

Abstract
Background:
Exposure to child maltreatment is a well-known risk factor for suicide ideation among adolescents. Recent stressful life events may also contribute to this risk. However, the association between these risk factors is unclear in the etiology of suicide ideation for adolescents from socioeconomically disadvantaged backgrounds.
Objective:
The present study tested the stress generation and stress sensitivity hypotheses in relation to child maltreatment, recent stressful life events (in the past year), and suicide ideation (in the past two weeks).
Participants and Setting:
We utilized a sample of diverse, socioeconomically disadvantaged, depressed adolescent girls (N = 175) who were part of a depression treatment intervention.
Results:
Child maltreatment was significantly associated with adolescent suicide ideation, β = .40, p < .001. Results supported the stress sensitivity hypothesis, in that exposure to interpersonal stressors in the past year exacerbated the association between child maltreatment and adolescents’ suicide ideation, β = .18, p < .05. We found evidence for a protective factor, cognitive reappraisal, in the association between stressful life events and suicide ideation, β = −.15, p < .05.
Conclusions:
These findings have several implications for clinical practice and suicide prevention with adolescent girls, and contribute to the extant literature on the role of chronic and acute stress in the etiology of adolescent suicide ideation.
Keywords: Child maltreatment, Suicidal ideation, Adolescence, Depression, Stressful life events
Suicide is currently the second cause of death for youth in the United States, and suicide rates are rising (Curtin & Heron, 2019). In the period from 2007 to 2017, the suicide rate for young people aged 15–29 increased by 76 % (Curtin & Heron, 2019). Rates of suicide ideation (SI), a leading risk factor for suicide, have similarly increased among adolescents, with 17.2 % of adolescents reporting SI and 13.6 % reporting having made a suicide plan in the past year (Kann et al., 2018). These rates are higher for adolescent1 girls, with 22.1 % reporting SI and 17.1 % reporting having made a suicide plan in the past year (Kann et al., 2018). Furthermore, racial and ethnic minority adolescents, and adolescents from low socioeconomic backgrounds, are at an increased risk for suicidal thoughts and behaviors (Dupéré et al., 2009; Lindsey et al., 2019). Adolescence is a period of heightened risk for psychopathology such as depression, and adolescent girls are particularly susceptible to mood disorders with twice as many reporting feelings of sadness or hopelessness compared to their male counterparts (Kann et al., 2018; Kessler et al., 2005). Prior research shows that adolescent girls are vulnerable to mood disorders such as depression due to biological, psychological, and environmental factors that coincide during this developmental period (e.g., sex-specific hormone changes and exposure to social stressors; Naninck et al., 2011). Consequently, there is a need for research that identifies key risk factors for suicidal thoughts and behaviors among diverse, socioeconomically disadvantaged adolescent girls, to inform theoretical models of adolescent suicide and contribute to effective suicide prevention strategies.
Exposure to child maltreatment is a potent risk factor for suicidal thoughts and behaviors among adolescents (Miller et al., 2013). According to the developmental psychopathology perspective, child maltreatment is a toxic rearing environment that can alter adolescent’s typical socioemotional development, and these developmental disruptions often cascade into psychopathology such as suicidal thoughts and behaviors (Cicchetti, 2016; Handley et al., 2018). Indeed, in a population based sample, adolescents who reported exposure to physical abuse and sexual abuse were 5.06 and 3.56 times more likely to exhibit SI, respectively (Gomez et al., 2017). With the direct association between child maltreatment and suicide risk clearly established, recent work has examined mechanisms or moderators in this association. For example, there is evidence that interpersonal processes and psychopathology underlie the developmental association between child maltreatment and adolescent SI (Handley et al., 2018; Kwok & Gu, 2019). It is also likely, but has not been empirically established, that recent stressful life events play a role in the association between child maltreatment and adolescent girls’ SI.
Stressful life events, such as the death of a loved one or romantic relationship problems, can lead to the onset of suicidal thoughts and behaviors (Liu & Miller, 2014). Acute life stressors may be particularly harmful for the mental health of adolescents due to the ongoing developmental changes during this time, including the growth and maturation of brain areas involved with emotions and the stress response (Andersen & Teicher, 2008). Indeed, the occurrence of stressful life events is a recognized risk factor in the literature on adolescent suicidal thoughts and behavior (e.g., Fergusson et al., 2000). Consistent with the interpersonal theory of suicide (Van Orden et al., 2010), stressful life events that are interpersonal in nature may be a particularly salient risk factor for suicidal thoughts among adolescents (Joiner & Rudd, 1995). Several studies have found that interpersonal life stressors have a stronger association with suicidal thoughts as compared to non-interpersonal stressors, such as achievement-related events (Joiner & Rudd, 1995; MacKin et al., 2017). There is also evidence that adolescent girls are more susceptible to the negative impacts of relational stress (Rudolph, 2002). However, it remains unclear how child maltreatment is associated with interpersonal stressful life events in the etiology of adolescent girls’ SI.
There are two competing hypotheses regarding the role of chronic childhood stress and stressful life events in the development of psychopathology (see Fig. 1). The stress sensitivity hypothesis suggests that exposure to early life adversity increases ones’ vulnerability to the harmful effects of stress experienced later in life (Hammen et al., 2000). For example, Hammen et al. (2000) found that adolescent girls who experienced recent stressful life events were more likely to exhibit an onset or exacerbation of depression if they had also experienced adversity in their childhood. To our knowledge, only one study has tested the role of child maltreatment and stress in predicting SI among adolescent girls, with results showing that chronic strain in peer, academic, and family domains was predictive of suicidal behaviors only for girls who had prior experience of physical and sexual abuse (Miller et al., 2017). However, the stress sensitivity hypothesis has not been tested in a model that operationalizes acute stress with independent stressful life events, nor within a low-socioeconomic status (SES) and diverse sample of adolescents.
Fig. 1.
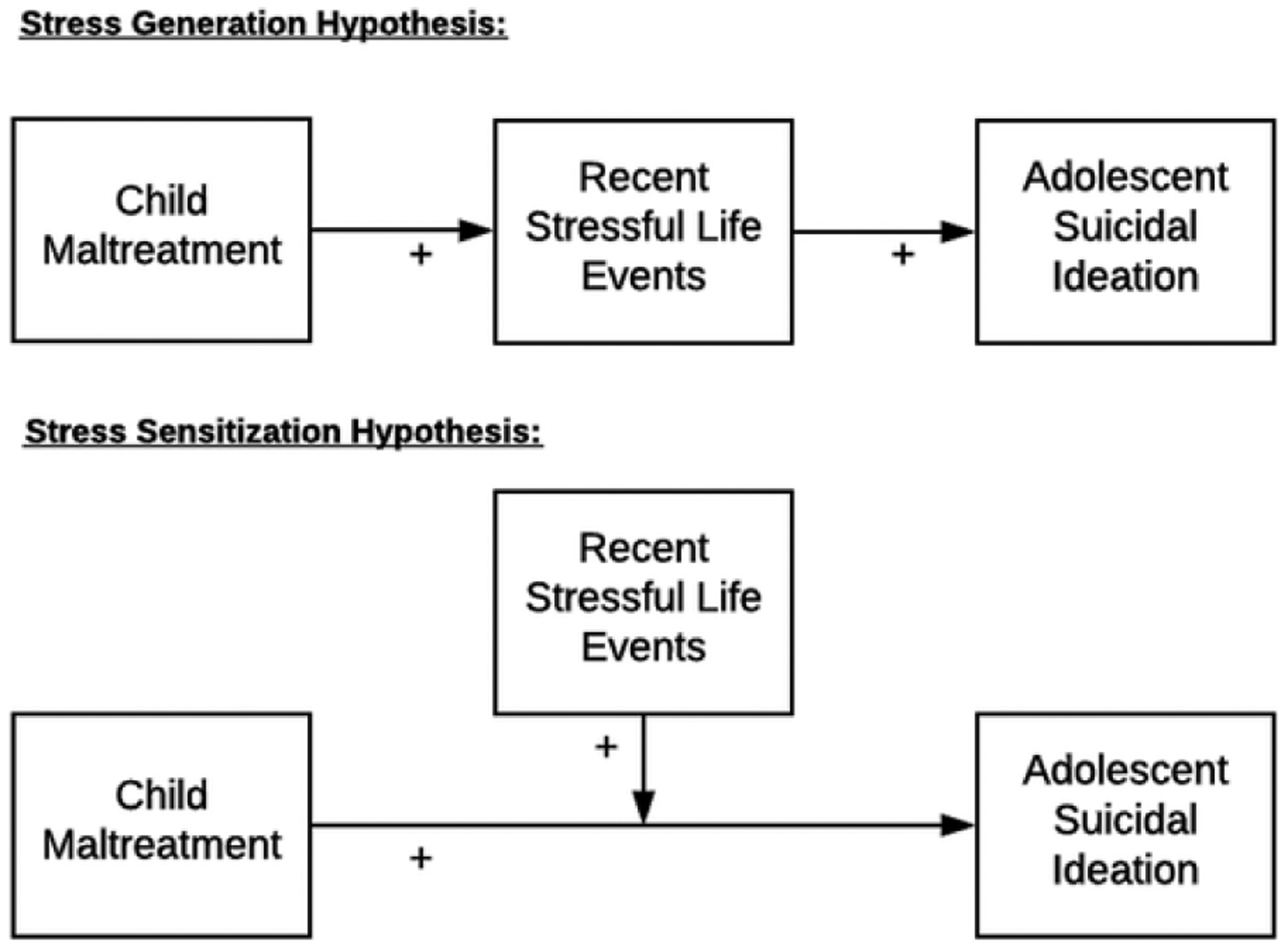
Depiction of the stress-generation and stress-sensitization hypotheses as applied to the association between child maltreatment and adolescent suicidal ideation.
There is also a lack of empirical work testing stressful life events as a mechanism, or mediator, in the pathway from child maltreatment to adolescent SI. Theoretically, the stress generation hypothesis is a competing hypothesis suggesting that stressors early in life prompt additional stressors later in life. Hence, recent stressful life events are hypothesized to mediate the association between childhood adversity and later psychopathology (Hankin, 2005). In support of this hypothesis, Hankin (2005) found that recent negative life events completely mediated the association between child maltreatment (specifically, emotional maltreatment) and psychopathology in a sample of young adults. There is also evidence garnered from a large longitudinal sample in New Zealand that adverse life events in adolescence mediated the association between childhood stressors and young adult suicidal behaviors (Fergusson et al., 2000). Thus, there is evidence for both stress-generation and stress-sensitization theories regarding the association between child maltreatment, stressful life events, and adolescent SI.
Testing these competing hypotheses regarding the roles of child maltreatment and stressful life events in the etiology of SI for adolescent girls will contribute to the current theoretical landscape in the suicide literature. For instance, the Integrated Motivational-Volitional (IMV) model of suicidal behavior posits that stressors, including both childhood stressors such as maltreatment and more recent stressful life events, are background factors that contribute to the emergence of suicidal thoughts and behaviors. However, the relation between different types of chronic and acute stressors has not been clarified within this nor other modern theories of suicide. These suicide models may be able to draw from the developmental literature, which posits unique relations between different types of stressors in the etiology of adolescent risk behaviors and maladaptive outcomes.
1. Study aims & hypotheses
The present study utilized baseline data from a diverse and socioeconomically disadvantaged sample of depressed adolescent girls who participated in a randomized control trial of a depression treatment (N = 175). We utilized a sample of depressed adolescents because depressive disorders are a major risk factor for suicidal thoughts, and by utilizing a sample of girls with depression, we were able to avoid statistical confounding between child maltreatment, depression, and suicidal ideation. The primary aim of the current study was to test the competing stress generation and stress sensitivity hypotheses in relation to child maltreatment, recent stressful life events (in the past year), and SI (in the past two weeks). We chose to assess SI in the past two weeks to reduce the possibility of SI being a causal factor for stressful life events in the past year.
This study fills the gap in the literature on the etiology of SI among adolescent girls in several ways. First, we sought to clarify the theoretical association between chronic stress (i.e., child maltreatment) and acute stress (i.e., past year independent stressful life events) in the etiology of adolescent SI. Second, we were particularly interested in the role of independent, interpersonal stressful life events as they relate to prior experience of child maltreatment and the consequent SI during adolescence. Independent stressful life events are those not precipitated by an individual’s behavior (e.g., a family member becomes serious ill). This contrasts with dependent stressful life events, which may be triggered by one’s actions or characteristics (e.g., getting in a fight with a friend). Thus, we investigated the role of independent stressful life events to avoid the issue of dependence between stressful events and psychopathology that may have contributed to prior findings on the associations between child maltreatment, stress, and suicidal thoughts and behavior. Additionally, independent and interpersonal stressful life events can be used to test the stress generation hypothesis because it is possible that child maltreatment triggers cascades of events that beget additional life stressors (i.e., having a family member who loses a job, or a close family member who is hospitalized). We hypothesized that child maltreatment would have a direct association with adolescent SI (Hypothesis 1 [H1]); and recent stressful life events would exacerbate the association between child maltreatment and adolescent SI (supporting the stress sensitivity hypothesis; Hypothesis 2 [H2]).
A secondary aim of the present study was to test a possible protective factor, emotion regulation, in the hypothesized pathways from child maltreatment and stressful life events to SI. Empirical studies on modifiable factors that can protect adolescents from developing suicidal thoughts can inform the development of innovative prevention efforts. There is growing evidence that emotion regulation skills can protect adolescents from a variety of adverse outcomes (e.g., Boyes et al., 2016). Maltreated and non-maltreated adolescents who are able to use emotion regulation skills, such as cognitive restructuring, may be able to cope better with recent stressful life events. Thus, we hypothesized (Hypothesis 3; [H3]) that emotion regulation would be protective for adolescents in the association between stressful life events and SI.
2. Method
2.1. Sample
The sample included socioeconomically disadvantaged and racially and ethnically diverse adolescent girls with depressive symptoms (N = 175) who were part of a larger randomized control trial (RCT) of a depression treatment (Toth et al., 2020). Participants’ average age was 14 (SD = .85; age range 13–15). The racial composition of the sample included 65.14 % adolescents who were African American, 21.14 % who were white, 6.29 % of adolescents who were biracial, and 7.43 % of adolescents who identified as another race. Additionally, 14.29 % of adolescents in the sample identified as Latina. The average family annual income was $27,970 (SD = $12,734), which included income from employment, public assistance, and other contributions to the household. The average family income did not significantly differ between adolescents with maltreatment histories (M = $27,370) and non-maltreated adolescents (M = $28,630), t (162) = .63, p = .53.
2.2. Procedures
All study procedures were approved by the Institutional Review Board for ethical conduct in research in the sponsoring university. The RCT aimed to test a psychotherapy intervention among depressed maltreated and non-maltreated adolescent girls (for more details on the RCT, see Toth et al., 2020). Adolescents with maltreatment and depression histories were recruited through a Department of Human Services (DHS) liaison and/or through advertisements in DHS waiting rooms. We also recruited maltreated adolescents through partnerships with pediatric social workers and other organizations that serve maltreated adolescents. Depressed and non-maltreated adolescent girls were recruited by a DHS liaison based on their family’s eligibility for Temporary Assistance to Needy Families (TANF). Adolescents met study inclusion criteria if their family was eligible for Temporary Assistance to Needy Families and if they were depressed. At enrollment, adolescent participants were screened via the Kiddie Schedule of Affective Disorders and Schizophrenia (K-SADS; Kaufman et al., 1997), and were included in the study if they met criteria for subsyndromal depression or clinical depression. To reduce heterogeneity among the maltreated adolescents in the sample, adolescents living in foster care were excluded. After being recruited into the study, adolescents and their parents provided their informed assent and consent, respectively. Due to variations in literacy, researchers read self-report measures to participants. The present analysis utilized baseline data from the RCT.
2.3. Measures
2.3.1. Child maltreatment
The Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) was used to assess child maltreatment. Participants responded to 28 items about their experiences of abuse and neglect while growing up, with response options ranging from 1 (never true) to 5 (very often true). The measure includes five subscales for maltreatment types (i.e., emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect). The presence of each type of maltreatment was determined using established cut-off criteria (Walker et al., 1999). A sum score of the number of maltreatment types the adolescents experienced was calculated. There were 91 girls in the sample who met criteria for maltreatment. Of the maltreated group, girls experienced on average two types of maltreatment (M = 2.11, SD = 1.23).
2.3.2. Stressful life events
Participants reported on negative life events they experienced in the past year with the Adolescent Life Events Questionnaire (Hankin & Abramson, 2002). For the present study, we utilized a subscale consisting of interpersonal and independent life events. One item was removed from the scale due to conceptual overlap with child maltreatment (“Don’t receive the love, respect, or interest from parents that you wanted”). Participants selected whether the event had occurred in the past year, and then rated how much the event bothered them from 0 (not at all) to 3 (a lot). A sum score was calculated from 12 items. On average, participants experienced 3–4 stressful life events (M = 3.65, SD = 2.42).
2.3.3. Suicide ideation
SI was assessed using participant self-report and clinical interviews. Participants reported on their SI in the past two weeks using one item (“I wish I were dead”) on the Beck Depression Inventory for Youth (BDI-Y; Beck et al., 2005). Response options ranged from 0 (never) to 3 (always). Two binary (yes/no) items from the K-SADS (Kaufman et al., 1997) were used to assess current SI, including recurrent thoughts of death and SI. Current symptomology was defined as either occurring in the worst two-week period of a current depressive episode, or in the last two months if there is was no current episode. There were 30.29 % of participants in the sample (n = 53) who were identified as having current suicidal ideation as assessed via the K-SADS or the BDI (i.e., scoring 1 or above).
2.3.4. Emotion regulation
Adolescents reported on their emotion regulation strategies using a revised version of the Emotion Regulation Questionnaire for Children and Adolescents (ERQ-CA; Gullone & Taffe, 2012). A summary score was calculated from the cognitive reappraisal subscale. Participants responded to six items on emotion regulation strategies, such as “When I want to feel happier, I think about something different”. Response options reliability (α = .77).
2.4. Analytic plan
Before testing study hypotheses, descriptive statistics, bivariate correlations, and data missingness were examined. We examined rates of stressful life events by group membership in the maltreated and non-maltreated group using chi-square difference tests. Missingness ranged from 1.14 to 2.29 %. Little’s Missing Completely at Random (MCAR) test was non-significant, χ2 = 10.24 (16), p = .86, indicating that the data were MCAR (i.e., ignorable missing data). Accordingly, missing data were handled using full information maximum likelihood (FIML).
The stress-sensitization and stress-generation hypotheses were then tested using structural equation modeling (SEM) with Mplus version 8.3 (Muthén & Muthén, 1998). Model parameters were estimated with a robust weighted least squares estimator (WLSMV), which is recommended for use in SEMs with categorical outcome variables. This estimator produces probit regression coefficients for categorical dependent variables in the model. We tested two separate SEMs. Model 1 tested the stress generation (mediation) hypothesis and Model 2 evaluated the stress sensitivity (moderation) hypothesis. The fit of all SEMs were evaluated based on standard cut-off criteria (Hu & Bentler, 1999). The measurement model included a latent variable of SI that consisted of three indicators. The mediation hypothesis was tested by evaluating the indirect effect using bootstrap-corrected confidence intervals with 5000 draws. The moderation hypothesis was tested by computing an interaction term between child maltreatment and recent stressful life events (both standardized before calculating the product term). Significant moderation effects were probed using the Johnson-Ney man approach (Hayes & Matthes, 2009). Last, we explored the protective role of emotion regulation using multiple regression analyses. A continuous indicator of SI from the BDI was used as the dependent variable, and a hierarchical regression analysis was used to test the three-way interaction (maltreatment * stressful life events * emotion regulation).
3. Results
3.1. Descriptive statistics and bivariate correlations
See Table 1 for descriptive statistics and bivariate correlations for all study variables. Data were inspected for normality and one variable (BDI - suicide ideation) was log transformed due to positive skewness (skewness = 2.36). Chi-square tests were used to explore whether experience of specific stressful life events differed by maltreatment status (See Table 2). Using standard cut-off scores on the CTQ, there were 15.43 % of the sample who reported sexual abuse, 28.00 % who reported physical abuse, 18.29 % who reported physical neglect, 14.86 % who reported emotion neglect, and 33.14 % who reported emotional abuse.
Table 1.
Bivariate Correlations (N = 175).
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Child maltreatment | – | |||||
| 2. Stressful life events | .19* | – | ||||
| 3. Emotion regulation | −.04 | .06 | – | |||
| 4. SI (K-SADS current thoughts of death) | .35*** | .16* | −.14 | – | ||
| 5. SI (K-SADS current SI | .30*** | .15 | −.11 | .67*** | – | |
| 6. SI (BDI SI) | .45*** | .25** | −.13 | .60*** | .64*** | – |
| Mean | 1.11 | 7.95 | 19.97 | 1.59 | 1.33 | .33 |
| SD | 1.38 | 6.17 | 4.12 | .84 | .70 | .68 |
Note. Child maltreatment refers to the number of subtypes. Among maltreated girls only, M = 2.11, SD = 1.23 for child maltreatment. SI = suicide ideation; K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia; BDI = Beck Depression Inventory.
p < .05.
p < .01.
p < .001.
Table 2.
Chi Square Difference Tests for Stressful Life Events.
| Life Event | Maltreatment Status | |
|---|---|---|
| Non-Maltreated (n = 82) | Maltreated (n = 91) | |
| Parents divorced | 10 (5.8 %) | 10 (5.8 %) |
| Close family member hospitalized | 50 (28.9 %) | 55 (31.8 %) |
| Close family member died | 33 (19.1 %) | 41 (23.7 %) |
| Close family member arrested | 23 (13.3 %) | 40 (23.1 %)* |
| Close family member can’t work due to injury/illness | 28 (16.2 %) | 39 (22.5 %) |
| Close family member has significant medical/emotional problems | 29 (16.8 %) | 48 (27.7 %) * |
| Boyfriend/girlfriend has been cheating on you | 13 (7.5 %) | 26 (15.0 %) * |
| Close friend was arrested | 11 (6.4 %) | 17 (9.8 %) |
| Friend was hospitalized | 19 (11.0 %) | 27 (15.6 %) |
| Close friend died | 9 (5.2 %) | 20 (11.6 %)† |
| Close friend moved away | 28 (16.2 %) | 32 (18.5 %) |
| Close friends withdraw their affection | 4 (2.3 %) | 19 (11.0 %)** |
p < .10.
p < .05.
p < .01.
3.2. Stress generation (mediation) model
The mediation model exhibited excellent fit, χ2 = .41 (df = 3), p = .94, CFI = 1.00, SRMR = .01. A latent variable with three indicators was created for SI. All indicators had a satisfactory factor loading (λ > .71) and were significant at p < .001. The error terms of two indicators obtained from the K-SADS measure were correlated (r = .84, p < .001, 95 % CI [.67, 1.00]). This latent variable for SI was used in all subsequent models. Consistent with our first hypothesis, child maltreatment was significantly associated with adolescent SI, β = .45, p < .001, 95 % CI [.27, .62], and stressful life events, β = .19, p < .05, 95 % CI [.02, .37]. Stressful life events were not directly associated with SI, β = .18, p = .051, 95 % CI [−.001, .35]. The indirect effect between child maltreatment and SI via stressful life events was not significant (α*β = .03, p = .20, 95 % CI [−.02, .09]). Because the association between stressful life events and SI was non-significant, this model did not support the stress generation hypothesis.
3.3. Stress sensitization (moderation) model
A moderation model was tested and exhibited excellent fit, χ2 = .93 (5), p = .97, CFI=1.00, SRMR = .01 (See Fig. 2). Consistent with our first hypothesis, child maltreatment was significantly associated with adolescent SI, β = .40, p < .001, 95 % CI [.24, .57]. The interaction term (child maltreatment × stressful life events) was significantly associated with SI, β = .18, p < .05, 95 % CI [.001, .36], indicating a moderation effect. The direct association between stressful life events and SI was not significant, β = .12, p = .16, 95 % CI [−.03, .27]. The moderation was probed using the Johnson-Neyman method (See Fig. 3). To facilitate interpretation, we re-scaled the x-axis to a score representing the number of maltreatment subtypes experienced. The association between stressful life events and SI was significant for adolescents who experienced more than one type of maltreatment, and this association became stronger with every additional type of maltreatment. Thus, our analysis supported our second hypothesis that child maltreatment would exacerbate the association between stressful life events and adolescent SI (i.e., the stress-sensitization model).
Fig. 2.
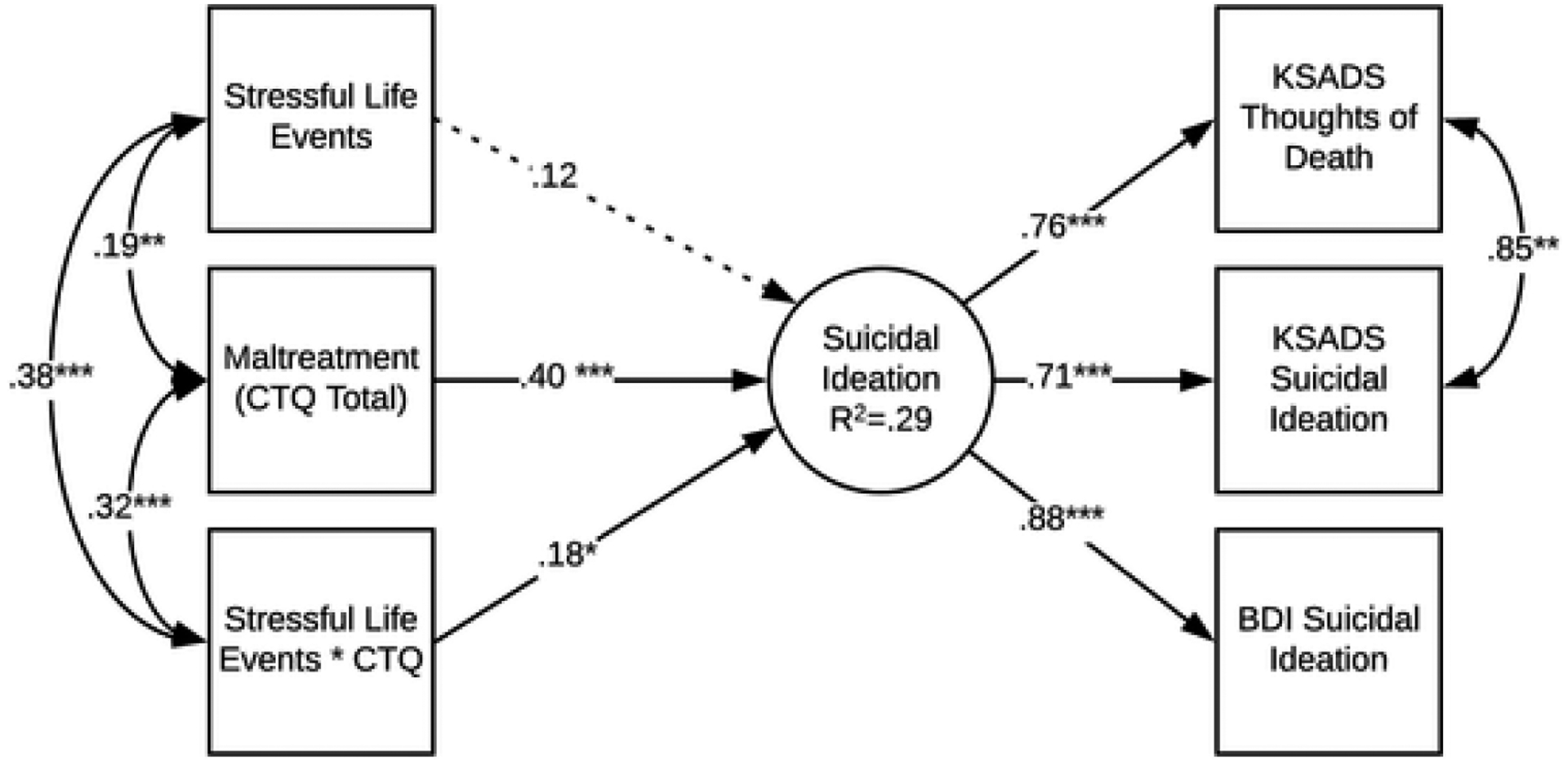
Structural equation model testing the stress-sensitization hypothesis. Note. An interaction term (stressful life events * CTQ) was included in the model to test for moderation. Model fit was excellent, CFI = 1.00, SRMR = .01, χ2 = .93 (5), p = .97. *p < .05, **p < .01, ***p < .001.
Fig. 3.
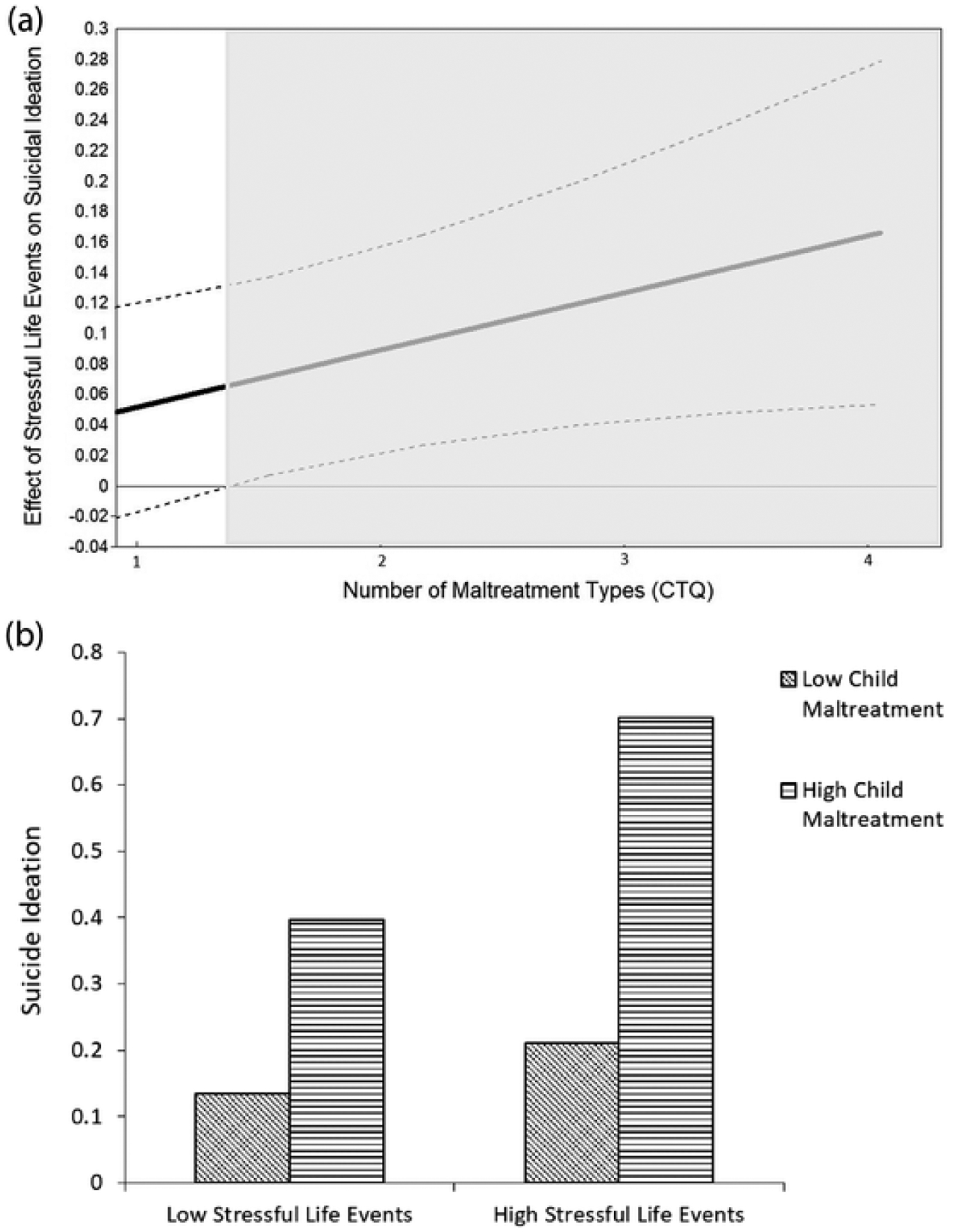
(a) Experiences of maltreatment moderate the association between stressful life events and SI (N = 175).Note. The shaded area represents the values of the moderator (maltreatment) in which the effect of stressful life events on SI is significant. Z-scores on CTQ (number of maltreatment types) were used in the analysis and then converted to raw scores to improve interpretability of the diagram. On the y-axis, numbers represent the adjusted effect size between stressful life events and suicidal ideation. (b) Experiences of maltreatment moderate the association between stressful life events and SI (N = 175). Note. In this moderation plot, “low” and “high” values of stressful life events are −1 SD and +1 SD from the mean, respectively. Low child maltreatment refers to children who experienced no subtypes, while high child maltreatment refers to adolescents who experienced three subtypes.
3.4. Emotion regulation as a protective factor
We used a hierarchical regression analysis to test the protective role of emotion regulation (Hypothesis 3). Results from the hierarchical regression analysis are displayed in Table 3. The interaction term of stressful life events × emotion regulation significantly predicted SI, supporting our hypothesis that emotion regulation would buffer the association between adolescents’ exposure to stressful life events and SI. Additionally, there was a significant association between the interaction of child maltreatment × stressful life events and SI. The three-way interaction term was not significantly associated with SI. Thus, the buffering role of emotion regulation in the association between stressful life events and SI did not differ by maltreatment experiences.
Table 3.
Hierarchical Regression Analysis to Test the Protective Role of Emotion Regulation (H3) (N = 172).
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE B | β | B | SE B | β | B | SE B | β | |
| Child maltreatment (CM) | .061 | .009 | .413*** | .054 | .009 | .368*** | .054 | .009 | .368*** |
| Stressful life events (SLE) | .023 | .009 | .151* | .018 | .009 | .121† | .018 | .009 | .121† |
| Emotion regulation (ER) | −.012 | .009 | −.077 | −.006 | .009 | −.041 | −.006 | .009 | −.040 |
| CM × SLE | .015 | .007 | .142* | .016 | .007 | .143* | |||
| CM × ER | .005 | .009 | .038 | .005 | .010 | .039 | |||
| SLE × ER | −.018 | .008 | −.145* | −.018 | .009 | −.144* | |||
| CM × SLE × ER | .000 | .005 | .004 | ||||||
| R 2 | .224 | .258 | .258 | ||||||
| F change | 21.490*** | 3.323* | .002 | ||||||
p < .10.
p < .05.
p < .001.
We probed the interaction between stressful life events and emotion regulation using a simple slopes test and found that the gradient of slope was significant for low (−1 SD) levels of emotion regulation, B = .036, p < .001, but not for high (+1 SD) levels of emotion regulation, B = .000, p = .071. Thus, consistent with a protective effect, the association between stressful life events and SI was significant only for adolescents with lower levels of emotion regulation skills.
4. Discussion
A recent study found that suicide rates for girls in early adolescence are increasing in comparison to boys in their age group (Ruch et al., 2019). Consequently, it is increasingly important to identify developmentally salient risk factors for suicidal thoughts and behaviors among adolescent girls to inform suicide prevention efforts. In the present study, we used a sample of diverse low-SES depressed adolescent girls and found that child maltreatment was directly associated with higher levels of SI, as expected. Further, we tested two competing theories of stress and psychopathology (the stress generation and stress sensitization theory) and found support for the latter. Namely, girls who experienced maltreatment were more likely to exhibit SI in response to the independent interpersonal stressors they experienced in the past year.
The stress sensitization hypothesis suggests that experiencing chronic stress during early childhood can exacerbate the impact of recent life stressors (Hammen et al., 2000). In other words, adolescents who face stressful life events may be more negatively impacted by these events if they also have a background of child maltreatment. Early childhood is a developmental period characterized by heightened plasticity, and the experience of chronic stress (e.g., maltreatment) can shape the way neurobiological stress response systems develop, leading to a heightened sensitivity to stressors that these adolescents experience later in life (Heim & Nemeroff, 2001). Specifically, chronic stressors in childhood such as child maltreatment have been found to disrupt physiological systems that handle an individual’s response to stress, such as the hypothalamic-pituitary-adrenal (HPA) axis and the autonomic nervous system (Alink et al., 2012; Loman & Gunnar, 2010; McLaughlin et al., 2015). Adolescents who have suffered child maltreatment and have not developed an adaptive physiological response to stress may not be able to cope with stressful life events. These stress sensitization effects may be even more pronounced during adolescence, a developmental period characterized by heightened brain plasticity in areas associated with social stress (Fuhrmann et al., 2015). However, further research is needed to test the neurobiological basis of associations between child maltreatment and acute life stressors with adolescent SI. Specifically, longitudinal studies that incorporate physiological measures of stress responsivity with measures of chronic and acute life stress will help to advance our understanding of stress and adolescent suicidality. Newer methodologies such as ecological momentary assessment with physiological data collection (i.e., Bertz et al., 2018), combined with prospective longitudinal designs, may be particularly suited for this goal. Simultaneously, there is also a need for applied studies that evaluate the efficacy and effectiveness of suicide prevention interventions for youth with maltreatment histories, along with studies that investigate the association between child maltreatment, stressful life events, and suicide deaths.
The present study findings also support emotion regulation strategies as a protective factor for adolescent girls who are at risk for suicidal thoughts. Specifically, we tested a component of emotion regulation, cognitive reappraisal, and found that adolescents who exhibited high levels of this emotion regulation skill were less likely to exhibit suicidal thoughts after exposure to stressful life events. This is consistent with prior research that shows emotion regulation strategies as protective for adolescents who experience life stress (Boyes et al., 2016). For example, in a recent study with adolescents in Australia, adverse life events predicted psychological distress one year later, but this association was buffered by higher levels of cognitive reappraisal (Boyes et al., 2016). The present study extends this work, finding that cognitive reappraisal moderates the association between recent stressful life events and suicidal thoughts for adolescent girls. Further, we found that the protective role of emotion regulation did not differ depending on adolescents’ exposure to child maltreatment. Thus, suicide prevention programs might be tailored for use with adolescent girls by incorporating emotion regulation skills training. However, this finding will need to be replicated in other samples of adolescent girls.
Despite the importance of these findings, several limitations must be considered. First, we used retrospective reports of child maltreatment via the CTQ, and operationalized child maltreatment as the number of types of maltreatment adolescents experienced. However, maltreatment is multidimensional and the consequences may differ by timing (i.e., when in a child’s life the maltreatment occurred), subtype, severity (Manly et al., 2001), and assessment method (Shaffer et al., 2008). It is possible that the results from this study would differ if considering other dimensions of child maltreatment. Additionally, retrospective self-reports of maltreatment such as the CTQ may be biased for several reasons including social desirability bias, and may have different associations with psychopathology than maltreatment assessed via official child protective services records (Shaffer et al., 2008). However, self-reported maltreatment is advantageous for use in research because maltreatment is often undetected in official reports (Fallon et al., 2010). Second, we are unable to make causal assumptions on the associations between child maltreatment, stressful life events, and SI due to the use of cross-sectional data. However, we did retain some temporal ordering by assessing current suicidal thoughts and stressful life events in the past year. Finally, our sample comprised of adolescent girls with depressive symptoms, who consented to being part of a therapeutic intervention. These results may not generalize to other genders, non-clinical populations of adolescents, or adolescents who are not part of therapeutic RCTs. However, the sample we recruited was not treatment seeking and thus these results are more likely to generalize to low-SES adolescent girls with depression who do not seek treatment.
These findings have several implications for suicide prevention. First, this study underscores the importance of primary prevention of child maltreatment. Preventing child abuse and neglect may have positive upstream benefits for youth mental health, including suicide prevention. Second, it is important to recognize that life stressors may have a greater negative impact on maltreated adolescents, compared to non-maltreated adolescents. Clinicians who work with depressed adolescent girls should assess their clients’ history of maltreatment, in addition to recent and current life stressors, when evaluating risk factors for suicide. Additionally, when working with adolescent girls with histories of maltreatment who have also experienced recent stressful life events, clinicians should take care to screen for suicidal thoughts and behaviors. Further, while it may not be possible to limit the number of life stressors that adolescents experience, clinicians may be able to strengthen youths’ ability to cope with these stressors by working on emotion regulation skills. Cognitive-focused interventions that have evidence of effectiveness with suicidal adolescents, such as CBT for suicide prevention, may be particularly useful (Stanley et al., 2009). Additionally, Interpersonal Psychotherapy (IPT) is an efficacious therapeutic model for individuals with maltreatment histories (Toth et al., 2013; Toth et al., 2020), and may be particularly helpful to reduce depressive symptoms and suicidal ideation for adolescents who experience interpersonal life stressors. Last, stressful life events often occur in the context of family and neighborhood poverty. It is important for researchers, clinicians, and other youth-serving professionals to continue to advocate for local, state, and federal policies that reduce the burden of poverty and con sequently reduce the frequency of stressful life events for low-SES adolescents.
Acknowledgements
This work was supported by funding through the National Institute on Mental Health (R01-MH091070). Training support was also provided to the lead author via the National Institute on Mental Health (T32 MH20061).
Footnotes
In this manuscript, in accordance with established guidelines (Patton et al., 2016), we define adolescence as the period from aged 10–19, and youth as the period from ages 15–24.
References
- Alink LRA, Cicchetti D, Kim J, & Rogosch FA (2012). Longitudinal associations among child maltreatment, social functioning, and cortisol regulation. Developmental Psychology, 48(1), 224–236. doi: 10.1037/a0024892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andersen SL, & Teicher MH (2008). Stress, sensitive periods and maturational events in adolescent depression. Trends in Neurosciences, 31(4), 183–191. doi: 10.1016/j.tins.2008.01.004. [DOI] [PubMed] [Google Scholar]
- Beck JS, Beck AT, Jolly JB, & Steer RA (2005). Beck youth inventories for children and adolescents manual (2nd ed.). PsychCorp. [Google Scholar]
- Bernstein DP, & Fink L (1998). Childhood trauma questionnaire: A retrospective self-report: Manual. Psychological Corporation. [Google Scholar]
- Bertz JW, Epstein DH, & Preston KL (2018). Combining ecological momentary assessment with objective, ambulatory measures of behavior and physiology in substance-use research. Addictive Behaviors, 83, 5–17. doi: 10.1016/j.addbeh.2017.11.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyes ME, Hasking PA, & Martin G (2016). Adverse life experience and psychological distress in adolescence: Moderating and mediating effects of emotion regulation and rumination. Stress and Health, 32(4), 402–410. doi: 10.1002/smi.2635. [DOI] [PubMed] [Google Scholar]
- Cicchetti D (2016). Socioemotional, personality, and biological development: Illustrations from a multilevel developmental psychopathology perspective on child maltreatment. Annual Review of Psychology, 67(1), 187–211. doi: 10.1146/annurev-psych-122414-033259. [DOI] [PubMed] [Google Scholar]
- Curtin SC, & Heron M (2019). Death rates due to suicide and homicide among persons aged 10 – 24: United States, 2000 – 2017. NCHS data brief, no 352. [PubMed] [Google Scholar]
- Dupéré V, Leventhal T, & Lacourse É (2009). Neighborhood poverty and suicidal thoughts and attempts in late adolescence. Psychological Medicine, 39(8), 1295–1306. doi: 10.1017/S003329170800456X. [DOI] [PubMed] [Google Scholar]
- Fallon B, Trocmé N, Fluke J, MacLaurin B, Tonmyr L, & Yuan YY (2010). Methodological challenges in measuring child maltreatment. Child Abuse and Neglect, 34(1), 70–79. doi: 10.1016/j.chiabu.2009.08.008. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Woodward LJ, & Horwood LJ (2000). Risk factors and life processes associated with the onset of suicidal behaviour during adolescence and early adulthood. Psychological Medicine, 30, 23–39. doi: 10.1017/S003329179900135X. [DOI] [PubMed] [Google Scholar]
- Fuhrmann D, Knoll LJ, & Blakemore SJ (2015). Adolescence as a sensitive period of brain development. Trends in Cognitive Sciences, 19(10), 558–566. doi: 10.1016/j.tics.2015.07.008. [DOI] [PubMed] [Google Scholar]
- Gomez SH, Tse J, Wang Y, Turner B, Millner AJ, Nock MK, & Dunn EC (2017). Are there sensitive periods when child maltreatment substantially elevates suicide risk? Results from a nationally representative sample of adolescents. Depression and Anxiety, 34(8), 734–741. doi: 10.1002/da.22650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gullone E, & Taffe J (2012). The emotion regulation questionnaire for children and adolescents (ERQ–CA): A psychometric evaluation. Psychological Assessment, 24(2), 409–417. doi: 10.1037/a0025777. [DOI] [PubMed] [Google Scholar]
- Hammen C, Henry R, & Daley SE (2000). Depression and sensitization to stressors among young women as a function of childhood adversity. Journal of Consulting and Clinical Psychology, 68(5), 782–787. doi: 10.1037/0022-006X.68.5.782. [DOI] [PubMed] [Google Scholar]
- Handley ED, Adams TR, Manly JT, Cicchetti D, & Toth SL (2018). Mother-daughter interpersonal processes underlying the association between child maltreatment and adolescent suicide ideation. Suicide & Life-threatening Behavior, 1–9. doi: 10.1111/sltb.12522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankin BL, & Abramson LY (2002). Measuring cognitive vulnerability to depression in adolescence: Reliability, validity, and gender differences. Journal of Clinical Child and Adolescent Psychology, 31(4), 491–504. doi: 10.1207/S15374424JCCP3104_8. [DOI] [PubMed] [Google Scholar]
- Hayes AF, & Matthes J (2009). Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behavior Research Methods, 41(3), 924–936. doi: 10.3758/BRM.41.3.924. [DOI] [PubMed] [Google Scholar]
- Heim C, & Nemeroff CB (2001). The role of childhood trauma in the neurobiology of mood and anxiety disorders: Preclinical and clinical studies. Biological Psychiatry, 49(12), 1023–1039. doi: 10.1016/S0006-3223(01)01157-X. [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling A Multidisciplinary Journal, 6(1), 1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Joiner TE, & Rudd MD (1995). Negative attributional style for interpersonal events and the occurrence of severe interpersonal disruptions as predictors of self-reported suicidal ideation. Suicide and Life-Threatening Behavior, 25(2), 297–304. doi: 10.1111/j.1943-278X.1995.tb00927.x. [DOI] [PubMed] [Google Scholar]
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Queen B, … Ethier K (2018). Youth risk behavior surveillance-united states 2017. MMWR Surveillance Summaries, Vol. 67(Issue 8). doi: 10.1144/jmpaleo2015-007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman J, Birmaher B, Brent D, Rao UMA, Flynn C, Moreci P, … Ryan N (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child & Adolescent Psychiatry, 36(7), 980–988. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- Kwok SYCL, & Gu M (2019). Childhood neglect and adolescent suicidal ideation: A moderated mediation model of hope and depression. Prevention Science, 20(5), 632–642. doi: 10.1007/s11121-018-0962-x. [DOI] [PubMed] [Google Scholar]
- Lindsey MA, Sheftall AH, Xiao Y, & Joe S (2019). Trends of suicidal behaviors among high school students in the United States: 1991–2017. Pediatrics, 144(5). doi: 10.1542/peds.2019-1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu RT, & Miller I (2014). Life events and suicidal ideation and behavior: A systematic review. Clinical Psychology Review, 34(3), 181–192. doi: 10.1016/j.cpr.2014.01.006. [DOI] [PubMed] [Google Scholar]
- Loman MM, & Gunnar MR (2010). Early experience and the development of stress reactivity and regulation in children. Neuroscience and Biobehavioral Reviews, 34(6), 612–624. doi: 10.1016/j.neubiorev.2009.05.007.Early. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKin DM, Perlman G, Davila J, Kotov R, & Klein DN (2017). Social support buffers the effect of interpersonal life stress on suicidal ideation and self-injury during adolescence. Psychological Medicine, 47(6), 1149–1161. doi: 10.1017/S0033291716003275. [DOI] [PubMed] [Google Scholar]
- Manly JT, Kim JE, Rogosch FA, & Cicchetti D (2001). Dimensions of child maltreatment and children’s adjustment: Contributions of developmental timing and subtype. Development and Psychopathology, 13(4), 759–782. [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, Tibu F, Fox NA, Zeanah CH, & Nelson CA (2015). Causal effects of the early caregiving environment on development of stress response systems in children. Proceedings of the National Academy of Sciences of the United States of America, 112(18), 5637–5642. doi: 10.1073/pnas.1423363112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller AB, Esposito-Smythers C, Weismoore JT, & Renshaw KD (2013). The relation between child maltreatment and adolescent suicidal behavior: A systematic review and critical examination of the literature. Clinical Child and Family Psychology Review, 16(2), 146–172. doi: 10.1007/s10567-013-0131-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller AB, Eisenlohr-Moul T, Giletta M, Hastings PD, Rudolph KD, Nock MK, & Prinstein MJ (2017). A within-person approach to risk for suicidal ideation and suicidal behavior: Examining the roles of depression, stress, and abuse exposure. Journal of Consulting and Clinical Psychology, 85(7), 712–722. doi: 10.1037/ccp0000210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2017). Mplus user’s guide (Eighth). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Naninck EFG, Lucassen PJ, & Bakker J (2011). Sex Differences in Adolescent Depression: Do Sex Hormones Determine Vulnerability? Journal of Neuroendocrinology, 23(5), 383–392. doi: 10.1111/j.1365-2826.2011.02125.x. [DOI] [PubMed] [Google Scholar]
- Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, … Viner RM (2016). Our future: A Lancet commission on adolescent health and wellbeing. Lancet, 387(10036), 2423–2478. doi: 10.1016/S0140-6736(16)00579-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruch DA, Sheftall AH, Schlagbaum P, Rausch J, Campo JV, & Bridge JA (2019). Trends in suicide among youth aged 10 to 19 years in the United States, 1975 to 2016. JAMA Network Open, 2(5), e193886. doi: 10.1001/jamanetworkopen.2019.3886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rudolph KD (2002). Gender differences in emotional responses to interpersonal stress during adolescence. Journal of Adolescent Health, 30(4), 3–13. doi: 10.1016/S1054-139X(01)00383-4. [DOI] [PubMed] [Google Scholar]
- Shaffer A, Huston L, & Egeland B (2008). Identification of child maltreatment using prospective and self-report methodologies: A comparison of maltreatment incidence and relation to later psychopathology. Child Abuse & Neglect, 32(7), 682–692. doi: 10.1016/j.chiabu.2007.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley B, Brown G, Brent DA, Wells K, Poling K, Curry J, … Hughes J (2009). Cognitive-behavioral therapy for suicide prevention (CBT-SP): Treatment model, feasibility, and acceptability. Journal of the American Academy of Child and Adolescent Psychiatry, 48(10), 1005–1013. doi: 10.1097/CHI.0b013e3181b5dbfe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toth SL, Rogosch FA, Oshri A, Gravener-Davis J, Sturm R, & Morgan-López AA (2013). The efficacy of interpersonal psychotherapy for depression among economically disadvantaged mothers. Development and Psychopathology, 25(4 PART 1), 1065–1078. doi: 10.1017/S0954579413000370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toth SL, Handley ED, Manly JT, Sturm R, Adams TR, Demeusy EM, & Cicchetti D (2020). The moderating role of child maltreatment in treatment efficacy for adolescent depression. Journal of Abnormal Child Psychology, 48(10), 1351–1365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, & Joiner TE (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575–600. doi: 10.1037/a0018697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker EA, Gelfand A, Katon WJ, Koss MP, Von Korff M, Bernstein D, & Russo J (1999). Adult health status of women with histories of childhood abuse and neglect. The American Journal of Medicine, 107(4), 332–339. doi: 10.1016/S0002-9343(99)00235-1. [DOI] [PubMed] [Google Scholar]
- Hankin Benjamin (2005). Childhood maltreatment and psychopathology: Prospective tests of attachment, cognitive vulnerability, and stress as mediating processes. Cognitive Therapy and Research, 29(6), 645–671. doi: 10.1007/s10608-005-9631-z. [DOI] [Google Scholar]