

Abstract
Objectives:
This study examined the roles of identity formation and moral identity in predicting college student mental health (anxiety and depressive symptoms), health-risk behaviors (hazardous alcohol use and sexual risk taking), and psychological well-being (self-esteem and meaning).
Method:
The sample comprised 9,500 college students (aged 18–25 years, mean = 19.78, standard deviation = 1.61: 73% female; 62% European American), from 31 different universities, who completed an online self-report survey.
Results:
Structural equation models found that identity maturity (commitment making and identity synthesis) predicted 5 of the health outcomes (except sexual risk taking), and moral identity predicted ail of the health outcomes. In most cases identity maturity and moral identity also interacted in predicting mental health and psychological well-being, but not health-risk behaviors.
Conclusions:
The maturity and specific contents of identity may both play unique and often interactive roles in predicting college student health. Thus, college student health might be bolstered by helping them establish appropriate identity commitments.
Keywords: identity formation, moral identity, health, mental health, risk taking, well-being, college student
Much research has examined correlates of identity formation (Kroger, 2007; Schwartz, Luyckx, & Vignoles, 2011). Such research often finds that individuals with a more mature sense of identity have better mental health and psychological well-being, and engage in less risk-taking behaviors. In other words, people who have made salient identity commitments and have a more coherent sense of who they are tend to be better off But most of this research measures the sense of identity as a unitary construct, viewing the content of one’s identity as less important. Little attention is paid to the relative importance or utility of various identity contents, even when multiple identity domains are assessed. However, some have suggested that in addition to identity formation, the types of things one bases his or her identity on are also important (i.e., identity contents; Blasi, 1993, 2004). In particular, when morality is central to identity (i.e., one has a moral identity), it motivates engagement in positive behaviors (e.g., volunteerism) and avoidance of negative behaviors (e.g., antisocial behavior; Hardy & Carlo, 2011a, 2011b). However, few studies have examined links between moral identity and mental health, health-risk behaviors, or psychological well-being.
Further, little is known about the relative roles of identity formation or maturity and identity contents (e.g., moral identity) in predicting such outcomes. Some suspect that the two interact (Blasi, 1993, 2004; Hardy & Carlo, 2011a, 2011b); in other words, identity content acts as a moderator such that identity formation more strongly predicts outcomes for people who center their identity more on morality. Unfortunately, this interaction hypothesis is yet to be tested empirically.
Last, while relations between identity and health may be important across the lifespan for many people worldwide, it may be particularly important to understand these processes among Western college students. This is because issues of identity and morality are particularly salient among these demographics in contemporary society (Arnett, 2004; Smith, Christoffersen, Davidson, & Snell Herzog, 2011). Thus, the purpose of the present study was to examine identity formation (indexed by commitment making and identity synthesis) and moral identity as predictors of college student health and well-being and moral identity as a moderator of the link between identity formation and outcomes.
Identity Formation and Health
Theory and research linking identity to health has largely been grounded in Erikson’s (1963, 1968) work on identity formation. He proposed that the key challenge of adolescence and young adulthood is resolving the identity conflict and argued that exploring identity possibilities and making identity commitments laid the foundation for healthy adult functioning (e.g., intimacy and generativity). Identity formation brings a sense of agency (i.e., autonomy and self-directedness), responsibility, integrity, commitment, and psychological maturity (Côté & Levine, 2002). Thus, people who have made identity commitments (i.e., decided certain things are important to who they are), ideally through a process of exploration, tend to engage in less risk behaviors, have fewer mental health problems, and experience greater psychological well-being.
Empirical studies have fairly consistently validated Erikson’s ideas regarding identity and healthy psychosocial functioning (Kroger, 2007). Specifically, individuals who have made identity commitments have fewer mental health concerns (e.g., anxiety and depression; Crocetti, Klimstra, Keijsers, Hale, & Meeus, 2009; Luyckx, Soenens, Goossens, Beckx, & Wouters, 2008), engage in fewer health-risk behaviors (e.g., alcohol use and sexual risk taking; Bishop, Weisgram, Holleque, Lund, & Wheeler-Anderson, 2005; Schwartz et al., 2009), and report higher levels of psychological well-being (e.g., self-esteem; Basak & Ghosh, 2008; Dunkel, Mathes, & Harbke, 2011). In short, theory and research on identity points to identity formation as protective against mental health and behavioral challenges.
Identity Formation and Identity Content
The studies just reviewed assume that identity formation is key to healthy psychosocial functioning, and that the type or quality of identity commitments is less important. However, in addition to identity formation (i.e., the formation of a mature identity structure), the specific contents on which one’s identity is based might also be important (Hardy & Carlo, 2011a, 2011b). Waterman (1993; Waterman et al., 2012) has argued that not all identity commitments are equivalent. Some are more “personally expressive” and thus conducive to feelings of flourishing or self-actualization. Likewise, based on the Self-Determination Theory, identity commitments that are in line with our intrinsic motivations and goals are more likely to fulfill innate psychological needs and yield value-congruent behaviors (Soenens, Berzonsky, Dunkel, Papini, & Vansteenkiste, 2011). In the possible selves literature, the specific contents of our ideal or desired selves, and our feared or dreaded selves, have important motivational implications, as people try to approach or avoid particular selves (Oyserman & James, 2011).
Last, Blasi (1993, 2004) has pointed to individual differences in the organization and structure of identity as well as the specific issues around which identities are based. Of primary interest to Blasi is the moral domain; thus, when people heavily base their identity on moral issues (such as being a moral person), it can lead to greater moral motivation and commitment. In other words, identity formation seems to provide the motivational impetus, while identity contents provide the direction, guiding individuals to specific courses of action.
Moral Identity and Health
An individual’s moral identity can be captured by the degree to which moral ideals, values, traits, goals, roles, and behaviors are central to a his or her identity (Hardy & Carlo, 2011a, 2011b). Moral identity forms when during adolescence and emerging adulthood, moral development and identity development processes become integrated (i.e., some individuals begin to define themselves based on their sense of morality). Empirical studies using a variety of methods have validated the role of moral identity as an important source of motivation for moral action. People with a greater sense of moral identity evidence more prosocial behavior (e.g., altruism and community involvement; Frimer & Walker, 2009; Hardy, 2006; Pratt, Hunsberger, Pancer, & Alisat, 2003), generativity (Pratt, Arnold, & Lawford, 2009), concern for others (including out-group members; Hardy, Bhattacharjee, Aquino, & Reed, 2010), and sustained moral commitments (Colby & Damon, 1992), and are less likely to engage in antisocial behavior (Barriga, Morrison, Liau, & Gibbs, 2001) and dishonesty (Aquino, Freeman, Reed, Lim, & Felps, 2009). However, most research has focused on outcomes that are very morally relevant such as these, so we know little about the role of moral identity in broader outcomes such as healthy or unhealthy psychological and behavioral outcomes.
Proposing a potential link between morality and health is not entirely new; in fact, Plato was one of the first to discuss the role of morality in mental illness. He stated that immorality was as harmful to the soul as disease was to the body (see Seeskin, 2008). However, this link has been somewhat ignored in contemporary psychology. Nevertheless, evidence is emerging to validate relations between morality and health. For instance, moral identity has been linked with lower levels of alcohol use (Lewis, Phillippi, & Neighbors, 2007), substance abuse (Amonini & Donovan, 2006), social anxiety (Wowra, 2007), and other forms of psychopathology (Glenn, Koleva, Iyer, Graham, & Ditto, 2010), as well as higher self-esteem (Higgins-D’Alessandro & Power, 2005). Nonetheless, more work is needed to substantiate links between morality and health.
Interactions Between Identity formation and Identity Content
The review above has highlighted the potential roles of identity formation, moral identity, and interactions between them in predicting healthy psychosocial functioning. On the one hand, one could argue that salient and coherent identity commitments will more strongly predict healthy thought, emotion, and behavior when centered on moral issues. In this case, identity contents are positioned as moderators of relations between identity formation and outcomes. This is largely the way the present study has been framed.
Alternatively, moral cognitions and emotions might more likely yield healthy functioning when woven into the core of a mature and organized identity structure. In this case, identity formation (the formation of a mature identity structure) is positioned as a moderator of relations between identity contents and outcomes. Thus, identity formation and identity content may interact in predicting outcomes, and this interaction can be viewed in two different ways (i.e., either facet of identity can play the role of moderator - although, in the present study, the emphasis is on moral identity content as a moderator).
Surprisingly, despite the intuitive nature of this interaction hypothesis, it has been the subject of little empirical research. Although research has investigated the relative importance of different identity contents (Haggar, Anderson, Kyriakaki, & Darkings, 2007), to our knowledge no study has examined interactions with identity formation. Nevertheless, there is precedent for such interactions in related areas of research. For instance, studies have demonstrated interactions between self-esteem level and contingencies of self-worth (Ferris, Brown, Lian, & Keeping, 2009; Park & Maner, 2009). In other words, both high and low self-esteem may differentially predict outcomes depending on the issues upon which people base their self-esteem. Hence, the notion of interactions between structure and content of self and identity has some initial theoretical and empirical support but is in need of further validation.
Another way of looking at the relative roles of identity formation and identity content is that both mature identity structure and moral identity contents might be necessary to effectively and consistently yield adaptive behaviors. A mature identity absent of moral identity contents might motivate behavior, but perhaps it may lead to less desirable behaviors. On the other hand, moral identity contents, if part of an immature identity structure, will be lofty ideals with little “wind in the sails” so to speak. Thus, moral identity can provide the direction and identity formation the power to move toward healthy psychosocial functioning. Indeed, some see such synergy as the pinnacle of moral developmetit and identity formation (Damon & Hart, 1992; Moshman, 2005). Although maturity of moral understanding and emotion is important in its own right, integration with identity may yield greater motivation and commitment. Moreover, while identities can be built on a variety of issues, it may be ideal (in terms of the well-being of the individual and those they interact with) and protective (in terms of health-risk behaviors) for them to be based on morality.
The Present Study
We examined the following hypotheses regarding identity formation and moral identity as predictors of health, as well as the interactions between them:
Hypothesis 1: Identity formation will be negatively related to mental health (anxiety and depression symptoms) and health-risk behaviors (hazardous alcohol use and risky sexual behavior), and positively related to psychological well-being (self-esteem and meaning in life).
Hypothesis 2: After accounting for identity formation, moral identity will be negatively related to mental health (anxiety and depression symptoms) and health-risk behaviors (hazardous alcohol use and risky sexual behavior), and positively related to psychological well-being (self-esteem and meaning in life).
Hypothesis 3: Links between identity formation (commitment making and identity synthesis) and health will be moderated by moral identity such that those links will be stronger at higher levels of moral identity.
Method
Sample and Procedures
Data for the present study came from the Multi-Site University Study of Identity and Culture (MUSIC; see Castillo & Schwartz, this issue, for more details on the sample and procedures). The MUSIC sample comprised 9,500 college students aged 18–25 years (mean [M] age = 19.78, standard deviation [SD] age = 1.61; 73% female; 62% European American, 15% Hispanic, 10% East Asian, 13% other). In terms of family background, 62% were from families with an annual income of $50,000 or above, and 72% came from an intact family (i.e., their biological or adoptive parents were still married).
Participants were recruited at 31 sites (large state universities, smaller state universities, major private universities, and smaller private colleges) from across the country through departments in various disciplines including psychology, sociology, business, family studies, education, and human nutrition. Data were collected via an online survey. At each site, participants were directed to the study website through printed or emailed announcements. Students received extra course credit for their participation or participated as part of a course research requirement. All measures were self-report surveys.
Measures
All alphas and other statistics reported below were derived from the analytic sample.
Identity formation.
Two measures were used as indexes of identity formation. The first measure of identity formation was the five-item (α = .92) Commitment Making subscale from the Dimension of Identity Development Scale (DIDS; Luyckx, et al., 2008). These items assess the extent to which people have made identity commitments, without specific reference to any particular domain of identity (sample item: “I have decided on the direction I want to follow in life”). Responses ranged from 1 (strongly disagree) to 5 (strongly agree). The five items were used as indicators of a latent construct. The second measure of identity formation was the six-item Identity Synthesis subscale (α = .81) from the Erikson Psychosocial Stage Inventory (EPSI; Rosenthal, Gurney, & Moore, 1981). The items assess the clarity and depth of a person’s identity (sample item: “I’ve got a clear idea of what I want to be”). Responses ranged from 0 (strongly disagree) to 4 (strongly agree). The six items were used as indicators of a latent construct.
Moral identity.
Moral identity was assessed using the five-item Internalization subscale (α = .82) from Aquino and Reed’s (2002) moral identity scale. The participants were given a list of moral qualities and were asked questions concerning the traits in terms of themselves (sample question: “It would make me feel good to be a person who has these characteristics”). The response options ranged from 1 (completely disagree) to 7 (completely agree). The five items were used as indicators of a latent construct.
Anxiety.
Anxiety symptoms were assessed using 18-items drawn from the Beck Anxiety Inventory (BAI; Beck, Epstein, Brown, & Steer, 1988) and the criteria for generalized anxiety disorder in Diagnostic and Statistical Manual of Mental Disorders Fourth Edition Text Revision (DSM-IV-TR; American Psychiatric Association, 1994). Responses ranged from 1 (strongly disagree) to 5 (strongly agree). Items were selected that reflect anxiety symptoms more common among the general population (sample item: “This week, I have been afraid of what was going to happen to me”), rather than those indicative of more extreme pathology (e.g., fear of dying). The 11 items from the BAI (α = .94) were averaged, as well as the four DSM-IV-TR items (α = .89) pertaining to sleep difficulties, and the three (α = .89) dealing with problems eating. These three composite scores (a = .82) were used as indicators of a latent construct.
Depression.
The 20-item (α = .92) Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) was used to assess symptoms of depression. The CES-D scale separates depression into four factors: positive affect (four items; α = .79); negative affect (seven items; a = .88); somatic symptoms (seven items; α = .82); and interpersonal problems (two items; a = .81). Participants rated their symptoms within the last week from 1 (strongly disagree) to 5 (strongly agree; sample item: “This week, my friends tried to cheer me up, but I didn’t feel happy”). Composite scores (item averages) for the four dimensions (α = .81) were used as indicators of a latent construct.
Hazardous alcohol use.
Hazardous alcohol use was asses by the 10-item (α = .82) Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). Prior research suggests a three-factor structure to the items (Doyle, Donovan, & Kivlahan, 2007): alcohol consumption (three items; α = .78); alcohol dependence (three items; α = .78); and harmful alcohol use (four items; α = .66). The questions gauged drinking behaviors and consequences in the past year on a scale from 1 (never) to 5 (daily/almost daily; sample item: “How often do you have six or more drinks on one occasion?”). The items for each area were averaged to create three composite scores (α = .76), which were used as indicators of a latent construct.
Sexual risk taking.
To measure sexual risk taking, we used a five-item (α = .69) subset of the Youth Risk Behavior Surveillance Survey (YRBSS; Kann, et al., 1998). These items assessed the frequency of certain sexual risk behaviors within a 30-day time period on a scale from 1 (never) to 5 (11 or more times; sample item: “In the last 30 days, how many times have you had sex with someone you have known for less than a week?”). The five items were used as indicators of a latent construct.
Self-esteem.
The 10-item (α = .88) Rosenberg Self-Esteem Scale (Rosenberg, 1989) was used to assess self-esteem. Participants rated the items from 1 (strongly disagree) to 5 (strongly agree; sample item: “On the whole, I am satisfied with myself). Prior research suggests a two-factor structure to the items (Roth, Decker, Herzberg, & Brähler, 2008): negatively worded statements (five items; α = .86) and positively worded statements (five items; α = .86). Items from these two factors were averaged to create two composite scores (α = .67), which were used as two indicators of a latent construct.
Meaning.
Five items (α = .87) from the Meaning in Life Questionnaire (MLQ; Steger, Frazier, Oishi, & Kaler, 2006) were used to assess meaning in life. The Presence subscale of the questionnaire was used to measure whether there was presence of meaning in the life of the participant (sample item: “My life has a clear sense of purpose”). Responses ranged from 1 (absolutely untrue) to 7 (absolutely true). The five items of the subscale were used as indicators of a latent construct.
Analysis Plan
The hypotheses regarding links between identity formation, moral identity, and health were assessed via structural equation modeling (SEM) with latent variables using the Mplus (version 6) statistical software. Model parameters were estimated using full information maximum likelihood estimation (FIML), which capitalizes on available data to estimate parameters, so all cases with data on at least one variable were included in the analysis. As indicators of model fit (Brown, 2006), we used the chi-square (χ2) statistic, the root mean squared error of approximation (RMSEA; values below .05 indicate good fit, below .08 indicate moderate fit, and below .10 indicating mediocre fit), and the comparative fit index (CFI; values above .95 indicate good fit, and values above .90 indicate moderate fit). Last, given the large sample size we used p < .01 as the criteria for the statistical significance of individual parameters.
First, a series of confirmatory factor analyses (CFAs) were conducted with all latent variables (moral identity, identity formation, and the six health outcomes) to achieve optimal model fit. These analyses were conducted twice, once with identity formation indexed as commitment making and the other with it indexed as identity synthesis (both being important aspects of identity formation). Model fit was improved based on the modification indexes by adding one correlated error at a time, starting with the one with the largest modification index value and working down, and using the CFI difference test to compare model fit, where a significant change in CFI is one that results in a difference of .01 or greater (Cheung & Rensvold, 2002). The CFI difference test was used instead of the chi-squared difference test because with large samples the chi-squared test is overly sensitive. Once the final model was selected, structural paths were added and the moderation hypotheses were assessed by estimating two interaction models (one for each moderator).
In Mplus, interactions between latent variables were estimated using the XWITH command and numerical integration (Muthén & Muthén, 1998–2010). This approach creates indicators for the latent interaction term with factor loadings that are the products of those for the indicators of the predictor and moderator variables (Klein & Moosbrugger, 2000). Such interactions between latent variables are continuous, regardless of whether the indicators are continuous.
Results
Preliminary Analyses
Descriptive statistics (means and standard deviations) for observed variables are presented in Table 1. Factor loadings of observed indicators on the latent variables are also presented in Table 1, while bivariate correlations among the latent variables (as well as age and gender) are presented in Table 2. These parameters were all estimated by conducting a CFA with all study variables (and with age and gender included as observed covariates). Age and gender correlated with a number of the study variables, and thus were included as control variables in all primary analyses. Commitment making and identity synthesis were strongly associated (r = .70) and were moderately linked to moral identity (rs .19 and .38, respectively). All three of these variables were negatively related to symptoms of depression and anxiety, levels of hazardous alcohol use, and sexual risk taking (although correlations for sexual risk taking with commitment making and identity synthesis were not statistically significant), and positively related to self-esteem and meaning. All health outcome variables were associated with each other in expected ways.
Table 1.
Observed Variable Descriptive Statistics and Latent Variable Factor Loadings
| Observed variable | |||
|---|---|---|---|
| Indicators | M | SD | Latent variable factor loadings |
| Commitment making - Item 1 | 3.79 | 1.05 | 0.87 |
| Commitment making - Item 2 | 3.72 | 1.08 | 0.92 |
| Commitment making - Item 3 | 3.53 | 1.11 | 0.89 |
| Commitment making - Item 4 | 4.00 | 0.90 | 0.74 |
| Commitment making - Item 5 | 4.03 | 0.95 | 0.75 |
| Identity synthesis - Item 1 | 3.63 | 1.12 | 0.62 |
| Identity synthesis - Item 2 | 3.95 | 0.95 | 0.66 |
| Identity synthesis - Item 3 | 3.49 | 1.02 | 0.69 |
| Identity synthesis - Item 4 | 3.98 | 0.90 | 0.73 |
| Identity synthesis - Item 5 | 4.36 | 0.84 | 0.51 |
| Identity synthesis - Item 6 | 4.20 | 0.87 | 0.72 |
| Moral identity - Item 1 | 6.20 | 1.44 | 0.90 |
| Moral identity - Item 2 | 5.89 | 1.40 | 0.89 |
| Moral identity - Item 3 | 6.39 | 1.26 | 0.51 |
| Moral identity - Item 4 | 5.83 | 1.61 | 0.37 |
| Moral identity - Item 5 | 5.82 | 1.48 | 0.77 |
| Anxiety - BAI composite | 2.39 | 0.98 | 0.98 |
| Anxiety - problems sleeping composite | 2.37 | 1.13 | 0.70 |
| Anxiety - problems eating composite | 1.96 | 1.01 | 0.71 |
| Depression - positive affect composite | 2.52 | 0.80 | 0.47 |
| Depression - negative affect composite | 2.51 | 0.95 | 0.92 |
| Depression - somatic symptoms composite | 2.72 | 0.86 | 0.85 |
| Depression - interpersonal problems composite | 2.06 | 1.00 | 0.70 |
| Alcohol use - alcohol consumption composite | 1.16 | 0.98 | 0.62 |
| Alcohol use - alcohol dependence composite | 0.33 | 0.60 | 0.80 |
| Alcohol use - harmful alcohol use composite | 0.49 | 0.68 | 0.84 |
| Sexual risk-taking - Item 1 | 0.14 | 0.49 | 0.39 |
| Sexual risk-taking - Item 2 | 0.76 | 1.29 | 0.64 |
| Sexual risk-taking - Item 3 | 0.91 | 1.20 | 0.68 |
| Sexual risk-taking - Item 4 | 0.12 | 0.48 | 0.42 |
| Sexual risk-taking - Item 5 | 0.41 | 0.78 | 0.72 |
| Self-esteem - negative composite | 3.56 | 0.93 | 0.71 |
| Self-esteem - positive composite | 3.99 | 0.70 | 0.73 |
| Meaning - Item 1 | 4.01 | 1.31 | 0.74 |
| Meaning - Item 2 | 4.03 | 1.24 | 0.84 |
| Meaning - Item 3 | 4.34 | 1.16 | 0.81 |
| Meaning - Item 4 | 4.01 | 1.25 | 0.81 |
| Meaning - Item 5 | 4.61 | 1.33 | 0.60 |
Note. M = mean; SD = standard deviation; BAI = Beck Anxiety Inventory.
ns ranged from 3771 to 8867 for the observed variables, while N = 9500 for the factor model.
Table 2.
Estimated Correlation Matrix for the Latent Variables and Demographics
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Moral identity | ||||||||||
| 2 | Commitment making | .19* | |||||||||
| 3 | Identity synthesis | .38* | .70* | ||||||||
| 4 | Depression | −.28* | −.17* | −.36* | |||||||
| 5 | Anxiety | −.32* | −.15* | −.33* | .97* | ||||||
| 6 | Alcohol use | −.29* | −.13* | −.16* | .22* | .26* | |||||
| 7 | Sexual risk taking | −.18* | −.002 | −.03 | .11* | .15* | .51* | ||||
| 8 | Self-esteem | .47* | .45* | .80* | −.70* | −.67* | −.25* | −.06* | |||
| 9 | Meaning | .35* | .54* | .67* | −.33* | −.29* | −.22* | −.08* | .63* | ||
| 10 | Age | −.03 | .05* | .03* | −.03* | −.02 | .05* | .14* | .04* | .08* | |
| 11 | Gender | .19* | .04* | .05* | .03 | .03* | −.12* | −.04* | .07* | .09* | .0001 |
Note. N = 9500.
P < .0l.
Primary Analyses
CFA.
For commitment making, a model was specified with latent variables for commitment making, moral identity, and the six health outcomes (anxiety symptoms, depressive symptoms, levels of hazardous alcohol use, sexual risk taking, self-esteem, and meaning), as well as covariances between all variables. The initial model fit the data moderately well, χ2 (436) = 12882.30, p = .0001, CFI = .90, RMSEA = .06. However, the modification indexes suggested a number of correlated errors in order to improve model fit. Three correlated errors, for indicators with similar content, were added before improvement in model fit plateaued (based on CFI difference tests), and the optimal model was obtained, χ2 (433) = 9837.11, p = .0001, CFI = .93, RMSEA = .05.
For identity synthesis, a model was specified with latent variables for identity synthesis, moral identity, and the six health outcomes, as well as covariances between these variables. The initial model fit the data moderately well, χ2 (467) = 14902.15, p = .0001, CFI = .88, RMSEA = .06. However, the modification indexes suggested a number of correlated errors to improve model fit. Four correlated errors, for indicators with similar content, were added before improvement in model fit plateaued (based on CFI difference tests) and the optimal model was obtained, χ2 (463) = 11219.48, p = .0001, CFI = .91, RMSEA = .05.
Structural equation model analyses with interactions.
Starting with the final CFA models obtained above, we added in the latent interaction terms, the structural paths, and the demographic covariates (age and gender). These models (one for commitment making and one for identity synthesis) allowed us to assess links between identity formation, moral identity, and health, as well as interactions between identity formation and moral identity (see Table 3). Full information maximum likelihood with numerical integration was used to estimate parameters, given our specification of latent interactions; this procedure does not yield fit indexes other than Akaike information criterion (AIC) and Bayesian information criteria (BIC).
Table 3.
Structural Equation Modeling Results
| Predictors | Outcomes | |||||
|---|---|---|---|---|---|---|
| Depression | Anxiety | Alcohol use | Sexual risk | Self-esteem | Meaning | |
| Model | b | b | b | b | b | b |
| Model 1 | ||||||
| Moral identity | −0.17* | −0.24* | −0.12* | −0.06* | 0.13* | 0.19* |
| Commitment making | −0.10* | −0.09* | −0.05* | 0.002 | 0.16* | 0.52* |
| Interaction | −0.07* | −0.06* | 0.02 | 0.02* | 0.03* | 0.01 |
| Model 2 | ||||||
| Moral identity | −0.16* | −0.23* | −0.12* | −0.06* | 0.10* | 0.09* |
| Identity synthesis | −0.35* | −0.35* | −0.07* | 0.006 | 0.52* | 0.98* |
| Interaction | −0.15* | −0.14* | −0.002 | 0.03* | 0.09* | 0.05* |
Note. Model 1 n = 8816, Model 2 n = 8792; Both models included age and gender as control variables; b coefficients are unstandardized regression coefficients (standardized are reported in the text).
p < .01.
On these indexes, smaller values indicate better model fit. Going from the CFA to the full structural equation models for testing moderation for the commitment making model resulted in slight decreases on both indexes (531,787 to 529,276 for AIC, and 532,687 to 530,303 for BIC). Commitment making was predictive of depressive symptoms (β = −.12), anxiety symptoms (β = −.09), levels of hazardous alcohol use (ß = −.08), self-esteem (β = .32), and meaning (β = .49), but not sexual risk taking. Even after accounting for identity formation (as indexed by commitment making), moral identity was negatively predictive of depressive symptoms (β = −.31), anxiety symptoms (β = −.36), levels of hazardous alcohol use (β = −.27), and sexual risk taking (β = −.29), and positively predictive of self-esteem (β = 0.38) and meaning (β = 0.25).
Further, the interaction between commitment making and moral identity was significant for all outcomes but alcohol use and meaning (see Figures 1–4). All significant interactions were in the expected direction (the links between identity and the outcomes were stronger at higher levels of moral identity). The interaction plots specify identity formation as the predictor and moral identity as the moderator, but the interpretation is the same if these roles are switched (i.e., the link between moral identity and the outcomes is stronger at higher levels of commitment making).
Figure 1.
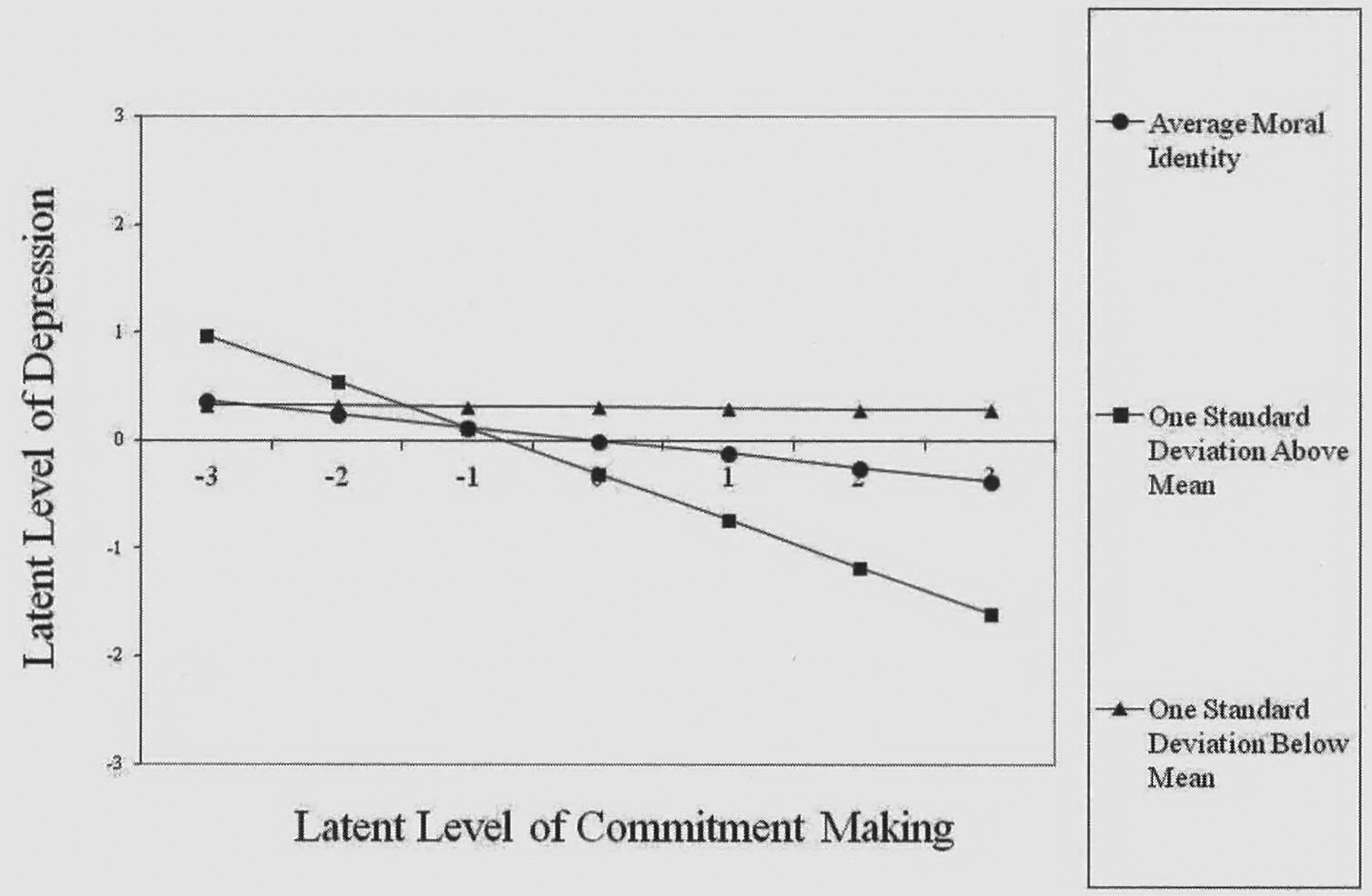
Interaction Plot of Link between Commitment Making and Depression at Various Levels of Moral Identity.
Figure 4.
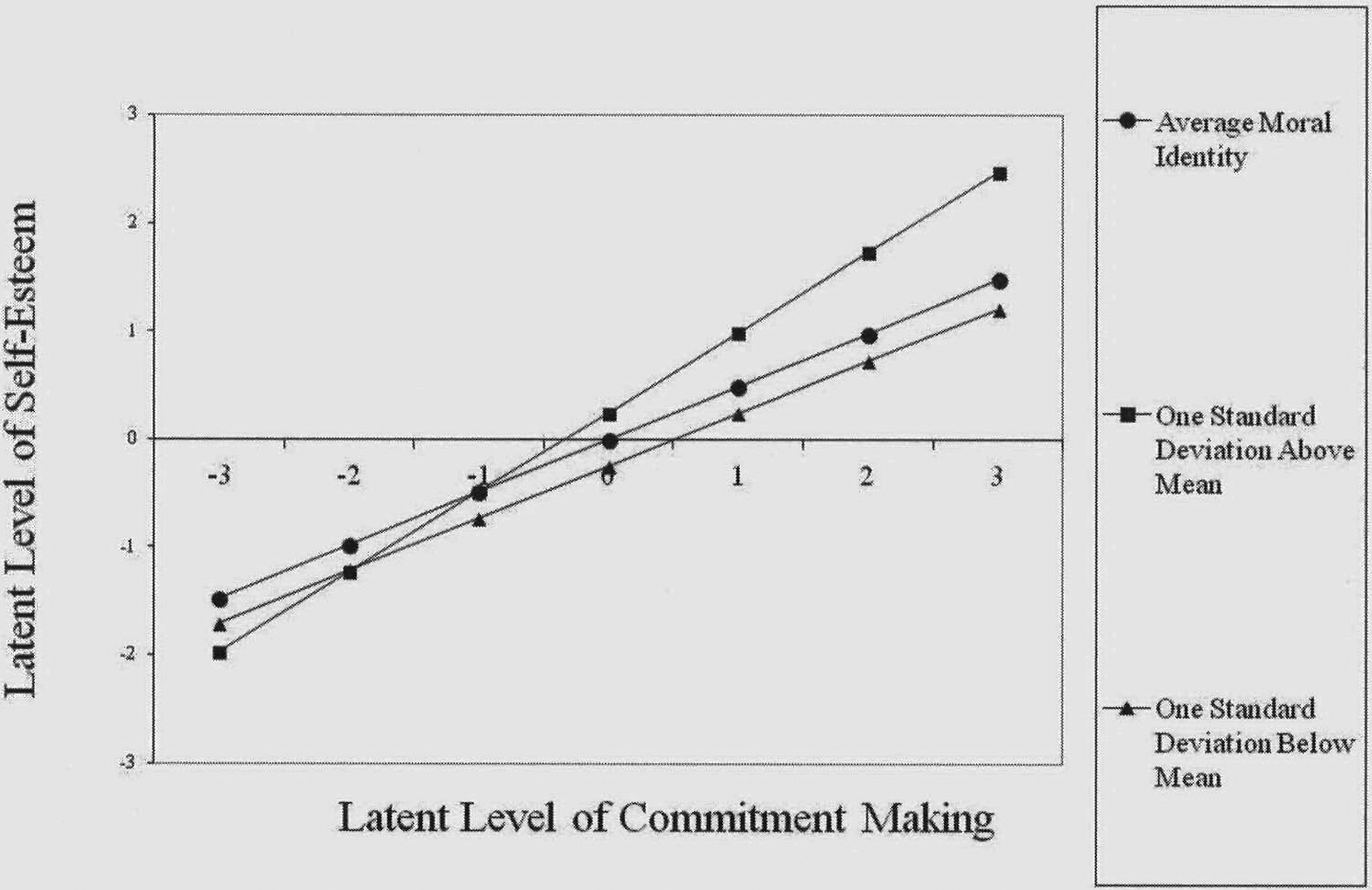
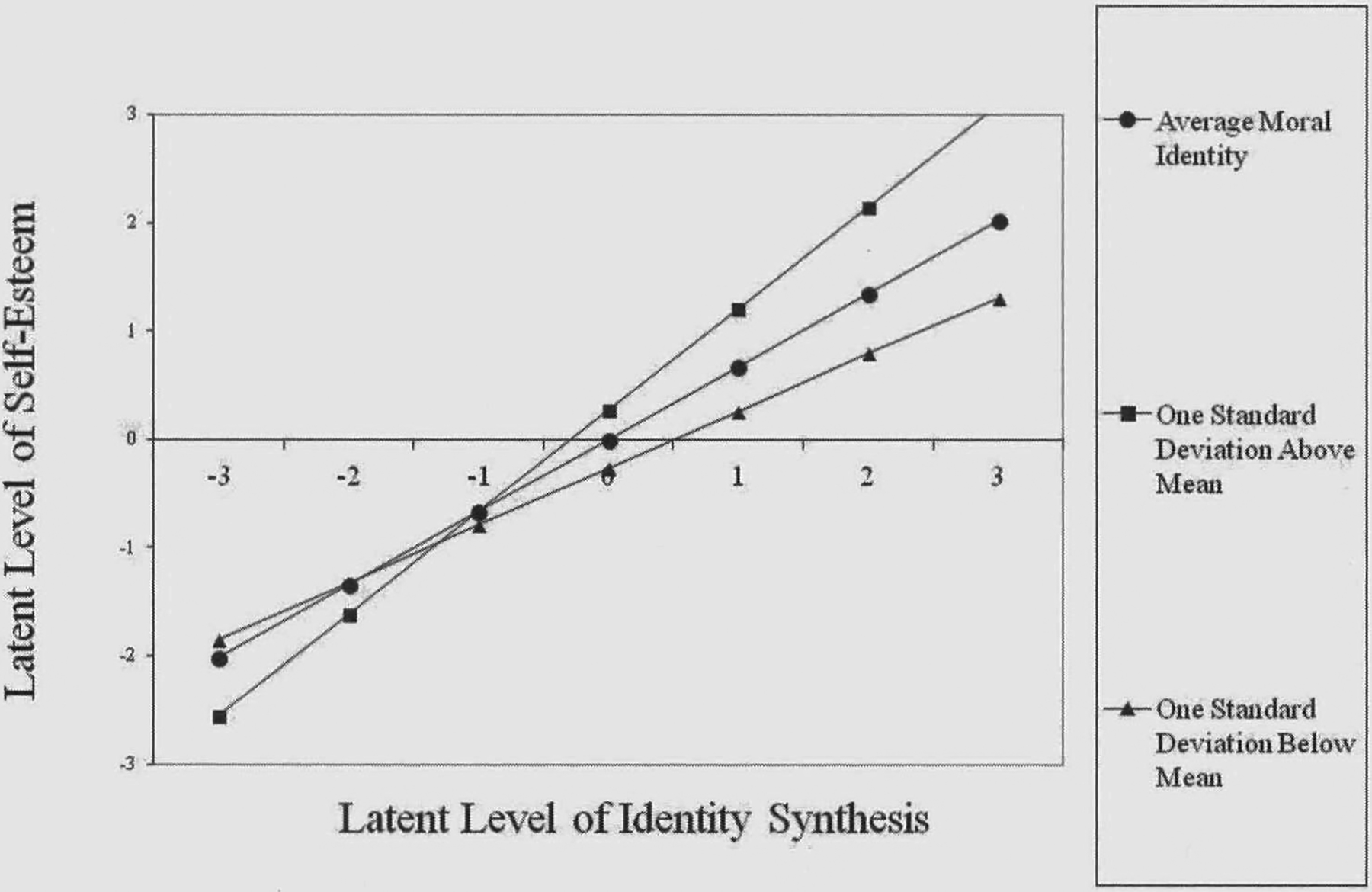
Interaction Plot of Link between Commitment Making and Self-Esteem at Various Levels of Moral Identity.
Going from the CFA to the full structural equation models for testing moderation for the identity synthesis model similarly resulted in slight decreases on both indexes (560,357 to 557,564 for AIC, and 561,286 to 558,619 for BIC). Identity synthesis was similarly predictive of depressive symptoms (β = −.30), anxiety symptoms (β = −.25), levels of hazardous alcohol use (β = −.07), self-esteem (β = .68), and meaning (β = .64), but not sexual risk taking. Even after accounting for identity formation (as indexed by identity synthesis), moral identity was negatively predictive of depressive symptoms (β = −.28), anxiety symptoms (β = −.33), levels of hazardous alcohol use (β = −.27), and sexual risk taking (β = −.28), and positively predictive of self-esteem (β = 0.27) and meaning (β = 0.12). Further, the interaction between identity synthesis and moral identity was significant for all outcomes but levels of hazardous alcohol use. All significant interactions were in the expected direction (the links between identity and the outcomes were stronger at higher levels of moral identity; see Figures 5–9).
Figure 5.
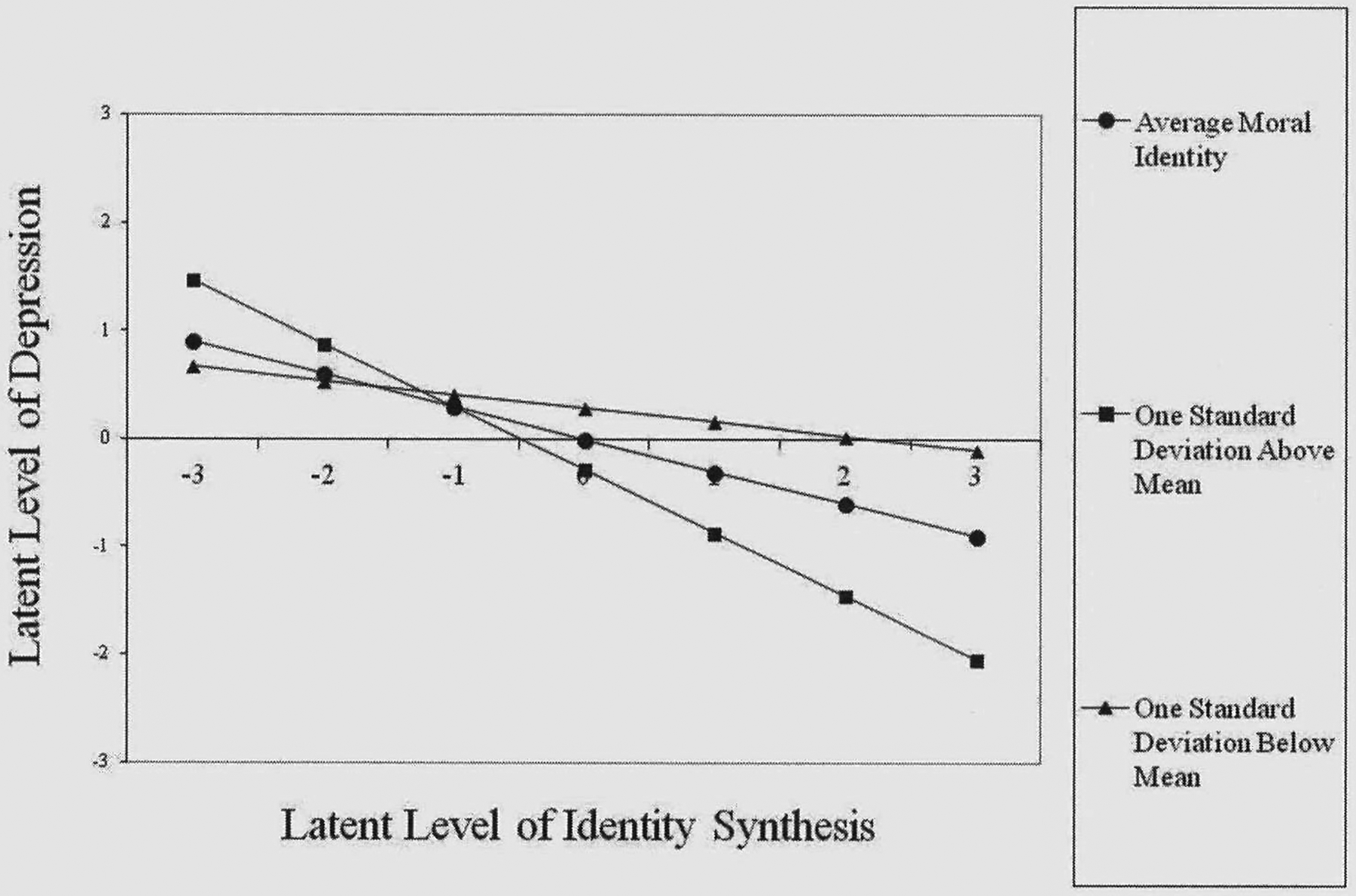
Interaction Plot of Link between Identity Synthesis and Depression at Various Levels of Moral Identity.
Figure 9.
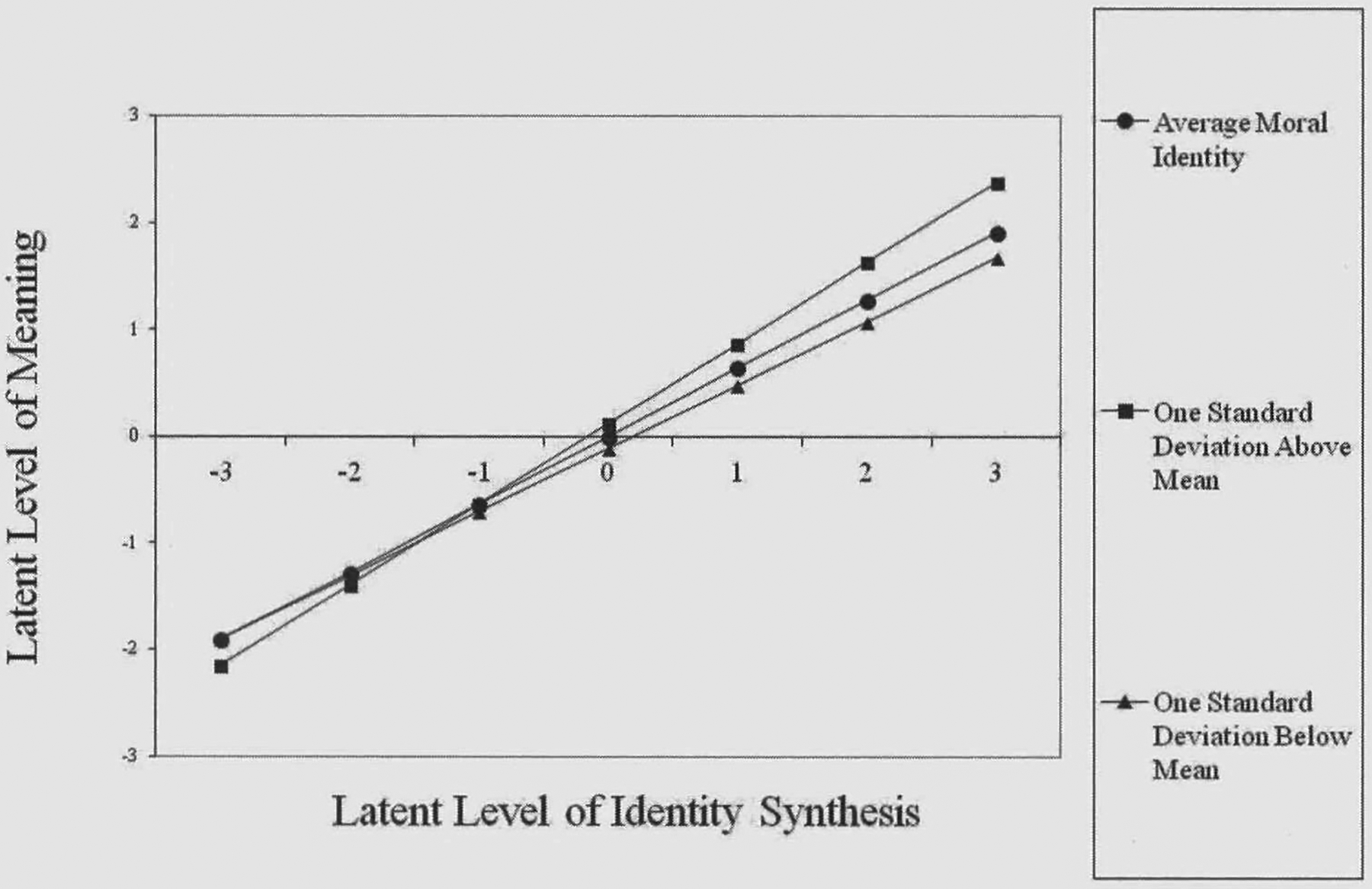
Interaction Plot of Link between Identity Synthesis and Meaning at Various Levels of Moral Identity.
Discussion
The purpose of the present study was to examine the relative and additive roles of identity formation and moral identity in predicting college student health, specifically mental health, health-risk behaviors, and psychological well-being. The study hypotheses were largely supported. When accounting for moral identity, identity formation (both commitment making and identity synthesis) was related to all health outcomes except sexual risk taking. When accounting for identity formation, moral identity was associated with all health outcomes. Nine of the 12 possible interactions between identity formation and moral identity were significant and in the expected direction (stronger links between one predictor and the outcomes at higher levels of the other predictor). Of the nonsignificant interactions, most were for the health-risk behaviors.
Our findings regarding links between identity formation and health are largely congruent with prior research (Basak & Ghosh, 2008; Bishop et al, 2005; Crocetti et al, 2009; Dunkel et al., 2011 ; Luyckx et al., 2008; Schwartz et al., 2009). Individuals higher on commitment making and identity synthesis (our two indexes of identity formation) were lower on symptoms of anxiety and depression and lower levels of hazardous alcohol use, while being higher on self-esteem and meaning. Thus, as Erikson (1963, 1968) suspected, it seems identity formation in adolescence and adulthood can help pave the way for better health and well-being. Nevertheless, it is unclear why identity formation was not related to sexual risk taking in the present sample (a finding consistent across the indexes of identity formation). Perhaps some degree of sexual risk taking is normative enough at this stage of life that psychosocial maturity is no longer a protective factor.
The present results replicate and extend the limited prior work linking moral identity to health (Amonini & Donovan, 2006; Glenn et al, 2010; Higgins-D’Alessandro & Power, 2005; Lewis et al., 2007; Wowra, 2007). In fact, even after controlling for identity formation, moral identity was predictive of all six health outcomes; individuals higher on moral identity reported lower anxiety and depressive symptoms and lower levels of hazardous alcohol use and sexual risk taking, and higher on self-esteem and meaning. Thus, in support of identity theory, both the structure and the contents of a person’s identity are independently important (Blasi 1993, 2004; Oyserman & James, 2011; Soenens et al., 2011; Waterman 1993; Waterman et al, 2012). In this case, independent of the level of identity formation (indexed by commitment making and identity synthesis), the extent to which people based their identity on morality was important to their health and well-being. Therefore, not au identity commitments are equally conducive to healthy functioning; moral commitments may be particularly adaptive.
As expected, we also found that the two facets of identity (identity formation and moral identity) more often than not interacted in predicting the health outcomes. Nine of the 12 possible interaction effects were significant. These interactions can be interpreted in two ways. By one interpretation, identity formation is more predictive of health outcomes at higher levels of moral identity. In other words, making identity commitments and forming a more coherent identity will matter more for one’s health to the extent that one bases his or her identity on being a moral person. This is perhaps because the motivating power of a mature and coherent identity is then moving the person in healthy directions in their life (Waterman et al, 2012).
From the other interpretation, moral identity is more predictive of health outcomes at higher levels of identity formation. In other words, placing importance on being a moral person will matter more to one’s health if he or she has stronger identity commitments or more coherent identity structure. This is perhaps because such moral identity contents will have stronger claims on peoples’ actions when they are a central part of a mature identity (Hardy & Carlo, 2011a, 2011b). The statistical results do not point to one interpretation or the other. Both interpretations are theoretically meaningful and validate ideas about interrelations between the two aspects of identity (Blasi 1993, 2004; Waterman 1993; Waterman et al., 2012).
In three instances (alcohol use for both identity variables, and meaning for commitment making) we did not find the proposed interaction. The lack of interaction suggests that the main effects are robust. Specifically, dentity maturity predicts alcohol use (as well as meaning in the case of commitment making) fairly consistently regardless of level of moral identity. Similarly, moral identity predicts these outcomes fairly consistently regardless of level of identity formation. In short, a lack of an interaction is still important in that it signifies unconditional effects.
Clinical Implications
These findings could be used to further our understanding of identity processes in intervention efforts for adolescents (Archer, 2008; Oyserman & Destin, 2010). Evidence is building that such interventions among adolescents can not only increase school engagement and academic achievement, but also decrease deviant behavior and improve mental health (Archer, 2008; Oyserman & Destin, 2010). Further, some argue that achievement of a healthy identity should be considered an important intervention outcome for its own sake, not just because it is a mediator to other positive outcomes (Berman, Kennerley, & Kennerley, 2008; Kurtines et al., 2008). At the very least, identity formation might provide insight to practitioners on how adolescents may respond to identity-related therapeutic challenges as well as be a marker of intervention success (Forthun & Montgomery, 2009). Unfortunately, little is known about identity-based interventions among college students, although there is some evidence for their feasibility and effectiveness (Berman et al., 2008).
The present study suggests that practitioners might be able to better serve college students if they have knowledge of developmental issues facing this population. Emerging adulthood is a transitional period that can take its toll on health and well-being (Arnett, 2004; Côté & Bynner, 2008; Smith et al., 2011). Practitioners who understand identity processes can better support individuals through this developmental period. In fact, the present findings indicate that problems with identity might be a health-risk factor that can be assessed and monitored. Moreover, perhaps practitioners should not just concern themselves with helping college students discover or create an identity that works for them, but should help guide them into considering the type of identity commitments that might be most conducive to healthy functioning. However, it may also be helpful for practitioners to know that the processes by which identity is linked to health might differ depending on the specific health outcome in question (e.g., mental health, risky behaviors, psychological well-being).
Last, as noted above, intervention programs might be developed that center on the facilitation of healthy identity formation (Archer, 2008; Oyserman & Destin, 2010). For example, one such program for college students involved reading about identity issues, discussing identity issues in small-group sessions, completing assignments designed to promote self-reflection and identity exploration (e.g., journaling), and then engaging in critical thinking and personalized problem solving in further group sessions (Berman et al., 2008). Based on the present study, such programs might be enriched by incorporating materials and discussions about moral issues and their relevance to identity.
Limitations
Despite the interesting and important pattern of findings, the present study had a number of notable limitations. First, the data were cross-sectional, limiting our ability to draw inferences about causality. As a consequence, we cannot rule out the possibility that healthy patterns of thought, emotion, and behavior are more conducive to identity formation and moral identity. Future research should employ longitudinal design to piece apart temporal ordering. Second, the measures were all self-report, which can lead to problems of shared method variance and social desirability bias. However, people tend to be fairly accurate in reporting their own behaviors and internal states (Clarke, Lewinsohn, Hops, & Seeley, 1992). Nevertheless, future research should utilize other measurement modalities, such as other-report, observational, or interview methods.
Last, in this study we looked only at the moral domain in terms of identity content. The interrelations between identity formation and identity content in predicting health might differ for various identity contents. After all, studies of contingencies of self-worth find interesting differences across domains upon which people base their self-worth (Crocker, 2002). Therefore, future research might look at the role of identity domains such as religion, academic or career achievement, athletic ability, and physical health or attractiveness.
Conclusion
The present results suggest that both identity formation (e.g., commitment making and identity synthesis) and identity content (e.g., moral identity) can be risk or protective factors for a number of health outcomes. Further, the two facets of identity seem to interact in meaningful ways. Identity formation may have more positive health effects when based on moral identity contents than when based on amoral or even immoral contents. Moral ideals and commitments can more powerfully motivate healthy living when a part of a mature and coherent identity than when they are merely a haphazard part of an immature or diffused identity. The interesting, fairly consistent, and reasonably strong pattern of relations between identity and health in the present study attest to the salient role identity plays in health and well-being, at least for college students in the United States. Practitioners can better serve this population if equipped with knowledge of identity development and functioning. To better inform theory and practice, further conceptual, empirical, and applied work is needed to explore the roles various facets and domains of identity (e.g., religion, career, academics, health, and athletics) play in physical, mental, and emotional health and well-being.
Future studies should also explore whether the present findings generalize to emerging adults not enrolled in college, to college students in other cultures, and to other age groups. Although identity may play a role in health fairly universally, the particular pattern of findings in the present study may partly reflect the unique situation of emerging adult college students in the United States.
Figure 2.
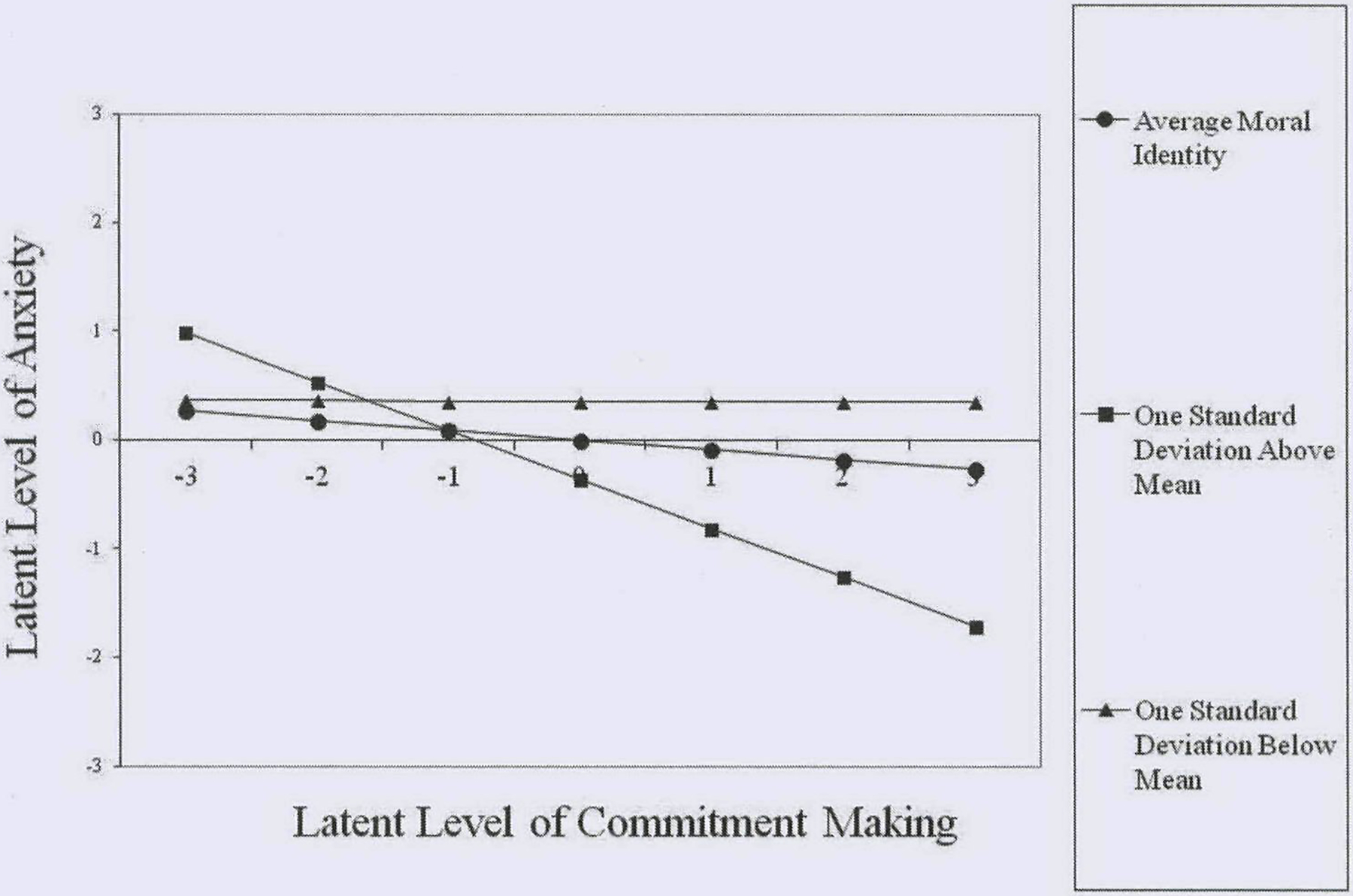
Interaction Plot of Link between Commitment Making and Anxiety at Various Levels of Moral Identity.
Figure 3.
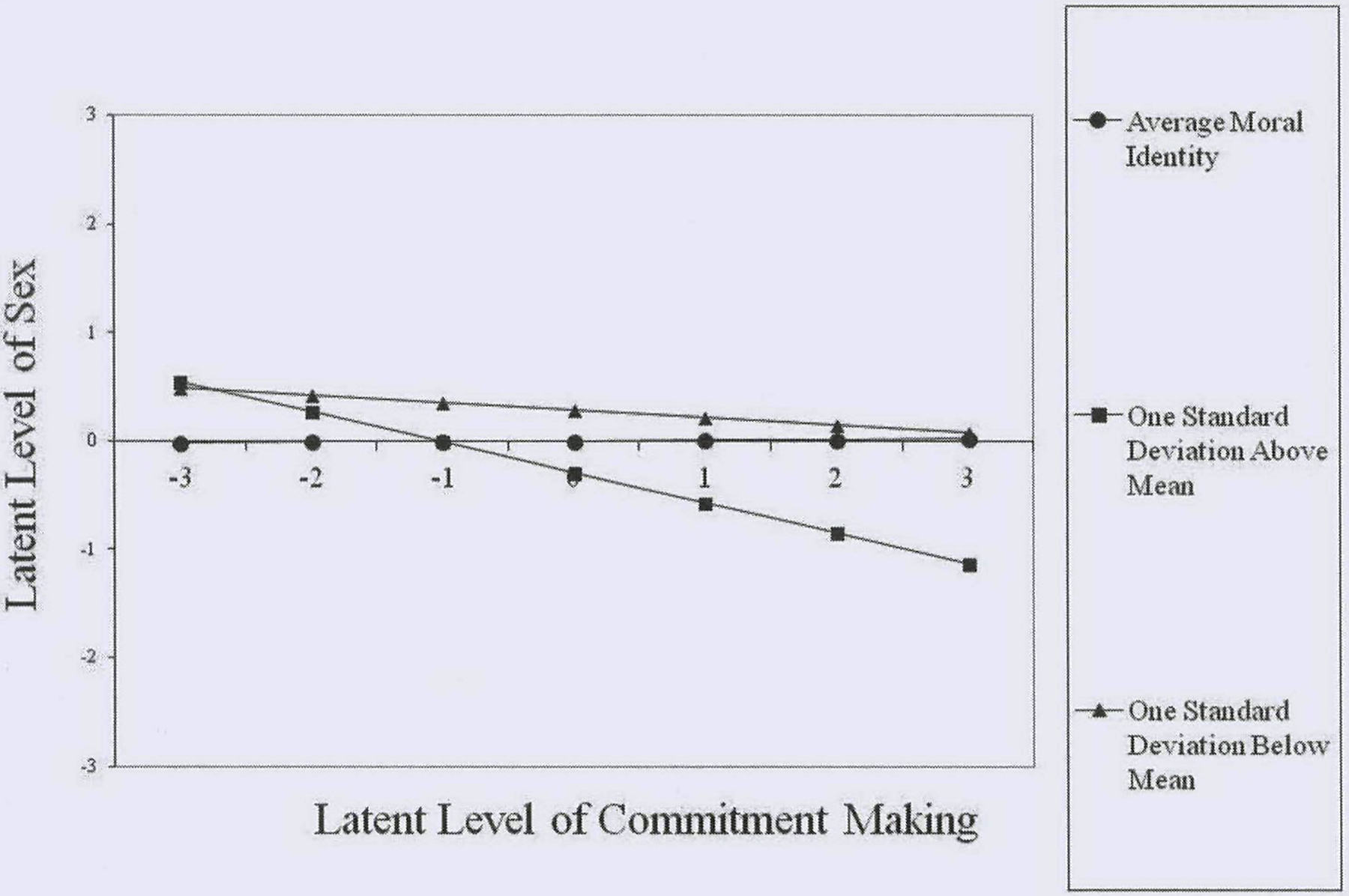
Interaction Plot of Link between Commitment Making and Sexual Risk Taking at Various Levels of Moral Identity.
Figure 6.
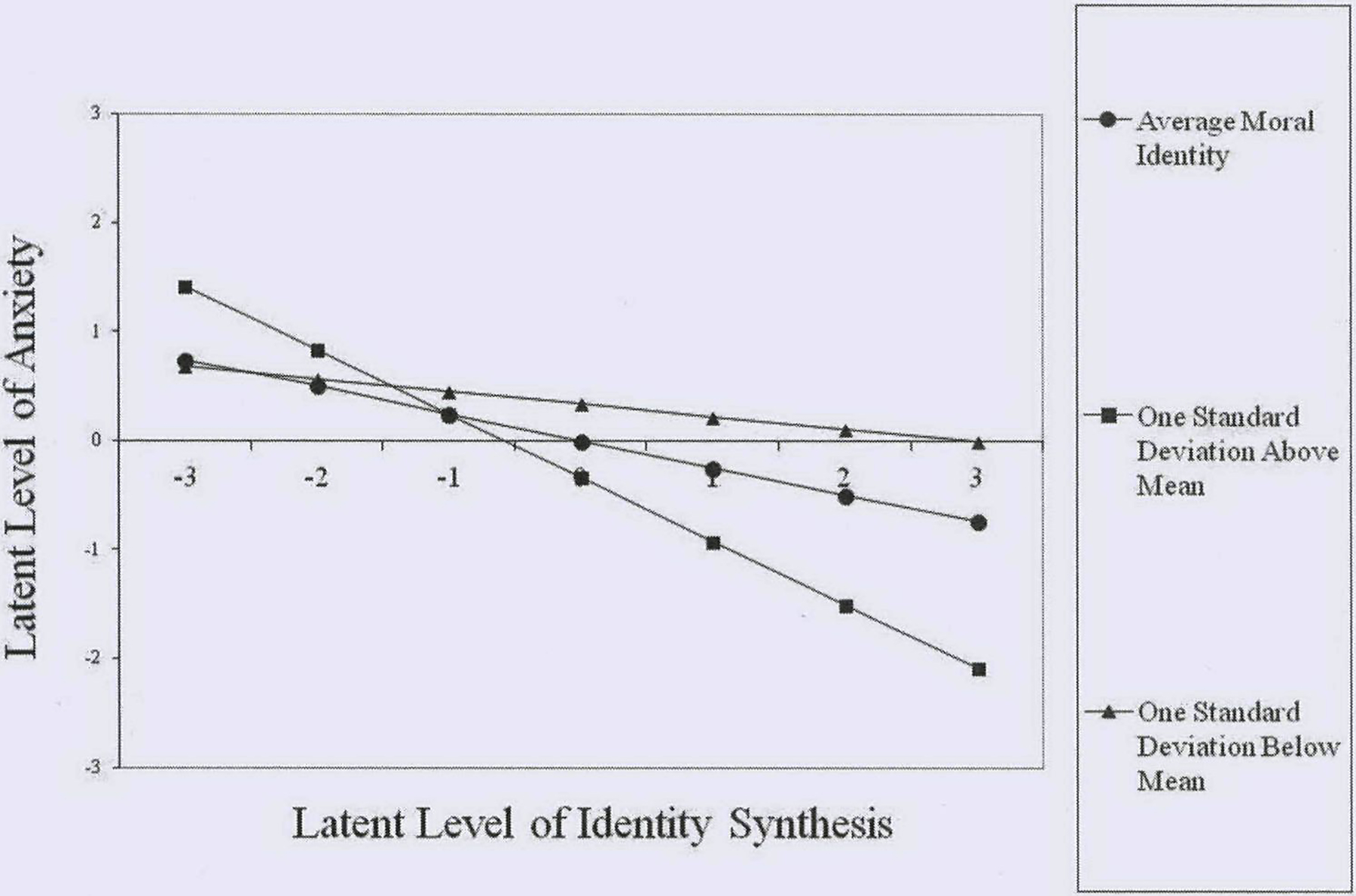
Interaction Plot of Link between Identity Synthesis and Anxiety at Various Levels of Moral Identity.
Figure 7.
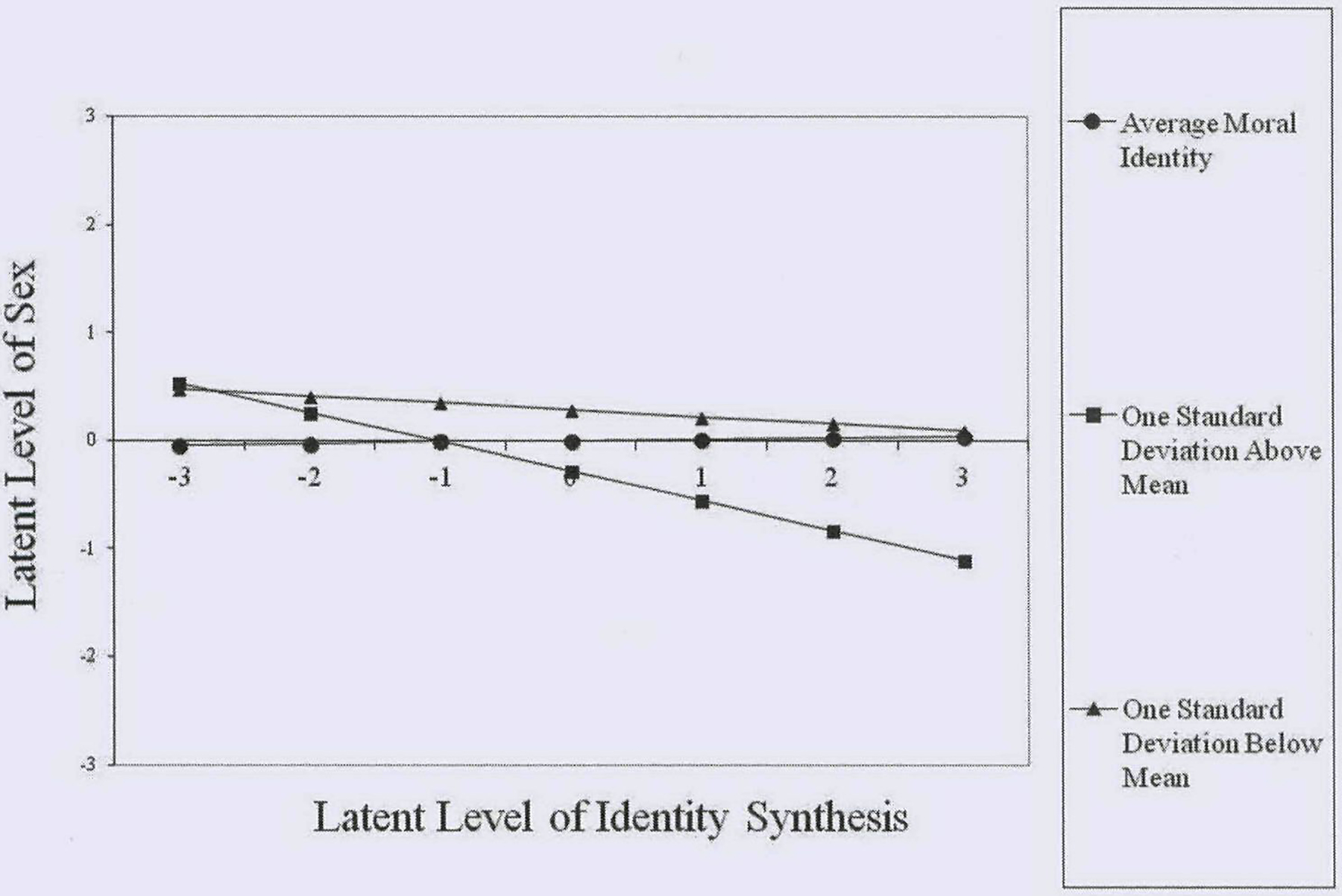
Interaction Plot of Link between Identity Synthesis and Sexual Risk Taking at Various Levels of Moral Identity
Figure 8.
Interaction Plot of Link between Identity Synthesis and Self-Esteem at Various Levels of Moral Identity.
Acknowledgments
We are grateful to Seth Schwartz and the rest of the MUSIC collaborative for their work with the research design, data collection, and data management. We also appreciate Elliot Tucker-Drob, Joseph Olsen, Chongming Yang and Zhiyong “Johnny” Zhang for statistical consultation.
References
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. [Google Scholar]
- Amonini C , & Donovan RJ (2006). The relationship between youth’s moral and legal perceptions of alcohol, tobacco and marijuana and use ofthese substances. Health Education Research. 21(2), 276–286. doi: 10.1093/her/cyh064 [DOI] [PubMed] [Google Scholar]
- Aquino K, Freeman D, Reed A II., Lim VKG, & Felps W (2009). Testing a social cognitive model of moral behavior: The interactive influence of situations and moral identity centrality. Journal of Personality and Social Psychology, 97, 123–141. doi: 10.1037/a0015406 [DOI] [PubMed] [Google Scholar]
- Aquino K, & Reed AI (2002). The self-importance of moral identity. Journal of Personality and Social Psychology, 83, 1423–1440. doi: 10.1037//0022-3514.83.6.1423 [DOI] [PubMed] [Google Scholar]
- Archer SL (2008). Identity and interventions: An introduction. Identity: An International Journal of Theory and Research, 8, 89–94. doi: 10.1080/15283480801938127 [DOI] [Google Scholar]
- Arnett JJ (2004). Emerging adulthood: The winding road from late teens through the twenties. New York, NY: Oxford University Press. [Google Scholar]
- Barriga AQ, Morrison EM, Liau AK, & Gibbs JC (2001). Moral cognition: Explaining the gender difference in antisocial behavior. Merrill-Palmer Quarterly, 47, 532–562. doi: 10.1353/mpq.2001.0020 [DOI] [Google Scholar]
- Basak R, & Ghosh A (2008). Ego-identity status and its relationship with self-esteem in a group of late adolescents. Journal of the Indian Academy of Applied Psychology, 34, 337–344. [Google Scholar]
- Beck AT, Epstein N, Brown G, & Steer RA (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Counseling and Clinical Psychology, 56, 893–897. Retrieved from http://https://www.lib.byu.edu/cgi-bin/remoteauth.pl?url=http://search.ebscohost.com/login.aspx?direct=true&db=pdhi&AN=ccp-56-6-893&site=ehost-live&scope=site [DOI] [PubMed] [Google Scholar]
- Berman SL, Kennerley RI , & Kennerley MA (2008). Promoting adult identity development: A feasibility study of a university-based identity intervention program. Identity: An International Journal of Theory and Research, 8, 139–150. doi: 10.10S0/15283480801940024 [DOI] [Google Scholar]
- Bishop DI, Weisgram ES, Holleque KM, Lund KE, & Wheeler-Anderson JR (2005). Identity development and alcohol consumption: Current and retrospective reports by college students. Journal of Adolescence, 28, 523–533. doi: 10.I016/j.adolescence.2004.10.007 [DOI] [PubMed] [Google Scholar]
- Blasi A (1993). The development of identity: Some implications for moral functioning In Noam GG, Wren TE, Nunner-Winkler G & Edelstein W (Eds.), Studies in contemporary German social thought (pp. 99–122). Cambridge, MA: The MIT Press. [Google Scholar]
- Blasi A (2004b). Neither personality nor cognition: An alternative approach to the nature of the self In Lightfoot C, Lalonde C, & Chandler M (Eds.), Changing conceptions of psychological life (pp. 3–25). Mahwah, NJ: Erlbaum. [Google Scholar]
- Brown TA (2006). Confirmatory factor analysis for applied research. New York, NY: Guilford Press. [Google Scholar]
- Cheung GW, & Rensvold RB (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9, 233–255. [Google Scholar]
- Clarke GN, Lewinsohn PM, Hops H, & Seeley JR (1992). A self- and parent-report measure of adolescent depression: The Child Behavior Checklist Depression scale (CBCL-D). Behavioral Assessment, 14,443–463. [Google Scholar]
- Colby A, & Damon W (1992). Some do care: contemporary lives of moral commitment. New York, NY:Free Press. [Google Scholar]
- Côté JE, & Bynner JM (2008). Changes in the transition to adulthood in the UK and Canada: The role of structure and agency in emerging adulthood. Journal of Youth Studies, 11, 251–268. doi: 10.1080/13676260801946464 [DOI] [Google Scholar]
- Côté JE, & Levine CG (2002). Identity formation, agency, and culture: A social psychological synthesis. Mahwah, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Crocetti E, Klimstra T, Keijsers L, Hale WW II, & Meeus W (2009). Anxiety trajectories and identity development in adolescence: A five-year longitudinal study. Journal of Youth and Adolescence, 38, 839–849. doi: 10.1007/sl0964-008-9302-y [DOI] [PubMed] [Google Scholar]
- Crocker J (2002). Contingencies of self-worth: Implications for self-regulation and psychological vulnerability. Self and Identity, 1, 143–149. [Google Scholar]
- Damon W, & Hart D (1992). Self-understanding and its role in social and moral development In Bornstein MH & Lamb ME (Eds.), Developmental psychology: An advanced textbook (3rd ed., pp. 421–464). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Doyle SR, Donovan DM, & Kivlahan DR (2007). The factor structure of the Alcohol Use Disorders Identification Test (AUDIT). Journal of Studies on Alcohol and Drugs, 68, 474–479. [DOI] [PubMed] [Google Scholar]
- Dunkel CS, Mathes E, & Harbke C (2011). Life history strategy, identity consolidation, and psychological well-being. Personality and Individual Differences, 51, 34–38. doi: 10.1016/j.paid.2011.03.005 [DOI] [Google Scholar]
- Erikson EH (1963). Childhood and society (2nd ed.). New York, NY: Norton. [Google Scholar]
- Erikson EH (1968). Identity: Youth and crisis. New York, NY: Norton. [Google Scholar]
- Ferris DL, Brown DJ, Lian H, & Keeping LM (2009). When does self-esteem relate to deviant behavior? The role of contingencies of self-worth. Journal of Applied Psychology, 94, 1345–1353. doi: 10.1037/a0016115 [DOI] [PubMed] [Google Scholar]
- Forthun LF, & Montgomery MJ (2009). Profiles of adolescent identity development: Response to an intervention for alcohol/other drug problems. Alcoholism Treatment Ouarterly, 27, 132–149. doi: 10.1080/07347320902784759 [DOI] [Google Scholar]
- Frimer JA, & Walker LJ (2009). Reconciling the self and morality: An empirical model of moral centrality development. Developmental Psychology, 45, 1669–1681. doi: 10.1037/a0017418 [DOI] [PubMed] [Google Scholar]
- Glenn AL, Koleva S, Iyer R, Graham J, & Ditto PH (2010). Moral identity in psychopathy. Judgment and Decision Making, 5(7), 497–505. [Google Scholar]
- Haggar MS, Anderson M, Kyriakaki M, & Darkings S (2007). Aspects of identity and their influence on intentional behavior: Comparing effects for three health behaviors. Personality and Individual Differences, 42, 355–367. doi: 10.1016/j.paid.2006.07.017 [DOI] [Google Scholar]
- Hardy SA (2006). Identity, reasoning, and emotion: An empirical comparison of three sources of moral motivation. Motivation and Emotion, 30, 207–215. doi: 10.1007/s11031-006-9034-9 [DOI] [Google Scholar]
- Hardy SA, Bhattacharjee A, Aquino K, & Reed A II. (2010). Moral identity and psychological distance: The case of adolescent parental socialization. Journal of Adolescence, 33, 111–123. doi: 10.1016/j.adolescence.2009.04.008. [DOI] [PubMed] [Google Scholar]
- Hardy SA, & Carlo G (2011a). Moral identity In Schwartz SJ, Luyekx K, & Vignoles VL (Eds.), Handbook of identity theory and research. Vol 2: Domains and categories (pp. 495–513). New York, NY: Springer. [Google Scholar]
- Hardy SA, & Carlo G (2011b). Moral identity: What is it, how does it develop, and is it linked to moral action? Child Development Perspectives, 5, 212–218. doi: 10.1111/j.1750-8606.2011.00189.x [DOI] [Google Scholar]
- Higgins-D’Alessandro A, & Power CF (2005). Character, responsibility, and the moral self In Lapsley DK & Power FC (Eds.), Character psychology and character education (pp. 101–120). Notre Dame, IN: University of Notre Dame Press. [Google Scholar]
- Kann L, Kinchen SA, Williams BI, Ross JG, Lowry R, Hill CV, … State and Local YRBSS Coordinators (1998). Youth Risk Behavior Surveillance-United States, 1997. Journal of Sehool Health, 68, 355–369. [DOI] [PubMed] [Google Scholar]
- Klein A, & Moosbrugger H (2000). Maximum likelihood estimation of latent interaction effects with the LMS method. Psychometrika, 65, 457–474. [Google Scholar]
- Kroger J (2007). Identity development: Adolescence through adulthood (2nd ed.). Thousand Oaks, CA:Sage. [Google Scholar]
- Kurtines WM, Montgomery MJ, Eichas K, Ritchie R, Garcia A, & Albrecht R (2008). Promoting positive identity development in troubled youth: A developmental intervention science out-reach research approach. Identity: An International Journal of Theory and Research, 8, 125–138. doi: 10.1080/1528348080I938515 [DOI] [Google Scholar]
- Lewis MA, Phillippi J, & Neighbors C (2007). Morally based self-esteem, drinking motives, and alcohol use among college students. Psychology of Addictive Behaviors, 21(3), 398–403. doi: 10.1037/0893-164X.21.3.398 [DOI] [PubMed] [Google Scholar]
- Luyckx K, Schwartz SI, Berzonsky MD, Soenens B, Vansteenkiste M, Smits I, & Goossens L (2008). Capturing ruminative exploration: Extending the four-dimensional model of identity formation in late adolescence. Journal of Research in Personality, 42, 58–82. doi: 10.1016/j.jrp.2007.04.004 [DOI] [Google Scholar]
- Luyckx K, Soenens B, Goossens L, Beckx K, & Wouters S (2008). Identity exploration and commitment in late adolescence: Correlates of perfectionism and mediating mechanisms on the pathway to well-being. Journal of Social and Clinical Psychology, 27, 336–361. doi: 10.1521/jscp.2008.27.4.336 [DOI] [Google Scholar]
- Moshman D (2011). Adolescent rationality and development: Cognition, morality, and identity (3rd ed.). New York, NY: Psychology Press. [Google Scholar]
- Muthén LK, & Muthén BO (1998–2010). Mplus User’s Guide (6th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Oyserman D, & Destin M (2010). Identity-based motivation: Implications for interventions. The Counseling Psychologist, 38, 1001–1043. doi: 10.1177/0011000010374775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oyserman D, & James L (2011). Possible identities In Schwartz SJ, Luyckx K, & Vignoles VL (Eds.), Handbook of identity theory and research. Vol 1: Structure and process (pp. 117–145). New York, NY: Springer. [Google Scholar]
- Park LE, & Maner JK (2009). Does self-threat promote social connection? The role of self-esteem and contingencies of self-worth. Journal of Personality and Social Psychology, 96, 203–217. doi: 10.1037/a0013933 [DOI] [PubMed] [Google Scholar]
- Pratt MW, Arnold ML, & Lawford H (2009). Growing towards care: A narrative approach to prosocial moral identity and generativity of personality in emerging adulthood In Narvaez D & Lapsley DK (Eds.), Personality, identity, and character: Explorations in moral psychology (pp. 295–315). New York, NY: Cambridge University Press. [Google Scholar]
- Pratt MW, Hunsberger B, Pancer SM, & Alisat S (2003). A longitudinal analysis of personal values socialization: Correlates of a moral self-ideal in late adolescence. Social Development, 12, 563–585. doi: 10.1111/1467-9507.00249 [DOI] [Google Scholar]
- Radloff LS (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. doi: 10.1177/014662167700100306 [DOI] [Google Scholar]
- Rosenberg M (1989). Society and the adolescent self-image. Princeton, NJ: Princeton University Press. [Google Scholar]
- Rosenthal DA, Gurney RM, & Moore SM (1981). From trust to intimacy: A new inventory for examining Erikson’s stages of psychosocial development. Journal of Youth and Adolescence, 10, 525–537. doi: 10.1007/BF02087944 [DOI] [PubMed] [Google Scholar]
- Roth M, Decker O, Herzberg PY, & Brähler E (2008). Dimensionality and norms of the Rosenberg Self-esteem Scale in a German general population sample. European Journal of Psychological Assessment, 24, 190–197. doi: 10.1027/1015-5759.24.3.190 [DOI] [Google Scholar]
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, & Grant M (1993). Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction, 88,791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Luyckx K, & Vignoles VL (Eds.) (2011). Handbook of identity theory and research. New York, NY: Springer. [Google Scholar]
- Schwartz SJ, Mason CA, Pantin H, Wang W, Brown CH, Campo AE, & Szapocznik A (2009). Relationships of social context and identity to problem behaviors among high-risk Hispanic adolescents. Youth & Society, 40, 541–570. doi: 10.1177/0044118x08327506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith C, Christoffersen K, Davidson H, & Herzog PS (2011). Lost in transition: The dark side of emerging adulthood. New York, NY: Oxford University Press. [Google Scholar]
- Soenens B, Berzonsky MD, Dunkel CS, Papini DR, & Vansteenkiste M (2011). Are all identity commitments created equal? The importance of motives for commitment for late adolescents’ personal adjustment. International Journal of Behavioral Development, 35, 358–369. [Google Scholar]
- Steger MF, Frazier P, Oishi S, & Kaler M (2006). The Meaning in Life Questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53, 80–93. doi: 10.1037/0022-0167.53.1.80 [DOI] [Google Scholar]
- Waterman AS (1993). Finding something to do or someone to be: A eudaimonist perspective on identity formation In Kroger J (Ed.): Discussions on ego identity (pp. 147–167). Hillsdale, NJ: Lawrence Erlbaum. [Google Scholar]
- Waterman AS, Schwartz SJ, Hardy SA, Kim SY, Lee RM, Armenta BE, … Agocha VB (2012). Good choices, poor choices: Relationship between the quality of identity commitments and psychosocial functioning. Manuscript submitted for publication. [DOI] [PMC free article] [PubMed]
- Wowra S (2007). Moral identities, social anxiety, and academic dishonesty among American college students. Ethics & Behavior, 17, 303–321. doi: 10.1080/10508420701519312. [DOI] [Google Scholar]