

Abstract
Introduction
In December 2019, cases of pneumonia, a new type of corona virus (SARS‐CoV‐2), began to be reported in Wuhan, China. We aimed to evaluate changes in sexual behaviour of men in the Covid‐19 outbreak in Turkey.
Material‐Method
In our cross‐sectional and descriptive study, an online questionnaire evaluating sexual habits during the Covid‐19 outbreak was conducted on the men living in the Western Black Sea Region between 8 and 25 June6 2020. In the questionnaire, questions were asked to evaluate the sociodemographic data of the participants, their comprehensive medical history, their sexual preferences, their family and social life during the Covid‐19 outbreak, their concerns about Covid‐19 and their changes in their sexual behaviour after the Covid‐19 outbreak.
Results
A total of 536 participants with mean age of 38.6 ± 10.3 years were included in the study. 23.9% (128) respondents stated that they had the fear of transmitting Covid‐19 to their partner during sexual intercourse. It was observed that 19.4% (104) of the participants developed a fear of Covid‐19 transmission from her sexual partner during the relationship. While the number of weekly sexual intercourse of the participants before the pandemic was 2.34 ± 1.35, this number was found to be 1.54 ± 1.45 during the epidemic period (P = .001).
Conclusion
The fear of infection and transmission of the disease to the partner that occurs during the Covid‐19 pandemic manifests itself in the form of a decrease in the frequency and quality of sexual intercourse.
What’s known
Fear of contagion and catching disease causes anxiety. Anxiety has an effect on people's sexual health.
What’s new
There are not enough publications on the effect of covid‐19 on sexual habits. During pandemic periods, sexual health of people is negatively affected.
1. INTRODUCTION
In December 2019, cases of pneumonia, whose causative agent was a new type of corona virus (SARS‐CoV‐2), were reported in Wuhan, China. 1 , 2 The World Health Organization (WHO) named the disease caused by this new type of corona virus as Covid‐19. 3 Because of the spread of Covid‐19 to many countries, WHO reported on 30 January 2020 that the outbreak was an international alarming emergency public health situation. 4 According to the WHO data, Covid‐19 infected about 12 million people in a total of 216 countries around the world, causing more than 545 000 deaths as of the date of writing this article. 5 In many countries, to prevent the spread of disease, many preventive measures have been taken such as restriction of entries to and exits from the country, closing schools, postponement of sports competitions, interrupting production except for important business lines and enforcement of home quarantine. According to the Ministry of Health of the Republic of Turkey data, Covid‐19 infected >200 000 people in Turkey and killed 5200 people. 6
Covid‐19 caused physical damage to individuals and negatively affected the society's mental health. During the pandemic, psychosocial stress factors such as being a health threat to one's self or loved ones may develop. 7 In the studies conducted, because of concerns about Covid‐19 transmission, sleep quality deteriorated, likelihood of developing anxiety and depressive symptoms increased and positive emotions and life satisfaction decreased. 8 , 9 , 10 Anxiety and depression play an important role in the development of sexual dysfunction 11 ; however, in the process of pandemics, the effects of both social isolation practices and anxiety that may occur in people on male sexual behaviour are not fully known. In the literature, there are limited studies to assess the sexual behaviour of people in cases of natural disasters affecting the whole world such as pandemics. For this purpose, we aimed to evaluate the changes in the sexual behaviour of men in the Western Black Sea Region of Turkey after the Covid‐19 outbreak.
2. MATERIALS AND METHODS
In this cross‐sectional and descriptive study, an online survey evaluating sexual habits during the Covid‐19 epidemic was applied to men living in the Western Black Sea Region from 8 to 25 June 2020.
The preliminary assessment of the survey was applied to 20 sexually active voluntary patient relatives who were admitted to the urology outpatient clinic to test comprehensibility of the questions. After correcting missing parts and errors, the survey was organised as four sections with 47 open and closed‐ended questions. In the survey's first part, sociodemographic data and extensive medical resume, habits and sexual preference were questioned. For this purpose, age, profession, the city where the patient resides, presence of chronic or psychological disorders, partner's age/profession/health status, drugs used and surgeries undergone were asked as open‐ended questions. Educational status of participants (literate/primary school/high school/university/master's degree), marital status (married, single, widow and divorce/separate), number of children (none, 1, 2, ≥3), sexual preference (homosexual/heterosexual/bisexual), income level (poor, moderate, good and very good) and partner's education status (literate/primary school/high school/university/master's degree) were questioned. Other questions (family type, relationship problem with partner and cigarette/alcohol/drug use) were designed as closed‐ended questions where the answer would be ‘yes’ or ‘no’.
In the second part of the survey, the participants were asked questions regarding their family and social life and their concerns about Covid‐19 during the Covid‐19 outbreak. The participants were asked questions regarding the sources of access to information about Covid‐19 (internet/television/social media/newspaper/other persons), the interest areas they most frequently engaged in during the time spent at home because of social isolation (internet/television/book/hobby/family members/distance working–education), and the reasons (work/shopping/sports/other) why people left home during the epidemic and how often they left home (0‐7/wk). Other questions were designed as closed‐ended questions (presence of Covid‐19‐infected person in the family, restriction in socialisation during the epidemic, rules of social distance at home, fear of infecting family members with Covid‐19) with an answer of ‘yes’ or ‘no’.
In the survey's third part, the participants were questioned in terms of changes in their sexual behaviour after the Covid‐19 outbreak. For this purpose, they were questioned regarding the frequency of sexual intercourse (0‐7), the use of drugs that increase sexual potency (yes/no), erection problems (yes/no) and whether or not they sought medical advice because of sexual problems (yes/no) in the 6‐month periods before and during the pandemic. Furthermore, they were questioned whether they had the fear of infecting their partner with Covid‐19 (yes/no) or of being infected by Covid‐19 by their partner (yes/no), and whether they avoided sexual intercourse because of fear of transmission (yes/no) or rejection (yes/no) by their partner in the pandemic process.
In the last part of the survey, the participants took the Turkish version of the International Index of Erectile Function‐5 (IIEF‐5) form, which independently evaluated the 6‐month period before the Covid‐19 outbreak and the epidemic period. 12
This study was created using a Google survey‐based form because of social isolation rules and transmitted online to the followers of the researches via their social networks. Each participant was then asked to share the survey form with their own groups via their personal social networks. The survey form was anonymously planned without questioning the persons’ identity. When the survey link was clicked, voluntary informed consent screen was first opened. The voluntary consent screen was designed to provide information about researchers, the purpose of the study and duration of the survey. It was clearly stated on the consent screen that personal data will remain confidential. After this screen was confirmed, the survey form was opened. At the end of the survey, the participants were offered the option to change the answers by clicking the “back” button. The survey was then designed to be uploaded to the system after the participant registered the email address in the system and responded to mandatory questions. Heterosexual male individuals aged 18‐65 with a history of sexual activity were included in the study. Surveys with the same or similar email record were not evaluated. Those participants who had severe erectile dysfunction, uncontrolled systemic disease or mental disorders were taking drugs that affect sexual function, had alcohol or drug addiction, hepatitis B/C or HIV infection before the pandemic, and those who had Covid‐19 positive or suspicion of the disease in themselves or their partner during the pandemic period were excluded from the study. Moreover, individuals with pregnant sexual partners, having problems with their partner and living in different regions were not included in the study.
Statistical analysis was evaluated using IBM SPSS Statistics 26 software. The conformity of the digital data to normal distribution was evaluated by the Kolmogorov–Smirnov test, the Chi‐square test was used to compare categorical data and the Mann–Whitney U test was performed in comparison of bilateral groups who did not show normal distribution such as marital status, having children, family type and fear of Covid‐19 transmission from partner to partner. The Wilcoxon test was performed in comparison of sexual frequency and IIEF scores before and during Covid‐19. The Negative Binominal Regression analysis was performed for analyzing factors affecting sexual frequency and IIEF scores. Numerical data were then expressed as mean ± standard deviation and non‐numeric data as %. The values P < .05 were considered to be statistically significant.
The study was conducted with the approvals of the Scientific Research Council of the Ministry of Health of the Republic of Turkey (2020‐05‐14T19‐18‐51) and the Karabük University Non‐Interventional Clinical Studies Ethics Council (2020/237).
3. RESULTS
It was determined that 738 participants approved the informed consent form by clicking on the survey link, and then started the survey. However, 611 (82.7%) respondents completely completed the survey. Total of 536 participants were included in the study. The flow chart of the participants’ selection is listed in Figure 1. The mean age of the participants was 38.6 ± 10.3. The mean age of the sexual partners of the participants was 32.2% ± 9.8%, while the educational status of these people was first‐secondary education with 41.6%, and university‐master degree with 58.4%. The sociodemographic data of the participants are given in Table 1.
FIGURE 1.
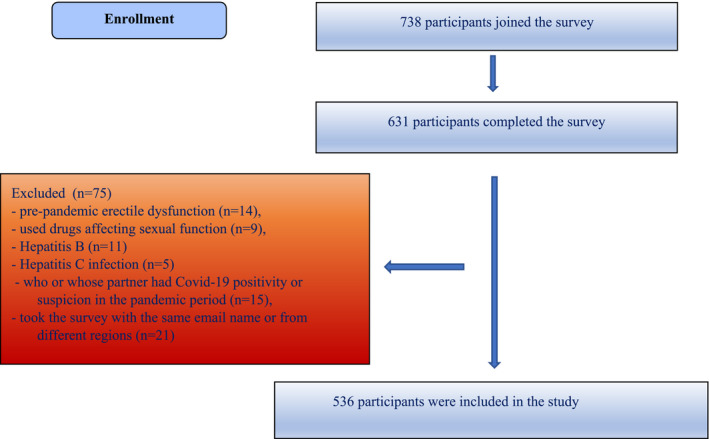
Flowchart
TABLE 1.
Demographic characteristics of participants (N = 536)
| Variables | Total (%) |
|---|---|
| Age (y) | |
| 18‐24 | 41 (7.6) |
| 25‐34 | 133 (24.8) |
| 35‐44 | 207 (38.6) |
| 45‐54 | 106 (19.8) |
| 55‐64 | 49 (9.1) |
| Marital status | |
| Married | 404 (75.4) |
| Single | 111 (20.7) |
| Divorced | 18 (3.4) |
| Widow | 3 (0.5) |
| Education status | |
| Literate | 10 (1.8) |
| Primary school | 56 (10.5) |
| High school | 116 (21.7) |
| University | 276 (51.5) |
| Master's Degree | 78 (14.5) |
| Income level | |
| Poor | 47 (8.8) |
| Moderate | 241 (45) |
| Good | 172 (32.1) |
| Very good | 76 (14.1) |
| Partner's Job | |
| Yes | 262 (48.9) |
| No | 274 (51.1) |
| Number of children | |
| None | 144 (26.9) |
| 1 | 128 (23.9) |
| ≥2 | 264 (49.2) |
| Family type | |
| Core | 483 (90.1) |
| Traditional | 53 (9.9) |
| Smoking | |
| Yes | 264 (49.3) |
| No | 272 (50.7) |
| Alcohol use | |
| Yes | 214 (39.9) |
| No | 322 (60.1) |
Note that 71% of the participants followed the information on Covid‐19 via Internet, while the rest of the participants were watching television and reading newspapers. The activities of the participants during the time when they had to stay at home because of social isolation rules are seen in Figure 2. Moreover, 81.3% of the respondents (n = 436) reported that their social life was restricted throughout the pandemic. During the pandemic, only 3.2% (n = 17) of the participants never left the house, and 42.4% (n = 237) of the respondents stated that they went out every day. Furthermore, 60.4% (n = 324) of the participants expressed the fear they experienced about infecting family members with Covid‐19. However, it was observed that only 32.9% (n = 212) of the participants adhered to the social distance rules at home.
FIGURE 2.
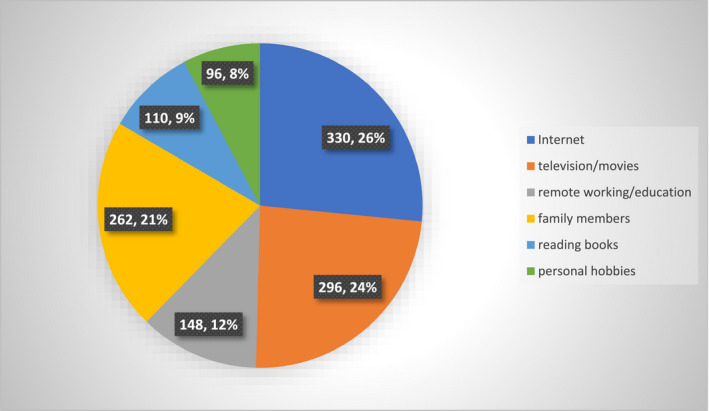
Interest areas of participants at home during the outbreak
Moreover, during sexual intercourse, 23.9% (128) of respondents expressed that they experience fear of transmitting Covid‐19 to their partner; this fear was most developed in individuals aged 25‐34 years (P = .025). The fear of infecting the partner was similar in married (23.5%) and single (25%) people (P = .728). Furthermore, 19.4% (104) of the participants developed fear of getting infected with Covid‐19 by their partner during intercourse. Moreover, individuals aged 18‐24 experienced this fear the least (12.2%), while individuals aged 25‐34 experienced it the most intensively (33.8%) (P < .001). The fear of Covid‐19 infection during sexual intercourse was reported to develop in 16.6% of married individuals (n = 67) and 28% (n = 37) of single participants (P = .004). Furthermore, 10.1% (n = 54) of the participants expressed that they were rejected by their partners from time to time because of the fear of Covid‐19 infection. Moreover, 29.5% (n = 158) of the participants stated that their partners did not agree to have sexual intercourse because of the fear of Covid‐19 infection in different periods of the pandemic. The mean weekly sexual intercourse number of the participants before the pandemic was 2.34 ± 1.35, while the number was 1.54 ± 1.45 during the epidemic period (P = .001). Table 2 lists the factors affecting the frequency of sexual intercourse.
TABLE 2.
Factors affecting the frequency of sexual intercourse after covid‐19 outbreak
| Variables |
Univariante analysis P value |
Multivariante analysis P value 95% CI |
|---|---|---|
| Age | <.001 a | |
| Marital status | <.001 b | |
| Education status | .859 a | |
| Income level | .075 a | |
| Having children | <.001 b | |
| Family type | .442 b | |
| Fear of infecting partner with covid‐19 | .015 b | .045 (0.654‐0.995) c |
| Fear of getting infected by partner with covid‐19 | .004 b | |
| Previous number of sexual intercourse | <.001 | <.001 (1.563‐2.460) c |
Kruskal‐Wallis test.
Mann‐Whitney U test.
Negative binominal regression analysis.
The total IIEF‐5 scores was 19.90 ± 5.1 before the pandemic and 19.31 ± 5.88 after the pandemic (P = .015). The total IIEF‐5 scores of married were 20.05 ± 4.96 before Covid‐19 and 19.55 ± 5.61 during the pandemic (P = .156). For singles, this score was 19.42 ± 5.85 before the pandemic and 18.60 ± 6.6 during the epidemic period (P = .026). The data obtained from answers to the IIEF‐5 questions for before and after the pandemic are shown in Table 3.
TABLE 3.
IIEF‐5 values before and after pandemic
| IIEF‐5 |
Pre‐pandemic Median (min/max) |
During pandemic Median (min/max) |
P value a |
|---|---|---|---|
| Self‐confidence in having an erection | 5 (1‐5) | 5 (1‐5) | .085 |
| To be able to have an erection | 4.5 (1‐5) | 4 (1‐5) | <.001 |
| To be able to maintain an erection | 4 (1‐5) | 4 (1‐5) | <.001 |
| To be able to maintain an erection until the end of sexual intercourse | 4 (1‐5) | 4 (1‐5) | <.001 |
| Sexual satisfaction | 5 (1‐5) | 5 (1‐5) | .041 |
| Total Score | 21 (8‐25) | 21 (5‐25) | .015 |
Wilcoxon test.
There were 160 (29.8%) health workers among the participants. Fear of Covid‐19 infection during sexual intercourse affected 37 (23.1%) health workers and 67 (17.8%) individuals from other professional groups (P = .155). Fear of infecting their partner with Covid‐19 during sexual intercourse developed in 48 (30%) health workers and 80 (21.3%) participants from other professional groups (P = .030). The number of weekly sexual intercourse in healthcare workers was 2.66 ± 1.48 prior to the pandemic and 1.78 ± 1.60 during the epidemic (P < .001). The IIEF‐5 total scores were 21.98 ± 3.56 before the Covid‐19 period and 21.18 ± 4.75 during the pandemic (P = .010).
4. DISCUSSION
After the first Covid‐19 case was identified in Turkey on 11 March 2020, a number of preventive measures were taken by the central government. These measures included restricting people under 18 and over 65 years of age from going outdoors, imposing total curfew on holidays, reduction in production, working from home, closure of restaurants and entertainment venues and mandatory mask applications. WHO acknowledges that restrictive measures taken by governments can lead to anger, stress, anxiety, agitation and withdrawal in humans. 13 In some studies, during the Covid‐19 pandemic, people develop different levels of anxiety, and related behavioural changes are observed. 14 In our study, we evaluated the effects of social restrictions and quarantine on male sexual behaviour.
Our study is the first survey study examining sexual behaviour changes in men before and during the Covid‐19 pandemic in Turkey. In our study, the vast majority of the participants had significant restrictions in their social lives, and they spend most of their time in a digital environment. While the fear of infecting family members with Covid‐19 during normal everyday life activities increased in the vast majority of participants, they did not follow rules of social distancing at home. Although it was reported in a study that the virus was isolated from semen samples in six patients, there is no clear data in the literature that Covid‐19 is sexually transmitted. 15 In our study, the vast majority of respondents did not experience fear of Covid‐19 transmission during sexual intercourse, and this fear developed less often in the married individuals. Similarly, the majority of respondents did not experience the fear of infecting their partner with the disease, and the proportion was similar among single and married individuals. For healthcare workers, the fear of being infected during sexual intercourse was similar to other individuals of society, but interestingly the fear of infecting their partners they experienced was more than other individuals. It was probably because there is a higher possibility for healthcare workers to encounter with the virus compared to individuals in other parts of society in their daily work lives, and their instinctual behaviour to protect their partners from the disease.
Li et al evaluated changes in the sexual behaviour of women and men aged 18‐45 years during the Covid‐19 outbreak through an online survey. 16 In this study, 25% of the respondents had a decrease in sexual desire, and this decrease was more in men than women (P = .001). In both sexes, a decrease in the number of sexual partners was reported. There was a decrease in the sexual intercourse frequency in 37% of the respondents. In the same study, the participants avoided risky sexual behaviour and there was a decrease in sexual satisfaction in 32% of the men. In another online survey conducted with individuals with good education level in Bangladesh, India and Nepal region, no significant difference was detected in the sexual activities of the participants before and during the pandemic. 17 An online survey conducted in UK reported that during the Covid‐19 pandemic, 39.9% of the respondents engaged in sexual activity at least once a week. 18 In this study, the mean number of weekly sexual intercourse was 1.75. Moreover, during the pandemic, the number of weekly sexual intercourse was reported as 3.23 in men and 0.88 in women. Because of this study, the number of sexual intercourses was correlated positively with male gender, young age, being married, having a high income level and alcohol consumption.
Yuksel et al 19 reported in their study evaluating the effect of the Covid‐19 pandemic on female sexual behaviour that the frequency of weekly sexual intercourse was 1.9 ± 0.9 before the pandemic and 2.4 ± 0.9 (P = .001) during the pandemic. In the same study, despite this increase in the frequency of weekly sexual intercourse, there was a significant decrease in sexual arousal, orgasm and satisfaction levels during the pandemic compared to the prepandemic period. In this study, during the pandemic period, the desire to become pregnant decreased and there was an increase in menstrual disorders.
In our study, we reported that during the Covid‐19 pandemic, the number of weekly sexual intercourse and the level of satisfaction from sexual intercourse were significantly reduced. We found that the frequency of weekly sexual intercourse during the pandemic period is associated with age, marital status, having children and fear of Covid‐19 infection/transmission during intercourse. In the negative binomial regression analysis, the number of weekly sexual intercourse during the pandemic is positively correlated with the number of sexual intercourse and negatively correlated with the fear of infecting their partner before the pandemic.
In our study, we observed that the total IIEF‐5 score decreased during the pandemic. When the IIEF‐5 questions were evaluated within themselves, there was no difference in participants’ self‐confidence in having and maintaining an erection before and during the pandemic. Compared to the prepandemic period, the ability of the participants to have and maintain an erection necessary for penetration until the end of sexual intercourse during the pandemic period decreased. During the epidemic, the level of satisfaction from sexual intercourse was significantly reduced compared to the prepandemic period. Accordingly, we observed that both weekly sexual intercourse numbers and total IIEF‐5 scores decreased in the healthcare workers.
Because our study is cross‐sectional and conducted in a localised area, it is not possible to generalise changes in sexual behaviour of men during the pandemic with this study. Moreover, the reliability of their answers is reduced because the study was conducted online, the questions were not directed face to face and the participants’ partners were not interviewed. Furthermore, it is among the limitations of the study that duplicate entries were verified only by e‐mail address declared by the participant and not by their IP addresses.
5. CONCLUSION
During the Covid‐19 pandemic, there is a fear of infecting or getting infected with the disease in individuals. The fear experienced manifests itself in the form of a decrease in the number and quality of sexual intercourse of male individuals. These results need to be supported by studies involving a larger sample size and different regions.
DISCLOSURE
The authors declare that there is no conflict of interest.
Baran O, Aykac A. The effect of fear of covid‐19 transmission on male sexual behaviour: A cross‐sectional survey study. Int J Clin Pract.2021;75:e13889. 10.1111/ijcp.13889
REFERENCES
- 1. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497‐506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:507‐513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. WHO . Novel Coronavirus–China; 2020. 2020. https://www.who.int/csr/don/12‐january‐2020‐novel‐coronavirus‐china/en/. Accessed January 12, 2020.
- 4. Mahase E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ. 2020;368:m408. [DOI] [PubMed] [Google Scholar]
- 5. World Health Organization . Coronavirus disease (COVID‐19) pandemic; 2020. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019
- 6. Türkiye'deki Covid‐19 Güncel Durum; 2020. https://covid19.saglik.gov.tr/
- 7. Taylor S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease. Newcastle upon Tyne, UK: Cambridge Scholars Publishing; 2019. [Google Scholar]
- 8. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID‐19 outbreak in China: a web‐based cross‐sectional survey. Psychiatry Res. 2020;288:112954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Sher L. COVID‐19, anxiety, sleep disturbances and suicide. Sleep Med. 2020;70:124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Choi EPH, Hui BPH, Wan EYF. Depression and Anxiety in Hong Kong during COVID‐19. Int J Environ Res Public Health. 2020;17:3740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hedon F. Anxiety and erectile dysfunction: a global approach to ED enhances results and quality of life. Int J Impotence Res. 2003;15:S16‐S19. [DOI] [PubMed] [Google Scholar]
- 12. Turunç T, Deveci S, Güvel S, Peşkircioğlu L. The assessment of Turkish validation with 5 question version of International Index of Erectile Function (IIEF‐5). Turk J Urol. 2007;33:45‐49. [Google Scholar]
- 13. World Health Organisation . Mental health and psychosocial considerations during the COVID‐19 outbreak 2020; 2020. Available at: https://www.who.int/docs/default‐source/coronaviruse/mental‐health‐considerations.pdf. Accessed March 18, 2020.
- 14. Barber SJ, Kim H. COVID‐19 Worries and behavior changes in older and younger men and women. J Gerontol B Psychol Sci Soc Sci. 2020;76:e17–e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Li D, Jin M, Bao P, Zhao W, Zhang S. Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Network Open. 2020;3:e208292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Li W, Li G, Xin C, Wang Y, Yang S. Challenges in the practice of sexual medicine in the time of COVID‐19 in China. J Sex Med. 2020;17:1225–1228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Arafat SMY, Alradie‐Mohamed A, Kar SK, Sharma P, Kabir R. Does COVID‐19 pandemic affect sexual behaviour? A cross‐sectional, cross‐national online survey. Psychiatry Res. 2020;289:113050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Jacob L, Smith L, Butler L, et al. COVID‐19 social distancing and sexual activity in a sample of the British Public. J Sex Med. 2020;17:1229‐1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Yuksel B, Ozgor F. Effect of the COVID‐19 pandemic on female sexual behavior. Int J Gynaecol Obstet. 2020;150:98‐102. [DOI] [PMC free article] [PubMed] [Google Scholar]