

Abstract
Objective:
To study the root and root canal morphology of mandibular premolars in a Kuwaiti subpopulation using cone-beam computed tomography (CBCT).
Methods:
152 CBCT images were obtained from the radiology department archives of four dental centers in Kuwait. A total of 476 mandibular premolar teeth were analyzed by two observers. The number of roots, root canal configuration types and canal curvature measurements were examined. The relationship between sex, tooth position, and incidence of an additional canal were compared using the chi-square test, and the level of significance was set at 0.05 (P=0.05).
Results:
The number of roots in mandibular first premolars was one in 73.9%, two in 24.9%, three and four in 1.2%. On the other hand, the number of roots in mandibular second premolars was one in 79.2% and two in 20.8%. Based on Vertucci’s classification system, 18.7% of the teeth were type II followed by type VI (14.3%). The majority of the examined teeth were straight (74.8%) and the incidence of distal root angulation was about 21%. Canal configurations not included in the Vertucci classification were reported in 102 teeth (21.4%). Variability was significantly higher in the second premolars compared to first premolar (P<0.05).
Conclusion:
The Kuwaiti population has complex root canal morphology in mandibular premolar teeth.
Keywords: Cone-beam computed tomography, mandibular premolar, root canal configuration, root canal morphology, root shape
HIGHLIGHTS.
The root canal morphology of mandibular premolar teeth of Kuwaiti population is complex.
The most common root canal configuration of mandibular premolars was type II (18.7%).
The majority of roots in mandibular premolars were straight (74.8%).
Males had greater variation in canal morphology compared to females.
INTRODUCTION
Adequate removal of infected pulp tissues is the main objective of root canal treatment procedures (1-3). Therefore, clinicians need to have sound knowledge and clear visualization of the internal and external tooth morphology and its common variations to improve the prognosis of root canal treatment.
The root canal anatomy of each tooth has certain commonly occurring characteristics, as well as a typical variations that require special attention during root canal treatment (4). The relative simplicity and uniformity of the external surfaces of the roots usually mask a complex internal morphology (5). Therefore, the exact details of the root canal system and its anatomical variations must be considered to achieve a successful outcome. Mandibular first premolars are amongst the most Challenging teeth to treat because of the high incidence of multiple roots or canals (4). In addition, these teeth have a high rate of failure after root canal treatment (6).
On average, 91.0% of mandibular second premolars have a single canal and 9.0% have two or more canals (7). In rare cases, two or three roots with four canals have been reported (8, 9). In addition, a high incidence rate (up to 24%) of C-shaped canals has been reported in Chinese populations (10). Most C-shaped premolars have a groove or concavity on the external root surface, which frequently presents on the proximal lingual area of the middle root (11). Numerous factors contribute to variation in the human root and canal morphology, including ethnicity, age, and sex (2, 12-16).
Few studies investigated the root and canal morphology in Kuwaiti population (17-19), which are mainly undertaken in first molars and mandibular premolars using conventional radiographic imaging (17). Previous studies on mandibular premolars have used methods such as hard tissue section, root canal staining and clearing, and micro-CT scanning to visualize (12, 16-17, 20, 21). More recently, Cone beam computed tomography (CBCT) has been used as reliable diagnostic tool (22). It provides high quality images and reduced exposure compared to conventional CT (23). This study aimed to investigate the root and canal morphology in mandibular first and second premolars in Kuwaiti population using CBCT.
MATERIALS AND METHODS
Sample collection
A total of 197 CBCT images were collected from the radiology department archives of four dental centers in Kuwait (Adan, Farwania, Jaber, and Alamirri) between October 2015 and February 2017. The images were collected from patients who had undergone CBCT scanning for various diagnostic purposes. Images were taken using a 3D X CBCT Creanex machine (SOREDEX Manufacturing Corp., Helsinki, Finland) with image capture parameters set at 90 kV and 5-10 mA, with an exposure time of 6.5 s, voxel size of 0.1mm, and slice thickness of 1.0 mm. The identities of the patients were not revealed and only information regarding sex and age was acquired. The study was approved by the Ethics Committee of Riyadh Elm University (registration number is FPGRP/43733003/220).
In all, 152 CBCT images (60 from Adan, 36 from Farwania, 29 from Jaber, and 27 from Amirri dental centers) were acquired from 80 male and 72 female patients. A total of 476 mandibular premolars (253 male and 223 female) were analyzed according to the following inclusion criteria: age 16–65 years; Kuwaiti citizenship; no periapical lesions, resorption, or canal calcification; no history of root canals; fully mature (closed) root apices; and good-quality CBCT images. The patient’s and sex as well as tooth position in the arch were recorded.
Radiographic evaluation
The CBCT images were analyzed using OnDemand 3D software (Cybermed, Seoul, Korea) and were evaluated retrospectively by two experienced examiners (one endodontist and one oral and maxillofacial radiologist). The CBCT images were numbered and evaluated separately to avoid any potential sources of bias. Axial, coronal, and sagittal sections of the CBCT images were displayed on a 32-inch LCD screen (HP Inc, USA) with a resolution of 1.280×1.024 pixels. The images were interpreted in a dark room. Adjustment of the magnification and contrast was done to ensure optimal visualization and examination. The data reliability was previously assessed through an inter-examiner calibration based on the anatomic diagnosis of the CBCT images. The CBCT images were evaluated according to the following criteria: root canal configuration in each root according to the Vertucci classification system (1) and the supplemental configurations reported by Sert and Bayirli (14).; the number of roots per tooth; root morphology categorized as fused (two or more roots that joined together) or separated (clearly divided–apical root bifurcations are considered as separate); angulation of the root (none, mesial, distal, lingual or buccal); curvature of the root canal based on the Schneider method (24) (moderate or severely curved); and the location of the radicular groove (none, mesial, distal, lingual or buccal). C-shaped root canal was also evaluated using Fan et al. (10) classification that include: category-I: a continuous “C” with no separation or division; category II (C2): a discontinuation in the “C” outline (semicolon-like); category III (C3): two separate round, oval, or flat canals; category IV (C4): only one round, oval, or flat canal in that cross-section; category V (C5): three or more separated canals in the cross-section; category; and category VI (C6): no canal lumen could be observed.
Pilot study
A pilot exercise was done with three samples presented by the oral and maxillofacial radiologist to familiarize the examiners with the CBCT images and tools and to reach an agreement on what should be recorded. Examiners read three CBCT images twice with a 1-week interval between the assessments. After the initial reading, the radiologist selected 10 additional CBCT images for evaluation with a 1-week interval between readings. After the exercise, intra- and inter-examiner reliability was determined.
Statistical analysis
All statistical analyses were performed using SPSS ver. 22 (IBM, Armonk, NY, USA). The relationship between sex, tooth position, and incidence of an additional canal were compared using the chi-square test. Inter- and intra-examiner reliability were measured using the Cohen’s kappa coefficient (κ) and intraclass correlation coefficient (ICC).
RESULTS
A total of 245 first and 231 second mandibular premolars (n=476) were evaluated. The number of roots in mandibular first premolars was one in 73.9%, two in 24.9%, three and four in 1.2%. On the other hand, the number of roots in mandibular second premolars was one in 79.2% and two in 20.8%. The Vertucci classifications of the canal configurations are listed in Table 1. The highest percentage of the teeth was type II (18.7%) (Fig. 1). The least common root canal configurations were type VII (1.9%) in the mandibular first (1.1%) and second (0.5%) premolars. Canal configurations not included in Vertucci’s classification were found in 102 teeth (Fig. 1). No significant difference between the first and second premolars (P<0.05). C-shaped canals were only detected in the second premolars (1.3%) (Fig. 2).
TABLE 1.
Assessment of configuration of root canal morphology of mandibular premolars according to Vertucci 1984 classification
| Configuration of root canals | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tooth | Type I (1-1) | Type II (2-1) | Type III (1-2-1) | Type IV (2-2) | Type V (1-2) | Type VI (2-1-2) | Type VII (1-2-1-2) | Type VIII (3-3) | Others (different types) | C-shaped | Total | Chi-square (df) | P value |
| Left | |||||||||||||
| First premolar | 13 (10.7%) | 20 (16.5%) | 23 (19%) | 12 (9.9%) | 11 (9.1%) | 18 (14.9%) | 2 (1.7%) | (0%) | 22 (18.2%) | (0%) | 121 (100%) | 68.01(7) | 0.001 |
| Second premolar | 14 (12%) | 24 (20.5%) | 13 (11.1%) | 13 (11.1%) | 5 (4.3%) | 15 (12.8%) | 2 (1.7%) | (0%) | 30 (25.6%) | 1 (0.9%) | 117 (100%) | ||
| Right | |||||||||||||
| First premolar | 24 (19.4%) | 23 (18.5%) | 18 (14.5%) | 8 (6.5%) | 8 (6.5%) | 16 (12.9%) | 3 (2.4%) | (0%) | 24 (19.4%) | (0%) | 124 (100%) | 70.09(8) | 0.9994 |
| Second premolar | 16 (14%) | 22 (19.3%) | 13 (11.4%) | 7 (6.1%) | 4 (3.5%) | 19 (16.7%) | 2 (1.8%) | (0%) | 26 (22.8%) | 5 (4.4%) | 114 (100%) | ||
| Total number of teeth | 67 (14.1%) | 89 (18.7%) | 67 (14.1%) | 40 (8.4%) | 28 (5.9%) | 68 (14.3%) | 9 (1.9%) | (0%) | 102 (21.4%) | 6 (1.3%) | 476 (100%) | ||
Figure 1.
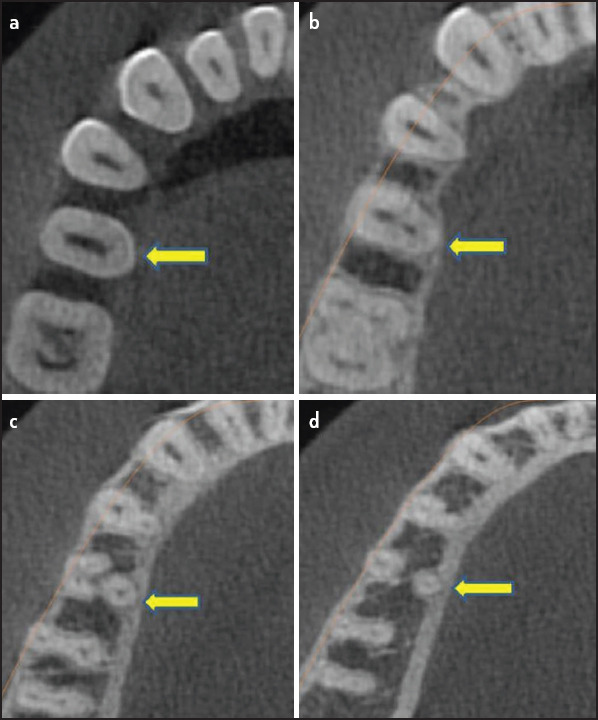
CBCT image of second mandibular premolar with joined roots at coronal third (b) then separated at the apical third (c and d) (yellow arrow). Canal configuration is 2-3-2 (a, b, c and d). The roots of the first premolar are fused with type II canal configuration
Figure 2.
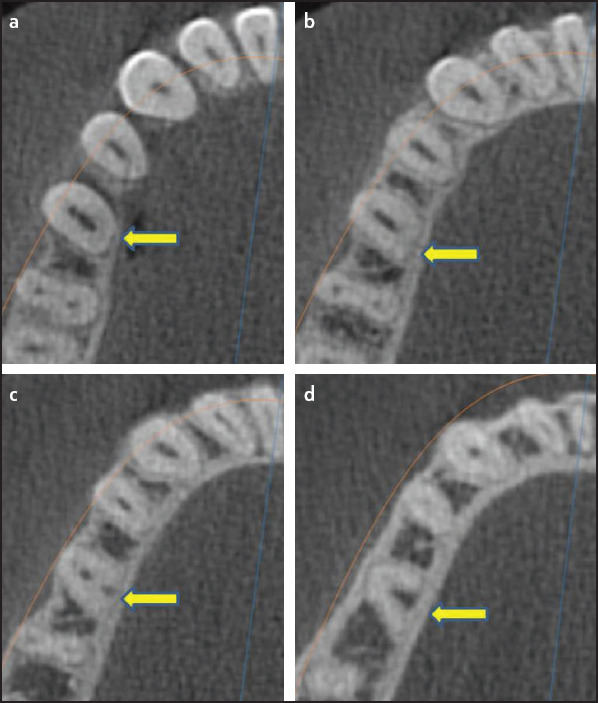
CBCT image of second mandibular premolar with C-shaped root canal configuration at different levels (a, b, c and d)
The majority of teeth had a single root (76.5%) in both the first (38.0%) and second (38.5%) premolars. Three and four roots were occasionally seen in the first premolars only.
The number of examined teeth was slightly higher in males (n=253) than females (n=223) (Table 2). No significant difference was detected in the number of roots in the first and second premolar between males and females (P>0.05). A few teeth (23.5%) had either separated (n=94, 19.6%) or fused roots (n=18, 3.8%) (Table 3) (Fig. 3). No significant difference was detected in root types between males and females (P>0.05).
TABLE 2.
Distribution of the number of roots in mandibular premolars according to gender
| Gender and number of teeth | Number of roots | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First premolar | Second premolar | |||||||||||
| One | Two | Three | Four | Chi-square | P value (df) | One | Two | Three | Four | Chi-square | P value (df) | |
| Male (253) | 93 (36.8%) | 31 (12.3%) | 2 (0.8%) | 0 (0%) | 0.0058 (1) | 0.939 | 99 (39.1%) | 28 (11.1%) | 0 (0%) | 0 (0%) | 0.276 (1) | 0.599 |
| Female (223) | 88 (39.5%) | 30 (13.5%) | 0 (0%) | 1 (0.5%) | 84 (37.7%) | 20 (9.0%) | 0 (0%) | 0 (0%) | ||||
| Total (476) | 181 (38.0%) | 61 (12.8%) | 2 (0.4%) | 1 (0.2%) | 183 (39.2%) | 48(10.3%) | 0(0%) | 0(0%) | ||||
TABLE 3.
Type of roots (fused/separated) in mandibular premolars according to gender
| Number of teeth | Type of roots | Total type with fused/separated roots | ||||||
|---|---|---|---|---|---|---|---|---|
| First premolar | Second premolar | Chi-square (df) | P value | |||||
| Fused | Separated | Fused | Separated | |||||
| Gender | ||||||||
| Male | 253 | 4 (6.6%) | 29 (47.5%) | 7 (11.5%) | 21 (34.4%) | 0.6867 (3) | 0.867 | 61 (54.5%) |
| Female | 223 | 5 (9.8%) | 26 (51%) | 2 (3.9%) | 18 (35.3%) | 51 (45.6%) | ||
| Total | 476 | 9 (8.0%) | 55 (49.1%) | 9 (8%) | 39 (34.8%) | 112 | ||
Figure 3.

Mesiodistal CBCT images of mandibular right first premolar. The image of the canal disappeared in the middle-third (a). Cross-section CBCT image showing two separated roots at the middle-third (b-f). Axial CBCT image at the cervical third showing 2 canals (g), more towered the middle showing 2 canals (h), close to the apical third showing 3 canals with fused roots (i) and 3 canals at the apex (j). Notice the lingual root fused to the distobuccal root. (Arrows points to the canals). Canal configuration is 2-3
The majority (74.8%) of the examined teeth were straight (n=356) and the incidence of distal root angulation was 21.01% (n=100) (Table 4). No significant differences in angulation were detected between the first and second premolars (P>0.05). Moderate (11.1%) to severe (14.1%) root angulations were seen in 53 and 67 teeth respectively (Table 5). A radicular groove was uncommon (8%), but when present, it was most commonly located in the mesial aspect of the first premolar root (4.8%) compared to other surfaces (Fig. 4). C-shaped canal configurations were only detected in the second mandibular premolars (1.3%) and they exhibit category III (C3) of Fan et al classification (10).
TABLE 4.
Root angulation presence and its orientation in first and second mandibular premolars
| Tooth | Number of teeth | Root angulation | Chi-square (df) | P value | ||||
|---|---|---|---|---|---|---|---|---|
| None (Straight) | Mesial | Distal | Lingual | Buccal | ||||
| First premolar | 255 | 183 (71.8%) | 11 (4.3%) | 61 (23.9%) | 0 (0%) | 0(0%) | 1.03 (2) | 0.579 |
| Second premolar | 221 | 173 (78.3%) | 8 (3.6%) | 39 (17.6%) | 1 (0.5%) | 0(0%) | ||
| Total | 476 | 356 (74.8%) | 19 (4%) | 100 (21.0%) | 1 (0.2%) | 0(0%) | ||
TABLE 5.
Number and distribution of teeth according to the degree root angulations
| Tooth | Number of teeth | Degree of root angulation | Chi-square (df) | P value | |||
|---|---|---|---|---|---|---|---|
| None | Moderate (10-20) | Sever >20 | |||||
| First premolar | 255 | 183 (71.7%) | 34 (13.3%) | 3.057(2) | 0.267 | ||
| Second premolar | 221 | 173 (78.3%) | 19 (8.6%) | 29 (13.1%) | |||
| Total | 476 | 356 (74.8%) | 53 (11.1%) | 67 (14.1%) | |||
Figure 4.
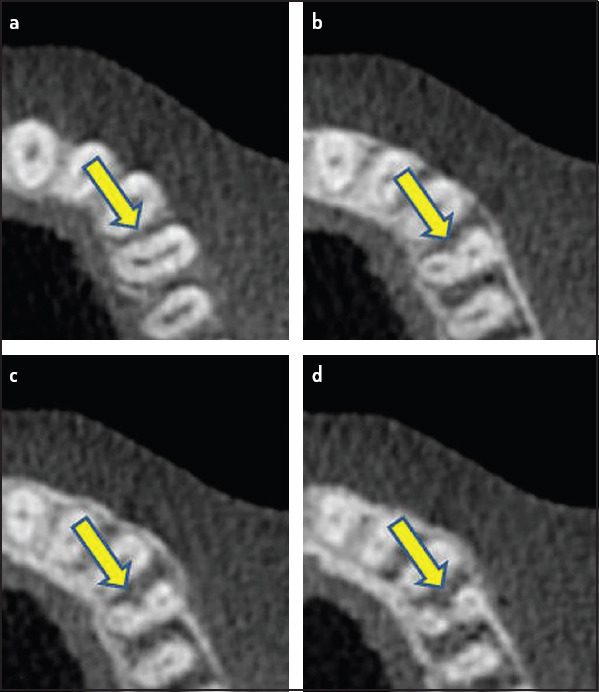
CBCT image of radicular groove located in the mesial aspect of the first mandibular premolar root surfaces at different levels (a, b, c and d)
The kappa test showed inter-rater reliability to be in average 93.6%. The intra-examiner reliability was 94% (ICC=0.8).
DISCUSSION
The success of nonsurgical endodontic therapy is closely associated with properly locating, cleaning, and shaping the root canal and placing appropriate filling materials (25). Therefore, it is essential for clinicians to have knowledge about root canal configurations, particularly because their morphology varies between races and even between individuals with the same racial background (26).
A pilot exercise was carried out starting with 3 CBCT images to reach an agreement between the examiners on what should be recorded. After that, an additional 10 CBCT images were evaluated independently. The number of evaluated samples was sufficient (27). Samples of 10-30 of were reported by Isaac and Michael (28) is simple and easy to calculate.
Several methodologies have been proposed for the evaluation of root canal anatomy. The clearing technique is frequently used (20) but can only be applied after extraction and has limitations in diagnosing C-shaped canals (10). The use of conventional radiographs at different angles is another often-used technique (17, 29) but it does not provide detailed information (11, 30). More recently, techniques such as micro-CT and CBCT have been used. Neelakantan et al. (31) investigated the accuracy of different radiographic techniques for studying root canal morphology. They found a significant difference between all methods except CBCT and the modified canal staining and clearing technique. They concluded that micro-CT and CBCT are as reliable as the clearing technique for identifying root canal systems.
The current study used CBCT imaging methods similar to previously reported studies (22, 32-35). CBCT is a reliable imaging technique because it is nondestructive and provides accurate 3D representations of the external and internal anatomy of the teeth. In addition, the degree of accuracy of CBCT for identifying the complexity of root canal configuration is high (36). CBCT is usually requested when radiographic images yield limited information (37). In the present study, CBCT was able to clearly visualize the roots and root canals.
The prevalence of single-rooted configuration has been reported to reach up to 100% in mandibular first and second premolars (33). In the current study, one root was mostly found in first [181 (73%) out of 245 teeth] and second [183 (79.2%) out of 231 teeth]. This is considered low compared to Llena et al (33) and Alfawaz et al (35) findings. The percentages of two-rooted configuration in the present study was high [61 (24.9%) out of 245 tooth in first] and [48 (20.8%) out of 231 tooth in second] compared to previously reported CBCT studies (33, 34-35, 38). Incidence of three-rooted configuration or more in mandibular premolar teeth is a rare occurrence (33, 35, 39). Few teeth with three roots (0.4%) and four roots (0.2%) were found in the first premolar and none in the second premolar in the present study.
The configuration of root canal systems was categorized according to the Vertucci classification system, which is the most commonly used system in endodontics. All types of Vertucci classifications were seen except Type VIII. Type II was the most common configuration in both the first (17.56%) and second (19.92%) premolars. This was following by type I (14.1%) and type III (14.1%). These findings differ from previous studies where type I was the most prevalent canal configuration in both sets of premolars (20, 22, 32-35, 40). Although CBCT was also used in these studies, the variation in the findings could be attributed to ethnic and racial differences.
Zaatar et al. (17) reported one canal in the mandibular first (85.0%) and second (95.3%) premolars in a Kuwaiti population using conventional radiographs. Furthermore, 15% of the first premolars had a trunk with two separate roots (bifurcated root canals) while only 4.7% of the second premolar had bifurcated roots. Similarly, this study identified one and two roots in both the first and second premolars, while three and four roots were occasionally seen in mandibular first premolars. Similar findings were reported by Cleghorn et al. (7), Celikten et al. (38) and Bürklein et al. (39). Other studies that have used a methodology other than CBCT have reported the presence of two or more root canals in the first and second mandibular premolars as high as 65% and 43%, respectively (12, 14, 20, 41). The differences in our results may be related to the use of CBCT compared conventional radiographs.
A number of root canal configuration types not listed in Vertucci classification was identified in this study. Previous studies have also reported complex canal configurations (13, 42-44). Examples of complex canal configurations identified in this study include 2-3-4-2 and 2-5-4-2-1 (Fig. 5, 6). Some of the samples resemble the supplementary configuration types to Vertucci classification that was reported by Sert and Bayirli (14).
Figure 5.
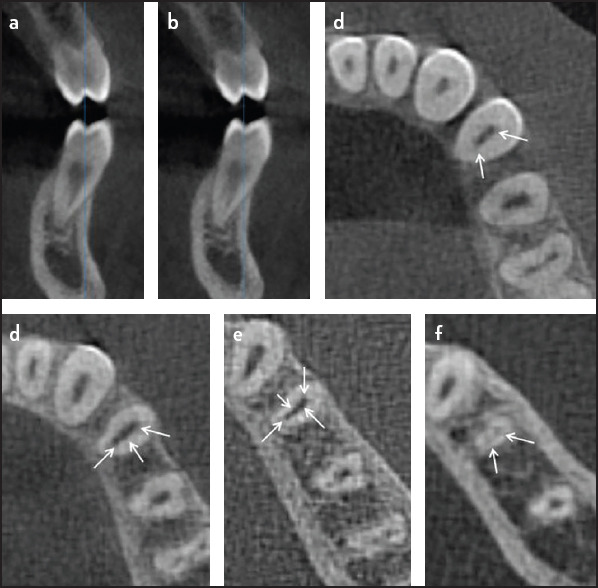
Cross-section CBCT images of mandibular left first premolar showing one root with two canals (a, b). Axial CBCT image at the cervical third showing 2 canals (c), the middle third shows 3 canals (d), close to the apical third showing 4 canals (e) and 2 canals at the apex (f). (Arrows points to the canals). Canal configuration is 2-3-4-2
Figure 6.

Cross-section and axial CBCT images of mandibular right first premolar showing one root with two separated canals at the middle-third (a-d). Axial CBCT image at the middle third level (d) showing 5 canals (e) that was traced with black dots (f) and shown with virtual reconstruction image (g). More towered the apical third 4 canals can be seen (h) and 2 canals at the apex (i). See the radicular groove located at the mesio-lingual area (f). (Arrows points to the canals). Canal configuration is 2-5-4-2
Ahmed et al. (45) introduced a new system for classifying root and root canal morphology. This new coding system can accurately classify the root and canal morphology using any diagnostic tool. Such morphological complex configurations identitied in this study can be classified using Ahmed’s system.
C-shaped root canal is one of the most challenging canals to treat due to its complex system where fin and isthmus are connected. It was classified by Fan et al (10) into five categories. In the present study, C-shaped canal configurations were only detected in mandibular second premolars (1.3%). Their presence was considered minor and they exhibit category III (C3) of Fan et al classification (10). These results are similar to previous reports (22, 32-34) and were higher than that reported by Yu et al. (46) and Martins et al (40).
Alfawaz et al. (35) and Hajihassani et al. (47) did not report C-shaped canals in mandibular premolars in Saudi and Iranian populations, respectfully. By contrast, a higher incidence of C-shaped canals (18%) in the mandibular first premolars has been reported in a Chinese population (11). The differences are likely due to racial characteristics and variation in study design.
The operator should be careful when accessing C-shaped canal. The cavity should be extended toward the buccolingual and/or mesiodistal direction as well as the bifurcation at the middle and apical third in order to find all canals (10, 48).
Mandibular premolar teeth having a high incidence of atypical anatomy (1, 4). In the current study, separate roots in the first (49.1%) and second (34.8%) premolars were more common compared to fused roots. Separated roots can be visualized at different angles on conventional radiographs or through the use of CBCT (49). However, CBCT images can more accurately confirm the exact number of roots and root canals compared to conventional radiographs. The presence of root fusion may be associated with a shallow or deep radicular groove either individually or on both the buccal and lingual aspects of the root (50). The radicular groove is a developmental malformation that extends along the root at varying lengths (50, 51). The ovoid cross-sectional-shaped root normally has grooves or depressions on the mesial and distal surfaces, and the depression on the distal surface is often the deeper of the two (52). In this study, radicular grooves in the first premolars were more often than the second, similar to Arslan et al. (53) and Martins et al (40). In addition, the radicular groove was located more often on the mesial surface of the first premolar (85.2%) and on the distal surface of the second premolar (71.4%, P<0.05). Previous studies have found a correlation between the presence of a C-shaped root canal configuration and the presence of these grooves (10, 53, Martins et al (40). The presence of radicular grooves may be a predisposing factor for advanced periodontal pathology with secondary pulpal involvement (54).
Most of the roots of the mandibular first (71.8%) and second (78.3%) premolars in the current study were straight. However, some distal angulation was identified as well. Similar findings were reported by Hajihassani et al (47).
Wasserstein et al. (55) reported that the majority of the roots in mandibular second premolars are distally curved in panoramic radiographs in the early developmental stage and move to an upright position spontaneously with progressing development. A deviation from an upright tooth germ position may be of genetic origin because distal angulation of the lower second premolars is more pronounced in patients with agenesis of the corresponding antimere (56). The spontaneous repositioning could also be a result of normal changes in tooth position during eruption (57) or it could simply be due to radiographic distortion following positioning errors (58).
Almost all teeth have roots with an angulation at some point along the long axis (59). An abnormal angulation or bend in the root is referred to as dilaceration. The authors observed that root curvature was more prevalent in the first (81.33%) than in the second (78.28%) premolars, with distal curvature being most common in the first premolars, similar to what was previously described in an Iranian population (60). In our study, the curvature angle was more than 20° in the first and the second premolars in 14.90% and 21.26% of the cases, respectively. These results are in accordance with Llena et al. (33) and Willershausen et al. (61). This configuration is important because increased curvature close to the tooth apex increases the difficulty performing the root canal procedure (62).
CONCLUSION
Within the limitations of this study, it can be concluded that cone beam computed tomography is a useful tool for evaluating the configuration of the root canal in the mandibular premolars. The mandibular first and second premolars in Kuwaiti population exhibited great variability in root canal morphology, with Type II Vertucci classification being most common. In addition, greater variation in canal morphology in male patients compared to females was found. The second mandibular premolars showed higher anatomical variability than the first premolars, and both sets of premolars exhibited a variety of morphological root configurations not classified by the Vertucci system.
Footnotes
Conflict of Interest: No conflict of interest.
Ethics Committee Approval: The study was approved by the ethics committee of Riyadh Elm University, College of Dentistry (registration number is FPGRP/43733003/220).
Peer-review: Externally peer-reviewed.
Financial Disclosure: No financial support.
Authorship contributions: Concept – S.A.N., D.J.A.; Design – S.A.N.; Supervision – D.J.A., S.A.N.; Funding - D.J.A., C.S., S.A.N.; Materials - D.J.A.; Data collection &/or processing – D.J.A.; Analysis and/or interpretation – S.A.N., D.J.A., N.A.M., C.S.; Literature search – D.J.A., S.A.N.; Writing – S.A.N.; Critical Review – S.A.N., D.J.A.
REFERENCES
- 1.Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc. 1978;97(1):47–50. doi: 10.14219/jada.archive.1978.0443. [DOI] [PubMed] [Google Scholar]
- 2.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 3.Cantatore G, Berutti E, Castellucci A. Missed anatomy:Frequency and clinical impact. Endod Topics. 2006;15(1):3–31. [Google Scholar]
- 4.Slowey RR. Root canal anatomy. Road map to successful endodontics. Dent Clin North Am. 1979;23(4):555–573. [PubMed] [Google Scholar]
- 5.Lee YY, Yeh PY, Pai SF, Yang SF. Maxillary first molar with six canals. J Dent Sci. 2009;4(4):198–201. [Google Scholar]
- 6.Jha P, Nikhil V, Arora V, Jha M. The root and root canal morphology of the human mandibular premolars:A literature review. J Rest Dent. 2013;1(1):3–10. [Google Scholar]
- 7.Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular first premolar:a literature review. J Endod. 2007;33(5):509–16. doi: 10.1016/j.joen.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 8.Al-Fouzan KS. The microscopic diagnosis and treatment of a mandibular second premolar with four canals. Int Endod J. 2001;34(5):406–10. doi: 10.1046/j.1365-2591.2001.00408.x. [DOI] [PubMed] [Google Scholar]
- 9.Al-Abdulwahhab B, Al-Nazhan S. Root canal treatment of mandibular second premolar with four root canals. Saudi Endod J. 2015;5(3):196–8. [Google Scholar]
- 10.Fan B, Yang J, Gutmann JL, Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I:Microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod. 2008;34(11):1337–41. doi: 10.1016/j.joen.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 11.Lu TY, Yang SF, Pai SF. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod. 2006;32(10):932–6. doi: 10.1016/j.joen.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 12.Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33(1):101–10. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 13.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34(5):359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 14.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 15.Kim E, Fallahrastegar A, Hur YY, Jung IY, Kim S, Lee SJ. Difference in root canal length between Asians and Caucasians. Int Endod J. 2005;38(3):149–51. doi: 10.1111/j.1365-2591.2004.00881.x. [DOI] [PubMed] [Google Scholar]
- 16.Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of Jordanian maxillary first premolars. J Endod. 2008;34(8):956–61. doi: 10.1016/j.joen.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 17.Zaatar EI, al-Kandari AM, Alhomaidah S, al-Yasin IM. Frequency of endodontic treatment in Kuwait:radiographic evaluation of 846 endodontically treated teeth. J Endod. 1997;23(7):453–6. doi: 10.1016/s0099-2399(97)80302-0. [DOI] [PubMed] [Google Scholar]
- 18.Zaatar EI, al Anizi SA, al Duwairi Y. A study of the dental pulp cavity of mandibular first permanent molars in the Kuwaiti population. J Endod. 1998;24(2):125–7. doi: 10.1016/S0099-2399(98)80092-7. [DOI] [PubMed] [Google Scholar]
- 19.Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population-a clinical study. Int Endod J. 2008;41(9):755–62. doi: 10.1111/j.1365-2591.2008.01427.x. [DOI] [PubMed] [Google Scholar]
- 20.Chourasia HR, Boreak N, Tarrosh MY, Mashyakhy M. Root canal morphology of mandibular first premolars in Saudi Arabian southern region subpopulation. Saudi Endod J. 2017;7(2):77–81. [Google Scholar]
- 21.Boschetti E, Silva-Sousa YTC, Mazzi-Chaves JF, Leoni GB, Versiani MA, Pécora JD, et al. Micro-CT Evaluation of Root and Canal Morphology of Mandibular First Premolars with Radicular Grooves. Braz Dent J. 2017;28(5):597–603. doi: 10.1590/0103-6440201601784. [DOI] [PubMed] [Google Scholar]
- 22.Ok E, Altunsoy M, Nur BG, Aglarci OS, Çolak M, Güngör E. A cone-beam computed tomography study of root canal morphology of maxillary and mandibular premolars in a Turkish population. Acta Odontol Scand. 2014;72(8):701–6. doi: 10.3109/00016357.2014.898091. [DOI] [PubMed] [Google Scholar]
- 23.Hashimoto K, Kawashima S, Kameoka S, Akiyama Y, Honjoya T, Ejima K, et al. Comparison of image validity between cone beam computed tomography for dental use and multidetector row helical computed tomography. Dentomaxillofac Radiol. 2007;36(8):465–71. doi: 10.1259/dmfr/22818643. [DOI] [PubMed] [Google Scholar]
- 24.Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32(2):271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 25.Nelson SJ. Wheeler's dental anatomy physiology and occlusion. 10th ed. Elsevier Health Sciences; 2014. [Google Scholar]
- 26.Peiris R. Root and canal morphology of human permanent teeth in a Sri Lankan and Japanese population. Anthropological Science. 2008;116(2):123–33. [Google Scholar]
- 27.Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31(2):180–91. doi: 10.1002/nur.20247. [DOI] [PubMed] [Google Scholar]
- 28.Isaac S, Michael WB. Handbook in research and evaluation. San Diego, CA: Educational and Industrial Testing Services; 1995. p. 101. [Google Scholar]
- 29.Yoshioka T, Villegas JC, Kobayashi C, Suda H. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod. 2004;30(2):73–4. doi: 10.1097/00004770-200402000-00002. [DOI] [PubMed] [Google Scholar]
- 30.Omer OE, Al Shalabi RM, Jennings M, Glennon J, Claffey NM. A comparison between clearing and radiographic techniques in the study of the root-canal anatomy of maxillary first and second molars. Int Endod J. 2004;37(5):291–6. doi: 10.1111/j.0143-2885.2004.00731.x. [DOI] [PubMed] [Google Scholar]
- 31.Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique cone-beam computed tomography peripheral quantitative computed tomography spiral computed tomography and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod. 2010;36(9):1547–51. doi: 10.1016/j.joen.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 32.Liao Q, Han JL, Xu X. Analysis of canal morphology of mandibular first premolar [Article in Chinese] Shanghai Kou Qiang Yi Xue. 2011;20(5):517–21. [PubMed] [Google Scholar]
- 33.Llena C, Fernandez J, Ortolani PS, Forner L. Cone-beam computed tomography analysis of root and canal morphology of mandibular premolars in a Spanish population. Imaging Sci Dent. 2014;44(3):221–7. doi: 10.5624/isd.2014.44.3.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Shetty A, Hegde MN, Tahiliani D, Shetty H, Bhat GT, Shetty S. A three-dimensional study of variations in root canal morphology using cone-beam computed tomography of mandibular premolars in a South Indian population. J Clin Diagn Res. 2014;8(8):ZC22–4. doi: 10.7860/JCDR/2014/8674.4707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Alfawaz H, Alqedairi A, Al-Dahman YH, Al-Jebaly AS, Alnassar FA, Alsubait S, et al. Evaluation of root canal morphology of mandibular premolars in a Saudi population using cone beam computed tomography:A retrospective study. Saudi Dent J. 2019;31(1):137–42. doi: 10.1016/j.sdentj.2018.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sousa TO, Haiter-Neto F, Nascimento EHL, Peroni LV, Freitas DQ, Hassan B. Diagnostic Accuracy of Periapical Radiography and Cone-beam Computed Tomography in Identifying Root Canal Configuration of Human Premolars. J Endod. 2017;43(7):1176–9. doi: 10.1016/j.joen.2017.02.021. [DOI] [PubMed] [Google Scholar]
- 37.Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in Endodontics - a review. Int Endod J. 2015;48(1):3–15. doi: 10.1111/iej.12270. [DOI] [PubMed] [Google Scholar]
- 38.Celikten B, Orhan K, Aksoy U, Tufenkci P, Kalender A, Basmaci F, et al. Cone-beam CT evaluation of root canal morphology of maxillary and mandibular premolars in a Turkish Cypriot population. BDJ Open. 2016;2:15006. doi: 10.1038/bdjopen.2015.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bürklein S, Heck R, Schäfer E. Evaluation of the Root Canal Anatomy of Maxillary and Mandibular Premolars in a Selected German Population Using Cone-beam Computed Tomographic Data. J Endod. 2017;43(9):1448–52. doi: 10.1016/j.joen.2017.03.044. [DOI] [PubMed] [Google Scholar]
- 40.Martins JNR, Francisco H, Ordinola-Zapata R. Prevalence of C-shaped Configurations in the Mandibular First and Second Premolars:A Cone-beam Computed Tomographic In Vivo Study. J Endod. 2017;43(6):890–5. doi: 10.1016/j.joen.2017.01.008. [DOI] [PubMed] [Google Scholar]
- 41.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3–29. [Google Scholar]
- 42.Kartal N, Yanikoğlu FC. Root canal morphology of mandibular incisors. J Endod. 1992;18(11):562–4. doi: 10.1016/S0099-2399(06)81215-X. [DOI] [PubMed] [Google Scholar]
- 43.Peiris HR, Pitakotuwage TN, Takahashi M, Sasaki K, Kanazawa E. Root canal morphology of mandibular permanent molars at different ages. Int Endod J. 2008;41(10):828–35. doi: 10.1111/j.1365-2591.2008.01428.x. [DOI] [PubMed] [Google Scholar]
- 44.Al-Qudah AA, Awawdeh LA. Root and canal morphology of mandibular first and second molar teeth in a Jordanian population. Int Endod J. 2009;42(9):775–84. doi: 10.1111/j.1365-2591.2009.01578.x. [DOI] [PubMed] [Google Scholar]
- 45.Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–70. doi: 10.1111/iej.12685. [DOI] [PubMed] [Google Scholar]
- 46.Yu X, Guo B, Li KZ, Zhang R, Tian YY, Wang H, et al. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med Imaging. 2012;12:18. doi: 10.1186/1471-2342-12-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hajihassani N, Roohi N, Madadi K, Bakhshi M, Tofangchiha M. Evaluation of Root Canal Morphology of Mandibular First and Second Premolars Using Cone Beam Computed Tomography in a Defined Group of Dental Patients in Iran. Scientifica (Cairo) 2017;2017:1504341. doi: 10.1155/2017/1504341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gu YC, Zhang YP, Liao ZG, Fei XD. A micro-computed tomographic analysis of wall thickness of C-shaped canals in mandibular first premolars. J Endod. 2013;39(8):973–6. doi: 10.1016/j.joen.2013.04.039. [DOI] [PubMed] [Google Scholar]
- 49.Reddy SJ, Chandra PV, Santoshi L, Reddy GV. Endodontic management of two-rooted mandibular premolars using spiral computed tomography:a report of two cases. J Contemp Dent Pract. 2012;13(6):908–13. doi: 10.5005/jp-journals-10024-1252. [DOI] [PubMed] [Google Scholar]
- 50.Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z. C-shaped canal system in mandibular second molars:Part I--Anatomical features. J Endod. 2004;30(12):899–903. doi: 10.1097/01.don.0000136207.12204.e4. [DOI] [PubMed] [Google Scholar]
- 51.Kotoku K. Morphological studies on the roots of Japanese mandibular second molars [Article in Japanese] Shikwa Gakuho. 1985;85(1):43–64. [PubMed] [Google Scholar]
- 52.Woelfel J, Scheid R. Dental anatomy:its relevance to dentistry. 6th ed. Philadelphia: Lippincott Williams &Wilkins; 2002. [Google Scholar]
- 53.Arslan H, Capar ID, Ertas ET, Ertas H, Akcay M. A cone-beam computed tomographic study of root canal systems in mandibular premolars in a Turkish population:Theoretical model for determining orifice shape. Eur J Dent. 2015;9(1):11–9. doi: 10.4103/1305-7456.149632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lee KW, Lee EC, Poon KY. Palato-gingival grooves in maxillary incisors. A possible predisposing factor to localised periodontal disease. Br Dent J. 1968;124(1):14–8. [PubMed] [Google Scholar]
- 55.Wasserstein A, Brezniak N, Shalish M, Heller M, Rakocz M. Angular changes and their rates in concurrence to developmental stages of the mandibular second premolar. Angle Orthod. 2004;74(3):332–6. doi: 10.1043/0003-3219(2004)074<0332:ACATRI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 56.Shalish M, Peck S, Wasserstein A, Peck L. Malposition of unerupted mandibular second premolar associated with agenesis of its antimere. Am J Orthod Dentofacial Orthop. 2002;121(1):53–6. doi: 10.1067/mod.2002.120399. [DOI] [PubMed] [Google Scholar]
- 57.Van der Linden FPGM, Duterloo HS. Development of the Human Dentition:An Atlas. Hagerstown: Harper &Row; 1976. pp. 204–5. [Google Scholar]
- 58.Mckee IW, Glover KE, Williamson PC, Lam EW, Heo G, Major PW. The effect of vertical and horizontal head positioning in panoramic radiography on mesiodistal tooth angulations. Angle Orthod. 2001;71(6):442–51. doi: 10.1043/0003-3219(2001)071<0442:TEOVAH>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 59.Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular second premolar:a literature review. J Endod. 2007;33(9):1031–7. doi: 10.1016/j.joen.2007.03.020. [DOI] [PubMed] [Google Scholar]
- 60.Khedmat S, Assadian H, Saravani AA. Root canal morphology of the mandibular first premolars in an Iranian population using cross-sections and radiography. J Endod. 2010;36(2):214–7. doi: 10.1016/j.joen.2009.10.002. [DOI] [PubMed] [Google Scholar]
- 61.Willershausen B, Kasaj A, Röhrig B, Briseño B. The determination of the initial straight length in root canals of mandibular premolars--an in vitro study. Eur J Med Res. 2009;14(2):85–9. doi: 10.1186/2047-783X-14-2-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lombart B, Michonneau JC. -Premolar anatomy and endodontic treatment. Rev Belge Med Dent. 2005;60(4):322–36. [PubMed] [Google Scholar]