

Abstract
Background
Self-efficacy and fear of re-injury have been documented as factors related to an athlete’s ability to return-to-sport after anterior cruciate ligament (ACL) reconstruction. The purpose of this study was to compare psychological readiness between athletes injured in their primary mode of sport versus those injured outside of their primary sport following ACL reconstruction.
Hypothesis
Athletes sustaining ‘in-sport’ injuries will demonstrate poorer psychological readiness when compared their matched counterparts injured outside of their primary sport.
Study Design
Case-Control Study
Methods
A single-surgeon database of 638 patients following ACL reconstruction was used to conduct a matched case-control analysis. Psychological readiness was examined 16-weeks postoperatively using the ACL-Return to Sport after Injury (ACL-RSI) questionnaire with subgroup analyses for the ‘emotional’, ‘confidence’ and ‘injury-risk’ subscales. Subject matching was performed for baseline patient and surgical demographics. All statistical comparisons were performed using a one-way (group) analysis variance (ANOVA) at a significance level of α = .05.
Results
Ninety-two matched patients (49 ‘in-sport’ injuries, 43 ‘out-of-sport’ injuries) were included in the final analysis. The ‘in-sport’ group exhibited significantly lower total ACL-RSI scores (55.3 ±12.9 versus 60.8 ±11.6, t = 2.747, P < .001) when compared to the ‘out-of-sport’ group. Subscale comparisons indicated lower ‘emotional’ (P < .016) and higher ‘injury risk’ (P < .001) psychological constructs for ‘in-sport’ athletes versus ‘out-of-sport’ athletes. No differences were found between groups for the ‘confidence’ subscale (P = .987).
Conclusions
Athletes sustaining ‘in-sport’ ACL injuries demonstrated poorer psychological readiness when compared to athletes injured outside their primary sport when in preparation for return-to-sport activities following ACL reconstruction.
Clinical Relevance
Clinicians should consider the potential impact of mode of injury on psychological readiness when returning athletes to sport after ACL reconstruction.
Keywords: acl injury, return to sport, mode-of-injury, psychological readiness
INTRODUCTION
There is an emerging body of evidence linking psychological factors to return-to-sport rates following ACL reconstruction.1–5 Previous research has reported that 52% of high school athletes and 50% of collegiate athletes who underwent ACL reconstruction chose not to return-to-sport due to fear of re-injury.6 These psychological factors also appear to have lasting consequences as athletes reporting a higher fear of reinjury display relatively lower return-to-sport rates for up to seven years following surgical reconstruction.3,7,8 In contrast, athletes who successfully return to their preinjury level of participation often exhibit more positive responses to psychological outcome measures, including higher knee-related quality of life,9 greater self-reported patient satisfaction,10 and a lower fear-avoidance behaviors when compared to those who are unable to return to their preinjury participation level.11,12 Furthermore, greater psychological readiness during rehabilitation has been shown to be a significant predictor of return to comparable level of performance.13
Prior studies have demonstrated that traumatic injuries often lead to altered psychological responses which negatively impact the recovery process.3,9,14–18 The theory of contextual fear conditioning, also known as classical conditioning, states that a neutral stimulus can become conditioned when paired with an aversive unconditioned stimulus, such as pain.19 When an injury occurs, the activity at the time of injury can become a conditioned stimulus to the individual, resulting in a heightened fear response. Behaviorists have developed models based on this theory in which classically conditioned fear acts as a driver that motivates and reinforces activity avoidance behaviors.19 Based on this theory, patients participating in their respective sport at the time of injury would, theoretically, report a higher ‘fear of re-injury’ compared to those who were injured outside of their primary sport. For example, a collegiate soccer player who injures her ACL in soccer practice would potentially demonstrate an increased fear of re-injury when returning to soccer versus an American football player who sustains an ACL injury during a recreational basketball game. Unfortunately, no known clinical studies have been conducted to test this hypothesis in an ACL reconstruction population. Additionally, current literature suggests that psychological factors are potentially modifiable, and should be evaluated in athletes over time.13 This recommendation was supported by the work of Ardern and colleagues which demonstrated that lower Anterior Cruciate Ligament-Return to Sport after Injury scale (ACL-RSI) scores assessed at 16-weeks following surgical reconstruction was a sensitive predictor for determining successful return to sport at 12-months.11 Therefore, the purpose of this study was to determine whether athletes who sustain ‘in-sport’ ACL injuries exhibited poorer psychological readiness scores as assessed by the ACL-RSI scale when compared to matched subjects who sustain their injury outside their primary mode of sport following surgical reconstruction. The authors hypothesize that athletes who sustain an ‘in-sport’ ACL injury will display lower psychological readiness scores when compared to their ‘out-of-sport’ counterparts at 16-weeks following surgical reconstruction.
METHODS
Study Design
A matched-case control study was conducted at the University of Texas Health Sciences Center examining a subset of patients enrolled within a larger prospective clinical trial. All eligible participants provided verbal and written consent that was approved by the University of Texas Health Sciences Center Institutional Review board. This study is registered at US National Institutes of Health (clinicaltrials.gov) as NCT # 03700996.
Participants
Recreational athletes with intentions of returning to their primary sport prior to undergoing ACL reconstruction were identified for study participation. Patients between 15 and 50 years of age were included if they received a unilateral ACL autograft reconstruction and regularly participated in level 1 or II sports (jumping, cutting, pivoting, and lateral movements) prior to surgery.20 Those undergoing multiple ligament reconstruction, revision ACL reconstruction, ACL repair, or complex concomitant meniscus and/or chondral procedures that would delay weight-bearing were excluded from participation. Subjects were regarded as ‘in-sport’ if they reported sustaining their ACL injury while participating in their self-reported primary mode of sport and ‘out-of-sport’ if they reported their injury occurring outside of their reported primary mode of sport.
Psychological Assessment
Psychological readiness was assessed using the ACL-RSI at 16-weeks following ACL reconstruction.21 This 12-item questionnaire evaluates three constructs of psychological involvement proposed to be associated with return-to-sport including confidence in performance, risk appraisal, and emotion. Previous studies have found the ACL-RSI scale to be valid, reliable, and predictive of return to preinjury level of sport following reconstruction surgery with a sensitivity of 0.97 and a specificity of 0.63.10,22,23 The 16-week assessment period was selected based on the work by Ardern and colleagues who examined the relationship between ACL-RSI scores and return-to-sport rates, discovering that athletes who scored lower than 56 on ACL-RSI at 16-weeks following reconstruction were less likely to return-to-sport at 12-months.10
Statistical Analysis
Case matching was performed using age, gender, body mass index (BMI), and preinjury activity level as determined by MARX scale with the ‘out-of-sport’ participants serving as the reference group due to the relatively fewer numbers of participants.24 Additionally, groups were matched by surgical characteristics including ACL graft type and frequency of meniscal involvement (e.g. meniscectomy/repair). Baseline patient demographics and surgical characteristics (graft type, meniscal injury) were analyzed using an independent t-test. Comparisons for ACL-RSI total scores and sub-scores between groups were analyzed using a univariate analysis of variance (ANOVA). An alpha level of .05 was selected to determine statistical significance, and IBM SPSS version 24 (Chicago, III, USA) was used for all statistical analyses.
RESULTS
From a cohort 638 patients undergoing ACL reconstruction, 187 met the inclusion criteria of the study, with 144 (29.3%) patients qualifying as an ‘in-sport’ injury and 43 (6.7%) patients sustaining ‘out-of-sport’ injuries (Figure 1). After patient matching the ‘in-sport’ contained 49 (7.7%) of similar age, gender and surgical profile (Table 1). A detailed list of activities in which patients had sustained their ACL injury is provided in Table 2.
Figure 1: Study Design.
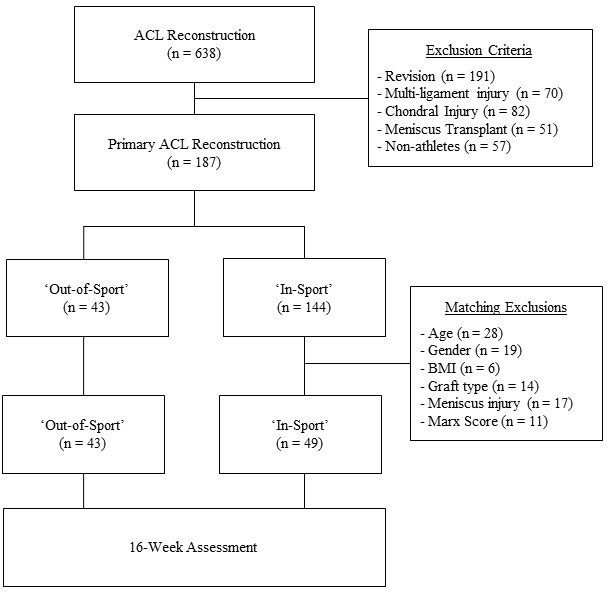
Table 1: Baseline Patient Demographics.
| In-sport (n = 49) | Out-of-sport (n = 43) | P-Value | |
|---|---|---|---|
| Age (yrs) | 25.5 ±10.8 | 26.4 ±13.0 | .561 |
| Gender (%) | 28 Males (57%) | 26 Males (60.5%) | .740 |
| BMI | 24.6 ±4.1 | 25.2 ±5.3 | .472 |
| Graft Type (n, %) Bone Patellar-Tendon Bone Hamstring Quadriceps |
45 (91.8%) 3 (6.1%) 1 (2.0%) |
40 (88.6%) 2 (4.7%) 1 (2.3%) |
.976 |
| Meniscus Repair (n, %) | 39 (79.6%) | 35 (81.4%) | .984 |
| MARX Scale (0-16) | 10.7 ± 5.0 | 10.4 ± 5.2 | .883 |
| Data reported as mean ± standard deviation | |||
Table 2: Mechanism of Injury.
| Activity | In-Sport (n = 49) | Out-of-Sport (n = 43) |
|---|---|---|
| Football | 13 (26.5)* | 9 (20.9) |
| Basketball | 7 (14.3) | 3 (7.0) |
| Baseball/Softball | 3 (6.1) | - |
| Soccer | 10 (20.4) | 3 (7.0) |
| Volleyball | 3 (6.1) | 3 (7.0) |
| Skiing/Snowboarding | 1 (2.0) | 10 (23.3) |
| Martial Arts | 1 (2.0) | 1 (2.3) |
| Running | 1 (2.0) | 2 (4.7) |
| Hockey | 1 (2.0) | 1 (2.3) |
| Rugby | 1 (2.0) | - |
| Lacrosse | 2 (4.1) | - |
| Dance | 1 (2.0) | - |
| Badminton | 1 (2.0) | - |
| Motocross | 1 (2.0) | 1 (2.3) |
| Trampoline | 1 (2.0) | 2 (4.7) |
| Field Events | 2 (4.1) | 1 (2.3) |
| Exercise | - | 2 (4.7) |
| Bowling | - | 1 (2.3) |
| Motor Vehicle Accident | - | 1 (2.3) |
| Slip/Fall | - | 3 (7.0) |
| *Data are presented as n (%) | ||
Between-group differences at 16 weeks were observed for the ‘out-of-sport’ group demonstrating higher ACL-RSI scores (60.8 ±11.6 versus 55.3 ±12.4, t = 2.747, P < .001) when compared to the ‘in-sport’ group. Further analysis of the ACL-RSI subscales indicated that the ‘out-of-sport’ group demonstrated higher sub-scores on the ‘emotional’ (53.9 ±16.8 versus 45.9 ±17.2, t = 2.042, P < .016) and ‘injury risk appraisal’ (68.5 ±16.2 versus 61.3 ±14.7, t = 3.243, P < .001) subscales. There were no differences between groups for the ‘confidence’ subscale (63.2 ±11.6 versus 63.1 ±12.9, t = .018, P = .987) of the ACL-RSI.
DISCUSSION
The purpose of this study was to determine whether athletes who sustain ‘in-sport’ ACL injuries exhibited poorer psychological readiness when compared to matched controls who sustain their injury outside their primary mode of sport following surgical reconstruction at 16-weeks. In support of our hypothesis, the ‘in-sport’ group displayed lower ACL-RSI scores when compared to athletes who sustain their injury ‘out-of-sport’. These results provide evidence to support the theory that ‘mode of injury’, specifically ‘in-sport’ injuries, can negatively impact psychological readiness scores at 16-weeks following ACL reconstruction.
The relationship between return-to-sport rates and the ACL-RSI has been well documented in previous studies.10,14,22,25,26 These studies have reported that the ACL-RSI was an effective measure with regard to its discriminative capabilities for determining return-to-sport readiness.22,26,27 Ardern and colleagues suggested that a score of less than 56 points when assessed at 16-weeks postoperatively was related to a higher likelihood of not returning to preinjury level of sport at 12 months and may help identify maladaptive psychological responses earlier in the recovery process.10 The average ACL-RSI score for “in-sport” injured athletes (55.3±12.4) in our study fell below the cutoff score, indicating that particular attention to psychological recovery may be warranted for individuals in this group. Similar work by Langford and coworkers concluded that patients who were able to return to their preinjury level of competition had an average ACL-RSI score of 72 when assessed 12-months after surgery.22 We recommend future investigators consider examining the differences between mode of injury at this timeframe to determine whether differences between groups persist out to a year. Regardless, when considering the link between low ACL-RSI scores and return-to-sport rates, clinicians should consider using strategies that enhance psychological readiness throughout all phases of rehabilitation.
The higher mean observed on the ‘injury risk’ subscale for ‘in-sport’ injuries was particularly interesting, and supports the theory of contextual fear conditioning.19 These data may be useful for future investigators and psychologists interested in the development of effective intervention strategies to potentially mitigate these negative psychological responses. Theoretically, if the impact of these negative responses could be avoided, it may potentially enhance the athletes’ ability to return to their prior level of function; however, it is necessary to conduct these studies to confirm this hypothesis.
Considering that mode of injury may negatively influence the psychological profile of athletes, it is recommended to utilize the ACL-RSI to identify athletes subject to these deficits with the goal of implementing intervention strategies early within the rehabilitation process to mitigate the negative consequences of these injury mechanisms. While there is a paucity of research regarding the utilization of these interventions in an ACL population, previous studies have demonstrated their effectiveness in fear-avoidance behaviors found in patients with low back pain,17,18,28–30 chronic disease,29 musculoskeletal pain,31 and knee osteoarthritis.32 Beyond a psychological referral, rehabilitation professionals might consider utilizing techniques including education33–35 to reduce fear-avoidance beliefs, health coaching,17 quota-based exercise,18 on-field rehab,36 and exposure therapy.28,29,37 Graded exposure involves progressive exposure to a hierarchy of situations or activities that cause fear for the purpose of showing that these activities can be completed without causing harm.28,29,37 Della Villa et al. proposed the idea of incorporating on-field rehabilitation into the recovery process of an athlete returning to sport following ACL reconstruction.36 Specifically, the authors recommend a progression from graded exposure in the clinical setting to an on-field setting in order to potentially address the environmental component of contextual fear conditioning. Caution should be used when considering these treatment recommendations as future research is warranted to examine the clinical effectiveness of these interventions for improving return-to-sport rates following ACL injury.
There are several limitations to this study which should be considered when examining these results. Previous studies have reported varying ACL-RSI cut-scores for predicting successful return-to-sport following reconstruction ranging from 56 to 76 based on the assessment timeframe.22,23,38 In the current study, we selected a 16-week assessment not only based on the previous research, but also to serve as a pragmatic means of delivering treatment interventions to patients displaying poorer psychological readiness. However, this may be considered as a limitation as only one ACL-RSI score was used to evaluate the psychological profile of athletes along the athletes’ entire continuum of care. It is recommended that future research be conducted to examine the differences between ‘in-sport’ and ‘out-of-sport’ injuries at the time of return-to-sport, and subsequently return to prior level of performance in order to validate these measures. Lastly, this sample only includes patients from a high-volume, single surgeon ACL database which may potentially limit the generalizability of these results.
CONCLUSION
Athletes who suffer ACL injuries within their primary sport exhibit poorer emotional psychological constructs, and higher self-reported injury-risk when compared to those injured outside of their primary sport following ACL reconstruction. Clinicians should consider the contextual factors involving ‘mode of injury’ when investigating psychological variables of injured athletes attempting to return-to-sport.
Conflict of Interest
Dr. Walter Lowe, MD is a paid consultant for DonJoy Inc. & Arthrex Inc. Neither DonJoy Inc. or Arthrex Inc had involvement with any phase of this study.
References
- Satisfaction With Knee Function After Primary Anterior Cruciate Ligament Reconstruction Is Associated With Self-Efficacy, Quality of Life, and Returning to the Preinjury Physical Activity. Ardern C. L., Osterberg A., Sonesson S., Gauffin H., Webster K. E., Kvist J. 2016Arthroscopy. 32(8):1631–1638 e1633. doi: 10.1016/j.arthro.2016.01.035. [DOI] [PubMed] [Google Scholar]
- Chmielewski T. L., Jones D., Day T., Tillman S. M., Lentz T. A., George S. Z. J Orthop Sports Phys Ther. 12. Vol. 38. The association of pain and fear of movement/reinjury with function during anterior cruciate ligament reconstruction rehabilitation; pp. 746–53. [DOI] [PubMed] [Google Scholar]
- Kvist J., Ek A., Sporrstedt K., Good L. Knee Surg Sports Traumatol Arthrosc. 5. Vol. 13. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction; pp. 393–7. [DOI] [PubMed] [Google Scholar]
- Lentz T. A., Zeppieri, G., Jr. George S. Z., Tillman S. M., Moser M. W., Farmer K. W., Chmielewski T. L. Am J Sports Med. 2. Vol. 43. Comparison of physical impairment, functional, and psychosocial measures based on fear of reinjury/lack of confidence and return-to-sport status after ACL reconstruction; pp. 345–53. [DOI] [PubMed] [Google Scholar]
- Morrey M. A., Stuart M. J., Smith A. M., Wiese-Bjornstal D. M. Clin J Sport Med. 2. Vol. 9. A longitudinal examination of athletes' emotional and cognitive responses to anterior cruciate ligament injury; pp. 63–9. [DOI] [PubMed] [Google Scholar]
- McCullough K. A., Phelps K. D., Spindler K. P., Matava M. J., Dunn W. R., Parker R. D., Moon Group. Reinke E. K. Am J Sports Med. 11. Vol. 40. Return to high school- and college-level football after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) cohort study; pp. 2523–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ardern C. L., Taylor N. F., Feller J. A., Webster K. E. J Sci Med Sport. 6. Vol. 15. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery; pp. 488–95. [DOI] [PubMed] [Google Scholar]
- Fear of reinjury, negative affect, and catastrophizing predicting return to sport in recreational athletes with anterior cruciate ligament injuries at 1 year postsurgery. Tripp D, Ebel-Lam. Stanish WA, et al. 2007Rehabil Psychol. 52:74–81. [Google Scholar]
- Everhart J. S., Best T. M., Flanigan D. C. Knee Surg Sports Traumatol Arthrosc. 3. Vol. 23. Psychological predictors of anterior cruciate ligament reconstruction outcomes: a systematic review; pp. 752–62. [DOI] [PubMed] [Google Scholar]
- Ardern C. L., Taylor N. F., Feller J. A., Whitehead T. S., Webster K. E. Am J Sports Med. 7. Vol. 41. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery; pp. 1549–58. [DOI] [PubMed] [Google Scholar]
- Ross M. D. J Orthop Traumatol. 4. Vol. 11. The relationship between functional levels and fear-avoidance beliefs following anterior cruciate ligament reconstruction; pp. 237–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flanigan D. C., Everhart J. S., Pedroza A., Smith T., Kaeding C. C. Arthroscopy. 8. Vol. 29. Fear of reinjury (kinesiophobia) and persistent knee symptoms are common factors for lack of return to sport after anterior cruciate ligament reconstruction; pp. 1322–9. [DOI] [PubMed] [Google Scholar]
- Webster K. E., McPherson A. L., Hewett T. E., Feller J. A. Am J Sports Med. 11. Vol. 47. Factors Associated With a Return to Preinjury Level of Sport Performance After Anterior Cruciate Ligament Reconstruction Surgery; pp. 2557–2562. [DOI] [PubMed] [Google Scholar]
- Ardern C. L. Sports Health. 3. Vol. 7. Anterior Cruciate Ligament Reconstruction-Not Exactly a One-Way Ticket Back to the Preinjury Level: A Review of Contextual Factors Affecting Return to Sport After Surgery; pp. 224–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Covassin T., Beidler E., Ostrowski J., Wallace J. Clin Sports Med. 2. Vol. 34. Psychosocial aspects of rehabilitation in sports; pp. 199–212. [DOI] [PubMed] [Google Scholar]
- Hsu C. J., Meierbachtol A., George S. Z., Chmielewski T. L. Sports Health. 2. Vol. 9. Fear of Reinjury in Athletes; pp. 162–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iles R., Taylor N. F., Davidson M., O'Halloran P. J Physiother. 4. Vol. 57. Telephone coaching can increase activity levels for people with non-chronic low back pain: a randomised trial; pp. 231–8. [DOI] [PubMed] [Google Scholar]
- Kernan T., Rainville J. J Orthop Sports Phys Ther. 11. Vol. 37. Observed outcomes associated with a quota-based exercise approach on measures of kinesiophobia in patients with chronic low back pain; pp. 679–87. [DOI] [PubMed] [Google Scholar]
- Lissek S., Powers A. S., McClure E. B., Phelps E. A., Woldehawariat G., Grillon C., Pine D. S. Behav Res Ther. 11. Vol. 43. Classical fear conditioning in the anxiety disorders: a meta-analysis; pp. 1391–424. [DOI] [PubMed] [Google Scholar]
- Daniel D. M., Stone M. L., Dobson B. E., Fithian D. C., Rossman D. J., Kaufman K. R. Am J Sports Med. 5. Vol. 22. Fate of the ACL-injured patient. A prospective outcome study; pp. 632–44. [DOI] [PubMed] [Google Scholar]
- Webster K. E., Feller J. A., Lambros C. Phys Ther Sport. 1. Vol. 9. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery; pp. 9–15. [DOI] [PubMed] [Google Scholar]
- Langford J. L., Webster K. E., Feller J. A. Br J Sports Med. 5. Vol. 43. A prospective longitudinal study to assess psychological changes following anterior cruciate ligament reconstruction surgery; pp. 377–81. [DOI] [PubMed] [Google Scholar]
- Muller U., Kruger-Franke M., Schmidt M., Rosemeyer B. Knee Surg Sports Traumatol Arthrosc. 12. Vol. 23. Predictive parameters for return to pre-injury level of sport 6 months following anterior cruciate ligament reconstruction surgery; pp. 3623–31. [DOI] [PubMed] [Google Scholar]
- Marx R. G., Stump T. J., Jones E. C., Wickiewicz T. L., Warren R. F. Am J Sports Med. 2. Vol. 29. Development and evaluation of an activity rating scale for disorders of the knee; pp. 213–8. [DOI] [PubMed] [Google Scholar]
- Ardern C. L., Taylor N. F., Feller J. A., Webster K. E. Am J Sports Med. 1. Vol. 40. Return-to-sport outcomes at 2 to 7 years after anterior cruciate ligament reconstruction surgery; pp. 41–8. [DOI] [PubMed] [Google Scholar]
- Ardern C. L., Osterberg A., Tagesson S., Gauffin H., Webster K. E., Kvist J. Br J Sports Med. 22. Vol. 48. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction; pp. 1613–9. [DOI] [PubMed] [Google Scholar]
- Webster K. E., Feller J. A. Am J Sports Med. 11. Vol. 44. Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction; pp. 2827–2832. [DOI] [PubMed] [Google Scholar]
- George S. Z., Zeppieri G. J Orthop Sports Phys Ther. 7. Vol. 39. Physical therapy utilization of graded exposure for patients with low back pain; pp. 496–505. [DOI] [PubMed] [Google Scholar]
- Woods M. P., Asmundson G. J. Pain. 3. Vol. 136. Evaluating the efficacy of graded in vivo exposure for the treatment of fear in patients with chronic back pain: a randomized controlled clinical trial; pp. 271–80. [DOI] [PubMed] [Google Scholar]
- Wertli M. M., Rasmussen-Barr E., Held U., Weiser S., Bachmann L. M., Brunner F. Spine J. 11. Vol. 14. Fear-avoidance beliefs-a moderator of treatment efficacy in patients with low back pain: a systematic review; pp. 2658–78. [DOI] [PubMed] [Google Scholar]
- Leeuw M., Goossens M. E., Linton S. J., Crombez G., Boersma K., Vlaeyen J. W. J Behav Med. 1. Vol. 30. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence; pp. 77–94. [DOI] [PubMed] [Google Scholar]
- Helminen E. E., Sinikallio S. H., Valjakka A. L., Vaisanen-Rouvali R. H., Arokoski J. P. BMC Musculoskelet Disord. Vol. 14. Effectiveness of a cognitive-behavioral group intervention for knee osteoarthritis pain: protocol of a randomized controlled trial; p. 46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Francis S. R., Andersen M. B., Maley P. J Sci Med Sport. 1. Vol. 3. Physiotherapists' and male professional athletes' views on psychological skills for rehabilitation; pp. 17–29. [DOI] [PubMed] [Google Scholar]
- O'Connor E HJ, Hammer P, Zimmerman I. Taylor J WG . Human Kinetics. Champaign, IL: Applying Sport Psychology: Four Perspectives; pp. 187–206. [Google Scholar]
- Vibe Fersum K., O'Sullivan P., Skouen J. S., Smith A., Kvale A. Eur J Pain. 6. Vol. 17. Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: a randomized controlled trial; pp. 916–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Della Villa S., Boldrini L., Ricci M., Danelon F., Snyder-Mackler L., Nanni G., Roi G. S. Sports Health. 1. Vol. 4. Clinical Outcomes and Return-to-Sports Participation of 50 Soccer Players After Anterior Cruciate Ligament Reconstruction Through a Sport-Specific Rehabilitation Protocol; pp. 17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macedo L. G., Smeets R. J., Maher C. G., Latimer J., McAuley J. H. Phys Ther. 6. Vol. 90. Graded activity and graded exposure for persistent nonspecific low back pain: a systematic review; pp. 860–79. [DOI] [PubMed] [Google Scholar]
- Gokeler A., Welling W., Zaffagnini S., Seil R., Padua D. Knee Surg Sports Traumatol Arthrosc. 1. Vol. 25. Development of a test battery to enhance safe return to sports after anterior cruciate ligament reconstruction; pp. 192–199. [DOI] [PMC free article] [PubMed] [Google Scholar]