

Abstract
BACKGROUND:
Adolescence is a vital stage of growth and development; however, many adolescents do die prematurely due to accidents, suicide, violence, poor mental stability, depression, and other illnesses that are either preventable or treatable. Life skills are important for the promotion of well-being of adolescents and to develop positive attitude and values to lead a healthy life.
OBJECTIVES:
The study was conducted to assess the change in life skills postintervention and study the association between different variables and the postintervention life skills score.
MATERIALS AND METHODS:
A quasi-experimental study was conducted among 137 adolescents each in urban and rural schools. Life skills training module based on ten domains of life skills given by the World Health Organization was implemented using interactive teaching–learning methods. After 6 months of implementation of life skills training sessions, a postintervention assessment was done using the life skills assessment scale, and the differences in the scores were measured.
RESULTS:
Higher life skills score was observed postintervention, and this difference was statistically significant (P < 0.001). Higher postintervention mean score (above 15) was seen in critical thinking (19.58), self-awareness (18.03), creative thinking (15.78), and interpersonal thinking (15.15).
CONCLUSION:
Increase in the postintervention scores using an educational intervention module and interactive teaching–learning methods suggests effectiveness of the life skills education program. Implementing this health promotion module on life skills in the school curriculum will address the overall development of the personality of the school students.
Keywords: Adolescents, life skills, modular education program, urban and rural schools
Introduction
The World Health Organization (WHO) defines adolescents as young people aged 10–19 years. Around one in six people in the world is an adolescent, that is, about 1.2 billion are adolescents, and their numbers are increasing. It is estimated that there are almost 331 million adolescents in India, which accounts to 30% of India's population.[1,2] It is a vital stage of growth and development. It is a period of transition from childhood to adulthood, which is characterized by rapid physiological changes and psychological maturation, but they are often thought of as a healthy group. Nevertheless, many adolescents do die prematurely due to accidents, suicide, violence, poor mental stability, depression, pregnancy-related complications, and other illnesses that are either preventable or treatable. Many more suffer chronic ill-health and disability. In addition, many serious diseases in adulthood have their roots in adolescence. For example, tobacco use, sexually transmitted infections including HIV, and poor eating and exercise habits lead to illness or premature death later in life.[3]
The present scenario of adolescent clearly depicts that the condition of our youth has significantly deteriorated. One best-practice model for contributing to the healthy development of adolescents is a life skills approach. The WHO defines life skills as “the abilities for adaptive and positive behaviour that enable individuals to deal effectively with the demands and challenges of everyday life,” “Adaptive” means that a person is flexible in approach and is able to adjust in different circumstances. “Positive behaviour” implies that a person is forward looking and even in difficult situations can identify a ray of hope and opportunities to find solutions.[4]
Life skills are important for the promotion of the health and well-being of children and adolescents and to develop knowledge, positive attitude, and values to lead a healthy life in future.
The study was thereby conducted to assess the change in life skills postintervention among the study group and to study the association between different sociodemographic variables, area of residence, and the postintervention life skills score.
Materials and Methods
Study design, study setting, and study population
A quasi-experimental study was conducted among the adolescent children studying in the schools of urban and rural field practice area of Yenepoya Medical College and Hospital, Dakshina Kannada district of Karnataka, with the approval of the institutional ethical committee.
Sample size and sampling method
With pretest mean and standard deviation (SD) as 15.31 and 4.0 and postterm mean and SD as 16.31 and 4.3 based on the pilot study conducted and at 5% level of significance, assuming an increase of 10% in the mean scores of life skills after conducting the life skills education program with 80% as the power of the study, the sample size was 137. The study was conducted among 137 students in each school in urban and rural areas among students studying in VI, VII, and VIII classes.
Purposive sampling was used to select the schools, two schools, one each in urban and rural areas receiving school health services from the department of community medicine. The probability proportionate to the population size method was followed to identify the number of students to be selected from VI, VII, and VIII classes of the selected schools. A simple random sampling method was followed to select the students from each class.
Method of data collection
Permission from the principals of both schools and written informed consent from either of the parent of the study participants and assent from the adolescents were obtained.
Information sheet to record the sociodemographic profile (age, gender, class, educational status of mother, educational status of father, occupation of mother, and occupation of father) of the study participants (students) was used.
Information related to age, gender, educational status, and occupation status was collected from the parent and teacher during the focus group discussion (FGD).
Life skills assessment scale
Identifying the conceptual framework of the WHO, the Life Skills Assessment Scale was constructed to assess the level of life skills among the Indian adolescents. The questionnaire used in the study comprised fifty questions pertaining to the ten core areas recommended by the WHO that are creative thinking, critical thinking, problem-solving, decision-making, coping with stress, managing emotion, empathy, self-awareness, interpersonal skills, and effective communication[5] Each core area had five questions. Each item was scored on a 5-point Likert-type scale for the respondent to check the appropriate response which is most descriptive of him/her.
A pilot study was carried out to check the feasibility of data collection before the commencement of the study Figure 1.
Figure 1.
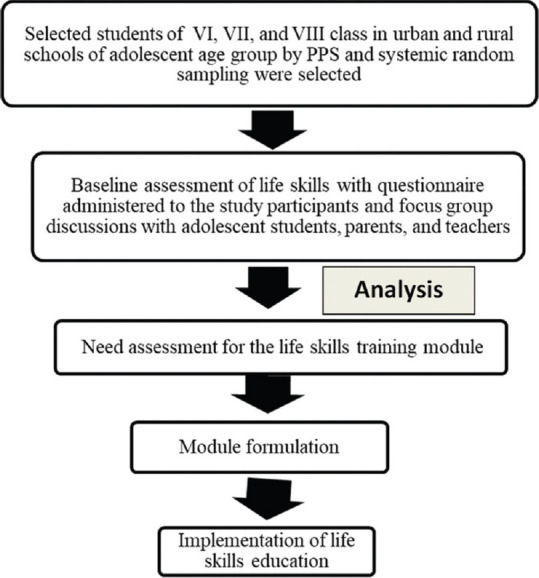
Flowchart depicting the procedure followed in the study
Phase 1: Baseline assessment
Baseline assessment of life skills level among adolescents was done using the life skills assessment scale.
Phase 2: Module formulation
The life skills training module was prepared following the needs assessment conducted by administering the Life Skills Assessment Scale for the students and FGDs with adolescents, parents, and teachers.
The module was based on ten domains of life skills given by the WHO that is decision-making, problem-solving, creative thinking, critical thinking, effective communication, interpersonal relationship, self-awareness, empathy, coping with emotions, and coping with stress.
Phase 3: Intervention
Implementation of life skills training was done using the formulated module. Each class was divided into two groups of 20–25 students each. Training was conducted in four sessions per group. Each session of life skills training lasted for 45–60 min. Teaching–learning methods for life skill training included stories, powerpoint presentations, charts, flip charts, blackboard, role play, games, and various group activities with active participation by students.
Phase 4: Postintervention assessment
After 6 months of implementation of life skills training sessions, postintervention assessment was done using the life skills assessment scale, and the differences in the scores were measured.
Data analysis
The data were analyzed using the Statistical Package for the Social Sciences software version 22.0. (Armonk, NY: IBM Corp). Descriptive statistics are reported as mean (SD) for continuous variables and frequency and percentages for categorical variables. Paired t-test is applied to study the differences in the mean scores of life skills (pre- and postintervention), and linear regression test is applied to identify the predictors of postintervention life skills scores.
Results
The study was conducted among 137 adolescents of rural and urban schools each. Majority of the participants were in the age group of 10–12 years and males. Our study comprised 33% of the students from 6thclass, followed by 32% from 7thclass, and 35% from 8thclass. Educational status of the mothers of study participants was majorly confined up to high school (53%), and 81% of the mothers were homemaker. Majority of the fathers of study participants were educated above high school.
The mean (SD) life skills score after the life skills modular training was 152.85 (29.54) as compared to 128.93 (27.24) before the intervention. The mean difference between post- and preintervention was 23.91 and was statistically significant (P < 0.001).
Table 1 shows domain-wise mean life skills score pre- and postintervention among the total study participants. Higher postintervention mean score (above 15) was seen in critical thinking (19.58), self-awareness (18.03), creative thinking (15.78), and interpersonal thinking (15.15). Postintervention mean score was higher than the preintervention mean score in all the ten domains of life skills. On applying paired t-test, the difference was statistically significant (P < 0.001).
Table 1.
Domain-wise mean life skills score before and after intervention among the total study participants (n=274)
| Life skills domains | Mean (SD) | MD** | t | CI | df*** | P | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Self -awareness | |||||||
| Postintervention | 18.03 (3.3) | 4.8 | 14.78 | 4.23 | 5.542 | 273 | <0.001* |
| Preintervention | 13.14 (3.9) | ||||||
| Critical thinking | |||||||
| Postintervention | 19.58 (2.5) | 5.2 | 16.70 | 4.67 | 5.924 | 273 | <0.001* |
| Preintervention | 14.28 (4.6) | ||||||
| Creative thinking | |||||||
| Postintervention | 15.78 (3.7) | 2.5 | 8.19 | 1.90 | 3.114 | 273 | <0.001* |
| Preintervention | 13.27 (3.9) | ||||||
| Effective communication | |||||||
| Postintervention | 13.23 (4.7) | 1.5 | 4.05 | 0.78 | 2.255 | 273 | <0.001* |
| Preintervention | 11.72 (4.2) | ||||||
| Interpersonal skills | |||||||
| Postintervention | 15.15 (5.0) | 2.0 | 5.52 | 1.33 | 2.807 | 273 | <0.001* |
| Preintervention | 13.08 (4.4) | ||||||
| Managing emotions | |||||||
| Postintervention | 14.09 (5.1) | 0.7 | 2.33 | 0.11 | 1.394 | 273 | <0.001* |
| Preintervention | 13.34 (3.9) | ||||||
| Coping with stress | |||||||
| Postintervention | 14.88 (5.2) | 2.4 | 6.25 | 1.70 | 3.267 | 273 | <0.001* |
| Preintervention | 12.39 (4.2) | ||||||
| Empathy | |||||||
| Postintervention | 14.95 (5.3) | 1.6 | 3.69 | 0.77 | 2.551 | 273 | <0.001* |
| Preintervention | 13.28 (5.5) | ||||||
| Decision-making | |||||||
| Postintervention | 13.13 (4.4) | 1.1 | 3.09 | 0.40 | 1.802 | 273 | <0.001* |
| Preintervention | 12.03 (3.6) | ||||||
| Problem-solving | |||||||
| Postintervention | 14.01 (4.6) | 1.6 | 4.47 | 0.90 | 2.334 | 273 | <0.001* |
| Preintervention | 12.39 (4.3) | ||||||
*Statistically significant, **MD=Mean difference, ***DF=Degree of freedom. CI=Confidence interval, SD=Standard deviation, *statistically significant
Table 2 shows predictors (area of the school, age, class, educational status of mother, and educational status of father), and we see that rural locality is the statistically significant (P < 0.001) correlate of life skills.
Table 2.
Univariate linear regression analysis of association between postintervention total mean score and sociodemographic variables
| Sociodemographic variables | B (regression coefficient) | SE | t | P | 95% CI for B | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Urban | −25.643 | 5.958 | 4.30 | <0.001* | 13.91 | 37.37 |
| 13-16 years | −7.434 | 4.242 | 1.75 | 0.081 | 0.91 | 15.78 |
| Class | −3.367 | 2.597 | 1.29 | 0.196 | 1.74 | 8.48 |
| Educational status of mother above high school | 2.142 | 2.158 | 0.99 | 0.322 | 2.10 | 6.39 |
| Educational status of father above high school | 0.446 | 1.544 | 0.28 | 0.773 | 2.59 | 3.48 |
CI=Confidence interval, SE=Standard error
Discussion
In this study, the mean life skills score after the life skills modular training was 152.85 ± 29.54 as compared to 128.93 ± 27.24 before the intervention. The mean difference between post- and preintervention was statistically significant (P < 0.001). Similar results were also seen in the study conducted by Mekala et al.[6] and Kaur[7] in Coimbatore and Ludhiana, respectively, where postintervention scores showed significant improvement as compared to the baseline life skills score (P < 0.001). This reflects the strong need for life skills training among adolescents which will enable them to identify the challenges in life and will prepare them for better future.
The study assessed domain-wise mean life skills score before and after intervention among the study participants. Higher postintervention mean score (above 15) was seen in critical thinking (19.58), self-awareness (18.03), creative thinking (15.78), and interpersonal thinking (15.15), and this difference was statistically significant. This shows that life skills training was very effective for adolescents, and this will empower them with essential skills to have positive attitude in life. The findings are supported by Mekala et al.[6] in Coimbatore where all the ten life skills domains showed statistically significant improvement in score postintervention (P < 0.001). Different findings were noticed by Srikala and Kishore[8] who conducted a study on empowering adolescents with life skills education in schools in Bangalore rural area and Udupi in year 2002, where the adolescents in the program had only significantly better self-esteem (P = 0.002), perceived adequate coping (P < 0.001), better adjustment (P < 0.001), and prosocial behavior (P = 0.001). Kaur[7] conducted a study in Ludhiana among sixty college students. He found positive impact of the life skills-based intervention program on the emotional intelligence abilities, self-awareness domain of life skills among respondents.
As per the univariate linear regression, only rural locality was the statistically significant (P < 0.001) correlate of life skills for postintervention life skills score group. A similar result was seen in a study conducted by Yoshimura et al.[9] where they observed that urban and semi-urban schools had higher scores than rural schools in the areas of, “personal health and life skills” in Japan. However, Kaur[10] found that rural school-going adolescents (120.08 ± 13.71) possess significantly more life skills than urban adolescents. A study done by Junge[11] reported that life skill differs as a function of age, gender, and ethnicity. This was different as compared to our study findings; it may be because of different geographical and cultural context. Anuradha studied life skills and self-concept of adolescents and found a moderate association between life skills and father's education and family income.[12]
The study has few strengths. This is one of the few studies conducted in India. We used simple random sampling to select the students, thus limiting the selection bias. The development of need-based structure life skills educational module based on FGD conducted with students, parents, and teachers tried to bridge the gap. We recommend the use of this module for the implementation of life skills training in schools. Interactive teaching–learning methods were used in modular training facilitated active learning.
The study has few limitations. First, the study was conducted in select schools from urban and rural areas. Thereby, we may not be able to generalize the findings. Second, we have not been able to assess the effect of socioeconomic status as a confounding variable.
The study has few implications and recommendations. First, the study showed higher postintervention scores. The health and family welfare department in collaboration with the department of education can adopt this model life skills education. Second, with the rising burden of mental health issues and peer pressure in adolescent age, training on life skills will play an important role in the personality development of the students.
Conclusion
This study observed an increase in the postintervention life skills scores among school students using an educational intervention module and interactive teaching–learning methods. Higher scores were observed in most of the domains of life skills in the postintervention phase. Implementing this modular training on life skills in the school curriculum will promote the personality development of the students and enable them to handle the different challenges in life.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors gratefully acknowledge the support of school authorities and teachers who cooperated during the data collection process.
References
- 1.World Health Organization. Adolescent Health. [Last accessed on 2020 Jun 14]. Available from: https://www.who.int/maternal_child_adolescent/documents/adolescent/en/
- 2.Progress for Children: A Report Card on Adolescents. Socio-Demographic Profile of Adolescents. UNICEF; 2012. [Last accessed on 2020 Jun 14]. Available from: http://www.unicef.org/publications/files/Progress_for_Children_-_No._10_EN_04232012.pd . [Google Scholar]
- 3.Dinesh R, Belinda R. Importance of life skills education for youth. Indian J Appl Res. 2014;4(12):92–4. [Google Scholar]
- 4.Ruchismita R. Essay on the Concept and Importance of Life Skill Education. 2016. [Last accessed on 2020 Jun 14]. Available from: http://www.laqsh.com/index.php/articles/100-life-skills/329essay-on-theconcept-and-importance-of-life-skill-education.html .
- 5.Subasree R, Nair AR. The Life Skills Assessment Scale: The construction and validation of a new comprehensive scale for measuring Life Skills. IOSR J Humanities Soc Sci. 2014;19:50–8. [Google Scholar]
- 6.Mekala CV, Aras R, Devadason JM. Effectiveness of behavioral change communication (Bcc) on life skills (Ls) for youth. Indian J Appl Res. 2015;5(4):631–33. [Google Scholar]
- 7.Kaur TD. Study of impact of life skills intervention training on emotional intelligence of college adolescents. Indian J Psychol Sci. 2011;2:112–25. [Google Scholar]
- 8.Srikala B, Kishore KK. Empowering adolescents with life skills education in schools – School mental health program: Does it work? Indian J Psychiatry. 2010;52:344–9. doi: 10.4103/0019-5545.74310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yoshimura N, Jimba M, Poudel KC, Chanthavisouk C, Iwamoto A, Phommasack B, et al. Health promoting schools in urban, semi-urban and rural Lao PDR. Health Promot Int. 2009;24:166–76. doi: 10.1093/heapro/dap004. [DOI] [PubMed] [Google Scholar]
- 10.Kaur M. Life skills among school going adolescents in relation to certain personal variables. MIER J Edu Stud Trends Pract. 2014;4:218–30. [Google Scholar]
- 11.EBSCO HOST connection. Building Life Skills through After School Participation in Experimental and Co-operative Learning. [Last accessed on 2020 Jun 14];Child Study Journal. 2003 33(3):165. Available from: http://connection.ebscohost.com/c/articles/13055413/building-life-skills-through-afterschool-participationexperimental-cooperative-learning . [Google Scholar]
- 12.Anuradha K. Life skills and self-concept of adolescents. Int J Sci Res. 2014;3(11):600–04. [Google Scholar]