

Abstract
The new coronavirus (SARS‐CoV‐2) appearance in Wuhan, China, did rise the new virus disease (COVID‐19), which spread globally in a short time, leading the World Health Organization to declare a new global pandemic. To contain and mitigate the spread of SARS‐CoV‐2, specific public health procedures were implemented in virtually all countries, with a significant impact on society, making it difficult to keep the regular practice of physical activity. It is widely accepted that an active lifestyle contributes to the improvement of general health and preservation of cardiovascular, respiratory, osteo‐muscular and immune system capacities. The positive effects of regular physical activity on the immune system have emerged as a pivotal trigger of general health, underlying the beneficial effects of physical activity on multiple physiological systems. Accordingly, recent studies have already pointed out the negative impact of physical inactivity caused by the social isolation imposed by the public sanitary authorities due to COVID‐19. Nevertheless, there are still no current narrative reviews evaluating the real impact of COVID‐19 on active lifestyle or even discussing the possible beneficial effects of exercise‐promoted immune upgrade against the severity or progression of COVID‐19. Based on the consensus in the scientific literature, in this review, we discuss how an exercise adherence could adequately improve immune responses in times of the ‘COVID‐19 Era and beyond’.
Keywords: COVID‐19, inflammaging, lifestyle, physical inactivity, SARS‐CoV‐2, vaccination
1. BRIEF SUMMARY OF THE COVID‐19 ERA AND ITS IMPACT ON THE LIFESTYLE
On 11 March 2020, the World Health Organization (WHO) officially declared that the world was facing a pandemic situation caused by the new coronavirus (SARS‐CoV‐2), a virus identified in December 2019 after the sequencing of clinical samples from a group of patients presenting pneumonia‐like symptoms in Wuhan, China. 1 By phylogenetic analysis, this new coronavirus (nCoV‐2019) was allocated into the genus Betacoronavirus, in which SARS‐CoV and MERS‐CoV are also found and, for this reason, the name SARS‐CoV2 was coined. 2 It is worth mentioning that the disease caused by SARS‐CoV‐2 is currently called ‘coronavirus disease‐2019’ or simply COVID‐19. 1
Among WHO recommendations, social isolation and/or social distance become mandatory and must be adopted by the governments worldwide (with exceptions) to minimize the SARS‐CoV‐2 spread. 3 Currently, there is no doubt that the quarantine period is of utmost importance to control the rapid viral infection spread. 1 However, as another side of the same coin, the sudden onset of a quarantine period not only implies a rapid change in people's lifestyles but also can impact the health of these isolated persons, since it favours impairment in dietary habits, 4 changes in psychosocial behaviour 5 and reduced levels of physical activity in all age individuals. 6 In this regard, it is noteworthy to emphasize that one of the most impacted habits in the current quarantine were those associated with regular physical exercise (rPE), including indoor or outdoor practice. 7 , 8 , 9 Corroborating these pieces of information, recent studies demonstrated that during COVID‐19 confinement, the overwhelming majority of the population declared not only a significant reduction of daily self‐reported physical activity as well as an increase in sedentary time. 9 , 10 , 11 , 12
These studies showed that, in a general way, the confinement imposed by the pandemic led to an expressive increase of sedentary behaviour with an elevation in the time watching TV (72.3%), logging to social media (81.9%) and using electronic gadgets (82.7%). These records are accordingly in opposition to the reduction of 40%‐60% of time spent in some aerobic exercises (eg walking and jogging), as well as in the practice of rPE at different intensities, either vigorous (≤15%) or moderate (≤30%), both men (21%) and women (9%) individuals. 11 , 12
There is a consensus in the scientific literature that maintaining an active lifestyle with rPE benefits populations of different age groups. 13 , 14 Since the rPE is closely associated with an establishment of favourable health status for the population, it is very important to define some points related to its practice by individuals. In this sense, whilst the performance of a single bout of exercise is named acute exercise, the performance of repeated bouts of exercise during a period of time is known as rPE, exercise training or chronic exercise. Moreover, the benefits of rPE are dependent on exercise intensity, which are defined as low [<40% of maximal oxygen uptake capacity (VO2max)], moderate (40%‐69% VO2max), vigorous or high (70%‐90% VO2max) and very high intensity, when its performed about above 90% VO2max. 15
In order to contextualize the benefit of rPE on human health, one should focus on the accurate and high responsiveness of the immune system (IS) upon rPE. 16 , 17 From this point, one of the topics that have sparked a worldwide discussion was the effectiveness of maintaining an active lifestyle in order to strengthen the IS, which is of vital importance during the ongoing pandemic of COVID‐19.
2. SYNOPSIS OF EVIDENCE ON rPE AND IMMUNITY
Many clinical studies from the 70s were designed to clarify how rPE could affect the human IS. 16 The significant breakthroughs in this field were properly compiled in the so‐called ‘Exercise Immunology’, a research field that grew exponentially in the last decades, allowing health and sports professionals to generally state, over the years, that the rPE has beneficial effects for IS, leading to the overall improvement of human health, independently of age. 18 Further, there are several studies confirming the benefits provided by rPE on the immune response, becoming a trigger and a sustainer of a healthy condition. 5 In association with rPE, the nutritional status of subjects can also influence the immune response. 19 Taken together, these aspects are being recently considered as the corollary of the healthy ageing condition. 20
Based on general health guidelines, rPE composed of a moderate (40%‐69% VO2max, 30 to 60 minutes, 3‐5 days/wk) to relatively intense volumes (70 to 85% VO2max, 30 to 45 minutes, 2‐3 days/wk) are directly associated with a lower upper respiratory tract infections (URTI) incidence. 15 , 16 This advance led to the ‘J‐curve’ hypothesis, in which the URTI incidence is reduced in the practitioners of a moderate‐intensity rPE regime, but increases again following periods of strenuous/intensive training or prolonged competitions. In these latter situations, URTI incidence is higher than that observed in sedentary people. 16 Higher URTI incidence in overtraining conditions could be explained by the fact that an excessive exercising session may exceed the body´s homeostasis limits, either acute or chronically, leading to a transient immunosuppressant status, known as the ‘open‐window’ opportunity. 21 In summary, whereas rPE performed at moderate intensities stimulates both cellular and humoral immunity and, thus, could significantly limit the risk of infections, exercise performances at high intensities could impose a transitory immunosuppression status that would jeopardize practicioners health. 16 , 21
As aforementioned, beyond the exercise intensities, both acute and chronic exercises could also significantly impact people´s health. 15 In fact, exercise immunology researchers have focused on the acute and chronic effects of exercise on the IS, looking particularly at the immune cells and factors involved in the innate and adaptive responses, aiming enhanced immunosurveillance and reduced systemic inflammation. 16 For instance, both types of acute and chronic exercises can act as promoters of the continuous exchange of leukocytes (mainly Natural Killers cells, neutrophils, monocytes and lymphocytes), between circulation and specific tissues, such as spleen, lung and skeletal muscles, to improve immune cellular clearance and functions. 13 , 22 Acute and chronic exercise also act as inducers of stress hormones, like cortisol, that down‐regulates excessive inflammation, which, in fact, represents a double‐edge sword regarding immune efficiency. 23 As observed in Figure 1, studies have shown recurrent patterns of change, both in acute and chronic exercise, with age, sex and magnitude of exercise modulating these specific responses.
FIGURE 1.
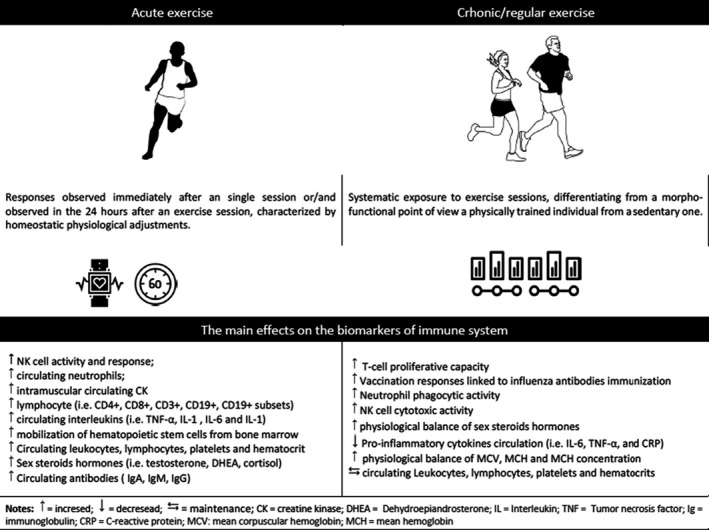
General evidence summary of acute and chronic exercise interventions induced changes on several cell subsets and biomarkers of immune function. 12 , 18 , 19 Acute moderate‐to‐vigorous exercise is an important adjuvant to arouse the IS. In the same direction, chronic physical exercise is capable of regulating the IS and attenuate the onset of negative pro‐inflammatory effects. For this review purposes, moderate‐to‐vigorous physical exercises are differentiated using an intensity threshold of 60% of the oxygen update and heart rate reserve, and a medium of duration threshold of 60 minutes 12
In this way, our group and colleagues have been consistently observing that lifelong training helps to maintain an adequate balance of pro‐inflammatory, such as interleukin (IL)‐8 and IL‐1β, and anti‐inflammatory cytokines, such as IL‐1ra and IL‐4. 24 In addition, we have also shown that in both experimental (mice) and clinical (human) studies, the maintenance of a controlled and anti‐inflammatory environment by the rPE, particularly in the respiratory airways, was able to significantly reduce pulmonary injury and the occurrence of upper respiratory airways symptoms after an exhaustive exercise session, such as running a marathon. 21 , 22 , 23 , 24 , 25 , 26
Also noteworthy is the fact that rPE apparently increase the levels of anti‐viral immunity markers—increased dendritic cell maturation, higher activation and proliferation of T cells, and proper balance of T‐helper responses—which can optimize the immune response both locally and systemic in physically and cognitively frail older people. 23 , 27 , 28 , 29 , 30 , 31
To have all the exercise‐related alterations occurring, a whole set of integrated cell signalling cascades are concomitantly triggered. 18 Consequently, complex and intricate molecular events, including transcription factors activation, mRNA transcription and protein synthesis, are all activated in almost all organs and tissues, with emphasis in the contractile skeletal muscles. 32 , 33 Among all molecular and cellular systems activated by exercises, the key role of cytokines secreted by the muscle, also named myokines, is of massive relevance. 34 Systemic elevations of myokines, particularly of interleukin‐6 (IL‐6), not only can optimize lipid and glucose metabolism but can also exert indirect anti‐inflammatory effects by promoting the secretion of classical anti‐inflammatory cytokines, IL‐1ra and IL‐10, with concurrent inhibition of TNF‐α action. 6
This is one of the most important myokines‐driving anti‐/pro‐inflammatory regulation mechanisms recently illustrated by several authors as the yin‐yang relationship. 35 However, we cannot exclude the key role of the redox signals hydrogen peroxide (H2O2) and nitric oxide (NO) in adjusting the extension of oxidative stress and the inflammation processes following any type of exercise. 36 Both H2O2 and NO are reactive oxygen and nitrogen species (ROS/RNS) extensively produced in contractile muscles, vascular endothelium, cardiomyocytes (heart), lungs, plasma, etc during exercise, that, due to their low reactivity and high diffusibility in aqueous systems, could exert long‐range redox signalling effects in order to provide a proper and overall antioxidant, inflammatory and cytoprotective responses against potentially harmful oxidative stress. 37 Interestingly, the in situ antioxidant capacity of all those aforementioned sites of ROS/RNS production will exactly determine the intensity of the integrated redox signal—here, understand, the effective concentration of H2O2 and NO produced—that will emanate from the active cells and tissues during exercise. Therefore, genetic issues, but mostly, adequate nutritional programs, gain major relevance on discussing immunological efficiency upon rPE, especially regarding elderly populations. 38 , 39
3. FROM CHILDHOOD TO OLD AGE: rPE IMPACTS ON IMMUNE SYSTEM RESPONSE
Genetic, metabolic, environmental, anatomical, physiological, nutritional and microbiological factors, as well as those related to the rPE, are some of the useful modulators of the immune and inflammatory responses upon exercise. 40 However, the ‘age factor’ is the prominent one that gives the IS its very unique endocrine and metabolic characteristics that distinguishably affects, in a direct and indirect way, the immune responsiveness of practitioners. 16 The IS development involves two parts: the Innate Immunity, which brings the background (genetic) information ready to act and protect the newborn 41 ; and the Acquired Immunity, which is developed throughout the individual's life, based on continuous exposure to immune‐eliciting factors. 42 Therefore, the IS will achieve its functional peak after a reasonably long life period in order to acquire additional immune repertoire against recurrent pathogens present in outer environment. 41 , 42
However, it is notorious that newborns, toddlers, and infant individuals share higher susceptibility to infections with the elderly populations, which is represented by the ‘inverted U‐shape’ curve of immune responsiveness capacity with age in the human population. 43 Significant alterations in the action potential of different leukocyte types, mainly T cells, and cytokine production are mainly responsible for the diminished immune response in these populations. 44 These changes are well‐related to specific pathologies and physiological characteristics of each age, despite the strong influence of genetic factors, which can pre‐determine, for example, the manifestation of autoimmune diseases. 45
Vaccination is considered the most effective mechanism to boost the IS and there are consistent pieces of evidence showing that rPE can improve the vaccination responses, particularly in older people, 46 which can putatively support the positive relationship between physical exercises and the maintenance of the normal functioning of the IS. 47 , 48
As shown in Figure 1, these recommendations are extended to all ages and are associated with the specific health‐promoting responses of regular physical exercise within each age group. Regarding the children, novel findings have shown that several of the genomic and epigenetic pathways modulated by physical exercise in children's immune cells were related to growth and oxidative repair, as well as disease prevention. 43 , 44 Despite the inflammatory mediators evaluated in childhood often being related to obesity and other clinical conditions, it was reported that regularly active children (engaged in rPE) presented lower levels of several inflammatory parameters compared with healthy but sedentary ones. 49
During adulthood, behavioural factors such as an inactive lifestyle, high‐fat or hypercaloric diets, smoking and elevated consumption of alcohol have a prominent influence on IS responses via increased oxidative stress and chronic inflammation. 40 , 50 In this age group, rPE can mediate several health benefits, not only through the maintenance of the normal function of the IS by modulation of the gut microbiome, affecting the host's IS pathways, 51 as well as by improving energy homeostasis and releasing certain neuroendocrine and immune‐modulatory factors that may lower inflammatory and oxidative stress.
Regarding the elderly population, it is paramount to clarify that ageing is a phenomenon that does not affect the IS uniformly, by strict mechanisms, or with equal intensity. 52 Therefore, these aspects have the potential to induce data misinterpretation about the possible interactions between different types of physical exercises and immunity. 53 Nonetheless, recent findings showed that adhesion in rPE programs may induce a 'cascade' of cellular reactions that, by promoting neurogenesis and synaptogenesis, will further delay immunosenescence occurrence. 54 , 55 It is well‐known that immunosenescence affects both innate and adaptive immunity by disturbing negatively the different groups of T cells and B cells. 52 Immunosenescence is also involved in the activation of powerful 'inflammatory pathways', which lead to the development of a chronic, sterile, low‐grade and ageing‐related inflammation, called ‘inflammaging’. 56 Nowadays, this coined term is used to describe complex organic responses to various inflammatory stimuli mediated by high levels of pro‐inflammatory cytokines, which appears to be triggered by chronic functional disorganization of the first cellular line of immune defence. 52 , 56
Interestingly, laboratory and clinical data have shown that the adoption of a rPE once, at any time, in lifetime ameliorates the IS profile for advanced ages. 53 One of the most studied modulating mechanisms is based on the attenuation of the age‐related declines in the number and also in the lymphocyte receptor sensitivity, which allows the (catecholamine‐mediated) redistribution of NK cells and T cells, in special viral‐specific T cells, between tissues and blood. 57 This systemic immune cell redistribution can improve immunosurveillance, diminishing latent viral reactivation. 50 In this respect, there is also a close relationship between these rPE‐mediated mechanisms on the IS and a reduction in the risk of viral respiratory infections. 58 Figure 2
FIGURE 2.
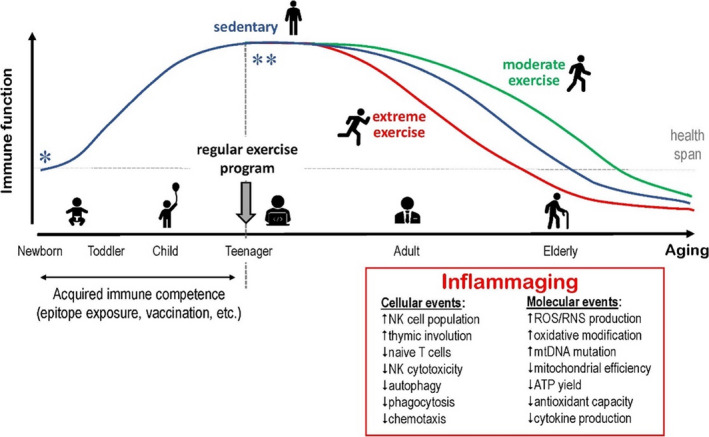
Immune function during lifetime, considering the application of regular and supervised exercises in the context. We assumed here that: (*) no inborn (inherent) immune diseases was diagnosed in newborns and the studied subjects had a healthy childhood sufficient for normal physiological and immunological development (including the common exposure to several epitopes and vaccination); and (**) as teenagers (13‐17y‐o), the subjects initiated a regular (supervised) exercising program (sPA), either exhaustive/extreme or moderate, or simply entered adulthood with sedentary habits, all of them under suitable nutritional conditions. The ‘inflammaging’ box illustrated major (immune) cellular and metabolic/molecular events associated with the ageing‐related decrease of immune functions 45 , 46 , 47 , 48
4. EFFECTS OF rPE ON HOST DEFENCE SYSTEM
As aforementioned, some lifestyles (ie PA levels, inadequate diet and pollutant exposure), combined with intrinsic alterations (ie modifications in body composition, noncommunicable diseases), impact negatively innate and adaptive immunity. 13 , 59 Particularly to the ageing process, the inflammaging process can be considered an essential player on the complex changes observed in immunosenescence, 56 which affects a range of immune cells, from their production by the hematopoietic stem cells to their function in the secondary lymphoid organs or in the mucosa, including in the mucosa of the upper airways. 52
The interaction between these biological and behavioural factors associated with the reduction of IS responses not only can lead to an increased susceptibility to URTI but can also minimize the response to the influenza virus vaccination and other rhinoviruses. 47 Current data have shown that these factors could also be characterized as a host risk factor associated with severe COVID‐19. 54 Viruses, such as rhinovirus, followed by influenza virus and respiratory syncytia virus, are the leading cause of respiratory tract infections. 60 , 61 Respiratory viruses are sub‐microscopic infectious agents that invade the respiratory mucosa and replicate within the host living cells. 55 Unlike bacterial infections, viruses depend entirely on the host cells for their metabolic functions, to promote viral replication, and increase the synthesis of viral proteins, as can be found in the respiratory infections by influenza virus, rhinoviruses and SARS‐CoV‐2. 54
Based on epidemiological data, an intriguing association between rPE and a decrease in the risk and severity of URTI has been described. 58 In addition, studies also show optimized antibody responses to the influenza immunization in elderly adults who are engaged in rPE programs, 57 , 62 since in this population, the Influenza virus vaccine‐induced immunogenicity is of only 30‐40%. 63 Recent findings by our group showed that an elderly group that exercised regularly presented higher levels of specific—IgM and IgG antibodies after influenza vaccination than in the sedentary elderly group. 47 Moreover, bulk evidence shows that rPE can also improve the host response to influenza vaccination in cases with sub‐optimal immunity or when antigen immunogenicity is low, as shown in Figure 2. 56
The improved host response was putatively obtained through cell‐mediated immune interactions, both by the induction of influenza‐specific lymphocyte proliferation and anti‐inflammatory expression of cytokines. 47 These data could indicate that rPE has a putative potential to reduce infection rates for viral and bacterial diseases. As appealing as these data could be, it is noteworthy to mention that current pieces of evidence include dietary protein adjustments for energy supply and accelerated protein turnover with rPE, aiming at the enhancement of vaccination effects against the influenza virus. 3 These purposeful concepts may open new hypotheses for future studies with vaccination against other viral diseases.
5. REGULAR SPA IN THE COVID‐19 ERA AND BEYOND
Taking into account the quantities of information previously presented here, the applications of rPE as a powerful tool in public health, especially against the susceptibility to URTI, 58 could be useful against the symptomatology of COVID‐19 and also on the benefits for the most susceptible population to contract the SARS‐CoV‐2. 54
It should be emphasized that, following the recent findings, middle‐aged and elderly people presenting hypertension, obesity and obesity‐diabetic are more likely to present a higher degree of COVID‐19 severity. 57 , 58 Therefore, rPE is a recommended and nonpharmacological strategy for bodyweight management and a co‐adjuvant topic in the treatment of hypertension and other cardiometabolic diseases, obviously taking the specificities of each aged population into account. 57 , 64 Besides, one of the distinctive hallmarks of exercise training is its anti‐inflammatory effect, which can putatively adjust appropriate elevations of pro‐inflammatory cytokines and consequently create a favourable environment to maintain the IS function and prevention of URTI occurrence. 7 , 65
Interestingly, the cumulative effect of rPE associated with other healthy behaviours appears to have positive effects on VO2max, and this fact has been suggested to confer a decreased risk of contracting chronic respiratory diseases. 59 Complementarily, a recent study showed that VO2max has the potential to be used as a clinically relevant triage tool for identifying risk patients during the COVID‐19 outbreak. 66 Another point that should be highlighted is the observation that some of the patients after the severe manifestation of COVID‐19—who will group for a new wave of the disease that will demand a high public health burden—should be involved in a cardiorespiratory rehabilitation process, for respiratory function recovery and re‐integration into their daily living and mobility activities. 60 Subsequently, the involvement in a specific rPE program (eg combining aerobic and resistance exercises) can lead to a substantial increase in the VO2max and also improve muscle mass, in order to recover from long‐term hospitalization. 57
Concerning the musculoskeletal system, it has been shown that this system, besides its motor functions, is also able to assist the IS to maintain its functions through myokine signalling pathways. 34 All physiological processes associated with exercise (aerobic, resistance or combined), including post‐exercise inflammation, are mediated by redox signals, such as H2O2 and NO, produced by contractile muscle cells, vascular‐endothelial cells, pro‐oxidant agents in plasma.. 67 Briefly, rPE performed in a moderate‐intensity impose mild oxidative conditions in many cells and tissues—in terms of controlled H2O2 and NO concentrations—that will require antioxidant responses through the activation of the Keap1‐Nrf2‐AREs pathway for redox rebalance. 68 On the other hand, extreme/intense exercises impose massive oxidative challenges to cells and tissues that could overwhelm present and inducible antioxidant capacities, leading to increased oxidative/nitrative modifications in vital biomolecules, inflammation, (p53‐mediated) apoptosis or even necrosis. 69 , 70
Ageing has been characterized by the gradual (chronic) accumulation of oxidative modifications in proteins, lipids and nucleic acid (DNA), which leads to mitochondrial and cellular dysfunctions. Therefore, it is not surprising that, by a hermetic principle, regular‐moderate exercises efficiently upregulate antioxidant defences to improve redox‐dependent immune responsiveness in physically active elderly subjects and lead to physiological adaptations that will provide general health and quality of life for these individuals. 71 Regular physical exercises will, thereby, upgrade antioxidant defences on physically active individuals, which will serve as an extended defensive barrier against free radical‐mediated pathological processes, such as chronic metabolic syndromes, diabetes and even neurodegenerative‐cognitive disorders. 72
Accordingly, recent studies have also shown the positive effects of moderate exercises (either prophylactic or ameliorative) against several viral infectious diseases, representing an efficient and nonpharmacological intervention to lower risks, incidence and fatalities caused by SARS‐CoV‐2 during the current COVID‐19 pandemic. 73 , 74 Upstream but strongly linked with redox signalling, mTOR pathway inhibitors, such as rapamycin and metformin, have been currently tested in Phase III (large clinical trials) with very promising results. 75 , 76 Figure 3 illustrates the theoretical redox‐dependent cellular fates in sedentary or exercising young and elderly subjects.
FIGURE 3.
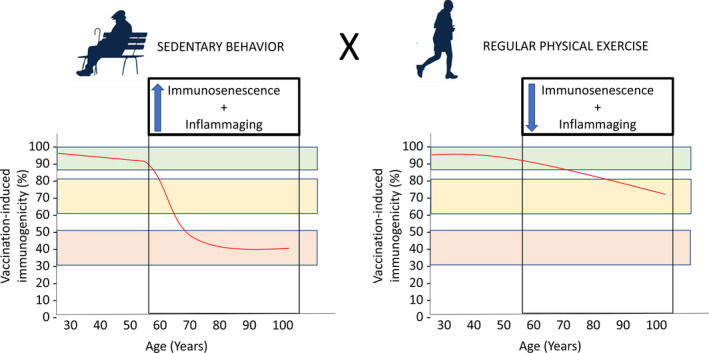
Vaccine‐induced immunogenicity during human life‐span. (A) A sedentary behaviours during ageing process impact negatively in vaccine‐induced immunogenicity during ageing due to the progressive development of the phenomena of immunosenescence and inflammaging. (B) Moderate‐to‐vigorous regular exercise can minimize the progressive development of the phenomena of immunosenescence and inflammaging, which, consequently, can maintain the vaccine‐induced immunogenicity during ageing 18 , 54
Based on current information, there is no doubt that the rPE can positively benefit people in different ways, 33 and taking the lessons already learned from other respiratory viruses into account, 77 , 78 it is putatively expected that the maintenance of an active lifestyle during the SARS‐CoV‐2 pandemic can establish a solid ground to elicit the immune response necessary to be triggered by the long‐awaited vaccination for COVID‐19. 79
In conclusion, when the pandemic COVID‐19 significantly altered the lifestyle of the population in quarantine, preventing people access to open areas, such as parks and squares, or even closed areas, such as gyms, the home‐based physical exercise is here recommended as a low‐cost solution to sustain the efficient immune responsiveness necessary to prevent or even remediate viral disease manifestation. 67 , 80 Further, rPE also assures cognitive benefits to exercised elderly, attenuating negative health‐related psychosocial outcomes. 68 , 81 , 82 Finally, it is worth clarifying that the physical and mental benefits of rPE during the pandemic should be encouraged for all ages, for preventive purposes.
CONFLICT OF INTEREST
All authors assume that they have no conflict of interest.
AUTHOR CONTRIBUTIONS
Guilherme Furtado and Rubens Letieri design the scope of paper and writing. André Bachi and Marcelo Barros helped directly in the design conception, writing and create the Figures 2, 3 and 4. Adriana Caldo‐Silva assisted in the systematic search of articles. Rodolfo Vieira and Ana Teixeira e Vilma Sardão contributed with their expertise for the final version of this work.
FIGURE 4.
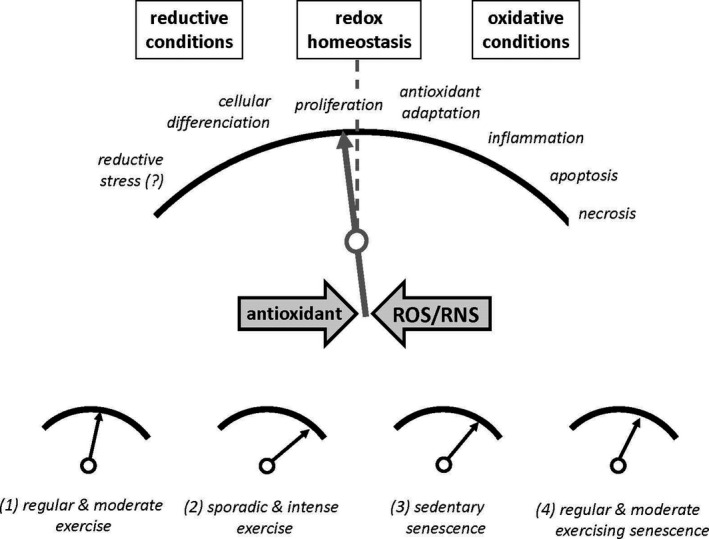
Theoretical cellular redox‐switches that determine cellular fates throughout proliferation, homeostasis, antioxidant adaptation, inflammation, apoptosis and necrosis, depending on increasing oxidizing conditions in cells. 68 , 69 Additional factors as exercise intensity and ageing (senescence) were also considered in the figure
ACKNOWLEDGEMENTS
This study was supported by the São Paulo Research Foundation (FAPESP) grants: #2017/06032‐2. The author Barros MP is a fellow of the Brazilian National Council for Scientific and Technology Development (CNPq; PQ‐2 #305818/2018‐0, Brazil).
Furtado GE, Letieri RV, Caldo‐Silva A, et al. Sustaining efficient immune functions with regular physical exercise in the COVID‐19 era and beyond. Eur J Clin Invest. 2021;51:e13485. 10.1111/eci.13485
REFERENCES
- 1. Cucinotta D, Vanelli M. WHO declares COVID‐19 a pandemic. Acta Biomed. 2020;91(1):157‐160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jaimes JA, André NM, Chappie JS, Millet JK, Whittaker GR. Phylogenetic Analysis and Structural Modeling of SARS‐CoV‐2 Spike Protein Reveals an Evolutionary Distinct and Proteolytically Sensitive Activation Loop. J Mol Biol. 2020;432(10):3309‐3325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Altenburg AF, Magnusson SE, Bosman F, Stertman L, de Vries RD, Rimmelzwaan GF. Protein and modified vaccinia virus Ankara‐based influenza virus nucleoprotein vaccines are differentially immunogenic in BALB/c mice. Clin Exp Immunol. 2017;190(1):19‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ruiz‐Roso MB, de Padilha PC, Mantilla‐Escalante DC, et al. Covid‐19 confinement and changes of adolescent’s dietary trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients. 2020;12(6):1‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Colizzi M, Sironi E, Antonini F, Ciceri ML, Bovo C, Zoccante L. Psychosocial and behavioral impact of COVID‐19 in autism spectrum disorder: An online parent survey. Brain Sci. 2020;10(6):1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Aktuğ ZB, İri R, Aktuğ DN. COVID‐19 immune system and exercise. J Hum Sci. 2020;17(2):513‐520. [Google Scholar]
- 7. Aubertin‐Leheudre M, Rolland Y. The Importance of Physical Activity to Care for Frail Older Adults During the COVID‐19 Pandemic. J Am Med Directors Assoc. 2020;21:973‐976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Constandt B, Thibaut E, De Bosscher V, Scheerder J, Ricour M, Willem A. Exercising in times of lockdown: An analysis of the impact of COVID‐19 on levels and patterns of exercise among adults in Belgium. Int J Environ Res Public Health. 2020;17(11):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Martinez‐Ferran M, de la Guía‐Galipienso F, Sanchis‐Gomar F, Pareja‐Galeano H. Metabolic impacts of confinement during the COVID‐19 pandemic due to modified diet and physical activity habits. Nutrients. 2020;12:1‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Schuch FB, Bulzing RA, Meyer J, et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self‐isolating people during the COVID‐19 pandemic: A cross‐sectional survey in Brazil. Psychiatry Res. 2020;292:1‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Castañeda‐Babarro A, Coca A, Arbillaga‐Etxarri A, Gutiérrez‐Santamaría B. Physical activity change during COVID‐19 confinement. Int J Environ Res Public Health. 2020;17(18):6878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Alomari MA, Khabour OF, Alzoubi KH. Changes in physical activity and sedentary behavior amid confinement: The bksq‐covid‐19 project. Risk Manag Healthc Policy. 2020;13:1757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ciolac EG, da Silva JMR, Vieira RP. Physical exercise as an immunomodulator of chronic diseases in aging. J Phys Act Heal. 2020;17(6):662‐672. [DOI] [PubMed] [Google Scholar]
- 14. Sothern MS, Loftin M, Suskind RM, Udall JN, Blecker U. The health benefits of physical activity in children and adolescents: Implications for chronic disease prevention. Eur J Pediatr. 1999;158(4):271‐274. [DOI] [PubMed] [Google Scholar]
- 15. Sellami M, Gasmi M, Denham J, et al. Effects of acute and chronic exercise on immunological parameters in the elderly aged: Can physical activity counteract the effects of aging? Front Immunol. 2018;9:2187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. 2019;8:201‐217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Walsh NP, Gleeson MM, Shephard RJ, et al. Position Statement Part one : Immune function and exercise. Exerc Immunol Rev. 2011;17:6‐63. [PubMed] [Google Scholar]
- 18. Terra R, da Silva SAG, Pinto VS, Dutra PML. Effect of exercise on the immune system: Response, adaptation and cell signaling. Rev Bras Med do Esporte. 2012;18(3):208‐214. [Google Scholar]
- 19. Cruzat VF, Krause M, Newsholme P. Amino acid supplementation and impact on immune function in the context of exercise. J Int Soci Sports Nutr. 2014;11:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Muchiri WA, Olutende OM, Kweyu IW, Vurigwa E. Meaning of physical activities for the elderly: a review. Am J Sport Sci Med. 2018;6(3):79‐83. [Google Scholar]
- 21. Martin SA, Pence BD, Woods JA. Exercise and respiratory tract viral infections. Exerc Sport Sci Rev. 2009;37(4):157‐164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Adams GR, Zaldivar FP, Nance DM, Kodesh E, Radom‐Aizik S, Cooper DM. Exercise and leukocyte interchange among central circulation, lung, spleen, and muscle. Brain Behav Immun. 2011;25(4):658‐666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Gleeson M. Immune function in sport and exercise. J Appl Physiol. 2007;103:693‐699. [DOI] [PubMed] [Google Scholar]
- 24. Minuzzi LGLG, Chupel MUMU, Rama L, et al. Lifelong exercise practice and immunosenescence: Master athletes cytokine response to acute exercise. Cytokine. 2019;115:1‐7. [DOI] [PubMed] [Google Scholar]
- 25. Vaisberg M, Paixão V, Almeida EB, et al. Daily intake of fermented milk containing lactobacillus casei shirota (lcs) modulates systemic and upper airways immune/inflammatory responses in marathon runners. Nutrients. 2019;11(7):1678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Vaisberg M, Suguri VM, Gregorio LC, Lopes JD, Bachi ALL. Cytokine kinetics in nasal mucosa and sera: new insights in understanding upper‐airway disease of marathon runners. Exerc Immunol Rev. 2013;19:49‐59. [PubMed] [Google Scholar]
- 27. Marques M, Chupel MU, Furtado GE, et al. Influence of chair‐based yoga on salivary anti‐microbial proteins, functional fitness, perceived stress and well‐being in older women: A randomized pilot controlled trial. Eur J Integr Med. 2017;12:44‐52. [Google Scholar]
- 28. Chupel MU, Direito F, Furtado GE, et al. Strength training decreases inflammation and increases cognition and physical fitness in older women with cognitive impairment. Front Physiol. 2017;8:377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Furtado G, Chupel MU, Minuzzi L, et al. The mediating effect of different exercise programs on the immune profile of frail older women with cognitive impairment. Curr Pharm Des. 2020;1‐10. [DOI] [PubMed] [Google Scholar]
- 30. Chupel MU, Minuzzi LG, Furtado GE, et al. Exercise and taurine in inflammation, cognition, and peripheral markers of blood‐brain barrier integrity in older women. Appl Physiol Nutr Metab. 2018;43:733‐741. [DOI] [PubMed] [Google Scholar]
- 31. Furtado GE, Carvalho HM, Loureiro M, et al. Chair‐based exercise programs in institutionalized older women: salivary steroid hormones, disabilities and frailty changes. Exp Gerontol. 2020;130:110790. [DOI] [PubMed] [Google Scholar]
- 32. Petriz BA, Gomes CPC, Almeida JA, et al. The effects of acute and chronic exercise on skeletal muscle proteome. J Cell Physiol. 2017;232(2):257‐269. [DOI] [PubMed] [Google Scholar]
- 33. Hegde BM. Health benefits of exercise. Kuwait Med J. 2018;50(2):143‐145. [Google Scholar]
- 34. Ost M, Coleman V, Kasch J, Klaus S. Regulation of myokine expression: Role of exercise and cellular stress. Free Radic Biol Med. 2016;98:78‐89. [DOI] [PubMed] [Google Scholar]
- 35. Pedersen BK. Anti‐inflammatory effects of exercise: role in diabetes and cardiovascular disease. Eur J Clin Invest. 2017;47:600‐611. [DOI] [PubMed] [Google Scholar]
- 36. Ji LL. Redox signaling in skeletal muscle: Role of aging and exercise. Adv Physiol Educ. 2015;39(1):352‐359. [DOI] [PubMed] [Google Scholar]
- 37. Nikolaidis MG, Margaritelis NV, Matsakas A. Quantitative Redox Biology of Exercise. Int J Sports Med. 2020;41:633‐645. [DOI] [PubMed] [Google Scholar]
- 38. Robinson SM, Reginster JY, Rizzoli R, et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin Nutr. 2018;37:1121‐1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Franzke B, Schober‐Halper B, Hofmann M, et al. Fat soluble vitamins in institutionalized elderly and the effect of exercise, nutrition and cognitive training on their status—the vienna active aging study (vaas): A randomized controlled trial. Nutrients. 2019;11(6):1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Kohut ML, Senchina DS. Reversing age‐associated immunosenescence via exercise. Exerc Immunol Rev. 2004;10:6‐41. [PubMed] [Google Scholar]
- 41. Georgountzou A, Papadopoulos NG. Postnatal innate immune development: From birth to adulthood. Front Immunol. 2017;8:957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Weng NP. Aging of the immune system: how much can the adaptive immune system adapt? Immunity. 2006;24(5):495‐499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Radom‐Aizik S, Zaldivar F, Leu SY, Cooper DM. Brief bout of exercise alters gene expression in peripheral blood mononuclear cells of early‐ and late‐pubertal males. Pediatr Res. 2009;65(4):447‐452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Radom‐Aizik S. Immune response to exercise during growth. Pediatr Exerc Sci. 2017;29(1):49‐52. [DOI] [PubMed] [Google Scholar]
- 45. Anaya JM, Ramirez‐Santana C, Alzate MA, Molano‐Gonzalez N, Rojas‐Villarraga A. The autoimmune ecology. Front Immunol. 2016;7:139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Long JE, Ring C, Drayson M, et al. Vaccination response following aerobic exercise: Can a brisk walk enhance antibody response to pneumococcal and influenza vaccinations? Brain Behav Immun. 2012;26(4):680‐687. [DOI] [PubMed] [Google Scholar]
- 47. Bachi ALLL, Suguri VM, Ramos LR, Mariano M, Vaisberg M, Lopes JD. Increased production of autoantibodies and specific antibodies in response to influenza virus vaccination in physically active older individuals. Results Immunol. 2013;3:10‐16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Monteiro FR, Roseira T, Amaral JB, et al. Combined Exercise Training and l‐Glutamine Supplementation Enhances Both Humoral and Cellular Immune Responses after Influenza Virus Vaccination in Elderly Subjects. Vaccines. 2020;8(4):685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Chamorro‐Viña C, Valentín J, Fernández L, et al. Influence of a moderate‐intensity exercise program on early NK cell immune recovery in pediatric patients after reduced‐intensity hematopoietic stem cell transplantation. Integr Cancer Ther. 2017;16:464‐472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Campbell JP, Turner JE. Debunking the myth of exercise‐induced immune suppression: Redefining the impact of exercise on immunological health across the lifespan. Front Immunol. 2018;9:648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Sohail MU, Yassine HM, Sohail A, Al Thani AA. Impact of physical exercise on gut microbiome, inflammation, and the pathobiology of metabolic disorders. Rev Diabet Stud. 2019;15(1):35‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Gruver AL, Hudson LL, Sempowski GD. Immunosenescence of ageing. J Pathol. 2007;211(2):144‐156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Senchina DS, Kohut ML. Immunological outcomes of exercise in older adults. Clin Interv Aging. 2007;2(1):3‐16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Duggal Niharika A. Reversing the immune ageing clock: lifestyle modifications and pharmacological interventions. Biogerontology. 2018;19(6):481‐496. 10.1007/s10522-018-9771-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Gomez‐Pinilla F, Hillman C. The influence of exercise on cognitive abilities. Compr Physiol. 2013;3(1):403‐428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Minciullo PL, Catalano A, Mandraffino G, et al. Inflammaging and anti‐inflammaging: the role of cytokines in extreme longevity. Arch Immunol Ther Exp. 2016;64:111‐126. [DOI] [PubMed] [Google Scholar]
- 57. Duggal NA, Niemiro G, Harridge SDR, Simpson RJ, Lord JM. Can physical activity ameliorate immunosenescence and thereby reduce age‐related multi‐morbidity? Nat Rev Immunol. 2019;19(9):563‐572. [DOI] [PubMed] [Google Scholar]
- 58. Walsh NP, Oliver SJ. Exercise, immune function and respiratory infection: An update on the influence of training and environmental stress. Immunol Cell Biol. 2016;94(2):132‐139. [DOI] [PubMed] [Google Scholar]
- 59. Simpson RJ, Campbell JP, Gleeson M, et al. Can exercise affect immune function to increase susceptibility to infection? Exerc Immunol Rev. 2020;26:8‐22. [PubMed] [Google Scholar]
- 60. Essaidi‐Laziosi M, Brito F, Benaoudia S, et al. Propagation of respiratory viruses in human airway epithelia reveals persistent virus‐specific signatures. J Allergy Clin Immunol. 2018;141(6):2074–2084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Goodwin K, Viboud C, Simonsen L. Antibody response to influenza vaccination in the elderly: A quantitative review. Vaccine. 2006;24(8):1159‐1169. [DOI] [PubMed] [Google Scholar]
- 62. Kohut ML, Arntson BA, Lee W, et al. Moderate exercise improves antibody response to influenza immunization in older adults. Vaccine. 2004;22(17–18):2298‐2306. [DOI] [PubMed] [Google Scholar]
- 63. Smetana J, Chlibek R, Shaw J, Splino M, Prymula R. Influenza vaccination in the elderly. Hum Vaccines Immunother. 2018;14:540‐549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Carter SJ, Baranauskas MN, Fly AD. Considerations for obesity, vitamin D, and physical activity amidst the COVID‐19 pandemic. Obesity. 2020;28:1176‐1177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Silva‐Renno A, Baldivia GC, Oliveira‐Junior MC, et al. Exercise performed concomitantly with particulate matter exposure inhibits lung injury. Int J Sports Med. 2018;39(2):133‐140. [DOI] [PubMed] [Google Scholar]
- 66. Shi Y, Yu X, Zhao H, Wang H, Zhao R, Sheng J. Host susceptibility to severe COVID‐19 and establishment of a host risk score: Findings of 487 cases outside Wuhan. Crit Care. 2020;24(1):108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Lauer N, Suvorava T, Rüther U, et al. Critical involvement of hydrogen peroxide in exercise‐induced up‐regulation of endothelial NO synthase. Cardiovasc Res. 2005;65(1):254‐262. [DOI] [PubMed] [Google Scholar]
- 68. Wang P, Li CG, Qi Z, Cui D, Ding S. Acute exercise stress promotes Ref1/Nrf2 signalling and increases mitochondrial antioxidant activity in skeletal muscle. Exp Physiol. 2016;101(3):410‐420. [DOI] [PubMed] [Google Scholar]
- 69. Ji LL, Kang C, Zhang Y. Exercise‐induced hormesis and skeletal muscle health. Free Radic Biol Med. 2016;98:113‐122. [DOI] [PubMed] [Google Scholar]
- 70. Beyfuss K, Hood DA. A systematic review of p53 regulation of oxidative stress in skeletal muscle. Redox Rep. 2018;23:100‐117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Bachi ALL, Barros MP, Vieira RP, et al. Combined exercise training performed by elderly women reduces redox indexes and proinflammatory cytokines related to atherogenesis. Oxid Med Cell Longev. 2019;2019:6469213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Tu W, Wang H, Li S, Liu Q, Sha H. The anti‐inflammatory and anti‐oxidant mechanisms of the Keap1/Nrf2/ARE signaling pathway in chronic diseases. Aging Dis. 2019;10(3):637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Alkhatib A. Antiviral functional foods and exercise lifestyle prevention of coronavirus. Nutrients. 2020;12:1‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Calder PC, Carr AC, Gombart AF, Eggersdorfer M. Optimal nutritional status for a well‐functioning immune system is an important factor to protect against viral infections. Nutrients. 2020;12:1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Del Campo JA, García‐Valdecasas M, Gil‐Gómez A, et al. Simvastatin and metformin inhibit cell growth in hepatitis C virus infected cells via mTOR increasing PTEN and autophagy. PLoS One. 2018;13(1):1‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Maiese K. The Mechanistic Target of Rapamycin (mTOR): Novel Considerations as an Antiviral Treatment. Curr Neurovasc Res. 2020;17(3):332‐337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Luzi L, Radaelli MG. Influenza and obesity: its odd relationship and the lessons for COVID‐19 pandemic. Acta Diabetol. 2020;57(6):759‐764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Pascoe AR, Fiatarone Singh MA, Edwards KM. The effects of exercise on vaccination responses: A review of chronic and acute exercise interventions in humans. Brain Behav Immun. 2014;39:33‐41. [DOI] [PubMed] [Google Scholar]
- 79. Li J. Rehabilitation management of patients with COVID‐19. Lessons learned from the first experiences in China. Eur J Phys Rehabil Med. 2020;56(3):335‐338. [DOI] [PubMed] [Google Scholar]
- 80. Ahmed I. COVID‐19 ‐ does exercise prescription and maximal oxygen uptake (VO2 max) have a role in risk‐stratifying patients? Clin Med. 2020;20(3):282‐284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Ranasinghe C, Ozemek C, Arena R. Exercise and well‐being during COVID 19 ‐ Time to boost your immunity. Expert Rev Anti Infect Ther. 2020;18(12):1195‐1200. [DOI] [PubMed] [Google Scholar]
- 82. Smolarek A, H. Ferreira L, P. Mascarenhas L, et al. The effects of strength training on cognitive performance in elderly women. Clin Interv Aging. 2016;11:749‐754. [DOI] [PMC free article] [PubMed] [Google Scholar]