

Abstract
A 74-year-old patient presented to the emergency department with acute atraumatic hip pain 9 years after her primary left total hip arthroplasty (THA). Plain radiographic imaging demonstrated lateralisation of the femoral head within the acetabular shell—indicating an issue with the polyethylene liner. The patient required revision of the acetabular component and the femoral head, as well as a new polyethylene liner. A detailed analysis of the components removed was performed by DePuy Synthes Engineering. Between 2009 and 2020, 8 publications have documented 52 cases of liner dissociation with the Pinnacle acetabular component and Marathon polyethylene liner. Various theories have been proposed in the literature as all of these components appear to fail in the same way, with shearing of the locking tabs in the polyethylene liner. In spite of a manufacturer analysis of the components, no root cause was identified as to why the polyethylene liner failed.
Keywords: prosthesis failure, hip prosthesis implantation, orthopaedics, orthopaedic and trauma surgery
Background
Total hip arthroplasty (THA) is a common orthopaedic procedure with over 1 million primary THAs performed between 2003 and 2018 in the UK. Over this time period, 31 410 revisions have been required. The most common causes of revision are documented as aseptic loosening, soft tissue reaction, dislocation/subluxation, pain and infection.1 Polyethylene liner disassociation is noted as a rare cause of prosthetic failure. According to the UK National Joint Registry (NJR), liner dissociation falls under the category of ‘Implant Wear’. This category includes the following mechanisms of failure: wear of the acetabular component; wear of the polyethylene component; and liner dissociation. In total, they account for 0.27 revisions per 1000 prosthesis-years. Only ‘Implant Fracture’ and ‘Head/Socket Size Mismatch’ are more infrequent causes for revision.1
Between 2009 and 2020, 8 publications have documented 52 cases of specific liner dissociation specifically with the Pinnacle acetabular component and Marathon polyethylene liner.2–9 In only one of these publications, a detailed laboratory analysis was performed on the failed component and in that case, no identifiable cause for failure was noted.3 We present a case report of a liner failure accompanied by a detailed engineering laboratory analysis.
Case presentation
A 74-year-old patient presented to the emergency department (ED) in July 2019 with atraumatic left-sided hip pain 9 years after her primary THA surgery. The patient had been trying to lift an object at home when she heard an audible crack from her hip which was associated with acute hip pain and an inability to weight bear.
The patient had a background history of a left-sided THA performed in 2010—the original implants were a 54 mm diameter Pinnacle Acetabular Sector II cup with one superior screw, a 32 mm neutral Marathon liner, a 32 mm+1 cobalt chromium femoral head and a size 4 Summit 12/14 tapered high offset Porocoat femoral stem. She also had simultaneous bilateral total knee replacements performed in July 2014 and a right THA performed in March 2017. She was then followed up regularly throughout 2014 to 2017 on an annual basis. Prior to the liner failure she did not require any walking aids and had painless hips.
In the ED, radiographs demonstrated lateralisation of the left femoral head within the acetabular shell (figure 1).
Figure 1.
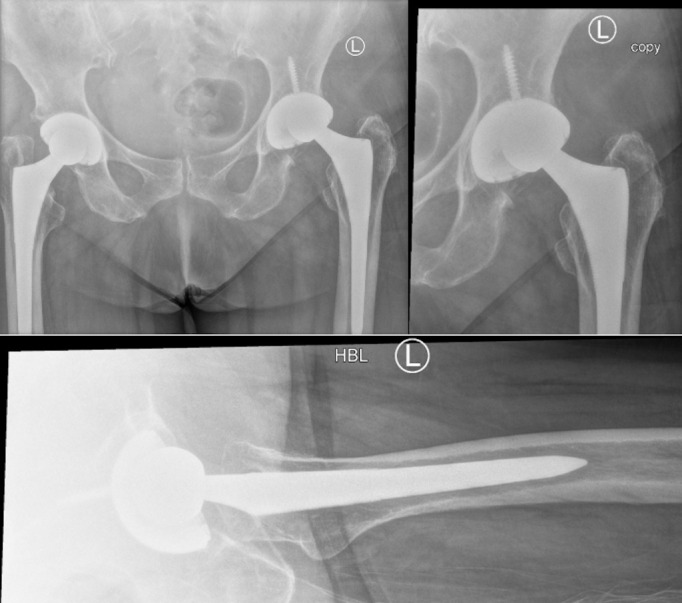
Radiograph demonstrating lateralisation of the left femoral head.
Postoperative imaging confirmed satisfactory positioning of the femoral and acetabular components (figure 2). Since the revision THA, the patient has been regularly followed up in the outpatient department, most recently at 1 year post revision, with no further complaint.
Figure 2.

Post revision radiograph.
Investigations
The patient underwent an anteroposterior and lateral pelvic X-ray on admission to the hospital. She also underwent a pelvic X-ray post revision to confirm satisfactory position of the new components.
The explanted acetabular shell, liner and femoral head were then sent to the DePuy Synthes Engineering laboratory for analysis to identify a root cause for the failure. The manufacturing records were reviewed for the failed components and no anomalies or deviations were noted. On analysis of the femoral head, the official report commented that “a Goldberg taper score of 3 was given, stripe wear noted, defined scratches of 1 or 2 identified and 25%–49% of fine scratches were located on the bearing surface”.
On analysis of the liner there was “no impingement or malalignment noted”. The report also noted “on the bearing surface edge wear was seen, a hood score for abrasion was visible, 3–5 deep scratching noticed and a wear scar was identified”.
The analysis of the acetabular shell does not identify any reason for failure. There was good bone incorporation noted on the outer shell. The official report does note that there was “damage to taper and inner dome” suggesting “articulation of the head against these surfaces, most likely to have occurred post-liner disassociation”. Unfortunately, no product defect was identified on any of the three components that make up the total hip replacement, and therefore no root cause was found as to why they failed.
Differential diagnosis
Based on the position of the femoral head on the admission images, the differential diagnoses included either dissociation or fracture of the polyethylene liner.
Treatment
Surgical management included revision of the acetabular and femoral head components, as well as the implantation of a new polyethylene liner. Intraoperatively, dissociation of the polyethylene liner was noted (figure 3). All other components were stable on examination. On inspection, three of the six anti-rotation locking tabs were sheared away (figure 4).
Figure 3.
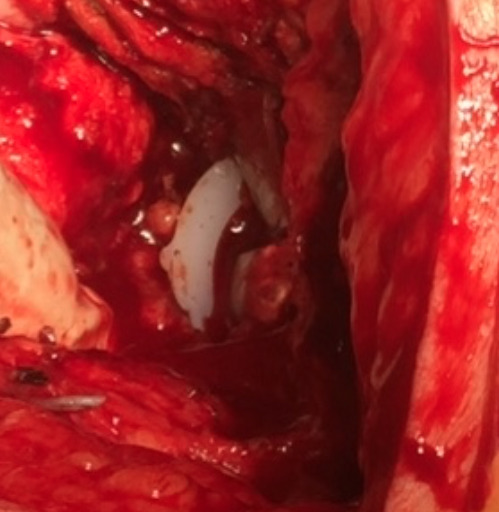
Intraoperative image of dissociated liner.
Figure 4.
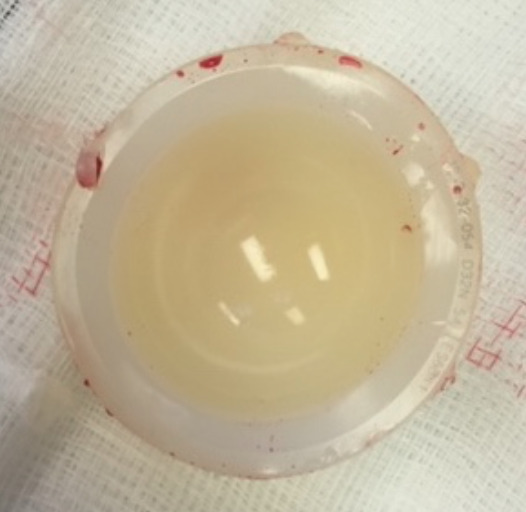
Explanted liner.
Outcome and follow-up
The patient has had 1 year follow-up post revision without any issues. This case report contributes to the literature surrounding polyethylene liner dissociation with the DePuy Synthes Pinnacle cup. We believe that due to the high number of cases reported in the literature, ‘Liner Dissociation’ should be listed as a separate indication for revision in the National Joint Registry and not included in ‘Implant Wear’. This would allow for better transparency about the true incidence of liner dissociation. Further investigation should be done to determine the reasons why this particular modular system has failed consistently, in the same way, over a long period of time in multiple geographical areas.2–9 This case is only the second in the literature to include a manufacturer analysis of the failed components. In order to understand the mechanisms behind this complication, future reported cases of liner dissociation should undergo detailed post-explant manufacturer analysis as in the case reported here.
Discussion
The DePuy Synthes Pinnacle acetabular system is a modular one which, by design, brings a risk of dissociation. It is compatible with polyethylene, metal or ceramic liners. Liner dissociation has been an issue for multiple manufacturers using this modular design. It was a specific problem with the early Harris-Galante hips.10 This was then addressed with the Duraloc design.11 Langdown et al identified incomplete seating of metal-back ceramic liners in 19 cases (16.4% of their cohort) using the Trident acetabular system however only one of those required revision due to complete spin-out and this was attributed to surgical error, not implant issues.12 A 2019 case report by Parkar et al was the first one published in the literature identifying polyethylene liner dissociation in an R3 (Smith & Nephew) acetabular component.13 Gwynne-Jones and Memon recently published a retrospective study of 961 hips split between the DePuy Synthes Pinnacle system and the R3 system and found a higher rate of polyethylene liner dissociation in the Pinnacle system. They attribute it to a specific design problem with the Pinnacle cup than an issue with third generation modular acetabular design.14
Multiple theories have been proposed in the literature to explain why certain polyethylene liners may fail in this way. These include the change from an ultra-high molecular weight polyethylene liner to a highly cross-linked polyethylene liner which has introduced an intermediate dose of radiation that is known to decrease fatigue strength.8 9 The new design has also resulted in decreased pull-out and lever-out strength.7–9 Femoral neck impingement on the polyethylene liner and edge loading may produce fatigue of the locking mechanism.4 6 The detailed analysis of the liner performed by DePuy Synthes indicated no malalignment or impingement was present 9 years after the index procedure. On that basis, we think it is not likely to be a contributing factor to failure in this case.
Of note, three of the six locking tabs were sheared away from the explanted polyethylene liner. This failure of three locking tabs appears to be a common finding in the literature.2 3 7 9 The manufacturer analysis identified bearing surface edge wear in the liner. We can speculate that this surface edge wear may have been caused by subluxation of the femoral head which may have caused eccentric loading of the liner, resulting in shearing of the anti-rotation tabs and failure of the component. However we do not know why there would have been subluxation of the femoral head in the first instance.
Various surgical factors have been proposed which may also contribute to early liner dissociation. These include the surgical approach used or the imperfect seating of the liner at the time of implantation.7 The six cases reported by Singleton et al were all originally performed via a lateral approach.7 Kagan et al used an anterior approach in the three failed cases.8 Of the six cases reported by Memon et al, five were performed via the direct lateral approach and one via the posterior approach.9 Our patient was performed via the posterior approach. Due to liner dissociation occurring with a variety of different approaches, we think this is unlikely to be a contributing factor towards their failure. It is standard practice for the operating surgeon to check the stability of the liner on implantation into the shell and there were no recorded concerns about liner seating during the primary procedure. If incorrect liner seating was a contributing factor, we would have expected it to fail before 9 years. It may be one or a combination of any of these factors which has contributed to the liner failure in this particular case.
Learning points.
Polyethylene liner failure is more common than was previously realised.
If a patient presents with hip pain and their pelvic X-ray demonstrates lateralisation of the femoral head in the acetabular component, then it is likely due to polyethylene liner failure as opposed to a fracture of the liner.
This injury requires, at a minimum, revision of the acetabular and femoral head components.
Polyethylene liner failure should be removed from the ‘Implant Wear’ category in National Joint Registries into its own specific category.
Footnotes
Contributors: DK - wrote first draft of paper. GAS - edited paper. JH - final review and approval of paper. PO - performed surgical case and approval of paper.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Registry UNJ NJR 16th annual report, 2019. [PubMed] [Google Scholar]
- 2.Mesko JW Acute liner disassociation of a pinnacle acetabular component. J Arthroplasty 2009;24:815–8. 10.1016/j.arth.2008.03.010 [DOI] [PubMed] [Google Scholar]
- 3.Mayer SW, Wellman SS, Bolognesi MP, et al. Late liner disassociation of a pinnacle system acetabular component. Orthopedics 2012;35:e561–5. 10.3928/01477447-20120327-29 [DOI] [PubMed] [Google Scholar]
- 4.Gray CF, Moore RE, Lee G-C. Spontaneous dissociation of offset, face-changing polyethylene liners from the acetabular shell: a report of four cases. J Bone Joint Surg Am 2012;94:841–5. 10.2106/JBJS.K.00506 [DOI] [PubMed] [Google Scholar]
- 5.Yun A, Koli EN, Moreland J, et al. Polyethylene liner dissociation is a complication of the DePuy pinnacle cup: a report of 23 cases. Clin Orthop Relat Res 2016;474:441–6. 10.1007/s11999-015-4396-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Napier RJ, Diamond O, O'Neill CKJ, et al. The incidence of dissociated liners in 4,751 consecutive total hip arthroplasties using pinnacle polyethylene acetabular liners. Hip Int 2017;27:537–45. 10.5301/hipint.5000512 [DOI] [PubMed] [Google Scholar]
- 7.Singleton N Polyethylene liner dissociation with the Depuy pinnacle cup: a report of 6 cases. OPROJ 2018;3:293–300. 10.31031/OPROJ.2018.03.000573 [DOI] [Google Scholar]
- 8.Kagan R, Anderson MB, Peters C, et al. Pinnacle polyethylene liner dissociation: a report of 3 cases. Arthroplast Today 2018;4:441–6. 10.1016/j.artd.2018.08.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Memon AR, Gwynne-Jones D. Polyethylene liner dissociation with the pinnacle acetabular component: should we be concerned? Arthroplast Today 2020;6:5–8. 10.1016/j.artd.2019.12.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.González della Valle A, Ruzo PS, Li S, et al. Dislodgment of polyethylene liners in first and second-generation Harris-Galante acetabular components. A report of eighteen cases. J Bone Joint Surg Am 2001;83:553–9. 10.2106/00004623-200104000-00010 [DOI] [PubMed] [Google Scholar]
- 11.Tradonsky S, Postak PD, Froimson AI, et al. A comparison of the disassociation strength of modular acetabular components. Clin Orthop Relat Res 1993;296:154???160–60. 10.1097/00003086-199311000-00028 [DOI] [PubMed] [Google Scholar]
- 12.Langdown AJ, Pickard RJ, Hobbs CM, et al. Incomplete seating of the liner with the trident acetabular system: a cause for concern? J Bone Joint Surg Br 2007;89:291–5. 10.1302/0301-620X.89B3.18473 [DOI] [PubMed] [Google Scholar]
- 13.Parkar AAH, Sukeik M, El-Bakoury A, et al. Acetabular liner dissociation: a case report and review of the literature. Sicot J 2019;5:31. 10.1051/sicotj/2019025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gwynne-Jones DP, Memon A. Acetabular liner dissociation: a comparative study of two contemporary Uncemented acetabular components. Arthroplast Today 2020;6:354–9. 10.1016/j.artd.2020.04.016 [DOI] [PMC free article] [PubMed] [Google Scholar]