

Abstract
Objective:
Consistent reporting of publications in a given topic is essential. This systematic review aimed to identify and evaluate the reporting items in previous publications related to root canal anatomy in major Endodontic journals.
Methods:
A systematic review was undertaken following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was performed by 2 independent reviewers using a customized search strategy in major Endodontic journals through Scopus until November 2019. Studies investigating root and canal anatomy were included. The selected publications were divided into 7 categories according to the study design: micro-computed tomography (microCT) and cone-beam computed tomography (CBCT) experimental studies (extracted teeth), CBCT and 2D clinical studies, CBCT and 2D case reports in addition to others (i.e. staining and clearing method and root sectioning). The selected studies were evaluated according to three domains: 1) Criteria for study sample selection; 2) Criteria for methodological procedures and 3) Criteria for detection and evaluation.
Results:
After the removal of duplicated and irrelevant papers, 137 articles were included. Results showed that microCT studies reported accurately the tooth type, number of teeth, classifications used, qualitative and/or quantitative analysis (if required) and the evaluation process. However, sample size calculation, calibration, and reproducibility were not reported in the majority of microCT studies. CBCT clinical studies presented information for the type of study, inclusion/exclusion criteria, number of patients, tooth type, and number of teeth. However, the majority did not report sample size calculation and calibration of examiners. Radiographic exposure descriptions and classifications used were not reported adequately in CBCT and 2D case reports. Sample size calculation, calibration and reproducibility were not reported in staining and clearing method.
Conclusion:
Despite accurate presentation of certain items, there is considerable inconsistent reporting of root and canal morphology regardless of the type of study and experimental procedure used. The PROUD checklist protocol presented in this systematic review aims to provide an accurate description of root canal anatomy in experimental, clinical, and case report publications.
Keywords: Morphology, protocol, reporting items, root canal anatomy, systematic review
HIGHLIGHTS.
This systematic review aimed to identify and evaluate the reporting items in previous publications related to root canal anatomy.
Results showed that there is considerable inconsistent reporting of root and canal morphology regardless of the type of study and experimental procedure used.
The PROUD checklist protocol presented in this systematic review paves the way for an accurate description of root canal anatomy in experimental, clinical, and case report publications.
INTRODUCTION
Effective root canal treatment requires a thorough knowledge of root canal anatomy (1). In the human dentition, a wide range of anatomical variations in each tooth type has been reported (1-4). For many decades, this topic has been the subject of numerous experimental reports in extracted teeth using different methodological procedures such as staining and clearing, 2D radiographic imaging, together with recent 3D technological advances including cone-beam computed tomography (CBCT) and micro-computed tomography (microCT), and others (4-9). This is in addition to CBCT clinical studies on different population groups, and 2D clinical studies as well as case reports that usually present anatomical variations and their detection methods using different imaging techniques, magnification, and other technical intra-operative procedures (2, 10-13).
Discrepancies and inconsistent reporting in studies may undermine the validity of the scientific effort, produce unfounded conclusions, and lead to the unnecessary repetition of studies with identical objectives (14). Current knowledge of root and canal morphology is based on research findings, clinical studies, and individual case reports (1, 4, 15). An accurate, consistent reporting of such information is essential. This would provide transparency in presenting a given data, facilitate accurate comparisons between different studies, facilitate the combination of quantitative and qualitative results from previous studies and present a high-quality reference to researchers and clinicians guiding them to build up high-quality research and satisfactory standards of clinical care, respectively.
Unfortunately, there is a lack of evidence for the level of consistent reporting in publications related to root and canal anatomy. This systematic review aimed to (1) extract and evaluate the reporting items related to root and canal anatomy in experimental and clinical studies as well as case reports published in major Endodontic journals; (2) introduce a protocol for consistent reporting of root and canal anatomy which can be applied in experimental and clinical studies and case reports.
MATERIALS AND METHODS
The current systematic review was prepared following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (16).
Literature search methodology
An electronic search was performed in the Scopus database (www-scopus-com). The following keywords were used – “root canal morphology” OR “root canal anatomy” OR “root canal configuration” OR “accessory canals” till November 2019. The search in Scopus was limited to four endodontic journals - Journal of Endodontics, International Endodontic Journal, Australian Endodontic Journal, and Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology (until 2011) and previous names of this journal.
Inclusion and exclusion criteria
a) Root canal anatomy:
Studies investigating root and canal anatomical variations in the human permanent dentition such as the number of roots, root canal configurations, morphology of the canal isthmuses, and accessory canals were included. Main classifications for root and canal anomalies such as radix entomolaris, C-shaped canals, dens invaginatus, palato-gingival grooves, taurodontism were included. The methods of detection, description, and classifications of root canal anatomy were recorded. The treatment procedures proposed for such anatomical variations were excluded.
b) Publication type:
Experimental and clinical studies as well as case reports were included in this systematic review. Case report publications having literature reviews were included. Literature reviews, editorials, and other publication types were excluded. Studies comparing different methodological procedures to assess root canal morphology were also excluded.
c) Experimental methods:
(i)Experimental studies related to microCT were included.
(ii)Experimental and clinical studies as well as case reports related to CBCT were included. Spiral computed tomography reports were excluded.
(iii)For 2D radiographic imaging, clinical studies were included, and for case reports, the most cited 10 publications and all reports published since 2010 were included.
(iv)For staining and clearing techniques (and others if applicable), all studies that were used as a reference to classify root canal morphology in the CBCT and microCT studies fitting the criteria of this systematic review were included.
Data extraction and analysis procedures
Phase 1:
Using the above-mentioned literature search methodology and inclusion criteria, the titles and abstracts were screened by 2 independent reviewers to identify the publications after duplicates removal. Using online kappa calculator (https://idostatistics.com/cohen-kappa-free-calculator/#risultati), the Cohen’s kappa analysis was calculated, and the level of agreement was determined.
Phase 2:
The selected studies were read in full text, and reviewed by the 2 independent reviewers, and a discussion was undertaken for the selection and collection of reporting items for each of the following categories:
a) Research studies:
These included (i) studies investigating root canal anatomy in “extracted teeth” using 3D methods (microCT and CBCT), in addition to other methods (such as staining and clearing) as mentioned in the inclusion criteria; (ii) studies investigating root canal anatomy in patients/population groups using CBCT or 2D radiographic imaging.
This category was divided into 3 domains:
Domain A: Study design and sampling method:
This domain included the type of study (e.g. experimental, clinical, ethical approval, a priori sample size calculation, population/ethnic group, tooth type, number of teeth, number, gender and age of patients (or donors/owners, if applicable), inclusion/exclusion criteria. The latter criteria were scored as present if the authors mentioned accurate details for the included samples (e.g. the presence of caries, root canal fillings, restorations, resorption defects, mature roots).
Domain B: Experimental/diagnostic procedures:
This domain included the details of the experimental method including the type of radiographic machine/scanner and specifications/settings [such as kilovoltage (Kv), milliamperage (mA), voxel size and field of view (FOV) (if applicable)]. If 2D radiographic imaging was used, details on angulation techniques (perpendicular to the horizontal plane, mesial, distal shift angulations) and image processing (digital or manual) were evaluated. Magnification, modified access cavities, exploration, negotiation with and without troughing were included in instances of studies that examined the detection of canals. Experimental procedures for staining and clearing were also evaluated.
Domain C: Evaluation process:
This domain included details for the evaluation objectives and methods used such as qualitative (e.g. root and canal configurations, presence/absence of C-shaped canals) and/or quantitative analysis (e.g. canal volume, thickness, distance between canal orifices), how the evaluation process was performed and software used. In addition, calibration, reproducibility of observers (e.g. Kappa score), classifications used for identification and statistical analysis were also evaluated.
b) Case reports:
These included CBCT and 2D radiographic case reports (or series).
This category was divided into 3 domains:
Domain A: Case description details
This domain included the population/ethnic group, tooth type, number of teeth, age, and gender of patients.
Domain B: Diagnostic procedures:
This domain included the details of radiographic machine/scanner and settings (such as Kv, mA and voxel size if applicable) and field of view (if applicable), in addition to other clinical procedures used for detection of canals such as magnification, modified access cavities, exploration, negotiation with and without troughing.
Domain C: Evaluation process:
This domain included the narrative details for the evaluation objectives and methods used such as qualitative and/or quantitative analysis, how the evaluation process was performed using the software, and classification used for identification.
Phase 3:
Each of the assessed items was dichotomized as present or absent by the authors. For calibration, the two independent reviewers have undertaken a pilot study in which 20 selected publications were analyzed in an Excel spreadsheet. Disagreements between reviewers were discussed until a decision was obtained by consensus.
Phase 4:
The two independent reviewers analyzed the included publications in each category, and a Cohen’s kappa analysis (https://idostatistics.com/cohen-kappa-free-calculator/#risultati) was calculated for each category. Disagreements between reviewers were discussed via emails, and discussion calls were considered, if needed, until a decision was reached by consensus.
Phase 5:
After data analysis and synthesis, a checklist protocol was developed for each of research and case report categories.
RESULTS
The search strategy results are presented in Figure 1. A total of 138 studies were included in this systematic review [37 microCT studies (17-53), 4 CBCT experimental studies (9, 54-56), 38 CBCT clinical studies (2, 10, 57-92), 10 2D clinical studies (11, 93-101), 12 staining and clearing and root sectional studies (including one study for tooth sectioning) (7, 102-112), 14 CBCT case reports (12, 113-125) and 22 2D case reports (13, 126-146)]. For phase 1, the agreement between reviewers was 90.05% (Cohen’s k=0.76 – substantial agreement). Table 1 shows Cohen’s kappa analysis for research studies and case reports.
Figure 1.
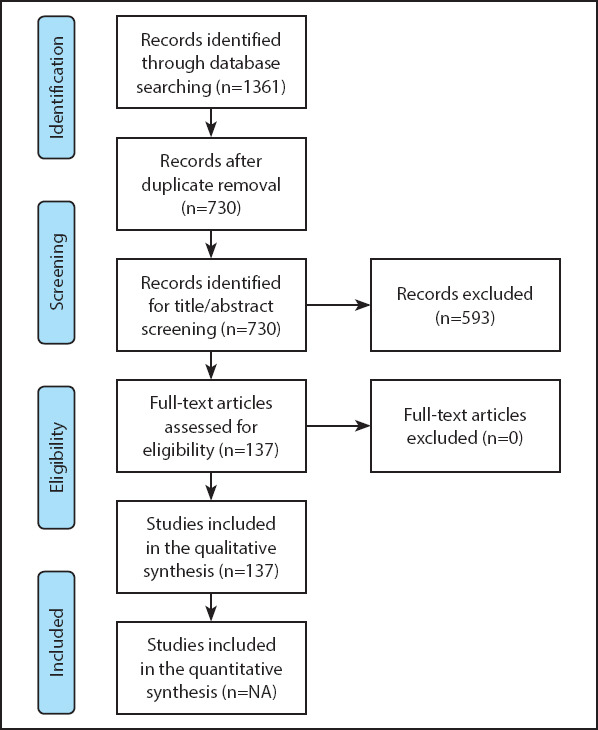
PRISMA flowshart of this systematic review
TABLE 1.
Cohen’s kappa analysis for all study categories included in this systematic review
| Categories | Number of publications included | Agreement percentage bet. reviewers | Cohen’s kappa | Level of agreement |
|---|---|---|---|---|
| MicroCT studies | 37 | 89.61% | 0.79 | Substantial |
| CBCT experimental studies | 4 | 86.1% | 0.67 | Substantial |
| CBCT clinical studies | 38 | 90.7% | 0.75 | Substantial |
| 2D clinical studies | 10 | 88.84% | 0.77 | Substantial |
| Staining and clearing studies | 12 | 98.0% | 0.96 | Almost perfect |
| CBCT case reports | 14 | 96.3% | 0.92 | Almost perfect |
| 2D case reports | 22 | 91.6% | 0.83 | Almost perfect |
| Total/mean | 137 | 91.59% | 0.81 | Almost perfect |
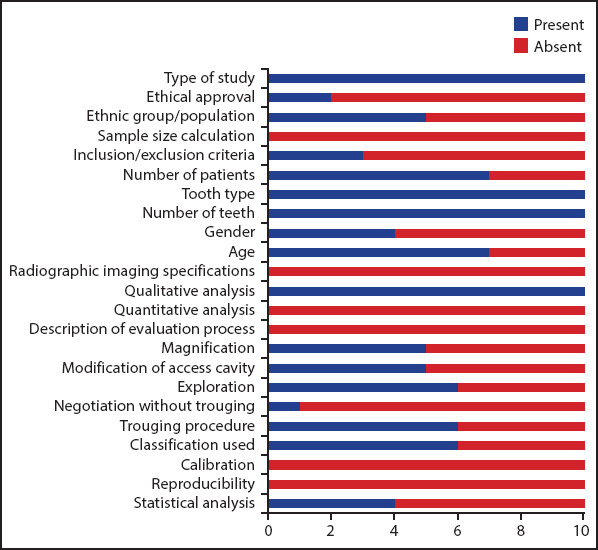
Results showed that all microCT studies presented the type of study, tooth type, number of teeth, and classifications used. The majority of studies described qualitative and/or quantitative analysis (if required) and the evaluation process (Fig. 2). However, a priori sample size calculation was not mentioned in any of the studies. Information related to age and gender of tooth donors/owners was not provided in the majority of studies; as often this information was not available since the teeth were extracted previously due to reasons not related to the studies. Only two studies provided details for calibration (21, 38), and none for reproducibility test. Four studies mentioned agreement consensus between examiners (21, 32, 35, 41).
Figure 2.
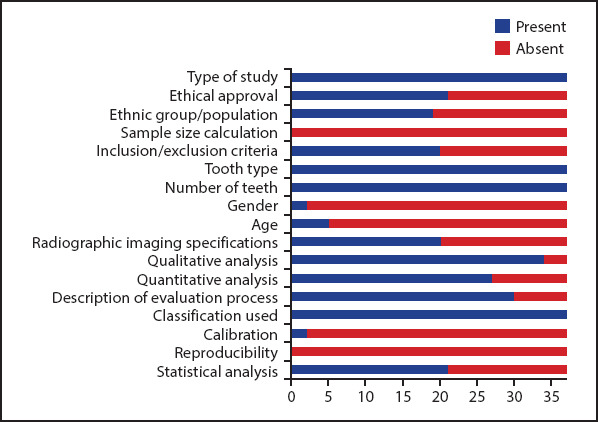
Bar chart for reporting items related to microCT studies
About half of the included studies did not provide information regarding ethical approval (19, 23, 25, 28, 30, 32-35, 37, 40, 43, 46, 51-53), or related ethnic group/population (18, 20, 22, 28-31, 35-38, 41, 42, 45-47, 50, 51), or complete description of imaging settings (machine brand, Kv, mA, voxel size) (19, 20, 28-30, 32, 35-38, 40, 41, 45, 47, 51-53). The inclusion and exclusion criteria were not mentioned in 4 studies (19, 28, 49, 53), and were considered incomplete in 13 studies (26, 29, 31, 37, 38, 40, 44-48, 51, 52). Less than half of the studies did not perform statistical analysis.
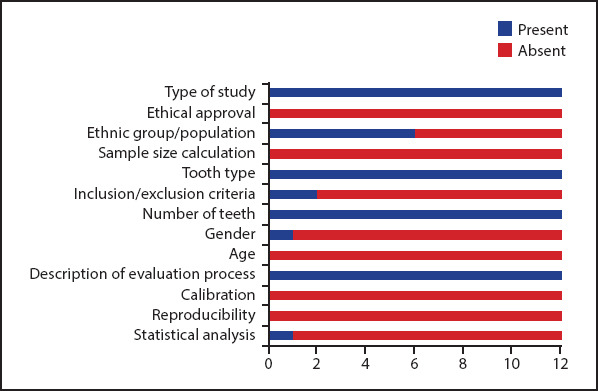
For CBCT experimental studies in extracted teeth, similar to microCT studies, all investigations included information related to the type of study, tooth type, tooth number and description of evaluation process, but none of the studies provided details regarding sample size calculation. Only one study provided information for ethical approval (55), and the calibration of examiners (56). One study did not mention the inclusion/exclusion criteria (54). Agreement between observers was performed in 3 studies (54-56). Two out of 4 studies provided information related to scanner type and imaging settings used (Kv, mA, voxel size and FOV) (9, 56). Similar to microCT studies, information related to age and gender of the teeth donors/owners was not provided in any study (Fig. 3).
Figure 3.
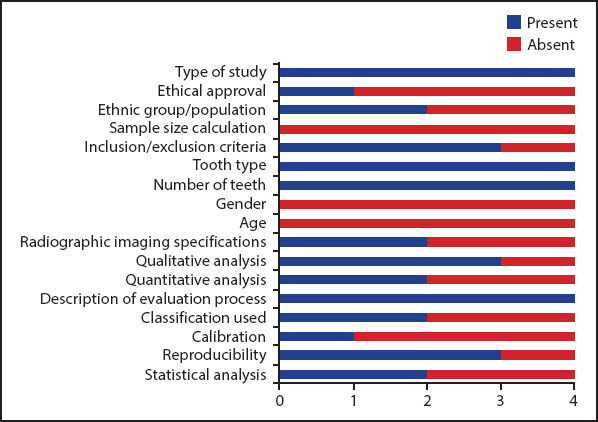
Bar chart for reporting items related to CBCT experimental studies
For CBCT clinical publications, results showed that all studies presented information for the type of study, inclusion/exclusion criteria, number of patients, tooth type, and number of teeth (Fig. 4). Few studies did not provide details on ethical approval (61, 64, 66, 75, 84, 85), ethnic group/population (78, 88-90) and gender (71, 79, 80, 89).
Figure 4.
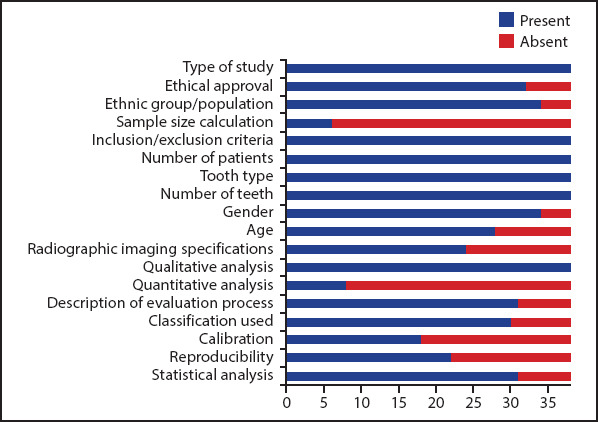
Bar chart for reporting items related to CBCT clinical studies
A number of CBCT clinical studies did not provide complete information on radiographic imaging specifications (machine, Kv, mA, voxel size and FOV) (10, 59, 60, 64, 66, 71, 74, 75, 79, 80, 84, 85, 87, 89), morphology classifications used (57, 59, 67, 78, 85, 88, 89, 91), and statistical analyses (68, 72, 75, 77, 82, 83, 85) (Fig. 4). More than half of the studies did not provide details on the calibration of examiners (2, 10, 57, 60, 61, 66, 71, 73-76, 78-83, 86, 88, 89), and 42% did not provide details for the analysis of agreement between observers (or same operator after a given time) assessment. While few studies did not mention details on the agreement per se (10, 58, 75, 86, 89), some studies mentioned different ways for reporting agreement (without analysis) either by consensus reached between examiners (64, 66, 67, 72, 76, 77, 81-83), or were resolved by a third reviewer (63, 71, 74, 79, 80, 91, 92). Only 6 out of 38 studies (16%) reported sample size calculation (57, 59, 64, 67, 78, 91).
For 2D clinical studies, results showed that included studies presented the type of study, tooth type, the number of teeth and qualitative analysis of radiographic images (Fig. 5). None of the studies provided information regarding sample size calculation or complete information on radiographic imaging specifications (machine, Kv, mA, angulation technique and processing). Five studies provided details on the angulation used for imaging (11, 93, 95, 99, 101). Ethical approval was mentioned in only 2 studies (11, 95), whereas 5 studies provided information regarding the ethnic group/population assessed (11, 93, 95, 96, 100). The majority provided information for age (11, 93, 95, 98-101), and less than half mentioned details on gender of the patients/subjects (93, 95, 99, 100).
Figure 5.
Bar chart for reporting items related to 2D clinical studies
Results showed that half of the 2D clinical studies reported the use of magnification for detection of canals (11, 94-96, 99). Clinical procedures performed to detect canals were mentioned in details, and varied based according to the aim of the study including modification of the access cavity (11, 93, 94, 99, 100), exploration (mainly using DG16) (11, 93-95, 98, 99), negotiation with hand files without troughing (95) or negotiation with troughing using ultrasonic tips or long shank round burs (11, 93, 94, 96, 98, 99) (Fig. 5). The root canals were either described based on a given classification such as Weine’s classification, (11, 93, 97-99) or without (94-96, 100, 101).
2D clinical studies reported a wide variations for the operators performing the clinical procedures; a single operator treated the cases in four studies (11, 94, 100, 101), two endodontists in two studies (93, 99), postgraduate students in one study (96) and three operators in another study (97), whereas this information was unclear in two studies (95, 98). No information was provided in any study with regards to calibration of operators. Only one study (93) provided details with regards to the number of years of experience of each operator. Reproducibility was not applicable since the treatment is carried out once.
Notably, two 2D clinical studies (147, 148) were not included in the bar chart since they evaluated the root and canal morphology using 2D radiographic imaging with different angles in the absence of clinical intervention.
For other type of studies, results showed that staining and clearing and root sectioning publications did not provide details for ethical approval, sample size calculation, calibration or reproducibility (Fig. 6). About half of the studies provided details on ethnic groups/populations. Only two out of 11 studies listed the inclusion and exclusion criteria (111, 112). Only 1 study provided details on gender of the teeth donors/owners (103), and reported statistical analysis (110). Similarly, Weine’s study (107), which was a sectioning experimental study performed on the mesiobuccal roots of extracted maxillary molars, did not perform sample size calculation, calibration and reproducibility, and did not mention inclusion/exclusion criteria (Fig. 6).
Figure 6.
Bar chart for reporting items related to classifications used staining and clearing
*Weine’s classification (107) is included in this chart (sectioning in extracted teeth)
For case reports, results showed that all CBCT publications presented age and gender of patients, tooth type, and number of teeth. Three reports mentioned the ethnic group/population of the patients (115, 116, 119). In general, complete details for radiographic imaging specifications (Kv, mA, voxel size, FOV) were not provided in any report. However, incomplete information was provided in some reports; twelve reports mentioned details on machine type (12, 113-117, 119, 121-125), 7 reports for Kv and mA (12, 116, 117, 119, 121, 122, 124), and none for FOV. All reports provided details for qualitative analysis (mainly root and canal configuration). Quantitative measurements were performed in one report (114). Description of the evaluation process was performed in 3 reports (116, 117, 119). Magnification was used in the majority of reports. The clinical procedures performed to detect canals were described in details, and varied based on the aim of the study (i.e. detection of canal orifices or apical canal bifurcations) (Fig. 7). Six reports provided details on the classification used (12, 115, 119, 123-125).
Figure 7.
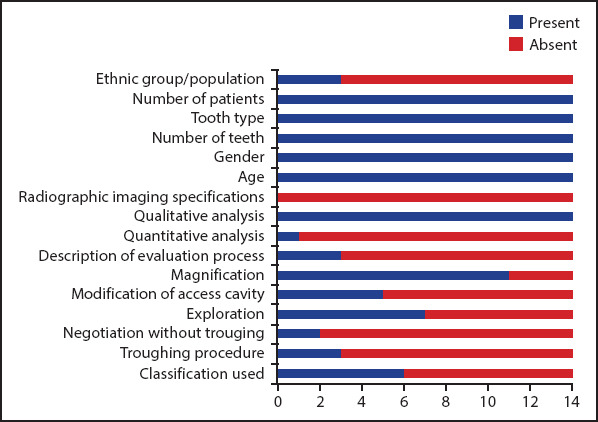
Bar chart for reporting items related to CBCT case reports
For 2D case reports, almost all publications presented information for the number, age, and gender of patients, tooth type, number of teeth and qualitative analysis of the radiographic views. Seven out of 22 reports mentioned the ethnic group/population of the patients (126, 127, 130, 131, 141, 143, 144). None of the reports provided complete information for radiographic imaging specifications (Kv, mA, angulations) or quantitative analysis or description of the evaluation process. Three reports provided information on the radiographic angulations used (126, 127, 139). Nine reports provided details on the configuration classification used (13, 126, 128, 132, 133, 135, 138, 144, 146). Magnification was used in 14 publications (13, 126-129, 132-136, 143-146). Clinical procedures performed to detect canals were often mentioned explicitly, and varied based on the aim of the study (i.e. detection of canal orifices or apical canal bifurcations) (Fig. 8).
Figure 8.

Bar chart for reporting items related to 2D case reports
DISCUSSION
Consistent reporting is an essential requirement in scientific publications (14). This systematic review aimed to evaluate the level of consistency for listing the reporting items related to root and canal anatomy publications. In general, for studies, results showed that despite the included publications provided accurate details on items related to the study type, tooth type, number of patients and teeth, there are obvious deficiencies to describe sample size calculations, calibration, reproducibility, inclusion/exclusion criteria, and ethnic groups/population. On the other hand, radiographic imaging specifications, technique, and processing together with describing the anatomy using a given classification were the main deficiencies for case reports.
Literature shows that different ethnic groups may show different root canal anatomical variations in the human dentition (4, 59). Except for CBCT clinical studies, this systematic review showed that more than half of the studies included, as well as case reports, did not mention the ethnic group or population of the examined teeth. One possible explanation that many countries, nowadays, are often populated by multiple ethnic groups; it seems complicated to accurately identify the origin of the study samples, especially if the study was performed on teeth extracted for reasons not related to that particular study. Furthermore, one country may have cities with various ethnic groups. Nevertheless, it is essential for authors to describe the nature of the ethnic group/population where the teeth were extracted (or the patients included). This would provide a consistent database source for future studies and systematic reviews to compare and propose valid conclusions.
Sample size calculation is usually performed at the time of planning a given study, and it varies according to the type of research question and study design. Whatever be the aim, if a hypothesis is being tested, sound conclusions can be drawn only with an appropriate sample size (149). Very often, a limited sample size is decided arbitrarily based on the researchers’ convenience, available time, and resources, resulting in potentially misleading findings due to an insufficient number of subjects studied (149). A very large sample size is also not recommended since it is a waste of available resources if an answer can be accurately achieved with a smaller sample, as long as there is sufficient power in the test (149).
Results of this systematic review showed that the sample size calculation was not reported in any of the microCT studies, experimental CBCT studies or staining and clearing studies. Only 6 out of 38 CBCT clinical studies reported sample size calculations (57, 59, 64, 67, 78, 91). It is well-known that microCT scanning of extracted teeth is an expensive procedure, and it requires a long time for scanning followed by sophisticated qualitative and quantitative analysis. However, reporting the sample size calculation is still essential to confirm that the results represent a given population of a particular tooth type. Similarly, a recent systematic review discussed microCT studies on rodent jawbone micro-architecture (150), and reported that none of the 46 included microCT studies performed sample size calculation, which was considered as one deficiency (150). Despite that ethical approval does not has an impact on root canal identification, it was included it in this systematic review because in addition to its legal and moral relevance, it may give a clue to other related items such as sample size calculation which is usually documented in ethical approval applications. Except for CBCT clinical studies, the majority of experimental investigations and 2D clinical studies did not mention information on ethical approval, which is considered as another deficiency in reporting.
Establishing inclusion and exclusion criteria is required when designing high-quality research protocols. Except for CBCT clinical studies, this systematic review showed that more than half of the studies did not provide accurate, detailed inclusion/exclusion criteria for the study samples. Few studies did not provide any details, and some provided incomplete criteria. For example, some studies mentioned the selection of teeth with a definite number of roots (some mentioned with fully formed apices and others did not) but with no details on the presence/absence of carious lesions, resorption defects, restorations, root canal fillings and others (26, 44, 45, 47). Notably, applying strict inclusion/exclusion criteria for selection of teeth with rare anatomical variations (such as three rooted maxillary premolars and maxillary incisors with palato-gingival grooves) could be challenging. However, it is important for authors to provide a detailed description of such criteria to ensure that the teeth were selected correctly with no confounding factors that may alter the anatomical features of the crown and/or root canal space.
Literature shows that ethnic groups/population, age and gender (with lesser extent) play a role in root canal anatomical variations (60, 61, 151). Except for CBCT clinical studies and case reports (CBCT and 2D), results showed that these items were rarely or less commonly reported in microCT, experimental CBCT and staining and clearing studies as well as 2D clinical studies. Listing such details is beneficial for accurate comparisons between study findings and providing valid explanations for potential differences; however, obtaining such information for extracted teeth is challenging since they are usually collected from hospitals and dental clinics, and patients’ details are usually unavailable.
Radiographic imaging specifications for both 2D and 3D imaging procedures, in addition to the software used for qualitative and quantitative analysis may influence the image quality and interpretation of canal anatomy (152, 153). This systematic review showed insufficient reporting of radiographic imaging specifications in all diagnostic methods, especially 2D clinical studies, CBCT and 2D case reports (Figs. 2-5, 7, 8). With the exception of CBCT and 2D clinical studies and 2D case reports, the majority of microCT and CBCT studies described the evaluation procedures, and how the qualitative and quantitative analyses were performed (Figs. 2-5, 7, 8). Such information has to be mentioned in studies and case reports for the reviewer to evaluate, the reader to understand and the researcher to refer when designing a future research.
In addition to the radiographic observations for the presence of additional canals either by presence of a “breakpoint” or canal bifurcations in different radiographic angulations, deviation of a previous filling material to one side of the canal, penetration of the root filling material into a missed canal space or CBCT (11, 119, 142), the description of clinical procedures used for detection of root canals is beneficial to the reader. Based on analysis of studies and case reports included in this systematic review, magnification (operating microscopes and loupes), modification of the access cavity, exploration (using DG16 or other), negotiation using K-files, troughing between canal orifices using ultrasonic tips or long shank burs (Figs. 5, 7, 8), in addition to other clinical landmarks such as presence of a bleeding point or sodium hypochlorite bubbling or staining of the pulp chamber floor (129, 135), have been reported.
Weine’s (107) and Vertucci’s classifications (and its supplemental configurations) (102-106, 108) are the most commonly used systems used to classify the root and canal morphology and, along the years, they have been used as the main references to describe the root and canal morphology in current publications using microCT, CBCT and others. In addition to some deficiencies in reporting some items related to inclusion/exclusion criteria, calibration and reproducibility, the authors have noticed the presence of inconsistent use of both classifications. For instance, in Weine’s classification, the floor of the pulp chamber was taken as a reference for the root canal orifice in the MB root of maxillary molars (107), but no information was given to the location of the orifice in single rooted teeth. Similarly, Vertucci’s classification did not define the location of the canal orifice, and it was defined later in his publication as “A root canal begins as a funnel-shaped canal orifices generally present at or slightly apical to the cervical line” (1), with no definition to this “slight apical” position. One possible reason is that Vertucci’s classification was based on staining and clearing method in which teeth were subject to decalcification, staining and clearing; such procedures significantly deteriorate the normal anatomical features of the tooth, including the CEJ, thus making its identification, in some samples, rather challenging. Secondly, the pulp chamber floor location may not coincide with the CEJ (located slightly apical) (1). Unfortunately, the majority of studies and case reports included in this review did not define the location of root canal orifice. Based on the above, it is obvious that the root canal orifice level should be explicitly defined in any related publication. Similar concerns have been raised for intercanal communications - whether they are part of the root canal configurations or not (154). Recently, a number of concerns and considerations have been discussed, and a new coding system has been introduced for accurate description of the root and canal morphology, accessory canals and anomalies (155-157).
Experimental and clinical observations must be reliably measured by calibrated examiners, preferably over time, to be interpreted with confidence (158). This is of particular importance during visual inspection of root canal configuration types, morphology of canal orifices and other morphological variations in 2D and 3D radiographic views, 3D reconstruction images and other conventional methods. This systematic review showed that the majority of studies did not report calibration of examiners or reproducibility tests. It is worth noting that calibration of the machine used for testing and performing measurements is also essential before undertaking quantitative analysis, and this was rarely reported in microCT studies (36, 41).
Statistical methods play an important role in dental research. Due to the developments in computer technology, computationally more demanding and novel statistical methods have also been applied more often (159). This probably justifies the reason for the increased use of inferential statistical analysis in recent root canal anatomy publications comprising qualitative and quantitative presentations compared to staining and clearing studies which mainly describe the root canal configuration types. It is important to note that statistical significance in anatomy publications does not necessarily equate with clinical significance, especially when describing minor details of the root canal system such as angles between canal orifices and length of accessory canals (18, 49).
A Proposal for a Standardized Protocol – Preferred Reporting Items for Root and Canal Anatomy in the Human Dentition (PROUD 2020)
This systematic review aimed to present the general mapping of reporting items related to root and canal morphology, and provide recommendations for consistent reporting in experimental and clinical studies as well as case reports. Based on the discussion above, it appears that a checklist is needed to help authors to document all necessary information required for consistent reporting, and equip researchers and clinicians with the information needed for future studies and reports. It will also help reviewers and editors to check such items during the reviewing process, especially with the development of new software programs with high-quality images, and different modes to enhance the visualization of complex anatomical structures (152, 160, 161).
The PROUD checklist for studies and case reports are designed based on the items extracted and evaluated in this systematic review (Tables 2, 3). The checklist is divided into three components: type of study/report, items for reporting study samples, and items for reporting the evaluation process. For simplicity, the checklists for studies and case reports are designed in a similar manner; but sample size calculation, inclusion/exclusion criteria and statistical analysis are excluded from the checklist for case reports. In the last column for both tables, the author(s) has/have to mention the page number where the items are reported in their submission. This would facilitate the reviewing process for editors and reviewers. Figures 9-13 show examples for reporting studies and case reports based on the PROUD proposed protocol.
TABLE 2.
Reporting items for root and canal morphology in research studies
| Section | Number | Checklist item | Listed on page number |
|---|---|---|---|
| Type of study | 1 | Experimental or clinical (cross-sectional or other); retrospective or prospective | |
| Ethical approval | 2 | Approval from the ethical board committee | |
| Ethnic group/population | 3 | Details on ethnic group or population | |
| Tooth type (or roots) | 4 | Tooth (teeth) type included in the study and/or roots | |
| Sample size calculation | 5 | Information on how the sample size was calculated before undertaking the research | |
| Number of teeth (and/or roots) | 6 | The number of study samples should be reported. | |
| Inclusion/Exclusion criteria | 7 | Information on how the teeth were selected – e.g. caries, resorption defects, restoration, root canal treated teeth, mature root apex, fractures, etc. Other factors related to imaging/ processing issues such as artifacts or samples loss because of chemicals (such as staining and clearing) have to be mentioned as criteria for exclusion. | |
| Age | 8 | If applicable, the age range (or groups) of the study samples or patients should be reported. | |
| Gender | 9 | If applicable, the gender of study samples should be reported. | |
| Diagnostic device specifications and technique | 10 | Radiographic machine: This includes machine type, exposure settings Kv, mA, voxel size (if applicable), FOV (if applicable), angulation techniques, etc, as well as software programs used for analysis. | |
| Other diagnostic tools (such as staining and clearing, SEM, etc): | |||
| The specifications and procedures should be mentioned in details. | |||
| For all, calibration of the machine (if applicable) should be reported. | |||
| Qualitative analysis | 11 | Such as root canal configurations, evaluation of root canal shapes. | |
| Quantitative analysis | 12 | Such as measuring volumes, areas diameters, distances, angles. | |
| How the evaluation process was performed | 13 | Such as examining the coronal/axial/sagittal sections in 3D imaging, or observing the canal bifurcations in | |
| 2D imaging under magnification, etc. | |||
| Endodontic procedures (if applicable) | 14 | Magnification, modification of the access cavity, exploration, negotiation with our without troughing and others (applicable for 2D clinical studies). | |
| Classification used | 15 | Classification used for root canal configurations (with clear definition for orifice location and intercanal communications), root anomalies, accessory canals. | |
| Calibration and reproducibility | 16 | How the examiners were calibrated. Methods for calibration must be described clearly. Intra-rater and/orinter-rater reliability tests must be mentioned. | |
| Statistical analysis (if applicable) | 17 | The type of statistical method and software used for analysis should be reported. |
TABLE 3.
Reporting items for root and canal morphology in case reports
| Section | Number | Checklist item | Listed on page number |
|---|---|---|---|
| Type of report | 1 | Case report, case series. | |
| Ethnic group/population | 2 | Details on ethnic group or population | |
| Age* | 3 | The age range of the patient(s) must be reported. | |
| Gender* | 4 | The gender of patient(s) must be reported. | |
| Tooth type | 5 | Tooth (teeth) type included in the report. | |
| Number of teeth included | 6 | Number of teeth included in the report. | |
| Diagnostic device specifications and technique | 7 | This includes machine type, exposure settings Kv, mA, voxel size (if applicable), FOV (if applicable),angulation techniques, etc. Software(s) used for the analysis. | |
| Qualitative analysis | 8 | Such as root canal configurations, evaluation of root canal shapes. | |
| Quantitative analysis | 9 | Such as measuring volumes, areas, diameters, distances, angles. | |
| How the evaluation process was performed | 10 | Such as examining the coronal/axial/sagittal sections in 3D imaging, or observing the canalbifurcations in 2D imaging under magnification, etc. | |
| Magnification | 11 | Operating microscope or dental loupes or other. | |
| Magnification step and assisted illumination (if used) have to mentioned. | |||
| Modification of the access cavity | 12 | Conventional or changing the access cavity configuration to detect anatomy. | |
| Exploration | 13 | Such as DG16 or other explorers. | |
| Negotiation with or without troughing | 14 | Using ultrasonic tips or burs (troughing) or pre-curved files (without troughing). | |
| Other special clinical observations | 15 | Such as bleeding point, NaOCl bubbling, etc. | |
| Classification used | 16 | Classification for root canal configurations (with clear definitions for the orifice location and intercanal communications),root anomalies, accessory canals, etc. |
In few occasions, case reports may have a presentation of both clinical case and extracted tooth – authors can mention “NA” if related information were not recorded for the extracted tooth
Figure 9.

An example for reporting anatomy in a microCT study. PGG: Palato-gingival groove. MicroCT images from Root canal anatomy project lead by HMA Ahmed and NS Mohamad (2020). PGG - Palato-gingival groove, ICC - Intercanal communication
Figure 13.

An example for reporting anatomy in a case report. Number of patients (and teeth included) should be provided in case series
Figure 10.

An example for reporting anatomy in an experimental CBCT study (extracted teeth)
Figure 11.

An example for reporting anatomy in a clinical CBCT study - X: Excluded because of root canal filling
Figure 12.

An example for reporting anatomy in a clinical study
It is worth noting that other methods have been reported to investigate the anatomical features of the root and canal “in extracted teeth” such as 2D radiographic imaging (162), scanning electron microscope (SEM) (5), stereomicroscope (6), cross sectional methods (163), and optical coherence tomography (164). Despite that these methods are less commonly used, the proposed checklist is applicable since all anatomy publications share similar reporting items for selection of the study samples, and the evaluation section listed in Table 2 can be applied for reporting other experimental procedures.
In addition to journals specialized in the field of pediatric dentistry, Endodontic journals have given a space for publications related to root and canal morphology as well as root canal treatment procedures in the primary dentition (165, 166). The checklist presented in this systematic review can be used for reporting root and canal anatomy in the primary teeth. Indeed, inclusion and exclusion criteria should have details for the stage of physiologic root resorption of the study samples (such as extracted primary molar teeth in which resorption does not exceed one third of root length) (167).
Recently, a number of developmental protocols have been introduced related to reporting guidelines in case reports (168), observational (169) and laboratory studies (170) in addition to clinical trials and animal studies (171, 172). These guidelines aim to improve the quality, accuracy and transparency of case reports and studies. For instance, the preferred reporting Items for case reports in Endodontics (PRICE) checklist (168) is composed of items including the title, abstract, introduction, informed consent, case report information including patient details such as age, gender, ethnicity, chief complain, medical and dental history, extra-oral findings in addition to diagnostic methods used, active treatments and outcomes followed by a number of items to be covered in the discussion section and conclusion. Obviously, following these guidelines “in general” is beneficial to authors, and they are important steps for more accurate and consistent reporting in Endodontics. The present systematic review aimed to present a comprehensive analysis, detect deficiencies of the current literature, and provide a detailed protocol for studies and case reports related to root and canal anatomy with emphasis to “more specific” items (such as how the canals were identified radiographically and clinically, classification used for describing the canal morphology, etc) that have to be mentioned in order to provide an accurate and consistent reporting of root and canal anatomy. The ability of researchers and clinicians to present their studies or reports with clear, accurate items from title to conclusions with special attention to fine details related to the main objective of the report (such as root canal anatomy) is necessary.
CONCLUSION
There is considerable inconsistent reporting of root and canal morphology regardless of the type of study and experimental procedure used. The checklist protocol presented in this systematic review paves the way for a consistent description of root canal anatomy in experimental, clinical, and case report publications.
Footnotes
Conflict of Interest: The authors deny any conflict of interest.
Ethics Committee Approval: Not applicable.
Peer-review: Externally peer-reviewed.
Financial Disclosure: Nil.
Authorship contributions: Concept – H.M.A.A., G.R.F.; Design – H.M.A.A., G.R.F.; Supervision – H.M.A.A., G.R.F.; Funding - None; Materials - None; Data collection &/or processing – None; Analysis and/or interpretation – H.M.A.A., G.R.F.; Literature search – H.M.A.A., G.R.F.; Writing – H.M.A.A., G.R.F.; Critical Review – H.M.A.A., G.R.F.
REFERENCES
- 1.Vertucci F. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3–29. [Google Scholar]
- 2.Martins JNR, Marques D, Mata A, Caramês J. Root and root canal morphology of the permanent dentition in a Caucasian population:a cone-beam computed tomography study. Int Endod J. 2017;50(11):1013–26. doi: 10.1111/iej.12724. [DOI] [PubMed] [Google Scholar]
- 3.Neelakantan P, Subbarao C, Subbarao CV, Ravindranath M. Root and canal morphology of mandibular second molars in an Indian population. J Endod. 2010;36(8):1319–22. doi: 10.1016/j.joen.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 4.Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars:A micro-CT study in different populations. Arch Oral Biol. 2016;61:130–7. doi: 10.1016/j.archoralbio.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 5.Morfis A, Sylaras SN, Georgopoulou M, Kernani M, Prountzos F. Study of the apices of human permanent teeth with the use of a scanning electron microscope. Oral Surg Oral Med Oral Pathol. 1994;77(2):172–6. doi: 10.1016/0030-4220(94)90281-x. [DOI] [PubMed] [Google Scholar]
- 6.Arora S, Tewari S. The morphology of the apical foramen in posterior teeth in a North Indian population. Int Endod J. 2009;42(10):930–9. doi: 10.1111/j.1365-2591.2009.01597.x. [DOI] [PubMed] [Google Scholar]
- 7.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 8.Weine FS, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japanese sub-population. Int Endod J. 1999;32(2):79–87. doi: 10.1046/j.1365-2591.1999.00186.x. [DOI] [PubMed] [Google Scholar]
- 9.Saber SEDM, Ahmed MHM, Obeid M, Ahmed HMA. Root and canal morphology of maxillary premolar teeth in an Egyptian subpopulation using two classification systems:a cone beam computed tomography study. Int Endod J. 2019;52(3):267–78. doi: 10.1111/iej.13016. [DOI] [PubMed] [Google Scholar]
- 10.Caputo BV, Noro Filho GA, de Andrade Salgado DM, Moura-Netto C, Giovani EM, Costa C. Evaluation of the root canal morphology of molars by using cone-beam computed tomography in a Brazilian population:Part I. J Endod. 2016;42(11):1604–7. doi: 10.1016/j.joen.2016.07.026. [DOI] [PubMed] [Google Scholar]
- 11.Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification:an in vivo investigation. J Endod. 2015;41(2):164–8. doi: 10.1016/j.joen.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 12.Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning:a case report. J Endod. 2010;36(5):915–21. doi: 10.1016/j.joen.2009.12.015. [DOI] [PubMed] [Google Scholar]
- 13.Ryan JL, Bowles WR, Baisden MK, McClanahan SB. Mandibular first molar with six separate canals. J Endod. 2011;37(6):878–80. doi: 10.1016/j.joen.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 14.Chan AW, Upshur R, Singh JA, Ghersi D, Chapuis F, Altman DG. Research protocols:waiving confidentiality for the greater good. BMJ. 2006;332(7549):1086–9. doi: 10.1136/bmj.332.7549.1086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ahmed HMA, Luddin N. Accessory mesial roots and root canals in mandibular molar teeth:Case reports. SEM analysis and literature review. ENDO - Endodontic Practice Today. 2012;6(3):195–205. [Google Scholar]
- 16.Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. Ann Intern Med. 2009;151(4):264–9. doi: 10.7326/0003-4819-151-4-200908180-00135. W64. [DOI] [PubMed] [Google Scholar]
- 17.Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, Villas-Bôas MH, Amoroso-Silva PA, Brandão CG, et al. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod. 2013;39(12):1529–33. doi: 10.1016/j.joen.2013.08.033. [DOI] [PubMed] [Google Scholar]
- 18.Ordinola-Zapata R, Bramante CM, Villas-Boas MH, Cavenago BC, Duarte MH, Versiani MA. Morphologic micro-computed tomography analysis of mandibular premolars with three root canals. J Endod. 2013;39(9):1130–5. doi: 10.1016/j.joen.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 19.Park JW, Lee JK, Ha BH, Choi JH, Perinpanayagam H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using micro-computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(3):437–42. doi: 10.1016/j.tripleo.2009.01.022. [DOI] [PubMed] [Google Scholar]
- 20.Divine KA, McClanahan SB, Fok A. Anatomic Analysis of Palatal Roots of Maxillary Molars Using Micro–computed Tomography. J Endod. 2019;45(6):724–8. doi: 10.1016/j.joen.2019.03.007. [DOI] [PubMed] [Google Scholar]
- 21.Marceliano-Alves MF, Lima CO, Bastos LGDPMN, Bruno AMV, Vidaurre F, Coutinho TM, et al. Mandibular mesial root canal morphology using micro-computed tomography in a Brazilian population. Aust Endod J. 2019;45(1):51–6. doi: 10.1111/aej.12265. [DOI] [PubMed] [Google Scholar]
- 22.Johnsen GF, Dara S, Asjad S, Sunde PT, Haugen HJ. Anatomic comparison of contralateral premolars. J Endod. 2017;43(6):956–63. doi: 10.1016/j.joen.2017.01.012. [DOI] [PubMed] [Google Scholar]
- 23.Wolf TG, Paqué F, Zeller M, Willershausen B, Briseño-Marroquín B. Root canal morphology and configuration of 118 mandibular first molars by means of micro-computed tomography:An ex vivo study. J Endod. 2016;42(4):610–4. doi: 10.1016/j.joen.2016.01.004. [DOI] [PubMed] [Google Scholar]
- 24.Marceliano-Alves M, Alves FR, Mendes Dde M, Provenzano JC. Micro-computed tomography analysis of the root canal morphology of palatal roots of maxillary first molars. J Endod. 2016;42(2):280–3. doi: 10.1016/j.joen.2015.10.016. [DOI] [PubMed] [Google Scholar]
- 25.Briseño-Marroquín B, Paqué F, Maier K, Willershausen B, Wolf TG. Root canal morphology and configuration of 179 maxillary first molars by means of micro-computed tomography:An ex vivo study. J Endod. 2015;41(12):2008–13. doi: 10.1016/j.joen.2015.09.007. [DOI] [PubMed] [Google Scholar]
- 26.Filpo-Perez C, Bramante CM, Villas-Boas MH, Húngaro Duarte MA, Versiani MA, Ordinola-Zapata R. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J Endod. 2015;41(2):231–6. doi: 10.1016/j.joen.2014.09.024. [DOI] [PubMed] [Google Scholar]
- 27.Leoni GB, Versiani MA, Pécora JD, Damião de Sousa-Neto M. Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod. 2014;40(5):710–6. doi: 10.1016/j.joen.2013.09.003. [DOI] [PubMed] [Google Scholar]
- 28.Harris SP, Bowles WR, Fok A, McClanahan SB. An anatomic investigation of the mandibular first molar using micro-computed tomography. J Endod. 2013;39(11):1374–8. doi: 10.1016/j.joen.2013.06.034. [DOI] [PubMed] [Google Scholar]
- 29.Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J. 2013;46(9):800–7. doi: 10.1111/iej.12061. [DOI] [PubMed] [Google Scholar]
- 30.Gu Y, Lee JK, Spångberg LS, Lee Y, Park CM, Seo DG, et al. Minimum-intensity projection for in-depth morphology study of mesiobuccal root. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(5):671–7. doi: 10.1016/j.tripleo.2011.04.036. [DOI] [PubMed] [Google Scholar]
- 31.Verma P, Love RM. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J. 2011;44(3):210–7. doi: 10.1111/j.1365-2591.2010.01800.x. [DOI] [PubMed] [Google Scholar]
- 32.Gu L, Wei X, Ling J, Huang X. A microcomputed tomographic study of canal isthmuses in the mesial root of mandibular first molars in a Chinese population. J Endod. 2009;35(3):353–6. doi: 10.1016/j.joen.2008.11.029. [DOI] [PubMed] [Google Scholar]
- 33.Somma F, Leoni D, Plotino G, Grande NM, Plasschaert A. Root canal morphology of the mesiobuccal root of maxillary first molars:a micro-computed tomographic analysis. Int Endod J. 2009;42(2):165–74. doi: 10.1111/j.1365-2591.2008.01472.x. [DOI] [PubMed] [Google Scholar]
- 34.Grande NM, Plotino G, Pecci R, Bedini R, Pameijer CH, Somma F. Micro-computerized tomographic analysis of radicular and canal morphology of premolars with long oval canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(3):e70–6. doi: 10.1016/j.tripleo.2008.04.022. [DOI] [PubMed] [Google Scholar]
- 35.Mannocci F, Peru M, Sherriff M, Cook R, Pitt Ford TR. The isthmuses of the mesial root of mandibular molars:a micro-computed tomographic study. Int Endod J. 2005;38(8):558–63. doi: 10.1111/j.1365-2591.2005.00994.x. [DOI] [PubMed] [Google Scholar]
- 36.Villas-Bôas MH, Bernardineli N, Cavenago BC, Marciano M, Del Carpio-Perochena A, de Moraes IG, et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod. 2011;37(12):1682–6. doi: 10.1016/j.joen.2011.08.001. [DOI] [PubMed] [Google Scholar]
- 37.Bjørndal L, Carlsen O, Thuesen G, Darvann T, Kreiborg S. External and internal macromorphology in 3D-reconstructed maxillary molars using computerized X-ray microtomography. Int Endod J. 1999;32(1):3–9. doi: 10.1046/j.1365-2591.1999.00172.x. [DOI] [PubMed] [Google Scholar]
- 38.Hartmann RC, Baldasso FE, Stürmer CP, Acauan MD, Scarparo RK, Morgental RD, et al. Clinically relevant dimensions of 3-rooted maxillary premolars obtained via high-resolution computed tomography. J Endod. 2013;39(12):1639–45. doi: 10.1016/j.joen.2013.07.029. [DOI] [PubMed] [Google Scholar]
- 39.Keleş A, Keskin C. Apical root canal morphology of mesial roots of mandibular first molar teeth with Vertucci type II configuration by means of micro-computed tomography. J Endod. 2017;43(3):481–5. doi: 10.1016/j.joen.2016.10.045. [DOI] [PubMed] [Google Scholar]
- 40.Fan B, Pan Y, Gao Y, Fang F, Wu Q, Gutmann JL. Three-dimensional morphologic analysis of isthmuses in the mesial roots of mandibular molars. J Endod. 2010;36(11):1866–9. doi: 10.1016/j.joen.2010.08.030. [DOI] [PubMed] [Google Scholar]
- 41.ElAyouti A, Hülber-J M, Judenhofer MS, Connert T, Mannheim JG, Löst C, et al. Apical constriction:location and dimensions in molars-a micro-computed tomography study. J Endod. 2014;40(8):1095–9. doi: 10.1016/j.joen.2013.12.002. [DOI] [PubMed] [Google Scholar]
- 42.Keleş A, Keskin C. A micro-computed tomographic study of band-shaped root canal isthmuses having their floor in the apical third of mesial roots of mandibular first molars. Int Endod J. 2018;51(2):240–6. doi: 10.1111/iej.12842. [DOI] [PubMed] [Google Scholar]
- 43.Keleş A, Keskin C. Deviations of mesial root canals of mandibular first molar teeth at the apical third:A micro-computed tomographic study. J Endod. 2018;44(6):1030–2. doi: 10.1016/j.joen.2018.02.028. [DOI] [PubMed] [Google Scholar]
- 44.Ordinola-Zapata R, Martins JNR, Niemczyk S, Bramante CM. Apical root canal anatomy in the mesiobuccal root of maxillary first molars:influence of root apical shape and prevalence of apical foramina - a micro-CT study. Int Endod J. 2019;52(8):1218–27. doi: 10.1111/iej.13109. [DOI] [PubMed] [Google Scholar]
- 45.Versiani MA, Pécora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars:a micro-computed tomography study. J Endod. 2012;38(7):977–82. doi: 10.1016/j.joen.2012.03.026. [DOI] [PubMed] [Google Scholar]
- 46.Versiani MA, Pécora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J. 2011;44(7):682–7. doi: 10.1111/j.1365-2591.2011.01879.x. [DOI] [PubMed] [Google Scholar]
- 47.Vier-Pelisser FV, Dummer PM, Bryant S, Marca C, Só MV, Figueiredo JA. The anatomy of the root canal system of three-rooted maxillary premolars analysed using high-resolution computed tomography. Int Endod J. 2010;43(12):1122–31. doi: 10.1111/j.1365-2591.2010.01787.x. [DOI] [PubMed] [Google Scholar]
- 48.Xu T, Tay FR, Gutmann JL, Fan B, Fan W, Huang Z, et al. Micro-computed tomography assessment of apical accessory canal morphologies. J Endod. 2016;42(5):798–802. doi: 10.1016/j.joen.2016.02.006. [DOI] [PubMed] [Google Scholar]
- 49.Xu T, Fan W, Tay FR, Fan B. Micro-computed tomographic evaluation of the prevalence distribution, and morphologic features of accessory canals in Chinese permanent teeth. J Endod. 2019;45(8):994–9. doi: 10.1016/j.joen.2019.04.001. [DOI] [PubMed] [Google Scholar]
- 50.Guerreiro D, Shin JM, Pereira M, McDonald NJ. Radicular groove accessory canal morphology in mandibular first premolars:Micro-computed tomographic study. J Endod. 2019;45(5):554–9. doi: 10.1016/j.joen.2018.12.017. [DOI] [PubMed] [Google Scholar]
- 51.Fan W, Fan B, Gutmann JL, Cheung GS. Identification of C-shaped canal in mandibular second molars. Part I:radiographic and anatomical features revealed by intraradicular contrast medium. J Endod. 2007;33(7):806–10. doi: 10.1016/j.joen.2007.04.007. [DOI] [PubMed] [Google Scholar]
- 52.Gu YC. A micro-computed tomographic analysis of maxillary lateral incisors with radicular grooves. J Endod. 2011;37(6):789–92. doi: 10.1016/j.joen.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 53.Zhang Q, Chen H, Fan B, Fan W, Gutmann JL. Root and root canal morphology in maxillary second molar with fused root from a native Chinese population. J Endod. 2014;40(6):871–5. doi: 10.1016/j.joen.2013.10.035. [DOI] [PubMed] [Google Scholar]
- 54.Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010;36(10):1622–7. doi: 10.1016/j.joen.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 55.Widmer SD, Kulild JC, Walker MP, Williams KB, Katz J. Predicting the anatomical position of the palatal root apex in maxillary first premolars during surgical endodontic treatment. J Endod. 2010;36(3):434–7. doi: 10.1016/j.joen.2009.12.013. [DOI] [PubMed] [Google Scholar]
- 56.Hiebert BM, Abramovitch K, Rice D, Torabinejad M. Prevalence of second mesiobuccal canals in maxillary first molars detected using cone-beam computed tomography direct occlusal sccess, and coronal plane grinding. J Endod. 2017;43(10):1711–5. doi: 10.1016/j.joen.2017.05.011. [DOI] [PubMed] [Google Scholar]
- 57.Fernandes NA, Herbst D, Postma TC, Bunn BK. The prevalence of second canals in the mesiobuccal root of maxillary molars:A cone beam computed tomography study. Aust Endod J. 2019;45(1):46–50. doi: 10.1111/aej.12263. [DOI] [PubMed] [Google Scholar]
- 58.de Lima CO, de Souza LC, Devito KL, do Prado M, Campos CN. Evaluation of root canal morphology of maxillary premolars:a cone-beam computed tomography study. Aust Endod J. 2019;45(2):196–201. doi: 10.1111/aej.12308. [DOI] [PubMed] [Google Scholar]
- 59.Martins JNR, Alkhawas MAM, Altaki Z, Bellardini G, Berti L, Boveda C, et al. Worldwide analyses of maxillary first molar second mesiobuccal prevalence:A multicenter cone-beam computed tomographic study. J Endod. 2018;44(11):1641–9. doi: 10.1016/j.joen.2018.07.027. [DOI] [PubMed] [Google Scholar]
- 60.Martins JNR, Ordinola-Zapata R, Marques D, Francisco H, Caramês J. Differences in root canal system configuration in human permanent teeth within different age groups. Int Endod J. 2018;51(8):931–41. doi: 10.1111/iej.12896. [DOI] [PubMed] [Google Scholar]
- 61.Martins JNR, Gu Y, Marques D, Francisco H, Caramês J. Differences on the root and root canal morphologies between Asian and White ethnic groups analyzed by cone-beam computed tomography. J Endod. 2018;44(7):1096–104. doi: 10.1016/j.joen.2018.04.001. [DOI] [PubMed] [Google Scholar]
- 62.Ratanajirasut R, Panichuttra A, Panmekiate S. A cone-beam computed tomographic study of root and canal morphology of maxillary first and second permanent molars in a Thai population. J Endod. 2018;44(1):56–61. doi: 10.1016/j.joen.2017.08.020. [DOI] [PubMed] [Google Scholar]
- 63.Shemesh A, Kavalerchik E, Levin A, Ben Itzhak J, Levinson O, Lvovsky A, et al. Root canal morphology evaluation of central and lateral mandibular incisors using cone-beam computed tomography in an Israeli population. J Endod. 2018;44(1):51–5. doi: 10.1016/j.joen.2017.08.012. [DOI] [PubMed] [Google Scholar]
- 64.Bürklein S, Heck R, Schäfer E. Evaluation of the root canal anatomy of maxillary and mandibular premolars in a selected German population using cone-beam computed tomographic data. J Endod. 2017;43(9):1448–52. doi: 10.1016/j.joen.2017.03.044. [DOI] [PubMed] [Google Scholar]
- 65.Pérez-Heredia M, Ferrer-Luque CM, Bravo M, Castelo-Baz P, Ruíz-Piñón M, Baca P. Cone-beam computed tomographic study of root anatomy and canal configuration of molars in a Spanish population. J Endod. 2017;43(9):1511–6. doi: 10.1016/j.joen.2017.03.026. [DOI] [PubMed] [Google Scholar]
- 66.Ghobashy AM, Nagy MM, Bayoumi AA. Evaluation of root and canal morphology of maxillary permanent molars in an Egyptian population by cone-beam computed tomography. J Endod. 2017;43(7):1089–92. doi: 10.1016/j.joen.2017.02.014. [DOI] [PubMed] [Google Scholar]
- 67.Tahmasbi M, Jalali P, Nair MK, Barghan S, Nair UP. Prevalence of middle mesial canals and isthmi in the mesial root of mandibular molars:An in vivo cone-beam computed tomographic study. J Endod. 2017;43(7):1080–3. doi: 10.1016/j.joen.2017.02.008. [DOI] [PubMed] [Google Scholar]
- 68.Tian XM, Yang XW, Qian L, Wei B, Gong Y. Analysis of the root and canal morphologies in maxillary first and second molars in a Chinese population using cone-beam computed tomography. J Endod. 2016;42(5):696–701. doi: 10.1016/j.joen.2016.01.017. [DOI] [PubMed] [Google Scholar]
- 69.Kim SY, Kim BS, Kim Y. Mandibular second molar root canal morphology and variants in a Korean subpopulation. Int Endod J. 2016;49(2):136–44. doi: 10.1111/iej.12437. [DOI] [PubMed] [Google Scholar]
- 70.Abella F, Teixidó LM, Patel S, Sosa F, Duran-Sindreu F, Roig M. Cone-beam computed tomography analysis of the root canal morphology of maxillary first and second premolars in a Spanish population. J Endod. 2015;41(8):1241–7. doi: 10.1016/j.joen.2015.03.026. [DOI] [PubMed] [Google Scholar]
- 71.Han T, Ma Y, Yang L, Chen X, Zhang X, Wang Y. A study of the root canal morphology of mandibular anterior teeth using cone-beam computed tomography in a Chinese subpopulation. J Endod. 2014;40(9):1309–14. doi: 10.1016/j.joen.2014.05.008. [DOI] [PubMed] [Google Scholar]
- 72.Silva EJ, Nejaim Y, Silva AI, Haiter-Neto F, Zaia AA, Cohenca N. Evaluation of root canal configuration of maxillary molars in a Brazilian population using cone-beam computed tomographic imaging:an in vivo study. J Endod. 2014;40(2):173–6. doi: 10.1016/j.joen.2013.10.002. [DOI] [PubMed] [Google Scholar]
- 73.Guo J, Vahidnia A, Sedghizadeh P, Enciso R. Evaluation of root and canal morphology of maxillary permanent first molars in a North American population by cone-beam computed tomography. J Endod. 2014;40(5):635–9. doi: 10.1016/j.joen.2014.02.002. [DOI] [PubMed] [Google Scholar]
- 74.Yang L, Chen X, Tian C, Han T, Wang Y. Use of cone-beam computed tomography to evaluate root canal morphology and locate root canal orifices of maxillary second premolars in a Chinese subpopulation. J Endod. 2014;40(5):630–4. doi: 10.1016/j.joen.2014.01.007. [DOI] [PubMed] [Google Scholar]
- 75.Plotino G, Tocci L, Grande NM, Testarelli L, Messineo D, Ciotti M, et al. Symmetry of root and root canal morphology of maxillary and mandibular molars in a white population:a cone-beam computed tomography study in vivo. J Endod. 2013;39(12):1545–8. doi: 10.1016/j.joen.2013.09.012. [DOI] [PubMed] [Google Scholar]
- 76.Kim SY, Kim BS, Woo J, Kim Y. Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population:variations in the number of roots and canals. J Endod. 2013;39(12):1516–21. doi: 10.1016/j.joen.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 77.Silva EJNL, Nejaim Y, Silva AV, Haiter-Neto F, Cohenca N. Evaluation of root canal configuration of mandibular molars in a Brazilian population by using cone-beam computed tomography:An in vivo study. J Endod. 2013;39(7):849–52. doi: 10.1016/j.joen.2013.04.030. [DOI] [PubMed] [Google Scholar]
- 78.Reis AG, Grazziotin-Soares R, Barletta FB, Fontanella VR, Mahl CR. Second canal in mesiobuccal root of maxillary molars is correlated with root third and patient age:a cone-beam computed tomographic study. J Endod. 2013;39(5):588–92. doi: 10.1016/j.joen.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 79.Yang H, Tian C, Li G, Yang L, Han X, Wang Y. A cone-beam computed tomography study of the root canal morphology of mandibular first premolars and the location of root canal orifices and apical foramina in a Chinese subpopulation. J Endod. 2013;39(4):435–8. doi: 10.1016/j.joen.2012.11.003. [DOI] [PubMed] [Google Scholar]
- 80.Tian YY, Guo B, Zhang R, Yu X, Wang H, Hu T, et al. Root and canal morphology of maxillary first premolars in a Chinese subpopulation evaluated using cone-beam computed tomography. Int Endod J. 2012;45(11):996–1003. doi: 10.1111/j.1365-2591.2012.02059.x. [DOI] [PubMed] [Google Scholar]
- 81.Kim Y, Lee SJ, Woo J. Morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a korean population:variations in the number of roots and canals and the incidence of fusion. J Endod. 2012;38(8):1063–8. doi: 10.1016/j.joen.2012.04.025. [DOI] [PubMed] [Google Scholar]
- 82.Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011;44(11):990–9. doi: 10.1111/j.1365-2591.2011.01904.x. [DOI] [PubMed] [Google Scholar]
- 83.Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J. 2011;44(2):162–9. doi: 10.1111/j.1365-2591.2010.01826.x. [DOI] [PubMed] [Google Scholar]
- 84.Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, et al. Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod. 2010;36(11):1786–9. doi: 10.1016/j.joen.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 85.Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36(9):1480–4. doi: 10.1016/j.joen.2010.06.018. [DOI] [PubMed] [Google Scholar]
- 86.Lee JH, Kim KD, Lee JK, Park W, Jeong JS, Lee Y, et al. Mesiobuccal root canal anatomy of Korean maxillary first and second molars by cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(6):785–91. doi: 10.1016/j.tripleo.2010.11.026. [DOI] [PubMed] [Google Scholar]
- 87.Wu YC, Cheng WC, Chung MP, Su CC, Weng PW, Cathy Tsai YW, et al. Complicated root canal morphology of mandibular lateral incisors is associated with the presence of distolingual root in mandibular first molars:A cone-beam computed tomographic study in a Taiwanese population. J Endod. 2018;44(1):73–9.e1. doi: 10.1016/j.joen.2017.08.027. [DOI] [PubMed] [Google Scholar]
- 88.Zhang Y, Xu H, Wang D, Gu Y, Wang J, Tu S, et al. Assessment of the second mesiobuccal root canal in maxillary first molars:A cone-beam computed tomographic study. J Endod. 2017;43(12):1990–6. doi: 10.1016/j.joen.2017.06.021. [DOI] [PubMed] [Google Scholar]
- 89.Parker J, Mol A, Rivera EM, Tawil P. CBCT uses in clinical endodontics:the effect of CBCT on the ability to locate MB2 canals in maxillary molars. Int Endod J. 2017;50(12):1109–15. doi: 10.1111/iej.12736. [DOI] [PubMed] [Google Scholar]
- 90.Akbarzadeh N, Aminoshariae A, Khalighinejad N, Palomo JM, Syed A, Kulild JC, et al. The association between the anatomic landmarks of the pulp chamber floor and the prevalence of middle mesial canals in mandibular first molars:An in vivo analysis. J Endod. 2017;43(11):1797–801. doi: 10.1016/j.joen.2017.07.003. [DOI] [PubMed] [Google Scholar]
- 91.Estrela C, Couto GS, Bueno MR, Bueno KG, Estrela LRA, Porto OCL, et al. Apical foramen position in relation to proximal root surfaces of human permanent teeth determined by using a new cone-beam computed tomographic software. J Endod. 2018;44(11):1741–8. doi: 10.1016/j.joen.2018.07.028. [DOI] [PubMed] [Google Scholar]
- 92.Estrela C, Rabelo LE, de Souza JB, Alencar AH, Estrela CR, Sousa Neto MD, et al. Frequency of root canal isthmi in human permanent teeth determined by cone-beam computed tomography. J Endod. 2015;41(9):1535–9. doi: 10.1016/j.joen.2015.05.016. [DOI] [PubMed] [Google Scholar]
- 93.Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population--a clinical study. Int Endod J. 2008;41(9):755–62. doi: 10.1111/j.1365-2591.2008.01427.x. [DOI] [PubMed] [Google Scholar]
- 94.Stropko JJ. Canal morphology of maxillary molars:clinical observations of canal configurations. J Endod. 1999;25(6):446–50. doi: 10.1016/S0099-2399(99)80276-3. [DOI] [PubMed] [Google Scholar]
- 95.Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars:incidence and related factors. J Endod. 2015;41(1):28–32. doi: 10.1016/j.joen.2014.08.004. [DOI] [PubMed] [Google Scholar]
- 96.Al-Fouzan KS, Ounis HF, Merdad K, Al-Hezaimi K. Incidence of canal systems in the mesio-buccal roots of maxillary first and second molars in Saudi Arabian population. Aust Endod J. 2013;39(3):98–101. doi: 10.1111/j.1747-4477.2010.00289.x. [DOI] [PubMed] [Google Scholar]
- 97.Peikoff MD, Christie WH, Fogel HM. The maxillary second molar:variations in the number of roots and canals. Int Endod J. 1996;29(6):365–9. doi: 10.1111/j.1365-2591.1996.tb01399.x. [DOI] [PubMed] [Google Scholar]
- 98.Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7(12):565–8. doi: 10.1016/S0099-2399(81)80216-6. [DOI] [PubMed] [Google Scholar]
- 99.Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root of the maxillary first molar:a clinical study. J Endod. 1994;20(3):135–7. doi: 10.1016/S0099-2399(06)80059-2. [DOI] [PubMed] [Google Scholar]
- 100.Neaverth EJ, Kotler LM, Kaltenbach RF. Clinical investigation (in vivo) of endodontically treated maxillary first molars. J Endod. 1987;13(10):506–12. doi: 10.1016/S0099-2399(87)80018-3. [DOI] [PubMed] [Google Scholar]
- 101.Fabra-Campos H. Three canals in the mesial root of mandibular first permanent molars:a clinical study. Int Endod J. 1989;22(1):39–43. doi: 10.1111/j.1365-2591.1989.tb00503.x. [DOI] [PubMed] [Google Scholar]
- 102.Al-Qudah AA, Awawdeh LA. Root and canal morphology of mandibular first and second molar teeth in a Jordanian population. Int Endod J. 2009;42(9):775–84. doi: 10.1111/j.1365-2591.2009.01578.x. [DOI] [PubMed] [Google Scholar]
- 103.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 104.Alavi AM, Opasanon A, Ng YL, Gulabivala K. Root and canal morphology of Thai maxillary molars. Int Endod J. 2002;35(5):478–85. doi: 10.1046/j.1365-2591.2002.00511.x. [DOI] [PubMed] [Google Scholar]
- 105.Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J. 2002;35(1):56–62. doi: 10.1046/j.1365-2591.2002.00452.x. [DOI] [PubMed] [Google Scholar]
- 106.Vertucci F, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol. 1974;38(3):456–64. doi: 10.1016/0030-4220(74)90374-0. [DOI] [PubMed] [Google Scholar]
- 107.Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28(3):419–25. doi: 10.1016/0030-4220(69)90237-0. [DOI] [PubMed] [Google Scholar]
- 108.Ng YL, Aung TH, Alavi A, Gulabivala K. Root and canal morphology of Burmese maxillary molars. Int Endod J. 2001;34(8):620–30. doi: 10.1046/j.1365-2591.2001.00438.x. [DOI] [PubMed] [Google Scholar]
- 109.De Deus QD. Frequency location, and direction of the lateral secondary, and accessory canals. J Endod. 1975;1(11):361–6. doi: 10.1016/s0099-2399(75)80211-1. [DOI] [PubMed] [Google Scholar]
- 110.Adorno CG, Yoshioka T, Suda H. Incidence of accessory canals in Japanese anterior maxillary teeth following root canal filling ex vivo. Int Endod J. 2010;43(5):370–6. doi: 10.1111/j.1365-2591.2010.01688.x. [DOI] [PubMed] [Google Scholar]
- 111.Kasahara E, Yasuda E, Yamamoto A, Anzai M. Root canal system of the maxillary central incisor. J Endod. 1990;16(4):158–61. doi: 10.1016/S0099-2399(06)81962-X. [DOI] [PubMed] [Google Scholar]
- 112.Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of the mandibular incisor. J Endod. 1997;23(8):479–84. doi: 10.1016/S0099-2399(97)80305-6. [DOI] [PubMed] [Google Scholar]
- 113.Ring J, Ring KC. Rare root canal configuration of mandibular second premolar using cone-beam computed tomographic scanning. J Endod. 2017;43(11):1897–900. doi: 10.1016/j.joen.2017.04.023. [DOI] [PubMed] [Google Scholar]
- 114.Levin A, Shemesh A, Katzenell V, Gottlieb A, Ben Itzhak J, Solomonov M. Use of cone-beam computed tomography during retreatment of a 2-rooted maxillary central incisor:Case report of a complex diagnosis and treatment. J Endod. 2015;41(12):2064–7. doi: 10.1016/j.joen.2014.04.016. [DOI] [PubMed] [Google Scholar]
- 115.Zoya-Farook A, Abhishek P, Shahabadi A. Cone-beam computed tomographic evaluation and endodontic management of a mandibular first premolar with type IX canal configuration:Case report. J Endod. 2017;43(7):1207–13. doi: 10.1016/j.joen.2017.01.011. [DOI] [PubMed] [Google Scholar]
- 116.Zeng C, Shen Y, Guan X, Wang X, Fan M, Li Y. Rare root canal configuration of bilateral maxillary second molar using cone-beam computed tomographic scanning. J Endod. 2016;42(4):673–7. doi: 10.1016/j.joen.2015.12.028. [DOI] [PubMed] [Google Scholar]
- 117.Lea C, Deblinger J, Machado R, Nogueira Leal Silva EJ, Vansan LP. Maxillary premolar with 4 separate canals. J Endod. 2014;40(4):591–3. doi: 10.1016/j.joen.2013.09.016. [DOI] [PubMed] [Google Scholar]
- 118.Kang M, Kim E. Unusual morphology of permanent tooth related to traumatic injury:a case report. J Endod. 2014;40(10):1698–701. doi: 10.1016/j.joen.2014.06.006. [DOI] [PubMed] [Google Scholar]
- 119.Kottoor J, Velmurugan N, Surendran S. Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning:a case report. J Endod. 2011;37(5):715–9. doi: 10.1016/j.joen.2011.01.008. [DOI] [PubMed] [Google Scholar]
- 120.Ioannidis K, Lambrianidis T, Beltes P, Besi E, Malliari M. Endodontic management and cone-beam computed tomography evaluation of seven maxillary and mandibular molars with single roots and single canals in a patient. J Endod. 2011;37(1):103–9. doi: 10.1016/j.joen.2010.09.001. [DOI] [PubMed] [Google Scholar]
- 121.Krithikadatta J, Kottoor J, Karumaran CS, Rajan G. Mandibular first molar having an unusual mesial root canal morphology with contradictory cone-beam computed tomography findings:a case report. J Endod. 2010;36(10):1712–6. doi: 10.1016/j.joen.2010.06.024. [DOI] [PubMed] [Google Scholar]
- 122.Kottoor J, Hemamalathi S, Sudha R, Velmurugan N. Maxillary second molar with 5 roots and 5 canals evaluated using cone beam computerized tomography:a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(2):e162–5. doi: 10.1016/j.tripleo.2009.09.032. [DOI] [PubMed] [Google Scholar]
- 123.Jeong JW, Zegar Z, Liu RY, Makins SR. Radiographic indications of Vertucci type V configuration in the distal root of mandibular molars:A case series. J Endod. 2019;45(4):453–8. doi: 10.1016/j.joen.2018.12.010. [DOI] [PubMed] [Google Scholar]
- 124.Badole GP, Warhadpande MM, Shenoi PR, Lachure C, Badole SG. A rare root canal configuration of bilateral maxillary first molar with 7 root canals diagnosed using cone-beam computed tomographic scanning:a case report. J Endod. 2014;40(2):296–301. doi: 10.1016/j.joen.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 125.La SH, Jung DH, Kim EC, Min KS. Identification of independent middle mesial canal in mandibular first molar using cone-beam computed tomography imaging. J Endod. 2010;36(3):542–5. doi: 10.1016/j.joen.2009.11.008. [DOI] [PubMed] [Google Scholar]
- 126.Fogel HM, Cunha RS. Maxillary first molars with 2 distobuccal canals:A case series. J Endod. 2017;43(11):1925–8. doi: 10.1016/j.joen.2017.07.004. [DOI] [PubMed] [Google Scholar]
- 127.Nosrat A, Verma P, Hicks ML, Schneider SC, Behnia A, Azim AA. Variations of palatal canal morphology in maxillary molars:A case series and literature review. J Endod. 2017;43(11):1888–96. doi: 10.1016/j.joen.2017.04.006. [DOI] [PubMed] [Google Scholar]
- 128.Calvert G. Maxillary central incisor with type V canal morphology:case report and literature review. J Endod. 2014;40(10):1684–7. doi: 10.1016/j.joen.2014.01.046. [DOI] [PubMed] [Google Scholar]
- 129.Ahmad IA, Al-Jadaa A. Three root canals in the mesiobuccal root of maxillary molars:case reports and literature review. J Endod. 2014;40(12):2087–94. doi: 10.1016/j.joen.2014.07.034. [DOI] [PubMed] [Google Scholar]
- 130.Kottoor J, Murugesan R, Albuquerque DV. A maxillary lateral incisor with four root canals. Int Endod J. 2012;45(4):393–7. doi: 10.1111/j.1365-2591.2011.01984.x. [DOI] [PubMed] [Google Scholar]
- 131.Floratos S, Kratchman SI. Conventional and surgical endodontic treatment of a maxillary first molar with unusual anatomy--a case report. Int Endod J. 2011;44(4):376–84. doi: 10.1111/j.1365-2591.2010.01834.x. [DOI] [PubMed] [Google Scholar]
- 132.Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar:a case report and literature review. Int Endod J. 2010;43(8):714–22. doi: 10.1111/j.1365-2591.2010.01737.x. [DOI] [PubMed] [Google Scholar]
- 133.Albuquerque DV, Kottoor J, Dham S, Velmurugan N, Abarajithan M, Sudha R. Endodontic management of maxillary permanent first molar with 6 root canals:3 case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(4):e79–83. doi: 10.1016/j.tripleo.2010.04.017. [DOI] [PubMed] [Google Scholar]
- 134.Poorni S, Karumaran CS, Indira R. Mandibular first premolar with two roots and three canals. Aust Endod J. 2010;36(1):32–4. doi: 10.1111/j.1747-4477.2009.00170.x. [DOI] [PubMed] [Google Scholar]
- 135.Karthikeyan K, Mahalaxmi S. New nomenclature for extra canals based on four reported cases of maxillary first molars with six canals. J Endod. 2010;36(6):1073–8. doi: 10.1016/j.joen.2009.12.001. [DOI] [PubMed] [Google Scholar]
- 136.Faramarzi F, Fakhri H, Javaheri HH. Endodontic treatment of a mandibular first molar with three mesial canals and broken instrument removal. Aust Endod J. 2010;36(1):39–41. doi: 10.1111/j.1747-4477.2009.00162.x. [DOI] [PubMed] [Google Scholar]
- 137.Reeh ES. Seven canals in a lower first molar. J Endod. 1998;24(7):497–9. doi: 10.1016/S0099-2399(98)80055-1. [DOI] [PubMed] [Google Scholar]
- 138.Baugh D, Wallace J. Middle mesial canal of the mandibular first molar:a case report and literature review. J Endod. 2004;30(3):185–6. doi: 10.1097/00004770-200403000-00015. [DOI] [PubMed] [Google Scholar]
- 139.Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod. 1985;11(12):568–72. doi: 10.1016/S0099-2399(85)80204-1. [DOI] [PubMed] [Google Scholar]
- 140.England MC, Jr, Hartwell GR, Lance JR. Detection and treatment of multiple canals in mandibular premolars. J Endod. 1991;17(4):174–8. doi: 10.1016/S0099-2399(06)82012-1. [DOI] [PubMed] [Google Scholar]
- 141.Bond JL, Hartwell G, Portell FR. Maxillary first molar with six canals. J Endod. 1988;14(5):258–60. doi: 10.1016/S0099-2399(88)80180-8. [DOI] [PubMed] [Google Scholar]
- 142.Malagnino V, Gallottini L, Passariello P. Some unusual clinical cases on root anatomy of permanent maxillary molars. J Endod. 1997;23(2):127–8. doi: 10.1016/S0099-2399(97)80260-9. [DOI] [PubMed] [Google Scholar]
- 143.Maggiore F, Jou YT, Kim S. A six-canal maxillary first molar:case report. Int Endod J. 2002;35(5):486–91. doi: 10.1046/j.1365-2591.2002.00533.x. [DOI] [PubMed] [Google Scholar]
- 144.Nallapati S. Three canal mandibular first and second premolars:a treatment approach. J Endod. 2005;31(6):474–6. doi: 10.1097/01.don.0000157986.69173.a6. [DOI] [PubMed] [Google Scholar]
- 145.Rödig T, Hülsmann M. Diagnosis and root canal treatment of a mandibular second premolar with three root canals. Int Endod J. 2003;36(12):912–9. doi: 10.1111/j.1365-2591.2003.00750.x. [DOI] [PubMed] [Google Scholar]
- 146.Holderrieth S, Gernhardt CR. Maxillary molars with morphologic variations of the palatal root canals:a report of four cases. J Endod. 2009;35(7):1060–5. doi: 10.1016/j.joen.2009.04.029. [DOI] [PubMed] [Google Scholar]
- 147.Sabala CL, Benenati FW, Neas BR. Bilateral root or root canal aberrations in a dental school patient population. J Endod. 1994;20(1):38–42. doi: 10.1016/s0099-2399(06)80025-7. [DOI] [PubMed] [Google Scholar]
- 148.Serman NJ, Hasselgren G. The radiographic incidence of multiple roots and canals in human mandibular premolars. Int Endod J. 1992;25(5):234–7. doi: 10.1111/j.1365-2591.1992.tb01155.x. [DOI] [PubMed] [Google Scholar]
- 149.Nayak BK. Understanding the relevance of sample size calculation. Indian J Ophthalmol. 2010;58(6):469–70. doi: 10.4103/0301-4738.71673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Faot F, Chatterjee M, de Camargos GV, Duyck J, Vandamme K. Micro-CT analysis of the rodent jaw bone micro-architecture:A systematic review. Bone Rep. 2015;2:14–24. doi: 10.1016/j.bonr.2014.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Martins JNR, Marques D, Francisco H, Caramês J. Gender influence on the number of roots and root canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int. 2018;49(2):103–11. doi: 10.3290/j.qi.a39508. [DOI] [PubMed] [Google Scholar]
- 152.Bueno MR, Estrela C, Azevedo BC, Diogenes A. Development of a new cone-beam computed tomography software for endodontic diagnosis. Braz Dent J. 2018;29(6):517–29. doi: 10.1590/0103-6440201802455. [DOI] [PubMed] [Google Scholar]
- 153.Ahmed HMA. Guidelines to enhance the interpretation of two-dimensional periapical radiographic images in endodontics. Eur J Gen Dent. 2015;4(3):106–12. [Google Scholar]
- 154.Karobari MI, Noorani TY, Halim MS, Dummer PMH, Ahmed HMA. Should inter-canal communications be included in the classification of root canal systems? Int Endod J. 2019;52(6):917–9. doi: 10.1111/iej.13106. [DOI] [PubMed] [Google Scholar]
- 155.Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–70. doi: 10.1111/iej.12685. [DOI] [PubMed] [Google Scholar]
- 156.Ahmed HMA, Neelakantan P, Dummer PMH. A new system for classifying accessory canal morphology. Int Endod J. 2018;51(2):164–76. doi: 10.1111/iej.12800. [DOI] [PubMed] [Google Scholar]
- 157.Ahmed HMA, Dummer PMH. A new system for classifying tooth root and canal anomalies. Int Endod J. 2018;51(4):389–404. doi: 10.1111/iej.12867. [DOI] [PubMed] [Google Scholar]
- 158.von Fraunhofer JA. Research writing in Dentistry. John Wiley &Sons; 2009:13–34. [Google Scholar]
- 159.Vähänikkilä H, Tjäderhane L, Nieminen P. The statistical reporting quality of articles published in 2010 in five dental journals. Acta Odontol Scand. 2015;73(1):76–80. doi: 10.3109/00016357.2014.954612. [DOI] [PubMed] [Google Scholar]
- 160.Bueno MR, Estrela CRA, Granjeiro JM, Sousa-Neto MD, Estrela C. Method to determine the root canal anatomic dimension by using a new cone-beam computed tomography software. Braz Dent J. 2019;30(1):3–11. doi: 10.1590/0103-6440201902462. [DOI] [PubMed] [Google Scholar]
- 161.Gambarini G, Ropini P, Piasecki L, Costantini R, Carneiro E, Testarelli L, et al. A preliminary assessment of a new dedicated endodontic software for use with CBCT images to evaluate the canal complexity of mandibular molars. Int Endod J. 2018;51(3):259–68. doi: 10.1111/iej.12845. [DOI] [PubMed] [Google Scholar]
- 162.Karaman GT, Onay EO, Ungor M, Colak M. Evaluating the potential key factors in assessing the morphology of mesiobuccal canal in maxillary first and second molars. Aust Endod J. 2011;37(3):134–40. doi: 10.1111/j.1747-4477.2010.00240.x. [DOI] [PubMed] [Google Scholar]
- 163.Lu TY, Yang SF, Pai SF. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod. 2006;32(10):932–6. doi: 10.1016/j.joen.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 164.Iino Y, Ebihara A, Yoshioka T, Kawamura J, Watanabe S, Hanada T, et al. Detection of a second mesiobuccal canal in maxillary molars by swept-source optical coherence tomography. J Endod. 2014;40(11):1865–8. doi: 10.1016/j.joen.2014.07.012. [DOI] [PubMed] [Google Scholar]
- 165.Ahmed HM. Anatomical challenges electronic working length determination and current developments in root canal preparation of primary molar teeth. Int Endod J. 2013;46(11):1011–22. doi: 10.1111/iej.12134. [DOI] [PubMed] [Google Scholar]
- 166.Ahmed HMA, Musale PK, El Shahawy OI, Dummer PMH. Application of a new system for classifying tooth root and canal morphology in the primary dentition. Int Endod J. 2020;53(1):27–35. doi: 10.1111/iej.13199. [DOI] [PubMed] [Google Scholar]
- 167.Fumes AC, Sousa-Neto MD, Leoni GB, Versiani MA, da Silva LA, da Silva RA, et al. Root canal morphology of primary molars:a micro-computed tomography study. Eur Arch Paediatr Dent. 2014;15(5):317–26. doi: 10.1007/s40368-014-0117-0. [DOI] [PubMed] [Google Scholar]
- 168.Nagendrababu V, Chong BS, McCabe P, Shah PK, Priya E, Jayaraman J, et al. PRICE 2020 guidelines for reporting case reports in Endodontics:explanation and elaboration. Int Endod J. 2020;53(7):922–47. doi: 10.1111/iej.13300. [DOI] [PubMed] [Google Scholar]
- 169.Nagendrababu V, Duncan HF, Fouad AF, Kirkevang LL, Parashos P, Pigg M, et al. Preferred Reporting items for OBservational studies in Endodontics (PROBE) guidelines:a development protocol. Int Endod J. 2020;53(9):1199–203. doi: 10.1111/iej.13318. [DOI] [PubMed] [Google Scholar]
- 170.Nagendrababu V, Murray PE, Ordinola-Zapata R, Peters OA, Rôças IN, Siqueira JF Jr, et al. A protocol for developing reporting guidelines for laboratory studies in Endodontology. Int Endod J. 2019;52(8):1090–5. doi: 10.1111/iej.13123. [DOI] [PubMed] [Google Scholar]
- 171.Nagendrababu V, Duncan HF, Bjørndal L, Kvist T, Priya E, Jayaraman J, et al. PRIRATE 2020 guidelines for reporting randomized trials in Endodontics:explanation and elaboration. Int Endod J. 2020;53(6):774–803. doi: 10.1111/iej.13304. [DOI] [PubMed] [Google Scholar]
- 172.Nagendrababu V, Kishen A, Murray PE, Nekoofar MH, de Figueiredo JAP, Priya E, et al. Preferred reporting items for animal studies in endodontology:a development protocol. Int Endod J. 2019;52(9):1290–6. doi: 10.1111/iej.13125. [DOI] [PubMed] [Google Scholar]