

Abstract
Background:
Patients who undergo anterior cruciate ligament (ACL) reconstruction (ACLR) can have a persistent postoperative pivot shift. Performing lateral extra-articular tenodesis (LET) concurrently has been proposed to address this; however, LET femoral fixation may interfere with the ACLR femoral tunnel, which could damage the ACL graft or its fixation.
Purpose:
To evaluate the safe maximum implant or tunnel depth for a modified Lemaire LET when combined with ACLR anteromedial portal femoral tunnel drilling and to validate the safe LET drilling angles to avoid conflict with the ACLR femoral tunnel.
Study Design:
Descriptive laboratory study.
Methods:
Twelve fresh-frozen cadaveric knees were used. With each knee at 120° of flexion, an ACLR femoral tunnel in the anteromedial bundle position was created arthroscopically via the anteromedial portal using a 5-mm offset guide, a guide wire, and an 8-mm reamer, which was left in situ. A modified Lemaire LET was performed using a 1 cm-wide iliotibial band strip harvested with the distal attachment intact, to be fixed in the femur. The desired LET fixation point was identified with an external aperture 10 mm proximal and 5 mm posterior to the fibular collateral ligament’s femoral attachment, and a 2.4-mm guide wire was drilled, aiming at 0°, 10°, 20°, or 30° anteriorly in the axial plane and at 0°, 10°, or 20° proximally in the coronal plane (12 different drilling angle combinations). The relationship between the LET drilling guide wire and the ACLR femoral tunnel reamer was recorded for each combination. When a collision with the femoral tunnel was recorded, the LET wire depth was measured.
Results:
Collision with the ACLR femoral tunnel occurred at a mean LET wire depth of 23.6 mm (range, 15-33 mm). No correlation existed between LET wire depth and LET drilling orientation (r = 0.066; P = .67). Drilling angle in the axial plane was significantly associated with the occurrence of tunnel conflict (P < .001). However, no such association was detected when comparing the drilling angle in the coronal plane (P = .267).
Conclusion:
Conflict of LET femoral fixation with the ACLR femoral tunnel using anteromedial portal drilling occurred at a mean depth of 23.6 mm but also at a depth as little as 15 mm, which is shorter than most implants. When longer implants or tunnels are used, the orientation should be directed at least 30° anteriorly in the axial plane to minimize the risk of tunnel conflict, bearing in mind the risk of joint violation.
Clinical Relevance:
This study provides important information for surgeons performing LET in combination with ACLR anteromedial portal femoral tunnel drilling regarding safe femoral implant or tunnel length and orientation.
Keywords: anterior cruciate ligament, lateral extra-articular tenodesis, anterolateral ligament tunnel conflict
Residual knee anterolateral rotational instability (ALRI) after anterior cruciate ligament (ACL) reconstruction (ACLR) is correlated with poorer functional outcomes and a higher risk of graft failure.1,12 Persisting ALRI has been shown to occur after even clinically successful ACLR in patients lacking symptoms after surgery.18 There is clinical evidence that a combined ACLR with an anterolateral complex procedure, either a lateral extra-articular tenodesis (LET) or an anterolateral ligament reconstruction (ALLR), can reduce the prevalence of residual pivot shifts,7,20,24,25 especially in chronic or revision ACLR.3,16,27 Consequently, more combined anterolateral complex procedures with ACLRs are now being performed, with the aim of achieving better clinical outcomes.6,8,28
Intertunnel relationships are an important consideration when drilling multiple tunnels in proximity. This has been studied, and recommendations have been made, to avoid tunnel conflict in combined ACLR and posterolateral corner reconstruction.14,19 Similarly, there is concern regarding femoral tunnel conflict when anterolateral complex procedures are performed concurrently with ACLR, but there has been little study of this. Such a conflict would risk damaging the ACL graft and/or its fixation. A cadaveric study23 has reported tunnel conflict in as much as 81% of combined ACLR and ALLR procedures, depending on the ALLR tunnel orientation.
The type of implants used in anterolateral complex procedures, the drilling angle, and the depth requirement of the implant can all affect the risk of ACLR femoral tunnel conflict. A few studies11,21–23 have considered this issue and have recommended that the LET or ALLR tunnel should be strategically oriented to avoid tunnel conflict. The reality is that there is little guidance for surgeons specifically on safe LET implant or tunnel orientation when performed with ACLR. Implant or tunnel depth is also critical but has been less studied.
The aim of this study was to establish, when performing a modified Lemaire LET technique,17,29 a safe femoral guide wire–simulated tunnel drilling depth and orientation to avoid interfering with the ACLR femoral tunnel using anteromedial portal drilling. The modified Lemaire LET was chosen as it is popular and has shown proven biomechanical and clinical benefits.5,7,29
Methods
We obtained 12 fresh-frozen, cadaveric, total knee joint specimens that included the proximal half of the tibia and fibula and the distal half of the femur with surrounding soft tissues from a commercial source (MedCure). All specimens were accredited by the American Association of Tissue Banks regarding their standards. There were 6 White male and 6 White female specimens, with a mean age of 69 years (range, 61-88 years). All specimens were thawed at room temperature for 24 hours before the experiments.
Experiment Setup
The distal femoral shaft of the cadaveric knee was immobilized in a leg holder that enabled knee flexion, with the proximal tibia and fibula free to move. The leg holder with the mounted knee specimen was placed on a dissection table for arthroscopic surgery. A gravity irrigation hand-pump system was used to simulate arthroscopic conditions. This setup (Figure 1) allowed for simulated ACLR surgery to be performed.
Figure 1.
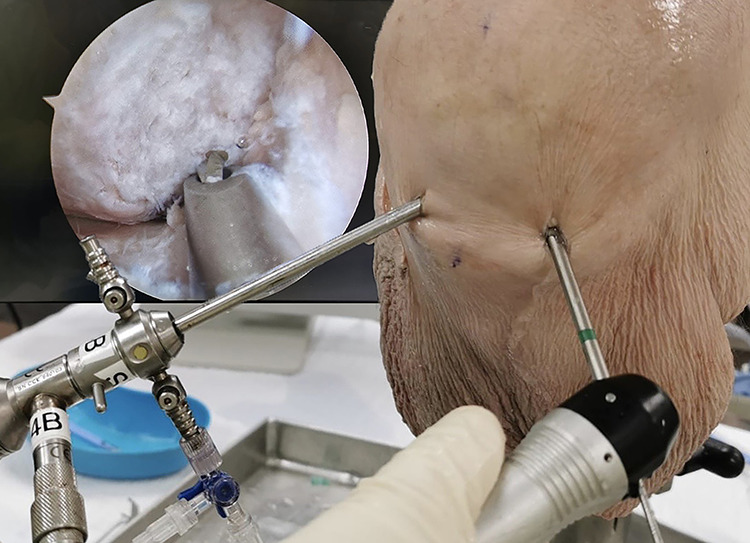
Arthroscopy setup and arthroscopic view of ACLR femoral guide wire drilling via the anteromedial portal on a cadaveric right knee. ACLR, anterior cruciate ligament reconstruction.
Femoral Tunnel Preparation and Modified Lemaire LET
In each specimen, knee arthroscopy and drilling of the ACLR femoral tunnel via the anteromedial portal were performed just as in clinical practice. Two standard parapatellar portals were made. Arthroscopic debridement of the native ACL and intercondylar notch preparation was performed with a shaver and electrocautery. Using a 5-mm posterior femoral condyle offset guide to keep the tunnel suitably deep or posterior in the intercondylar notch, and with the knee at 120° of flexion, a 2.4-mm guide wire was drilled in the desired position (clockface positions of 10 o’clock for the right knee and 2 o’clock for the left) within the anteromedial bundle footprint of the ACL. Without removing the guide wire, an 8 mm--diameter femoral tunnel was reamed to a depth of 30 mm. This was done to simulate the femoral tunnel depth used in clinical practice to undertake an ACL graft with a cortical button or an interference screw femoral fixation. An 8-mm diameter was chosen, as this is the average tunnel size used for a 4-strand hamstring graft in the lead authors’ institution. The reamer was kept in situ within the femoral tunnel when the modified Lemaire LET was performed.
The LET procedure without the final fixation was then performed with modification of the Lemaire technique.17 A lateral skin incision was made and the iliotibial band (ITB) was exposed. A 1 × 10–cm strip of the ITB was harvested, leaving intact its distal attachment to the Gerdy tubercle. This created a “window” in the ITB, which allowed identification of the femoral graft fixation point. The fibular collateral ligament (FCL) and its femoral insertion on the lateral femur were then identified. The LET femoral fixation point was chosen to be 10 mm proximal and 5 mm posterior to the femoral insertion of FCL, as shown in Figure 2.29
Figure 2.

The LET femoral insertion point (forceps tip) was identified 10 mm proximal and 5 mm posterior to the femoral insertion (asterisk) of the fibular collateral ligament (red line). LET, lateral extra-articular tenodesis.
Before drilling the LET guide wire from lateral to medial, the transepicondylar axis was identified by palpation and taken to be the neutral orientation in all planes (Figure 3A). For drilling from posterior to anterior, angles were defined by aligning the guide wire at the desired angle relative to the transepicondylar axis of the femur in the axial plane (Figure 3B). Similarly, the transepicondylar axis was taken as the reference line for drilling from distal to proximal in the coronal plane of the femur (Figure 3C). A goniometer was used to guide each of the drilling angles, with both the surgeon (D.Y.H.L.) and assistant (M.Z.) in agreement regarding the angles. A 2.4-mm guide wire was drilled at the identified LET femoral fixation point. By varying the orientation of the guide wire, the relationship between the guide wire and ACLR femoral tunnel reamer was able to be recorded. The LET drilling angles were in combinations of 0°, 10°, 20°, or 30° anteriorly in the axial plane and 0°, 10°, or 20° proximally in the coronal plane (12 possible combinations).
Figure 3.

LET drilling orientation demonstrated with regard to the coronal plane (blue) and axial plane (yellow) of the femur. The red solid line denotes the guide wire projection on the respective planes, and the black dotted line denotes the transepicondylar axis. LET drilling shown at (A) 0° axial and 0° coronal, (B) 30° axial and 0° coronal, and (C) 20° axial and 10° coronal. LET, lateral extra-articular tenodesis.
For this experiment, it was decided to only drill the 2.4-mm guide wire rather than to create a wider tunnel with a drill or reamer. With multiple drills of a wider diameter, cavitation of the bone would occur, affecting stability of the reamer in the ACLR femoral tunnel and the accuracy of subsequent guide wire drilling. Furthermore, often in described modified Lemaire techniques, graft fixation utilizes a suture anchor, and the recommended diameter of tunnel preparation for such devices is 2.4 mm or only slightly more.
Measurements
The first drilling orientation performed was 0° in both axial and coronal planes. For each drilling orientation, 3 mutually exclusive relationships between the LET drilling guide wire and ACLR femoral tunnel reamer, as illustrated in Figure 4, were recorded: no conflict, conflict, or critical collision. No conflict was defined as when the guide wire was drilled through to the opposite cortex smoothly, without touching the ACLR femoral tunnel reamer. Conflict was deemed to have occurred when the guide wire hit the reamer in the femoral ACLR tunnel, deflected, and passed through to the medial femur. Critical collision occurred when advancement of the guide wire was completely blocked by the reamer, suggesting that the guide wire hit the midpoint of the reamer and so could not slide to one side or the other. When a critical collision was noted, the depth of the guide wire from the lateral femoral cortex to the reamer was calculated by comparing with a guide wire of the same length placed on the lateral femoral cortex. The drilling of the guide wire was repeated at the 11 other combinations of the LET drilling angles, and the relationship between the guide wire and the ACLR femoral tunnel reamer was recorded for all 12 orientations. The same procedure was repeated for all 12 cadaveric specimens. The risk of potential tunnel conflict to any degree in each orientation was the sum of the conflict and critical collision rate based on the measurement from 12 specimens.
Figure 4.
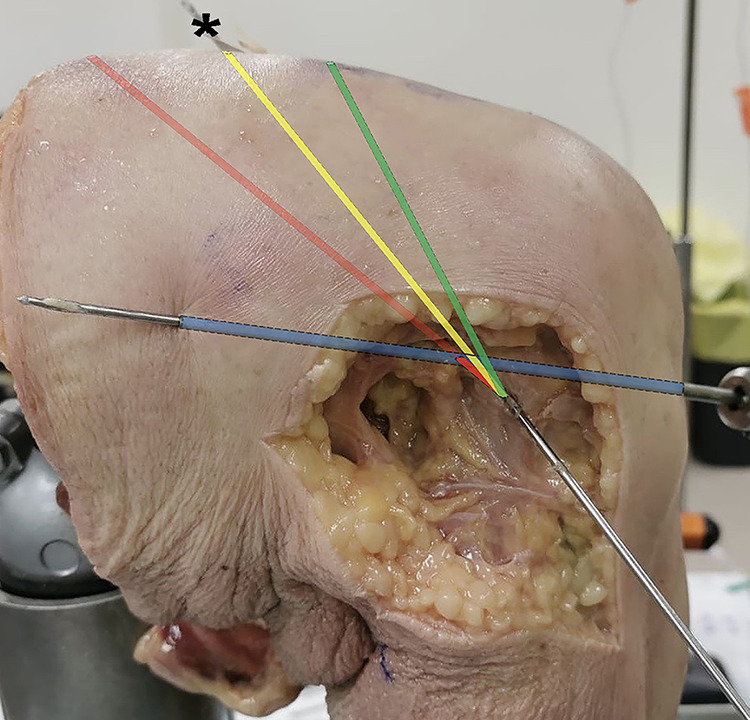
Illustration of the relationship between the LET drilling guide wire and ACLR femoral tunnel reamer (blue) with different drilling trajectories: no conflict (green), conflict (yellow), or critical collision (red). In this illustration, there is conflict but the wire passes through and is able to exit the opposite cortex and skin as seen (asterisk). ACLR, anterior cruciate ligament reconstruction; LET, lateral extra-articular tenodesis.
Statistical Analysis
Statistical analyses were performed using SPSS (IBM Corp). The risk of potential tunnel conflicts at different drilling angels in the coronal or axial plane was compared using the Cochran Q test. The Pearson correlation coefficient was calculated for the LET wire depth versus LET drilling angles, as well as for the risk of potential tunnel conflict versus LET drilling angles. A P value of <.05 was considered statistically significant.
Results
Table 1 summarizes the relationship between the LET drilling guide wire and ACLR femoral tunnel reamer at the different LET drilling orientations. Also shown are the LET wire depths when a critical collision occurred. The detailed results for all 12 drilling orientations in the 12 specimens are tabulated in Appendix Table A1. The risk of potential tunnel conflict was 83.3% to 100% when the drilling angle was directed at 0° in the axial plane. The LET wire depth ranged from 15 to 33 mm when it had a critical collision with the ACLR reamer. The mean LET wire depth was 23.6 mm (95% CI, 22.2-25.0 mm). No correlation existed between the LET wire depth and the LET drilling orientations (r = 0.066; P = .67).
Table 1.
Relationship Between the LET Femoral Drilling Guide Wire and the ACLR Femoral Tunnel Reamer at Different LET Drilling Angles for the 12 Study Specimensa
| LET Drilling Angle Combination | Relationship to ACLR Femoral Tunnel Reamer, n (%) of Specimens | Risk of Potential Tunnel Conflict, % | LET Wire Depth at Critical Collision, mm Mean (Range) |
|||
|---|---|---|---|---|---|---|
| Axial/Ant | Coronal/Prox | No Conflict | Conflict | Critical Collision | ||
| 0° | 0° | 0 (0) | 2 (16.7) | 10 (83.3) | 100.0 | 24 (15-30) |
| 0° | 10° | 0 (0) | 1 (8.3) | 11 (91.7) | 100.0 | 25 (17-33) |
| 0° | 20° | 2 (16.7) | 0 (0) | 10 (83.3) | 83.3 | 25 (17-32) |
| 10° | 0° | 6 (50.0) | 1 (8.3) | 5 (41.7) | 50.0 | 21 (18-25) |
| 10° | 10° | 3 (25.0) | 3 (25.0) | 6 (50.0) | 75.0 | 23 (15-30) |
| 10° | 20° | 6 (50.0) | 3 (25.0) | 3 (25.0) | 50.0 | 21 (20-23) |
| 20° | 0° | 11 (91.7) | 1 (8.3) | 0 (0) | 8.3 | — |
| 20° | 10° | 10 (83.3) | 1 (8.3) | 1 (8.3) | 16.7 | 18 |
| 20° | 20° | 10 (83.3) | 2 (16.7) | 0 (0) | 16.7 | — |
| 30° | 0° | 12 (100) | 0 (0) | 0 (0) | 0 | — |
| 30° | 10° | 12 (100) | 0 (0) | 0 (0) | 0 | — |
| 30° | 20° | 12 (100) | 0 (0) | 0 (0) | 0 | — |
aDashes indicate no occurrence of critical collision. Ant, anterior; LET, lateral extra-articular tenodesis; Prox, proximal.
The risk of potential tunnel conflict differed depending on the drilling angle, especially in the axial plane. The drilling angle in the axial plane was significantly associated with the occurrence of tunnel conflict (P < .001). The risk of potential tunnel conflict fell when the drilling angle was increased in the axial plane by directing it more anteriorly (r = −0.711; P < .001). There was no difference in the risk of potential tunnel conflict when comparing the drilling angle in the coronal plane (P = .267).
Discussion
This is the first cadaveric study of a modified Lemaire LET in combination with ACLR using anteromedial portal femoral tunnel drilling that evaluated safe drilling orientations and depths of the LET implant or tunnel. There are 2 valuable findings of the present study for practicing surgeons. First, the safe maximum drilling depth of a modified Lemaire LET was as little as 15 mm, with a mean depth of only 23.6 mm when critical collision occurred. Therefore, any technique needing an implant or tunnel deeper than 15 mm risks tunnel conflict, which could damage the ACL graft and disrupt the fixation. If a suspensory fixation is used, complete loss of ACL graft fixation could occur. Second, when an LET implant or tunnel deeper than 15 mm is required, the guide wire drilling angle in the axial plane should be no less than 30° anteriorly. This brings the risk of potential tunnel conflict to nearly zero. This must be carefully balanced with the risk of damage to the trochlear articular surface by the surgeon.
The importance of tunnel conflict has been studied in multiligament knee surgery. Since femoral tunnel(s) in posterolateral reconstruction techniques are reasonably close to that of the modified Lemaire LET and ALLR, studies14,19 of tunnel conflict in this scenario are relevant to some degree to the present study. For combined ACLR and posterolateral corner reconstruction surgery, Kim et al14 proposed that the safe angles for creation of FCL and popliteal tendon tunnels with an ACLR femoral tunnel present are 20° anterior in the axial plane and 10° proximal in the coronal plane to reduce the risk of tunnel conflict.
In the present study, the femoral fixation point for the modified Lemaire LET was chosen to be a point 10 mm proximal and 5 mm posterior to the lateral epicondyle. At this point in the original description of the technique, Lemaire created a bony tunnel for graft fixation.17 Kittl et al15 reported that a graft, having been passed deep to the FCL and fixed to an area proximal to the lateral femoral epicondyle, would have less strain and exhibit better isometry during knee motion. Indeed, 1 of the points tested was previously described as the Lemaire point. In a biomechanical study, Katakura et al13 compared 3 femoral insertion sites for anterolateral complex procedures and concluded that this Lemaire point, when used for femoral fixation, was the most effective in reducing ALRI. This point also coincides with the femoral origin of the anterolateral ligament first described by Dodds et al.4 Because the points of graft fixation on the femur are the same for the anatomical ALLR and modified Lemaire LET procedures, the findings of the present study are relevant to ALLR as well as to the LET procedure we studied.2,29
Jaecker et al11 investigated tunnel convergence of femoral tunnels for ACLR with 2 LET surgical techniques (Lemaire and MacIntosh). In the MacIntosh procedure, femoral graft fixation is more proximal to the lateral femoral epicondyle. Not surprisingly, the authors reported much more frequent tunnel conflict (70% of cases) with the Lemaire LET in which a 6-mm tunnel was drilled in the midaxial plane (0° in the axial plane in the present study) and 30° proximally in the coronal plane. This correlates well with the finding in the present study of high tunnel conflict risk when drilling at 0° in the axial plane. It is worth noting that a more proximal graft fixation greatly reduces the risk of tunnel conflict but at the price of a larger wound.
In a clinical study analyzing postoperative computed tomography (CT) scans on 52 patients having the Lemaire LET plus ACLR, Perelli et al21 recommended a femoral tunnel inclination of at least 20° anteriorly in the axial plane for the modified Lemaire LET to avoid interference with the ACLR femoral tunnel. There was invariably tunnel conflict with an LET tunnel inclination of less than 15° in the axial plane, which confirms the importance of the drilling angle in the axial plane emphasized by the present study. However, we suggest that an angle of 30° is the safest and that drilling a tunnel at 20° can still result in tunnel conflict. Smeets et al22 performed a CT analysis of tunnel convergence during combined ACLR and ALLR in cadavers. They reported that tunnel conflict occurred in 87% of cases when the ALLR tunnel was drilled at 0° coronal and 20° axial orientation and in 47% of cases when drilled at 30° coronal and 30° axial orientation. This too agrees with the present study’s finding that increasing the axial plane drilling angle reduces the risk of potential tunnel conflict.
In another study, Smeets et al23 simulated ALLR 4.5-mm femoral tunnel drilling at different angles using postoperative CT scans in patients who had undergone ACLR to study tunnel conflict. They again found significantly increased risk of tunnel collision when the ALLR femoral tunnel was drilled at 0° in the axial plane. They also reported that by aiming the drill at 0° coronal and 40° axial orientation, tunnel collision was avoided. While this information is useful advice for surgeons, it does not replicate an actual surgery, as radiological landmarks were used, whereas a surgeon relies on the anatomic landmarks available during surgery. Smeets et al23 also reported that drilling the ACLR femoral tunnel via the anteromedial portal increased the risk of tunnel collision compared with transtibial tunnel drilling, owing to the resultant angle of the ACLR femoral tunnel. In the present study, drilling of the ACLR femoral tunnel via the anteromedial portal was used, as it is a popular technique26 and it is our practice to do so.
Smeets et al,22 in their cadaveric study mentioned earlier, reported that in specimens where tunnel convergence occurred, the mean ALLR tunnel depth was 15.9 mm (95% CI, 13.6-18.1 mm). This was independent of the tunnel drilling orientation. A mean LET wire depth of 23.6 mm was found in the present study. The discrepancy may be partially because the estimations of ALLR fixation point and the depth was measured on CT images by Smeets et al22, whereas measurements were made directly on the cadaveric specimens in the present study.
The risk of tunnel conflict is further increased when larger diameter LET femoral implants or tunnels are used. A guide wire of only 2.4 mm was used in the present study, as our technique of LET in practice involves using a suture anchor for graft fixation with an implant requiring a short 2.4-mm starting tunnel. To illustrate this, the size and tunnel preparation requirements for commonly used suture anchors are tabulated in Appendix Table A2. While the choice of using a 2.4-mm guide wire for drilling is reflective of many techniques, it is important to note that others (eg, using an interference-fit screw) demand larger diameter tunnels, which will inevitably have higher rates of tunnel conflict than reported in the present study. Based on the present study and the other studies11,21–23 referenced earlier, for techniques of modified Lemaire and ALLR requiring a deeper tunnel, it is strongly advised that the surgeon increase the axial plane drilling angle anteriorly to more than 30° to avoid tunnel collision. Great care is needed to avoid entering the knee joint via the trochlea. Alternatively, surgeons could also choose a suitable suture anchor or staple fixation with shorter depth and smaller diameter.
It is pertinent to note that the length of most interference-fit screws’ exceeds 15 mm, as do many suture anchor devices. Of course, a safe option is to change the technique to avoid such a large diameter or deep tunnel. One of the authors of the current study changed from using interference-fit screws for fixation of ITB grafts to using an anchor, owing to experiences of tunnel conflict.29 Suture anchors with a tunnel depth of not more than 15 mm are available and can provide adequate fixation. If suture anchors of more than 15-mm length are used, then increasing the axial drilling angle will increase the safety of their use. The modified Lemaire LET with a graft tension of only 20 N can restore the rotational kinematics of an ACL-deficient knee to the intact state without increasing articular contact pressures, as evidenced by Inderhaug et al.9,10 The graft must not be overtensioned—the graft in LET should be thought of as a simple check rein, as in medial patellofemoral ligament reconstruction. In a cadaveric study, 40 N tension on the graft was found to increase tibiofemoral contact pressures, whereas 20 N did not.9 While no prior studies have compared the biomechanical properties of the various implants used in the context of anterolateral complex procedures of the knee, it is likely, in view of the relatively low graft tensioning needed, that suture anchor fixation is adequate.
To help reduce the risk and potential complications of tunnel conflict when drilling the femoral tunnel for LET or ALLR, another option is to do this part of the operation before passing and fixing the ACL graft. This can be achieved by either leaving the ACLR femoral tunnel reamer in its tunnel (as in the present study) or by viewing the femoral tunnel arthroscopically while the LET or ALLR tunnel is being reamed.
There are limitations to the present study. A 2.4-mm guide wire was used to simulate the drilling of the LET tunnel. The reasons for this choice are discussed earlier in the text. The ACLR femoral tunnel size of 8 mm was chosen, as it was the average tunnel size used in the lead authors’ institution and the minimum graft diameter found to reduce ACLR failure. If a larger diameter ACLR femoral tunnel is used, such as using a bone-tendon-bone or quadriceps tendon graft, the safe LET implant or tunnel depth can be further reduced. Hence, caution is needed in extrapolating our results to surgical techniques employing bigger diameter implants or tunnels in which the risk of tunnel conflict is even higher and is still significant, even with changing the drilling angle to more than 30° anteriorly in the axial plane.
Second, the size of the cadaveric femoral specimen will affect the likelihood of tunnel conflict. The small sample size from the present study prevented it from deriving a meaningful regression model, whereas dichotomization of the sample based on femoral size would be arbitrary and does not reflect the population. Therefore, using the minimal value of the tunnel depth from the whole sample, independent of the femoral size, would be more appropriate. We also acknowledge racial variation in anatomy, as the cadavers we used were White. As such, surgeons should still be vigilant when operating on small patients and should not take the recommended values as being necessarily correct for their patient in question. The recommendations will help minimize the risk of tunnel conflict, although not eradicate it.
Another limitation was that repeated drilling at the same LET femoral entry point may weaken and widen the cortex, even with the narrow 2.4-mm guide wire, thus causing errors. This effect was minimized by using guide wire alone and not using wider drills.
Although care was taken to reproduce normal clinical practice, the study setup in which the proximal femoral bone was visible might have helped in the judgment of drilling orientations. In actual practice, especially with obese patients when anatomical landmarks are more difficult to palpate, achievement of accurate drilling orientations may be more difficult.
Finally, the present study used an anteromedial portal approach for ACLR femoral tunnel drilling. The results are relevant to this technique and less so to femoral ACLR tunnel drilling with other techniques (eg, transtibial or outside-in). Instead, an outside-in technique of femoral tunnel drilling can plan the tunnel trajectories and avoid tunnel conflict. Changing the location of the anteromedial portal or the degree of knee flexion during ACLR femoral tunnel drilling may also affect the safe LET implant or tunnel depth and orientation. However, the present study has taken into account these variations and proposed the safe depth and orientation with a safety margin.
Conclusion
LET femoral fixation poses risk of conflict with the ACLR femoral tunnel created via the anteromedial portal, and the risk can be abated by using an implant or tunnel of not more than 15 mm in length. When longer implants are used, the orientation of the femoral tunnel should be directed at least 30° anteriorly in the axial plane to minimize risk of tunnel conflict.
Appendix
Table A1.
Results for All 12 LET Drilling Angles in All Study Specimensa
| LET Drilling Angle Combination | Specimen No. | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Axial/Ant | Coronal/Prox | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| 0° | 0° | CC (24) |
CC (27) |
CC (30) |
C | CC (18) |
CC (18) |
CC (15) |
CC (30) |
CC (24) |
CC (25) |
C | CC (24) |
| 0° | 10° | CC (22) |
CC (21) |
CC (32) |
CC (32) |
CC (20) |
CC (23) |
CC (17) |
C | CC (33) |
CC (24) |
CC (23) |
CC (27) |
| 0° | 20° | CC (22) |
NC | NC | CC (23) |
CC (25) |
CC (22) |
CC (29) |
CC (29) |
CC (32) |
CC (27) |
CC (21) |
CC (17) |
| 10° | 0° | CC (24) |
NC | NC | C | NC | CC (20) |
CC (18) |
NC | NC | NC | CC (18) |
CC (25) |
| 10° | 10° | NC | NC | C | NC | CC (27) |
CC (20) |
CC (15) |
C | CC (30) |
C | CC (20) |
CC (23) |
| 10° | 20° | CC (21) |
NC | NC | C | NC | CC (20) |
NC | NC | NC | CC (23) |
C | C |
| 20° | 0° | NC | NC | NC | NC | NC | C | NC | NC | NC | NC | NC | NC |
| 20° | 10° | NC | NC | NC | NC | NC | CC (18) |
NC | NC | NC | NC | NC | C |
| 20° | 20° | NC | NC | NC | NC | NC | NC | NC | NC | NC | C | NC | NC |
| 30° | 0° | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC |
| 30° | 10° | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC |
| 30° | 20° | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC | NC |
aData in parentheses indicate LET wire depth at critical collision (in mm). Ant, anterior; LET, lateral extra-articular tenodesis; Prox, proximal; NC: no conflict; C: conflict; CC: critical collision.
Table A2.
Sizes of Commonly Used Suture Anchors and Recommended Tunnel Sizes
| Anchor (Manufacturer) | Tunnel Diameter, mm | Tunnel Length, mm | Suture Anchor Diameter, mm | Suture Anchor Length, mm |
|---|---|---|---|---|
| Twinfix (Smith & Nephew) | 3.8 | 21.7 | 4.5 or 5.5 | 19 |
| Bioraptor (Smith & Nephew) | 3.2 | 15 | 3.7 | 11.5 |
| Bio-SutureTak (Arthrex) | 2.4 | 18 | 3.0 | 14.5 |
| Gryphon (Mitek) | 2.4 | 17.8 | 3.0 | 10.8 |
Footnotes
Final revision submitted Aug 6, 2020; accepted August 27, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.L.Y.H. has received educational speaking fees from Mitek and Smith & Nephew and hospitality payments from Arthrex, Mitek, Smith & Nephew, and Zimmer Biomet. A.W. has received educational speaking fees from Arthrex, Smith & Nephew, and Stryker; research support from Smith & Nephew; and royalties from Innovate Orthopaedics; has stock/stock options in Innovate Orthopaedics; and is a board member of the Fortius Clinic. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
- 1. Ayeni OR, Chahal M, Tran MN, Sprague S. Pivot shift as an outcome measure for ACL reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2012;20(4):767–777. [DOI] [PubMed] [Google Scholar]
- 2. Chahla J, Menge TJ, Mitchell JJ, Dean CS, LaPrade RF. Anterolateral ligament reconstruction technique: an anatomic-based approach. Arthrosc Tech. 2016;5(3):e453–e457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Devitt BM, Bell SW, Ardern CL, et al. The role of lateral extra-articular tenodesis in primary anterior cruciate ligament reconstruction: a systematic review with meta-analysis and best-evidence synthesis. Orthop J Sports Med. 2017;5(10):2325967117731767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Dodds AL, Halewood C, Gupte CM, Williams A, Amis AA. The anterolateral ligament: anatomy, length changes and association with the Segond fracture. Bone Joint J. 2014;96(3):325–331. [DOI] [PubMed] [Google Scholar]
- 5. Geeslin AG, Moatshe G, Chahla J, et al. Anterolateral knee extra-articular stabilizers: a robotic study comparing anterolateral ligament reconstruction and modified Lemaire lateral extra-articular tenodesis. Am J Sports Med. 2018;46(3):607–616. [DOI] [PubMed] [Google Scholar]
- 6. Getgood A, Brown C, Lording T, et al. The anterolateral complex of the knee: results from the International ALC Consensus Group Meeting. Knee Surg Sports Traumatol Arthrosc. 2019;27(1):166–176. [DOI] [PubMed] [Google Scholar]
- 7. Getgood AMJ, Bryant DM, Litchfield R, et al. Lateral extra-articular tenodesis reduces failure of hamstring tendon autograft anterior cruciate ligament reconstruction: 2-year outcomes from the STABILITY study randomized clinical trial. Am J Sports Med. 2020;48(2):285–297. [DOI] [PubMed] [Google Scholar]
- 8. Hewison CE, Tran MN, Kaniki N, et al. Lateral extra-articular tenodesis reduces rotational laxity when combined with anterior cruciate ligament reconstruction: a systematic review of the literature. Arthroscopy. 2015;31(10):2022–2034. [DOI] [PubMed] [Google Scholar]
- 9. Inderhaug E, Stephen JM, El-Daou H, Williams A, Amis AA. The effects of anterolateral tenodesis on tibiofemoral contact pressures and kinematics. Am J Sports Med. 2017;45(13):3081–3088. [DOI] [PubMed] [Google Scholar]
- 10. Inderhaug E, Stephen JM, Williams A, Amis AA. Biomechanical comparison of anterolateral procedures combined with anterior cruciate ligament reconstruction. Am J Sports Med. 2017;45(2):347–354. [DOI] [PubMed] [Google Scholar]
- 11. Jaecker V, Ibe P, Endler CH, et al. High risk of tunnel convergence in combined anterior cruciate ligament reconstruction and lateral extra-articular tenodesis. Am J Sports Med. 2019;47(9):2110–2115. [DOI] [PubMed] [Google Scholar]
- 12. Jonsson H, Riklund-Ahlstrom K, Lind J. Positive pivot shift after ACL reconstruction predicts later osteoarthrosis: 63 patients followed 5-9 years after surgery. Acta Orthop Scand. 2004;75(5):594–599. [DOI] [PubMed] [Google Scholar]
- 13. Katakura M, Koga H, Nakamura T, et al. Biomechanical effects of additional anterolateral structure reconstruction with different femoral attachment sites on anterior cruciate ligament reconstruction. Am J Sports Med. 2019;47(14):3373–3380. [DOI] [PubMed] [Google Scholar]
- 14. Kim SJ, Chang CB, Choi CH, et al. Intertunnel relationships in combined anterior cruciate ligament and posterolateral corner reconstruction: an in vivo 3-dimensional anatomic study. Am J Sports Med. 2013;41(4):849–857. [DOI] [PubMed] [Google Scholar]
- 15. Kittl C, Halewood C, Stephen JM, et al. Length change patterns in the lateral extra-articular structures of the knee and related reconstructions. Am J Sports Med. 2015;43(2):354–362. [DOI] [PubMed] [Google Scholar]
- 16. Lee DW, Kim JG, Cho SI, Kim DH. Clinical outcomes of isolated revision anterior cruciate ligament reconstruction or in combination with anatomic anterolateral ligament reconstruction. Am J Sports Med. 2019;47(2):324–333. [DOI] [PubMed] [Google Scholar]
- 17. Lemaire M. Ruptures anciennes du ligament croisé antérieur du genou. J Chir 1967;83:311–320. [Google Scholar]
- 18. Logan MC, Williams A, Lavelle J, Gedroyc W, Freeman M. Tibiofemoral kinematics following successful anterior cruciate ligament reconstruction using dynamic multiple resonance imaging. Am J Sports Med. 2004;32(4):984–992. [DOI] [PubMed] [Google Scholar]
- 19. Moatshe G, Brady AW, Slette EL, et al. Multiple ligament reconstruction femoral tunnels: intertunnel relationships and guidelines to avoid convergence. Am J Sports Med. 2017;45(3):563–569. [DOI] [PubMed] [Google Scholar]
- 20. Nitri M, Rasmussen MT, Williams BT, et al. An in vitro robotic assessment of the anterolateral ligament, part 2: anterolateral ligament reconstruction combined with anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(3):593–601. [DOI] [PubMed] [Google Scholar]
- 21. Perelli S, Erquicia JI, Ibanez M, et al. Evaluating for tunnel convergence in anterior cruciate ligament reconstruction with modified Lemaire tenodesis: what is the best tunnel angle to decrease risk? Arthroscopy. 2020;36(3):776–784. [DOI] [PubMed] [Google Scholar]
- 22. Smeets K, Bellemans J, Lamers G, et al. High risk of tunnel convergence during combined anterior cruciate ligament and anterolateral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):611–617. [DOI] [PubMed] [Google Scholar]
- 23. Smeets K, Van Haver A, Van den Bempt S, et al. Risk analysis of tunnel collision in combined anterior cruciate ligament and anterolateral ligament reconstructions. Knee. 2019;26(5):962–968. [DOI] [PubMed] [Google Scholar]
- 24. Song GY, Hong L, Zhang H, et al. Clinical outcomes of combined lateral extra-articular tenodesis and intra-articular anterior cruciate ligament reconstruction in addressing high-grade pivot-shift phenomenon. Arthroscopy. 2016;32(5):898–905. [DOI] [PubMed] [Google Scholar]
- 25. Sonnery-Cottet B, Barbosa NC, Vieira TD, Saithna A. Clinical outcomes of extra-articular tenodesis/anterolateral reconstruction in the ACL injured knee. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):596–604. [DOI] [PubMed] [Google Scholar]
- 26. Tibor L, Chan PH, Funahashi TT, et al. Surgical technique trends in primary ACL reconstruction from 2007 to 2014. J Bone Joint Surg Am. 2016;98(13):1079–1089. [DOI] [PubMed] [Google Scholar]
- 27. Trojani C, Beaufils P, Burdin G, et al. Revision ACL reconstruction: influence of a lateral tenodesis. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1565–1570. [DOI] [PubMed] [Google Scholar]
- 28. Weber AE, Zuke W, Mayer EN, et al. Lateral augmentation procedures in anterior cruciate ligament reconstruction: anatomic, biomechanical, imaging, and clinical evidence. Am J Sports Med. 2019;47(3):740–752. [DOI] [PubMed] [Google Scholar]
- 29. Williams A, Ball S, Stephen J, et al. The scientific rationale for lateral tenodesis augmentation of intra-articular ACL reconstruction using a modified “Lemaire” procedure. Knee Surg Sports Traumatol Arthrosc. 2017;25(4):1339–1344. [DOI] [PubMed] [Google Scholar]