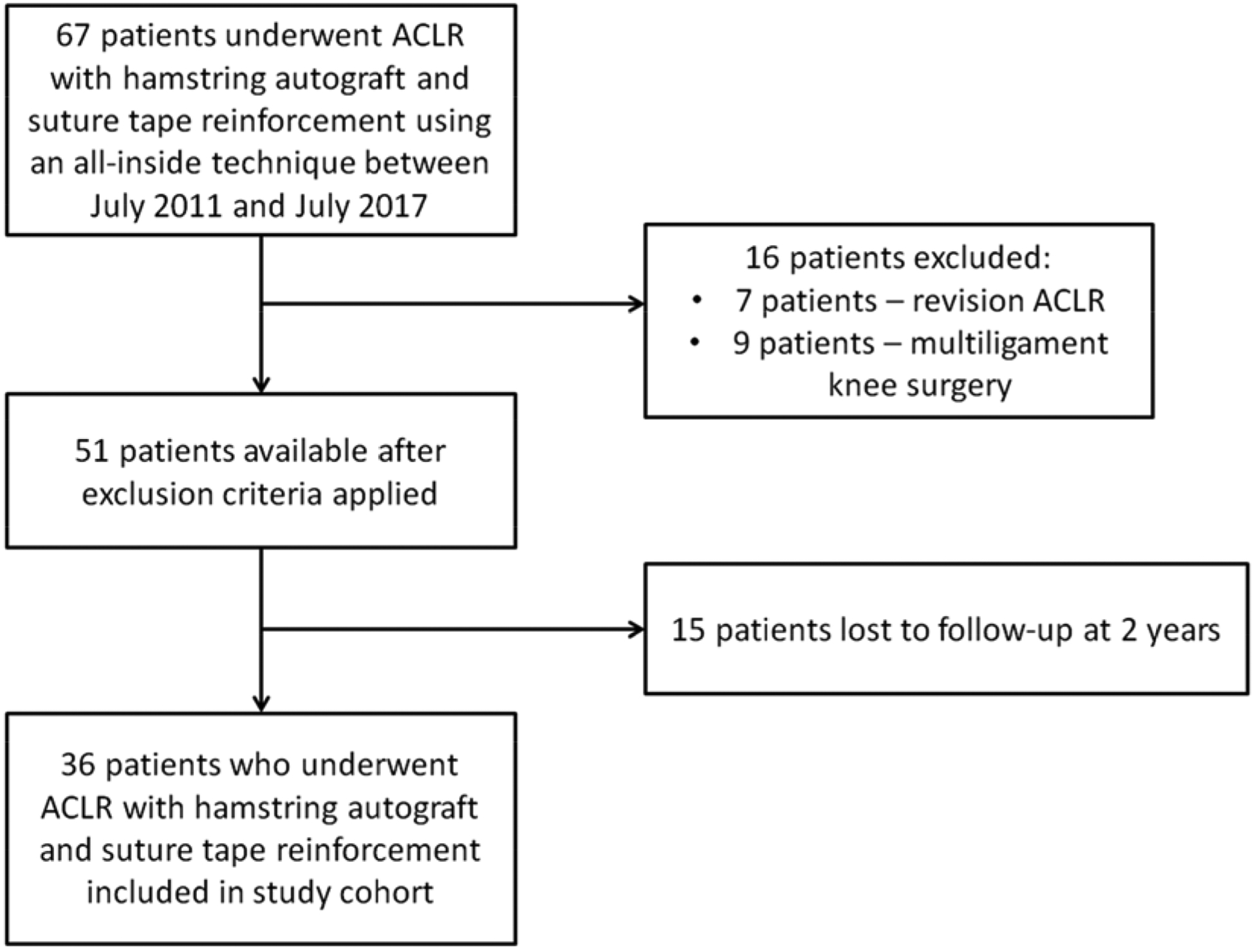
Flow chart of study patients in the suture tape cohort
TABLE 1:
Demographic Characteristics of Patient Study Cohorts
| Characteristic | Suture tape cohort (n = 36) | Control cohort (n = 72) | P |
|---|---|---|---|
| Age, years (range) | 25.3 ± 8.6 (13–44) | 24.9 ± 9.6 (13–54) | 0.629 |
| Sex, % male | 69 (25 of 36) | 69 (50 of 72) | 1.000 |
| BMI, kg/m2 | 25.9 ± 4.7 | 25 ± 4.2 | 0.391 |
| VAS at rest (initial visit) | 1.3 ± 1.2 | 1.5 ± 1.7 | 0.957 |
| VAS with use (initial visit) | 3.8 ± 2.7 | 3.7 ± 2.7 | 0.950 |
| Pre-injury Tegner activity score | 7.2 ± 0.8 | 6.7 ± 1.5 | 0.075 |
| Injury to reconstruction, months (range) | 7.6 ± 16.0 (0.2–76.2) | 7.1 ± 18.6 (0.3–124.4) | 0.311 |
| Clinical follow-up, months (range) | 26.1 ± 2.5 (24.0–31.3) | 31.3 ±12.9 (24.0–69.3) | 0.898 |
Note: values expressed as mean ± standard deviation (range) or percentage (count) when applicable
Injury characteristics and additional operative procedures at the time of ACLR are provided in Table 2. There were no statistically significant differences in injury characteristics or additional operative procedures, aside from the incidence of medial collateral ligament (MCL) injuries, which was higher in the suture tape cohort. All MCL injuries were treated non-operatively.
TABLE 2:
Injury Characteristics and Additional Procedures
| Suture tape cohort cohort (n = 36) | Control cohort (n = 72) | P | |
|---|---|---|---|
| Medial meniscus injury | 14 (39%) | 32 (44%) | 0.681 |
| Lateral meniscus injury | 17 (47%) | 32 (44%) | 0.839 |
| Medial and lateral meniscus injury | 4 (11%) | 16 (22%) | 0.196 |
| Meniscus repair or partial meniscectomy, n (%) | 24 (67%) | 46 (64%) | 0.833 |
| Tibial or femoral chondral lesion | 12 (33%) | 18 (25%) | 0.372 |
| MCL injury | 8 (22%) | 2 (3%) | 0.002 |
Note: values expressed as count (percentage)
Patient reported outcome data is presented in Table 3. There was a high rate of return to sport in both groups, including 89% in the suture tape cohort and 88% in the control cohort (p = 1.000) at a mean time of 11.9 and 11.6 months (p = 0.587), respectively. There was a statistically significant difference in post-operative Tegner activity scores (suture tape: 7.1 vs. control: 6.6, p = 0.026); however, 95% CI demonstrated overlap (suture tape: 6.5–7.6 vs. control: 6.2–6.6). The mean change in pre to post-operative Tegner activity score between groups was also found to be statistically significant at 0.09 (95% CI: −0.04–0.21) in the suture tape group and 0.27 (95% CI: 0.14–0.4) in the control group (p = 0.0291) There were no statistically significant differences in PRO (Lysholm scores or IKDC scores), physical exam data (ROM, Lachman exam, presence of effusion).. Patients in both groups who experienced graft failure were excluded from statistical analysis for clinical outcome data consisting of PRO’s (Lysholm and IKDC scores), range of motion, Lachman exam, pivot shift exam, and presence of effusion.
TABLE 3:
Patient Outcome Data
| Suture tape cohort (n = 36) | Control cohort (n = 72) | P | |
|---|---|---|---|
| Return to sport, n (%) | 32 (89%) | 63 (88%) | 1.000 |
| Return to sport time, months (95% CI) | 11.9 (10.3–13.4) | 11.6 (10.5–12.7) | 0.587 |
| Range of motion arc at final follow-up, degrees | 136 ± 6.1 | 137 ± 7.0 | 0.436 |
| • Extension, degrees | −0.09 ± 6.4 | −0.44 ± 6.5 | 0.175 |
| • Flexion, degrees | 135.9 ± 0.9 | 136.6 ± 1.7 | 0.621 |
| Post-operative Tegner activity score, mean (95% CI) | 7.1 (6.5–7.6) | 6.4 (6.2–6.6) | 0.026 |
| Lysholm, mean (95% CI) | 95.6 (93.5–97.7) | 94 (92.1–95.7) | 0.165 |
| IKDC, mean (95% CI) | 94.4 (91.7–97.1) | 93.8 (91.8–95.7) | 0.436 |
| Lachman exam | |||
| • Patients with grade 0 | 34 (97%) | 65 (96%) | 0.699 |
| • Patients with grade 1 | 1 (1%) | 3 (3%) | |
| Pivot shift exam | |||
| • Patients with grade 0 | 35 (100%) | 66 (97%) | 0.547 |
| • Patients with grade 1 | 0 (0%) | 2 (3%) | |
| Presence of effusion | 0 (0%) | 0 (0%) | 1.000 |
Note: values expressed as mean ± standard deviation and 95% CI or percentage (count) when applicable
Complications and reoperations are listed in Table 4. Overall, 3% (1/36) of patients in the suture tape cohort and 6% (4/72) of patients in the control cohort (p = 0.663) experienced graft failure and underwent revision ACLR. Two patients in the suture tape cohort underwent reoperation for repeat meniscal procedures following initial meniscus repair, one patient underwent arthroscopic debridement of a cyclops lesion, and two patients developed arthrofibrosis requiring arthroscopic lysis of adhesions. One patient in the control cohort developed an infection requiring arthroscopic irrigation and debridement, three patients underwent reoperation for meniscal procedures following initial meniscus repair, and three patients developed arthrofibrosis requiring arthroscopic lysis of adhesions. The patient in the control group who developed a post-operative infection requiring arthroscopic irrigation and debridement subsequently developed arthrofibrosis which necessitated arthroscopic lysis of adhesions, thus accounting for two complications.
TABLE 4:
Complication, Reoperation, and Failure Rates in the Study Cohorts
| Complications, reoperations, and failures | Suture tape cohort (n = 36) | Control cohort (n = 72) | P |
|---|---|---|---|
| None | 31 (86%) | 62 (86%) | 1.000 |
| Infection | 0 (0%) | 1 (1%) | 0.366 |
| Arthrofibrosis | 2 (6%) | 3 (4%) | 0.750 |
| Revision meniscal procedure | 2 (6%) | 3 (4%) | 0.750 |
| Graft failure + revision ACLR | 1 (3%) | 4 (6%) | 0.663 |
| Total reoperations | 5 (14%) | 10 (14%) | 1.000 |
Note: values expressed as count (percentage)
one patient in the control ACLR group experienced two complications (infection requiring arthroscopic irrigation and debridement followed by arthrofibrosis requiring arthroscopic lysis of adhesions)
DISCUSSION
The principal finding of this matched cohort comparison was similar rates of ACL graft failure at 2+ year clinical follow-up after hamstring autograft ACLR utilizing an all-inside technique with and without the addition of independent suture tape reinforcement. Additionally, our study did not identify statistically significant differences in complication and reoperation rates, return to sport, and PRO between the two groups.. Both surgical techniques were demonstrated to be performed safely with low rates of short-term failure and high rates of return to sport and PRO.
Post-operative total complication rates in the suture tape reinforced and control cohorts were both 14% and not statistically different. No patients in the suture tape cohort developed a joint effusion or signs of synovitis. The rate of arthrofibrosis was 6% in suture tape cohort versus 4% in the control ACLR group, all of whom underwent arthroscopic lysis of adhesions. These rates are comparable to that demonstrated in current literature. A recent retrospective review by Bodendorfer et al. reported that 6.7% of patients who underwent suture augmented ACLR developed arthrofibrosis requiring lysis of adhesions.15 This is an important finding, as synthetic ligament devices utilized in ACLR have historically led to poor outcomes, demonstrating high rates of failure, synovitis, and sterile effusions in former studies.7, 18, 19 As such, the introduction of suture tape into the intra-articular environment of the knee may concern surgeons for a resulting synovial reaction and iatrogenic articular cartilage damage. Although this has yet to be confirmed in a clinical study, Smith et al used a canine model to demonstrate no additional synovitis or cartilage damage with intact or transected suture tape in comparison to controls at second look arthroscopy.20
In regard to graft failure, one patient (3%) in the suture tape cohort and four patients (6%) in the control ACLR cohort experienced graft failure requiring revision ACLR. Our findings are consistent with those demonstrated by Bodendorfer et al., who reported graft failure rates of 6.7% in suture augmented ACLRs.15 These results are similar to the reported rates for graft failure following ACLR with hamstring autograft without suture tape reinforcement utilizing an all-inside technique of 2.2%21, 4.0%22, and 9.8%23. The rate of re-rupture in this suture tape cohort is similar to the 4.8% rate reported following ACL repair with suture tape reinforcement at 2 year clinical follow-up.24 The primary goal of suture tape reinforcement in ACLR is graft protection during the healing and maturation phases. However, the risk of over-tensioning the suture tape and effectively stress-shielding the soft tissue graft does exist. In a biomechanical study of ACLR with suture tape reinforced bovine grafts, Bachmaier et al. reported low level loads were transferred through the soft tissue graft with the suture tape experiencing load only after a high level had been reached. Ultimately, their study reported suture tape reinforcement to result in decreased graft elongation and increased ultimate load to failure in both small (8 mm) and regular (9 mm) sized soft tissue grafts.8 This finding was reaffirmed by Noonan et al., who reported suture tape reinforcement to result in decreased total elongation via increasing dynamic stiffness and load to failure in both tripled and quadrupled bovine grafts.25 In a preclinical canine model, Smith et al. reported ACLR with quadriceps tendon allograft and suture tape reinforcement to demonstrate less lameness, less pain, and increased ROM at 6 months post-operative compared to ACLR with patellar tendon autograft.26
A high number of patients in the suture tape cohort (89%) returned to their prior level of sport at a mean of 11.8 months, which was not statistically different from the control cohort (88%; mean 11.6 months). Patients in both cohorts demonstrated excellent ROM, mean Lysholm, and mean IKDC scores at final follow up. Mean post-operative IKDC scores were 94.4 (95% CI: 91.7–97.1) in the suture tape group and 93.8 (91.8–95.7) in the control group (p = 0.436) indicating patients in both groups achieved near normal knee function with minimal symptoms following ACLR.27 Mean post-operative Lysholm scores were 95.6 (95% CI: 93.5–97.7) in the suture tape group and 94 (95% CI: 92.1–95.7) in the control group (p = 0.165) suggesting the vast majority of patients in both groups achieved good to excellent knee function post-operatively.28 The mean post-operative Tegner activity score was 7.1 (95% CI: 6.5–7.6) in the suture tape group and 6.4 (95% CI: 6.2–6.6), indicating patients in both groups returned to similar level of activity following ACLR. Although this difference was found to be statistically significant (p = 0.026), given the overlapping 95% CI and the average change between pre and post-operative Tegner activity scores (suture tape: 0.08, control: 0.27) not meeting the level of minimal detectable change of 1, these findings are unlikely to be clinically relevant.29 A study by Heusdens et al. reported high Marx activity scores (although decreased in comparison to pre-injury scores) with improvements in post-operative pain and functional scores following ACL repair with suture tape reinforcement at 2 year follow-up.24 In contrast, Bodendorfer et al. reported suture augmentation to be significantly correlated with an increased percentage of patients returning to pre-injury level of activity, decreased time to achieve pre-injury activity level, and greater PRO when compared to standard ACLR.15 It is important to note the inclusion of allograft, combined autograft /allograft ACLR grafts, and revision ALCR patients in that study, whereas these factors constituted exclusion criteria in the present study. There were also differences in operative technique between these studies. ACLR grafts were fixed in full extension in the our study, versus 30 degrees of flexion in Bodendorfer et al.15 Previous studies have demonstrated that graft fixation in full extension may avoid overconstraint, graft stretch, and loss of knee extension, whereas fixation in 30 degrees of flexion yields superior restoration of rotational stability of the knee.30 As such, the results in the present study are important and demonstrate the need for additional clinical research to evaluate this popular surgical technique.
Limitations
The present study is not without limitations. The results and conclusions provided are based upon a retrospective review of hamstring autograft ACLR with and without suture tape reinforcement, and thus may be susceptible to the inherent bias of the retrospective process. Neither patients nor surgeons were blinded to operative technique, and thus patient reported outcomes and surgeon reported clinical outcomes may have been subject to bias. Additionally, a post-hoc power analysis revealed the total sample size needed to detect a difference to be 1,290 patients with 430 in the suture tape group, which was larger than the current study.
CONCLUSION
ACLR with hamstring autograft and independent suture tape reinforcement was performed safely with a low rate of complications, graft failure, and reoperation with similar patient reported outcomes, function, and return to sport when compared to hamstring autograft ACLR without suture tape reinforcement at minimum 2-year follow-up.
Supplementary Material
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Primary Location where this investigation was performed: Mayo Clinic, Rochester, MN
REFERENCES
- 1.Tibor L, Chan PH, Funahashi TT, Wyatt R, Maletis GB, Inacio MC. Surgical Technique Trends in Primary ACL Reconstruction from 2007 to 2014. J Bone Joint Surg Am. 2016;98:1079–1089. [DOI] [PubMed] [Google Scholar]
- 2.Magnussen RA, Granan LP, Dunn WR, et al. Cross-cultural comparison of patients undergoing ACL reconstruction in the United States and Norway. Knee Surg Sports Traumatol Arthrosc. 2010;18:98–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Samuelsen BT, Webster KE, Johnson NR, Hewett TE, Krych AJ. Hamstring Autograft versus Patellar Tendon Autograft for ACL Reconstruction: Is There a Difference in Graft Failure Rate? A Meta-analysis of 47,613 Patients. Clin Orthop Relat Res. 2017;475:2459–2468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Consortium M, Spindler KP. Risk Factors and Predictors of Subsequent ACL Injury in Either Knee After ACL Reconstruction: Prospective Analysis of 2488 Primary ACL Reconstructions From the MOON Cohort. Am J Sports Med. 2015;43:1583–1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Conte EJ, Hyatt AE, Gatt CJ Jr., Dhawan A. Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthroscopy. 2014;30:882–890. [DOI] [PubMed] [Google Scholar]
- 6.Kennedy JC, Roth JH, Mendenhall HV, Sanford JB. Presidential address. Intraarticular replacement in the anterior cruciate ligament-deficient knee. Am J Sports Med. 1980;8:1–8. [DOI] [PubMed] [Google Scholar]
- 7.Batty LM, Norsworthy CJ, Lash NJ, Wasiak J, Richmond AK, Feller JA. Synthetic devices for reconstructive surgery of the cruciate ligaments: a systematic review. Arthroscopy. 2015;31:957–968. [DOI] [PubMed] [Google Scholar]
- 8.Bachmaier S, Smith PA, Bley J, Wijdicks CA. Independent Suture Tape Reinforcement of Small and Standard Diameter Grafts for Anterior Cruciate Ligament Reconstruction: A Biomechanical Full Construct Model. Arthroscopy. 2018;34:490–499. [DOI] [PubMed] [Google Scholar]
- 9.Soreide E, Denbeigh JM, Lewallen EA, et al. In vivo assessment of high-molecular-weight polyethylene core suture tape for intra-articular ligament reconstruction: an animal study. Bone Joint J. 2019;101-B:1238–1247. [DOI] [PubMed] [Google Scholar]
- 10.Black AK, Schlepp C, Zapf M, Reid JB 3rd. Technique for Arthroscopically Assisted Superficial and Deep Medial Collateral Ligament-Meniscotibial Ligament Repair With Internal Brace Augmentation. Arthrosc Tech. 2018;7:e1215–e1219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hopper GP, Heusdens CHW, Dossche L, Mackay GM. Posterolateral Corner Repair With Suture Tape Augmentation. Arthrosc Tech. 2018;7:e1299–e1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hopper GP, Heusdens CHW, Dossche L, Mackay GM. Posterior Cruciate Ligament Repair With Suture Tape Augmentation. Arthrosc Tech. 2019;8:e7–e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wilson WT, Hopper GP, Byrne PA, MacKay GM. Anterior Cruciate Ligament Repair with Internal Brace Ligament Augmentation. Surg Technol Int. 2016;29:273–278. [PubMed] [Google Scholar]
- 14.van der List JP, DiFelice GS. Arthroscopic Primary Anterior Cruciate Ligament Repair With Suture Augmentation. Arthrosc Tech. 2017;6:e1529–e1534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bodendorfer BM, Michaelson EM, Shu HT, et al. Suture Augmented Versus Standard Anterior Cruciate Ligament Reconstruction: A Matched Comparative Analysis. Arthroscopy. 2019;35:2114–2122. [DOI] [PubMed] [Google Scholar]
- 16.Irrgang JJ, Anderson AF, Boland AL, et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med. 2001;29:600–613. [DOI] [PubMed] [Google Scholar]
- 17.Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med. 2009;37:890–897. [DOI] [PubMed] [Google Scholar]
- 18.Klein W, Jensen KU. Synovitis and artificial ligaments. Arthroscopy. 1992;8:116–124. [DOI] [PubMed] [Google Scholar]
- 19.Prescott RJ, Ryan WG, Bisset DL. Histopathological features of failed prosthetic Leeds-Keio anterior cruciate ligaments. J Clin Pathol. 1994;47:375–376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Smith PA, Bozynski CC, Kuroki K, Henrich SM, Wijdicks CA, Cook JL. Intra-Articular Biocompatibility of Multistranded, Long-Chain Polyethylene Suture Tape in a Canine ACL Model. J Knee Surg. 2019;32:525–531. [DOI] [PubMed] [Google Scholar]
- 21.Kouloumentas P, Kavroudakis E, Charalampidis E, Kavroudakis D, Triantafyllopoulos GK. Superior knee flexor strength at 2 years with all-inside short-graft anterior cruciate ligament reconstruction vs a conventional hamstring technique. Knee Surg Sports Traumatol Arthrosc. 2019;27:3592–3598. [DOI] [PubMed] [Google Scholar]
- 22.Browning WM 3rd, Kluczynski MA, Curatolo C, Marzo JM. Suspensory Versus Aperture Fixation of a Quadrupled Hamstring Tendon Autograft in Anterior Cruciate Ligament Reconstruction: A Meta-analysis. Am J Sports Med. 2017;45:2418–2427. [DOI] [PubMed] [Google Scholar]
- 23.Desai VS, Anderson GR, Wu IT, et al. Anterior Cruciate Ligament Reconstruction With Hamstring Autograft: A Matched Cohort Comparison of the All-Inside and Complete Tibial Tunnel Techniques. Orthop J Sports Med. 2019;7:2325967118820297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Heusdens CHW, Hopper GP, Dossche L, Roelant E, Mackay GM. Anterior cruciate ligament repair with Independent Suture Tape Reinforcement: a case series with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2019;27:60–67. [DOI] [PubMed] [Google Scholar]
- 25.Noonan BC, Bachmaier S, Wijdicks CA, Bedi A. Independent Suture Tape Reinforcement of Tripled Smaller-Diameter and Quadrupled Grafts for Anterior Cruciate Ligament Reconstruction With Tibial Screw Fixation: A Biomechanical Full Construct Model. Arthroscopy. 2019. [DOI] [PubMed] [Google Scholar]
- 26.Smith PA, Stannard JP, Bozynski CC, Kuroki K, Cook CR, Cook JL. Patellar Bone-Tendon-Bone Autografts versus Quadriceps Tendon Allograft with Synthetic Augmentation in a Canine Model. J Knee Surg. 2019. [DOI] [PubMed] [Google Scholar]
- 27.Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ, International Knee Documentation C. The International Knee Documentation Committee Subjective Knee Evaluation Form: normative data. Am J Sports Med. 2006;34:128–135. [DOI] [PubMed] [Google Scholar]
- 28.Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res (Hoboken). 2011;63 Suppl 11:S208–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Harris JD, Brand JC, Cote MP, Faucett SC, Dhawan A. Research Pearls: The Significance of Statistics and Perils of Pooling. Part 1: Clinical Versus Statistical Significance. Arthroscopy. 2017;33:1102–1112. [DOI] [PubMed] [Google Scholar]
- 30.Debandi A, Maeyama A, Hoshino Y, et al. The Influence of Knee Flexion Angle for Graft Fixation on Rotational Knee Stability During Anterior Cruciate Ligament Reconstruction: A Biomechanical Study. Arthroscopy. 2016;32:2322–2328. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.