

Abstract
Objective
To examine associations between suicidal ideation and sexual and physical abuse among active and recently retired elite athletics (track and field) athletes.
Methods
The study population consisted of all athletes (n=402) selected for a Swedish Athletics team between 2011 and 2017. Data on suicidal ideation, suicidal events (estimated through the 1 year non-sports injury prevalence), lifetime abuse experiences, sociodemographics, sense of coherence and coping strategies were collected using a cross-sectional survey. The data were analysed using binary logistic regression with suicidal ideation and non-sports injury as outcomes.
Results
192 athletes (47.8%) returned data. The prevalence of suicidal ideation was 15.6% (men 17.4%; women 14.2%) and the non-sports injury prevalence was 8.0% (men 11.6%; women 5.7%). Among women, suicidal ideation was associated with having been sexually abused (OR 5.94, 95% CI 1.42 to 24.90; p=0.015) and lower sense of coherence (OR 0.90, 95% CI 0.85 to 0.96; p=0.001) (Nagelkerke R2=0.33). Among men, suicidal ideation was only associated with use of behavioural disengagement for coping (OR 1.51, 95% CI 1.18 to 1.95; p=0.001) (R2=0.25). Among women, non-sports injury prevalence was associated with having been sexually abused (OR 8.61, 95% CI 1.34 to 55.1; p=0.023) and participating in an endurance event (OR 7.37, 95% CI 1.11 to 48.9; p=0.039 (R2=0.23), while among men, having immigrant parents (OR 5.67, 95% CI 1.31 to 24.5; p=0.020) (R2=0.11) was associated with injury outside sports.
Conclusions
About one out of six international athletics athletes reported having experienced suicidal ideation. World Athletics and National Olympic Committees need to include suicide prevention in their athlete protection programmes.
Keywords: sexual harassment, sport psychology, athletics, suicide
Introduction
‘Suicide, drugs, darkness’1 has been used to describe the aftermath of the sexual abuse scandal in the USA Gymnastics, where the physician Larry Nassar for at least 14 years abused hundreds of young female athletes.2 In addition to being at risk of sexual (and physical) abuse, athletes competing at the highest level also have to manage multiple other pressures affecting their mental health and these pressures can be aggravated by injury or failure to meet performance goals.3 4
This mental load can lead to suicide ideation (thinking about, considering or planning suicide) and even suicidal behaviour, for example, a suicide attempt (a non-fatal, self-inflicted destructive act with the explicit or inferred intent to die) (Box 1).5 6 The incidence of suicidal ideation and suicidal behaviour peaks among adolescents and young adults, with a global prevalence of lifetime suicidal ideation between 12% and 33% and lifetime suicidal behaviour between 4% and 9%.5 Suicidal events denote the worsening of suicide ideation into, for instance, a suicide attempt, an emergency referral for ideation or suicidal behaviour.5 Emergency room visits for injury are one example of events indicating increased suicide risk.7
Box 1. Definitions.
Suicidal ideation: thoughts about taking action to end one’s life, including identifying a method, having a plan or having intent to act.
Suicidal events: events suggesting the worsening of suicide ideation to suicidal behaviour, eg, emergency room visits or suicide attempts.
Suicide attempt: a potentially self-injurious behaviour associated with at least some intent to die.
Suicide: a fatal self-injurious act with some evidence of intent to die.
Globally, the overall suicide rate is estimated to 11/100 000 per year.5 For collegiate sports in the USA, the suicide rate of 1/100 000 per year8–10 represents about 7% of all-cause mortality among student athletes.9 Studies of suicidal ideation, suicidal events and suicide in non-collegiate elite athletes are scarce.10 The occupational category identified with the highest women’s suicide rates (16/100 000) in 2015 in the USA included professional athletes, while among men in this occupational category showed the largest increase (47%) in suicide rates from 2012.11 Participation in football, repeated concussions and chronic traumatic encephalopathy have been associated with increased risk of suicide among male elite athletes in the USA.10 12 There are few studies of suicidal ideation among elite athletes,13 but having been sexually and/or physically abused is a risk factor for suicidal ideation in the general population.14 We have previously reported correlates between having been sexually and physically abused and injury risk among female athletics (track and field) athletes.15
We aimed to explore the determinants of suicidal ideation and suicidal events among elite athletics athletes by investigating associations with lifetime abuse victimisation, aspects of sports participation and the athlete’s mental and behavioural resources. The motivational-volitional theory of suicidal behaviour16 was used for structuring the analysis. This theory conceptualises suicide as a behaviour that develops through a motivational phase that comprises development of suicidal ideation and intent, and a volitional phase that determines whether the ideation leads to suicidal events. We hypothesised that when individual athletes encounter situations of defeat and entrapment, the likelihood that suicidal ideation will emerge is increased when negative motivational elements are present. Physical and sexual abuse victimisation have been connected with negative effects long after the abuse has stopped in long-term studies outside of sport.17–19
Methods
The study used a cross-sectional design. Suicidal ideation was used as the primary outcome measure, while suicidal events were used as a secondary outcome measure (figure 1). Recording of suicidal events was limited to the 1-year period prevalence of emergency room-treated non-sports injuries. The explanatory variables were the athlete’s personal and sociodemographic characteristics, athletics participation, lifetime experience of sexual and/or physical abuse, sense of coherence and coping strategies. The data were collected in January 2018 using an anonymous web-questionnaire (BriteBack AB, Norrköping, Sweden). Two reminders were sent to non-responders during a 2-week period.
Figure 1.
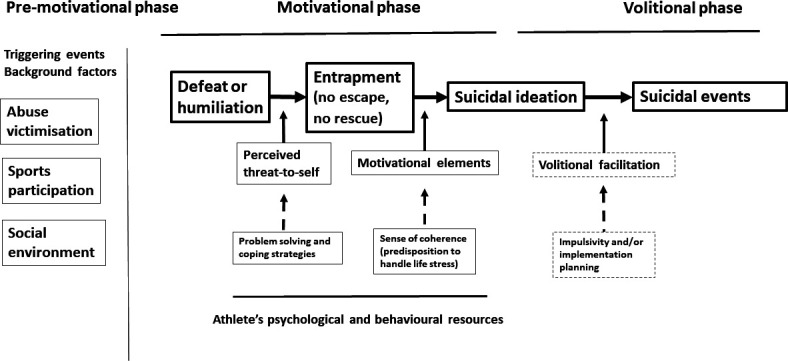
Conceptual model of suicidal ideation and risky behaviour developed from the motivational-volitional theory.16 The theory conceptualises suicide as a behaviour that develops through a motivational phase where suicidal ideation and intent develop, and a volitional phase that determines whether the ideation leads to suicidal events.
Participants
The study population consisted of all Swedish international athletics athletes who had participated in a national team between 2011 and 2017 in the event categories sprints (60–400 metres), hurdles, throws, jumps, middle-distance and long-distance running (800–42.125 metres), combined events and race walks. Athlete listing was obtained from Swedish Athletics for each event category.
Patient and public involvement
The study was supported by an advisory group consisting of athletes and coaches representing Swedish Athletics. This advisory group partnered with us for the design of the study and construction of the survey questions. At the end of the study, the advisory group commented on the findings and contributed to the dissemination plan.
Definitions and data collection
A web questionnaire based on the theoretical model was developed. Initial data collected in the questionnaire were regarding demographics and athletics background. Second, data on sexual orientation, lifetime sexual and physical abuse victimisation including perpetrators and suicidal ideation were gathered. The point in time of the abuse was specifically determined. Thereafter, data from two standardised scales, the Brief COPE and Sense of Coherence instruments were collected. The concept of sense of coherence (SOC) was put forward by Aaron Antonovsky to explain why some people become ill under stress and others stay healthy.20 The respondents were finally asked whether they had suffered a significant non-sports injury (cut, contusion, concussion, etc) during the past year (1 year injury prevalence) that required emergency room treatment.
Suicidal ideation was defined as lifetime thoughts about committing suicide. Suicidal events indicating progress to the volatile phase of suicidal behaviour16 were recorded using non-sports injury as proxy measure. A non-sports injury was defined as a physical injury sustained outside sports requiring treatment at an emergency medical facility.
Sexual abuse was defined as any sexual interaction involving physical contact with person(s) of any age that was perpetrated against the victim’s will, without consent or in an aggressive, exploitative, manipulative or threatening manner. Precisely, the variable used to collect data on sexual abuse was derived from the statement and questions originally developed by Mossige21 and used in earlier Swedish studies22 23: “Sometimes people are persuaded, pressed, or forced to do sexual activities they cannot protect themselves from. The following questions are about such situations. Have you been exposed to any of the following against your will?” (it is possible to choose several alternatives): (a) “Somebody exposed himself or herself indecently toward you, (b) Somebody has pawed (touched your body in an indecent way) you, (c) You masturbated somebody else, (d) You have had sexual intercourse, (e) You have had oral sex, and (f) You have had anal sex”.
Physical abuse was defined as being deliberately hurt by an adult person causing injuries such as bruises, broken bones, burns or cuts.24 The questionnaire asked whether it had happened that an adult had done any of the following to the athlete: “(a) Pushed, shoved or shook you up, (b) Thrown something at you, (c) Hurt you with her/his hands, (d) Kicked, bit or hit you with her/his fists, (e) Hurt you with a weapon, (f) Burned or scalded you, (g) Tried to smother you (took stranglehold) and (h) Physically attacked you otherwise”. Bullying was defined as being deliberately verbally or physically hurt as a child or adolescent by another child or adolescent. The survey asked whether it had happened that a child or adolescent had done any of the following to the athlete: “(a) repeated abused you verbally, (b) Pushed, shoved or shook you up, (c) Thrown something at you, (d) Hurt you with her/his hands, (e) Kicked, bit or hit you with her/his fists, (f) Hurt you with a weapon, (g) Burned or scalded you, (h) Tried to smother you (took stranglehold) and (i) Physically attacked you otherwise”.
The athlete’s mental and behavioural resources were measured by estimating their sense of coherence and personal coping strategies. The SOC-13 instrument was used to measure the athletes’ sense of coherence.25 A person’s sense of coherence is built on the components of comprehensibility, manageability and meaningfulness and is expected to reflect a person’s ability to handle stressful life situations.26 This instrument consists of 13 questions estimated on a 7-grade scale from 1 (very seldom or never) to 7 (very often). High scores indicate a high sense of coherence.
The Brief COPE instrument was used to measure the athletes’ coping strategies (ie, practices used to manage life challenges).27 28 The Brief COPE instrument cover two concepts, adaptive or maladaptive coping strategies. Adaptive strategies cover items for active coping, emotional support, instrumental support, positive reframing, planning, mood, acceptance and religion while maladaptive strategies are covered by the items self-distraction, denial, substance, behavioural disengagement, venting and self-blame. Each item is scored on a 4-point Likert scale from 1 (I have not been doing this at all) to 4 (I have been doing this a lot).
Data analysis
The SOC-13 data were compiled into a total summary score ranging from 13 to 91. The items included in the Brief COPE instrument, except self-blame, were analysed using Principal Component Analysis (PCA), where items were combined into four components (behavioural disengagement, exploiting support to take action, humour and positive reframing and turning to religion) that thereafter were investigated separately. The item self-blame was retained in its original form (table 1). To explore possible dependencies between the explanatory variables, correlations (Pearson’s r) between SOC-13 scores, Brief COPE component scores and age were investigated. T-tests were used to analyse differences in SOC-13 scores with regard to sex and between abuse victims and non-victims.
Table 1.
Principal Component Analysis of Brief COPE items
| Brief COPE items | Brief COPE components | ||||
| 1 r |
2 r |
3 r |
4 r |
Component categorisation | |
| 1. Active coping | 0.58 | 0.39 | 1 | ||
| 2. Planning | 0.60 | 0.32 | 0.42 | 1 | |
| 3. Positive reframing | 0.64 | 3 | |||
| 4. Acceptance | 0.43 | 0.50 | 3 | ||
| 5. Humour | 0.74 | 3 | |||
| 6. Religion | 0.84 | 4 | |||
| 7. Using emotional support | 0.87 | 1 | |||
| 8. Using instrumental support | 0.89 | 1 | |||
| 9. Self-distraction | 0.54 | 3 | |||
| 10. Denial | 0.56 | 2 | |||
| 11. Venting | 0.58 | 2 | |||
| 12. Substance use | 0.66 | 2 | |||
| 13. Behavioural disengagement | 0.76 | 2 | |||
Rotated component matrix (Pearson’s correlations r>0.30 are displayed) (n=192).
*Brief COPE components: component 1 (exploiting support to take action) includes items 1, 2, 7, 8; component 2 (behavioural disengagement) includes items 10, 11, 12, 13; component 3 (humour and positive reframing) includes items 3, 4, 5, 9; component 4 (turning to religion) includes items 6. Item 14 (Brief COPE) was not included in any component, but used separately, based on empirical groundings.
For the analyses of determinants of suicidal ideation and non-sports injury, the data collected for the variables characterising the athlete were recoded into binary format: lifetime sexual abuse victimisation involving physical contact (yes/no), lifetime physical abuse victimisation (yes/no), both parents (each of them) ≤12 years formal education (yes/no), at least one parent immigrant (yes/no), family perceived by athlete as financially disadvantaged (yes/no), age >13 years when commencing training athletics (yes/no), training load >20 hours/week (yes/no) and sports injury (yes/no). Athletics events were recoded into speed/power (sprints, hurdles, throws, jumps, combined events) and endurance events (middle-distance and long-distance running, race walking). We first performed analyses with simple models (logistic regression analyses with one explanatory variable) and thereafter analyses with multiple models (logistic regression analyses with several explanatory variables) using suicidal ideation (yes/no) and non-sports injury (yes/no) as outcomes. The explanatory variables were abuse types (sexual/physical/bullying), the Brief COPE components, SOC-13 and the binary athlete characteristic variables. The multiple models were fitted using backward elimination of non-significant variables (ie, variables with p≥0.05 were stepwise eliminated). Nagelkerke R2 was obtained for all multiple models to estimate their accountability levels.29 The Statistical Package for the Social Sciences for Windows V.25.0 was used for the analyses. All statistical tests were two-sided and outcomes with p<0.05 were considered to be statistically significant.
Results
Of 402 eligible athletes, 192 (47.8%) returned complete data sets. Twenty-eight per cent of the respondents had retired from participation in elite sport at the time of the study. The proportion of responders was similar among women (51.8%) and men (48.2%) and between active (45.5%) and retired (54.5%) athletes. The mean age of the respondents was 28.9 years (SD 6.7 years); males 29.1 years (SD 6.9 years) and females 28.8 years (SD 6.6 years) (table 2). Ninety-six per cent of the athletes reported their sexual orientation as heterosexual. A majority of athletes stated that during their childhood and adolescence they had been living in families with stable finances (82.8%) and at least one parent/custodian having had >12 years of formal education (75.0%).
Table 2.
Description of study sample (n=192)
| At-peak and postpeak athletes (January 2018) from the Swedish Athletics team 2011–17. | |||
| Male athletes (n=86) | Female athletes (n=106) | All athletes (n=192) | |
| Personal characteristics | |||
| Age, mean (SD) | 29.1 (6.9) | 28.8 (6.6) | 28.9 (6.7) |
| Sexual orientation—homosexual/bisexual, n (%) | 0 (0.0) | 7 (6.6) | 7 (3.6) |
| Childhood | |||
| Financially disadvantaged (athlete self-report), n (%) | 17 (19.8) | 16 (15.1) | 33 (17.2) |
| Parents <12 years formal education, n (%) | 20 (23.3) | 28 (26.4) | 48 (25.0) |
| Parents immigrants (at least one parent), n (%) | 12 (14.0) | 4 (3.8) | 16 (8.3) |
| Athletics | |||
| Commencing >12 years of age, n (%) | 28 (32.6) | 32 (30.2) | 60 (31.3) |
| Endurance athlete (middle-distance/long-distance running), n (%) | 35 (40.7) | 31 (29.2) | 66 (34.4) |
| Speed/power athlete (jump, throw, sprints, combined), n (%) | 51 (59.3) | 75 (70.8) | 126 (65.6) |
| At-peak athlete, n (%) | 71 (82.6) | 67 (63.2) | 138 (71.9) |
| Training load >14 hours/week, n (%) | 45 (52.3) | 41 (38.7) | 86 (44.8) |
| Athletics injury previous year, n (%) | 43 (50.0) | 45 (42.5) | 88 (45.8) |
| Suicidal ideation and non-sport injury | |||
| Lifetime suicidal ideation, n (%) | 15 (17.4) | 15 (14.2) | 30 (15.6) |
| Hospital-treated injury previous year, n (%) | 10 (11.6) | 6 (5.7) | 16 (8.3) |
| Abuse victimisation | |||
| Sexual abuse, n (%) | 4 (4.7) | 16 (15.1) | 20 (10.4) |
| Sexual abuse in athletics, n (%) | 1 (1.2) | 4 (3.8) | 5 (2.6) |
| Physical abuse, n (%) | 12 (14.0) | 9 (8.5) | 21 (10.9) |
| Bullying, n (%) | 54 (62.8) | 36 (34.0) | 90 (46.9) |
| Sense of coherence | |||
| SOC-13 (score 13–91), mean (SD) | 68.3 (11.1) | 65.8 (11.7) | 67.0 (11.5) |
| Coping strategies (Brief COPE) | |||
| Self-blame (score 0–6), mean score (SD) | 3.2 (1.5) | 3.4 (1.6) | 3.3 (1.6) |
| ‘Exploiting support to take action’* (score 0–24), mean score (SD) | 15.6 (4.5) | 16.5 (4.0) | 16.1 (4.3) |
| ‘Behavioural disengagement’† (score 0–24), mean score (SD) | 3.0 (2.5) | 3.9 (2.7) | 3.5 (2.7) |
| ‘Humour and positive reframing’‡ (score 0–24), mean score (SD) | 12.3 (3.8) | 12.4 (3.6) | 12.4 (3.7) |
| ‘Turning to religion’§ (score 0–6), mean score (SD) | 0.5 (1.3) | 0.5 (1.2) | 0.5 (1.2) |
*Includes items active coping, planning, using emotional support, using instrumental support.
†Includes items denial, venting, substance use, behavioural disengagement.
‡Includes items positive reframing, acceptance, humour, self-distraction.
§Includes item religion.
Lifetime suicidal ideation and non-sports injury prevalence
The prevalence of suicidal ideation among the participating athletes was 15.6% (men 17.4%; women 14.2%) (table 2). Eight per cent of the athletes (men 11.6%; women 5.7%) reported having sustained a non-sports related injury in the previous year that required emergency medical care.
Being subjected to sexual and physical abuse
Twenty (10.4%) of the participating athletes reported having sustained sexual abuse (table 2), 15.1% among women and 4.7% among men. Five athletes (2.6%) reported sexual abuse in the athletics setting. The perpetrators of sexual abuse in athletics were all male and were coaches, other adults and other athletes; 10.9% of participants had suffered physical abuse at some point in their life (14.0% of men, 8.5% of women). The perpetrators of physical abuse were predominantly parents/custodians; three athletes reported having been physically abused by a coach. All abuse episodes had occurred more than 1 year before the data collection.
Relationship among related determinants (eg, coping, abuse, etc)
The athletes’ sense of coherence did not differ by sex in unadjusted analyses (SOC-13 mean scores 65.8 for females and 68.3 for males; p=0.130), but there was a small correlation between the sense of coherence and age in both females (r=0.22; p=0.040) and males (r=0.23; p=0.020). Sense of coherence did not differ with regard to sexual abuse victimisation in female (SOC-13 mean scores 65.1 for victimised and 66.0 for non-victimised) or male athletes (SOC-13 mean scores 67.0 for victimised and 68.4 non-victimised). Regarding physical abuse victimisation, the sense of coherence was slightly lower among victimised than among non-victimised female athletes (SOC-13 mean scores 58.0 for non-victimised and 66.5 for victimised; p=0.036), but not among male athletes (SOC-13 mean scores 69.0 for victimised and 68.4 for non-victimised).
Among female athletes, the sense of coherence displayed a strong negative correlation (r=–0.52; p<0.001) with the Brief COPE component ‘behavioural disengagement’ and a moderate negative correlation (r=–0.36; p<0.001) with the item ‘self-blame’ (online supplementary table 1). No statistically significant correlations were observed with the remaining Brief COPE components. Among male athletes, only a moderate negative correlation (r=–0.44; p<0.001) between the sense of coherence and the Brief COPE component ‘behavioural disengagement’ was observed.
bjsports-2019-101386supp001.pdf (195.3KB, pdf)
Suicidal ideation models
The simple model analyses showed among female athletes that lifetime suicidal ideation was associated with sexual abuse victimisation (OR 4.85, 95% CI 1.45 to 16.3; p=0.011), lower sense of coherence (OR 0.90, 95% CI 0.85 to 0.96; p<0.001), a financially disadvantaged childhood (OR 5.40, 95% CI 1.59 to 18.4; p=0.007) or using self-blame (OR 1.84, 95% CI 1.19 to 2.82; p=0.006) and behavioural disengagement (OR 1.26, 95% CI 1.06 to 1.51; p=0.011) for coping (table 3). Among male respondents, athletes reporting suicidal ideation showed a lower sense of coherence (OR 0.92, 95% CI 0.87 to 0.97; p=0.004) or used behavioural disengagement as coping strategy (OR 1.51, CI 1.18 to 1.95; p=0.001).
Table 3.
Determinants associated with suicidal ideation among athletes (n=192) having participated in the Swedish Athletics team 2011–17 (ORs (95% CI) established by binary logistic regression analyses)
| Male athletes (n=86) | Female athletes (n=106) | All athletes (n=192) | ||||
| Simple models | Multiple model Nagelkerke R 2=0.25 |
Simple models | Multiple model Nagelkerke R 2=0.33 |
Simple models | Multiple model Nagelkerke R 2=0.25 |
|
| Personal characteristics | ||||||
| Financially disadvantaged childhood | n.s. | 5.40 (1.59 to 18.4) (p=0.007) | 2.46 (1.01 to 6.02) (p=0.048) | |||
| Parents immigrants | n.s. | n.s. | n.s. | |||
| Endurance athlete | n.s.* | n.s. | n.s. | |||
| At-peak athlete | n.s. | n.s. | n.s. | |||
| Training load | n.s. | n.s. | n.s. | |||
| Abuse victimisation | ||||||
| Sexual abuse | n.s. | 4.85 (1.45 to 16.3) (p=0.011) | 5.94 (1.42 to 24.9) (p=0.015) | 3.22 (1.17 to 8.82) (p=0.023) | ||
| Physical abuse | n.s. | n.s. | n.s.† | |||
| Bullying | n.s. | n.s.‡ | 2.63 (1.16 to 5.97) (p=0.021) | |||
| Athletics | ||||||
| Athletics injury previous year | n.s. | n.s. | n.s§ | |||
| Sense of coherence | ||||||
| SOC-13 | 0.92 (0.87 to 0.97) (p=0.004) | 0.90 (0.85 to 0.96) (p<0.001) | 0.90 (0.85 to 0.96) (p=0.001) | 0.91 (0.88 to 0.95) (p<0.001) | 0.92 (0.88 to 0.96) (p<0.001) | |
| Coping strategies (Brief COPE) | ||||||
| Self-blame | n.s.¶ | 1.84 (1.19 to 2.82) (p=0.006) | 1.60 (1.21 to 2.11) (p=0.001) | 1.40 (1.05 to 1.87) (p=0.023) | ||
| ‘Exploiting support to take action’ | n.s. | n.s. | n.s. | |||
| ‘Behavioural disengagement’ | 1.51 (1.18 to 1.95) (p=0.001) | 1.51 (1.18 to 1.95) (p=0.001) | 1.26 (1.06 to 1.51) (p=0.011) | 1.33 (1.16 to 1.52) (p<0.001) | ||
| ‘Humour and positive reframing’ | n.s. | n.s. | n.s. | |||
| ‘Turning to religion’ | n.s. | n.s. | n.s. | |||
*(0.30 (0.08 to 1.17) (p=0.084).
†(2.45 (0.87 to 6.93) (p=0.091).
‡(2.57 (0.85 to 7.79) (p=0.095).
§(1.97 (0.89 to 4.36) (p=0.094).
¶(1.46 (1.00 to 2.13) (p=0.051).
n.s, not significant at 5% level.
In the multiple model for female athletes, suicidal ideation was associated only with sexual abuse victimisation (OR 5.94, 95% CI 1.42 to 24.9; p=0.015) and a lower sense of coherence (OR 0.90, 95% CI 0.85 to 0.96; p=0.001) (Nagelkerke R2=0.33), while suicidal ideation among male athletes was only associated with the use of behavioural disengagement for coping (OR 1.51, 95% CI 1.18 to 1.95; p=0.001) (Nagelkerke R2=0.25).
Suicidal event models
With regard to the secondary outcome measure the simple model analyses showed that among female athletes, the 1-year non-sports injury prevalence was associated only with sexual abuse victimisation (OR 6.14, 95% CI 1.13 to 33.5; p=0.036), while among male athletes, the 1-year non-sports injury prevalence was associated only with having immigrant parents (OR 5.67, 95% CI 1.31 to 24.5; p=0.020) (table 4).
Table 4.
Determinants associated with having suffered a non-sports injury previous year among athletes (n=192) having participated in the Swedish Athletics team 2011–17 (ORs (95% CI) established by binary logistic regression analysis)
| Male athletes (n=86) | Female athletes (n=106) | All athletes (n=192) | ||||
| Simple models | Multiple model Nagelkerke R 2=0.11 |
Simple models | Multiple model Nagelkerke R 2=0.23 |
Simple models | Multiple model Nagelkerke R 2=0.05 |
|
| Personal characteristics | ||||||
| Financially disadvantaged childhood | n.s. | n.s. | n.s. | |||
| Parents immigrants | 5.67 (1.31 to 24.5) (p=0.020) | 5.67 (1.31 to 24.5) (p=0.020) | NA | NA | 4.56 (1.27 to 16.3) (p=0.020) | 4.56 (1.27 to 16.3) (p=0.020) |
| Endurance athlete | n.s. | n.s.* | 7.37 (1.11 to 48.9) (p=0.039) | n.s. | ||
| At-peak athlete | n.s. | n.s. | n.s. | |||
| Training load | n.s. | n.s. | n.s. | |||
| Abuse victimisation | ||||||
| Sexual abuse | NA | NA | 6.14 (1.13 to 33.5) (p=0.036) | 8.61 (1.34 to 55.1) (p=0.023) | n.s. | |
| Physical abuse | n.s. | n.s. | n.s.† | |||
| Bullying | n.s.‡ | n.s. | n.s.§ | |||
| Sense of coherence | ||||||
| SOC-13 | n.s. | n.s. | n.s. | |||
| Coping strategies (Brief COPE) | ||||||
| Self-blame | n.s. | n.s. | n.s. | |||
| ‘Exploiting support to take action’ | n.s. | n.s. | n.s. | |||
| ‘Behavioural disengagement’ | n.s. | n.s. | n.s. | |||
| ‘Humour and positive reframing’ | n.s. | n.s. | ||||
| ‘Turning to religion’ | n.s. | n.s. | n.s. | |||
*(5.41 (0.94 to 31.2) (p=0.059).
†(3.12 (0.91 to 10.7) (p=0.072).
‡(2.70 (0.90 to 8.10) (p=0.076).
§(6.20 (0.75 to 51.5) (p=0.091).
NA, not available; n.s, not significant at 5% level.
Among female athletes, the 1-year non-sports injury prevalence was associated with sexual abuse victimisation (OR 8.61, 95% CI 1.34 to 55.1; p=0.023) and having competed in an endurance event (OR 7.37, 95% CI 1.11 to 48.9; p=0.039) (Nagelkerke R2=0.23). The multiple model for male athletes was represented by a simple model, since only having immigrant parents (OR 5.67, 95% CI 1.31 to 24.5; p=0.020) was included (Nagelkerke R2=0.11).
Discussion
We report a 15.6% lifetime prevalence of suicidal ideation among Swedish athletics athletes competing at the international level. This compares with a 13.9% lifetime prevalence reported from Army servicemen,30 but is lower than the 32.7% lifetime prevalence recently observed among college students.31 Sports-related factors such as sports injuries and retirement from elite level competitions did not correlate with suicidal ideation.
Determinants of suicidal ideation and suicidal events
Among female participants, having been sexual abused and perceiving daily life as less comprehensible, manageable and meaningful were the strongest determinants of both suicidal ideation and suicidal events. Among male participants, the main determinant for suicidal ideation was using an avoidant strategy for coping with life challenges, and for suicidal events, having immigrant parents. However, the accountability level for the latter model among male athletes was low (Nagelkerke R2=0.11). The single aspect of sport participation found to be relevant was an increased likelihood of suicidal events in female athletes participating in an endurance event. These findings correspond with present aetiological theories of suicide, which typically suggest that negative consequences of pre-existing vulnerability factors are pronounced when challenged by stress.16 32 33
Sexual abuse history
A history of sexual abuse was thus a central determinant of suicidal ideation and suicidal events among the female athletes. The prevalence (15.1%) corresponds to previous reports from research among competitive athletes.15 34 Several large studies in the general population have documented associations between sexual abuse and the subsequent experience of suicidal ideation and suicidal events.35 36 However, these associations have also been found to diminish with age.36 In this study, we observed a correlation between the psychological resource sense of coherence and increasing age, and an inverse correlation between sense of coherence and avoidant coping strategies. These findings indicate that although there exists intrusive and distressing traumatic memories from previous sexual abuse, the athlete’s capacity to manage this experience may improve with increasing age. This finding also implies that negative consequences of abuse may even be more prevalent in younger elite athletes than in the sample of experienced elite athletes (mean age 28.9 years) in this study.
Use of avoidant coping strategies
Among the male athletes in this study, the only determinant for suicidal ideation was the use of an avoidant coping strategy, that is, behavioural disengagement involving denial, venting and substance use. Sexual abuse was not a risk factor among males, possibly due to the relatively low life-time prevalence (4.7%) compared with females (15.1%). Coping with life challenges may be achieved by directly solving the problem or avoiding the concern without reaching a solution.37 According to the notions of affect regulation,16 38 the use of avoidant or maladaptive coping strategies to handle stressful life situations increases the probability of experiencing feelings of entrapment (no escape, no rescue) and, subsequently, of suicidal ideation. The fact that individuals who contemplate suicide have difficulties with problem solving and coping is not surprising, and studies in non-sports settings have consistently shown a link between suicidal behaviour and deficits in these abilities.39 40
Implications for suicide prevention
We found that about one out of six elite athletes had experiences of suicidal ideation. Conversion to suicide attempts was not included in the present study, but a meta-analysis of studies among college students estimated that about one-half (53.4%) of lifetime ideators transition to a suicide plan and 22.1% of lifetime planners transition to an attempt, while attempts among lifetime ideators without plan are less frequent (3.1%).31 No suicides among Swedish elite athletics athletes were publicly reported during the time period for the study (2011–17), but such events were reported from other sports, for example, ice hockey.41 Internationally, several suicides among athletes competing at the highest level have been reported during recent years, for example, from figure skating in association with sexual abuse accusations.42 Practical implications of our results are that suicide prevention strategies43 among female athletics athletes should include targeting sexual abuse victimisation and strengthening the athletes’ personal psychological resources, while among male athletes the corresponding interventions should comprise coping strategies and problem solving skills. Female athletes with a sexual abuse history should be provided an opportunity to discuss what they have experienced, and individual care plans should be developed.44 At the societal level, efforts should be made to detect sexual abuse early and sports federations should formulate action plans for suicide prevention. In parallel, sports clinicians must increase their general attention on improving the mental health of athletes.45
Study strengths and weaknesses
This is the first study to address the topic of suicidal ideation in sport with a specific paucity of research on correlates to suicidal ideation and suicidal events in elite athletes. It was designed as a cross-sectional analysis using best-practice procedures adjusted for the research topic. All multiple models of determinants displayed satisfactory accountability levels (Nagelkerke R2 >0.20), except for non-sports injury among males. An important limitation of the study is that >90% of the participating athletes were living with a Swedish lifestyle, social background and benefiting from national education and health systems. The results obtained cannot therefore be immediately generalised to the international population of elite athletics athletes. Also, use of hospital-treated non-sports injuries as proxy for suicidal events has limitations, due to the fact that not all hospital-treated injuries are associated with suicidal events, that is, no-fault car accidents. Moreover, the population was relatively small (n=404) and the participation was 49%. Even though no difference in participation was observed with regard to sex or current international-level competition status, the possibility of bias cannot be ruled out. Finally, not all relevant determinants of suicidal ideation were included in the study, for example, previous episodes of clinically treated psychiatric disorders and the athlete’s ethnicity were not assessed.
Conclusion
Among elite athletics athletes, sexual abuse victimisation combined with a low sense of coherence were the main determinants of suicidal ideation and suicidal events among female athletes, while among male athletes, suicidal ideation was primarily associated with avoidant strategies for coping with stressful life events. Sports injury history and retirement from international competitions were not identified as determinants. In other words, mental harm resulting from abuse and the athletes’ psychological resources and behavioural traits, respectively, appeared to be the leading influences on susceptibility for suicidal thoughts and actions. Given that about one out of six athletes had experienced suicidal ideation, these results should be used to plan how to prevent suicidal ideation, suicide attempts and suicide for top-level athletes in the sport of athletics.
What are the findings?
The prevalence of suicidal ideation among elite athletics athletes appears similar to that in general populations of young adults.
Having been victims of sexual abuse combined with having decreased psychological resources to deal with life stress (low sense of coherence) predicted suicidal ideation in female elite athletics athletes.
Among male elite athletes, suicidal ideation was associated with use of avoidant strategies for coping with challenging life events, for example, substance use and denial.
How might it impact on clinical practice in the future?
Sport medicine clinicians should be aware of determinants for suicidal ideation among athletes—women who have a history of having been sexually abused and who have signs of psychological vulnerability and men who display avoidant coping behaviours.
Footnotes
Twitter: @Jenny_Jacobsson, @margo.mountjoy
Contributors: TT was the lead investigator. TT, OD and CGS conceived the study. All authors were involved in the study design and reviewed the draft of the report. TT, OD and AS coordinated the data management, and TT drafted the report. AS carried out the statistical analysis, reviewed by OD and JK. All authors approved the final version of the report. TT is the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the 'Methods' section for further details.
Patient consent for publication: Not required.
Ethics approval: Ethical approval for the study was obtained from the Research Ethics Board in Linköping, Sweden (Dnr 2017/601-32).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: No data are available.
References
- 1. New York Post Suicide, drugs, ‘darkness’: Perv doctor’s gymnastics victims out in force. Available: https://nypost.com/2018/01/16/suicide-drugs-darkness-perv-doctors-gymnastics-victims-out-in-force/
- 2. New York Times Larry Nassar Sentencing: ‘I Just Signed Your Death Warrant'. Available: https://www.nytimes.com/2018/01/24/sports/larry-nassar-sentencing.html
- 3. Hammond T, Gialloreto C, Kubas H, et al. The prevalence of failure-based depression among elite athletes. Clin J Sport Med 2013;23:273–7. 10.1097/JSM.0b013e318287b870 [DOI] [PubMed] [Google Scholar]
- 4. Junge A, Feddermann-Demont N. Prevalence of depression and anxiety in top-level male and female football players. BMJ Open Sport Exerc Med 2016;2:e000087 10.1136/bmjsem-2015-000087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet 2016;387:1227–39. 10.1016/S0140-6736(15)00234-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Klonsky ED, Saffer BY, Bryan CJ. Ideation-to-action theories of suicide: a conceptual and empirical update. Curr Opin Psychol 2018;22:38–43. 10.1016/j.copsyc.2017.07.020 [DOI] [PubMed] [Google Scholar]
- 7. Rhodes AE, Sinyor M, Boyle MH, et al. Emergency department presentations and youth suicide: a case-control study. Can J Psychiatry 2019;64:88–97. 10.1177/0706743718802799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Maron BJ, Haas TS, Murphy CJ, et al. Incidence and causes of sudden death in U.S. college athletes. J Am Coll Cardiol 2014;63:1636–43. 10.1016/j.jacc.2014.01.041 [DOI] [PubMed] [Google Scholar]
- 9. Rao AL, Asif IM, Drezner JA, et al. Suicide in national collegiate athletic association (NCAA) athletes: a 9-year analysis of the NCAA resolutions database. Sports Health 2015;7:452–7. 10.1177/1941738115587675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rao AL Athletic Suicide - Separating fact from fiction and navigating the challenging road ahead. Curr Sports Med Rep 2018;17:83–4. 10.1249/JSR.0000000000000462 [DOI] [PubMed] [Google Scholar]
- 11. Peterson C, Stone DM, Marsh SM, et al. Suicide rates by major occupational group - 17 States, 2012 and 2015. MMWR Morb Mortal Wkly Rep 2018;67:1253–60. 10.15585/mmwr.mm6745a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gardner A, Iverson GL, McCrory P. Chronic traumatic encephalopathy in sport: a systematic review. Br J Sports Med 2014;48:84–90. 10.1136/bjsports-2013-092646 [DOI] [PubMed] [Google Scholar]
- 13. Reardon CL, Hainline B, Aron CM, et al. Mental health in elite athletes: international Olympic Committee consensus statement (2019). Br J Sports Med 2019;53:667–99. 10.1136/bjsports-2019-100715 [DOI] [PubMed] [Google Scholar]
- 14. Thompson MP, Kingree JB, Lamis D. Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child Care Health Dev 2019;45:121–8. 10.1111/cch.12617 [DOI] [PubMed] [Google Scholar]
- 15. Timpka T, Janson S, Jacobsson J, et al. Lifetime history of sexual and physical abuse among competitive athletics (track and field) athletes: cross sectional study of associations with sports and non-sports injury. Br J Sports Med 2019;53:1412–7. 10.1136/bjsports-2018-099335 [DOI] [PubMed] [Google Scholar]
- 16. O'Connor RC, Nock MK. The psychology of suicidal behaviour. Lancet Psychiatry 2014;1:73–85. 10.1016/S2215-0366(14)70222-6 [DOI] [PubMed] [Google Scholar]
- 17. Monnat SM, Chandler RF. Long term physical health consequences of adverse childhood experiences. Sociol Q 2015;56:723–52. 10.1111/tsq.12107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Coles J, Lee A, Taft A, et al. Childhood sexual abuse and its association with adult physical and mental health: results from a national cohort of young Australian women. J Interpers Violence 2015;30:1929–44. 10.1177/0886260514555270 [DOI] [PubMed] [Google Scholar]
- 19. Buckingham ET, Daniolos P. Longitudinal outcomes for victims of child abuse. Curr Psychiatry Rep 2013;15:342 10.1007/s11920-012-0342-3 [DOI] [PubMed] [Google Scholar]
- 20. Antonovsky A, Sagy S. Aaron Antonovsky, the scholar and the man behind salutogenesis : Mittelmark MB, Sagy S, Eriksson M, The Handbook of Salutogenesis [Internet]. Cham (CH): Springer, 2017. http://www.ncbi.nlm.nih.gov/books/NBK435855/ [PubMed] [Google Scholar]
- 21. Mossige S Ungdoms holdninger til seksuelle krenkelser og overgrep [Young persons’ attitudes towards sexual violations and abuse] Report 16/01. Oslo: Norwegian Social Research (NOV A), 2001. [Google Scholar]
- 22. Priebe G, Svedin CG. Prevalence, characteristics, and associations of sexual abuse with sociodemographics and consensual sex in a population-based sample of Swedish adolescents. J Child Sex Abus 2009;18:19–39. 10.1080/10538710802584635 [DOI] [PubMed] [Google Scholar]
- 23. Svedin CG, Priebe G, Wadsby M, et al. Ungas sex och Internet – i en föränderlig värld. [Youth sexuality and the Internet – in a changing world.]. Rapport. Linköping: Linköpings Universitet, 2015. [Google Scholar]
- 24. Jernbro C, Janson S. Violence against children 2016 – a national Swedish study. Stockholm: Allmänna Barnhuset, 2018. [Google Scholar]
- 25. Antonovsky A The structure and properties of the sense of coherence scale. Soc Sci Med 1993;36:725–33. 10.1016/0277-9536(93)90033-Z [DOI] [PubMed] [Google Scholar]
- 26. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and the relation with health: a systematic review. J Epidemiol Community Health 2006;60:376–81. 10.1136/jech.2005.041616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Carver CS You want to measure coping but your protocol's too long: consider the brief cope. Int J Behav Med 1997;4:92–100. 10.1207/s15327558ijbm0401_6 [DOI] [PubMed] [Google Scholar]
- 28. Kristiansen E, Roberts GC, Abrahamsen FE. Achievement involvement and stress coping in elite wrestling. Scand J Med Sci Sports 2008;18:526–38. 10.1111/j.1600-0838.2007.00646.x [DOI] [PubMed] [Google Scholar]
- 29. Nagelkerke NJD A note on a general definition of the coefficient of determination. Biometrika 1991;78:691–2. 10.1093/biomet/78.3.691 [DOI] [Google Scholar]
- 30. Nock MK, Stein MB, Heeringa SG, et al. Prevalence and correlates of suicidal behavior among soldiers: results from the army study to assess risk and resilience in Servicemembers (army STARRS). JAMA Psychiatry 2014;71:514–22. 10.1001/jamapsychiatry.2014.30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Mortier P, Auerbach RP, Alonso J, et al. Suicidal thoughts and behaviors among first-year college students: results from the WMH-ICS project. J Am Acad Child Adolesc Psychiatry 2018;57:263–73. 10.1016/j.jaac.2018.01.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Schotte DE, Clum GA. Problem-Solving skills in suicidal psychiatric patients. J Consult Clin Psychol 1987;55:49–54. 10.1037/0022-006X.55.1.49 [DOI] [PubMed] [Google Scholar]
- 33. Mann JJ, Waternaux C, Haas GL, et al. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry 1999;156:181–9. 10.1176/ajp.156.2.181 [DOI] [PubMed] [Google Scholar]
- 34. Mountjoy M, Brackenridge C, Arrington M, et al. International Olympic Committee consensus statement: harassment and abuse (non-accidental violence) in sport. Br J Sports Med 2016;50:1019–29. 10.1136/bjsports-2016-096121 [DOI] [PubMed] [Google Scholar]
- 35. Dube SR, Anda RF, Felitti VJ, et al. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the adverse childhood experiences study. JAMA 2001;286:3089–96. 10.1001/jama.286.24.3089 [DOI] [PubMed] [Google Scholar]
- 36. Bruffaerts R, Demyttenaere K, Borges G, et al. Childhood adversities as risk factors for onset and persistence of suicidal behaviour. Br J Psychiatry 2010;197:20–7. 10.1192/bjp.bp.109.074716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Frydenberg E, Lewis R, Kennedy G, et al. Coping with concerns: an exploratory comparison of Australian, Colombian, German, and Palestinian adolescents. J Youth Adolesc 2003;32:59–66. 10.1023/A:1021084524139 [DOI] [Google Scholar]
- 38. Klonsky ED The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev 2007;27:226–39. 10.1016/j.cpr.2006.08.002 [DOI] [PubMed] [Google Scholar]
- 39. Pollock LR, Williams JMG. Problem-Solving in suicide attempters. Psychol Med 2004;34:163–7. 10.1017/S0033291703008092 [DOI] [PubMed] [Google Scholar]
- 40. Guerreiro DF, Cruz D, Frasquilho D, et al. Association between deliberate self-harm and coping in adolescents: a critical review of the last 10 years' literature. Arch Suicide Res 2013;17:91–105. 10.1080/13811118.2013.776439 [DOI] [PubMed] [Google Scholar]
- 41. Aftonbladet Tror inte att speltiden i Surahammar var avgörande. [We do not believe that ice time was the decisive factor.]. Available: https://www.aftonbladet.se/sportbladet/a/m62344/tror-inte-att-speltiden-i-surahammar-var-avgorande
- 42. ESPN Nothing about it is easy': Skater's suicide leaves more questions than answers. Available: https://www.espn.com/olympics/story/_/id/25870759/john-coughlin-suicide-leaves-more-questions-answers-figure-skating-community
- 43. Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016;3:646–59. 10.1016/S2215-0366(16)30030-X [DOI] [PubMed] [Google Scholar]
- 44. Ades V, Goddard B, Pearson Ayala S, et al. Caring for long term health needs in women with a history of sexual trauma. BMJ 2019;367:l5825 10.1136/bmj.l5825 [DOI] [PubMed] [Google Scholar]
- 45. Mann BJ, Grana WA, Indelicato PA, et al. A survey of sports medicine physicians regarding psychological issues in patient-athletes. Am J Sports Med 2007;35:2140–7. 10.1177/0363546507304140 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bjsports-2019-101386supp001.pdf (195.3KB, pdf)