

Abstract
Background
The postoperative reconstruction of ear canal cancer with a local flap such as the snail flap technique has been reported for cases with few tissue defects. The snail flap technique requires a large skin incision and is at risk of facial neuropathy. We have devised a new flap that addresses these problems.
Methods
An 80‐year‐old woman underwent total right ear canal resection for cancer of the right ear canal, and the defect of the ear canal was reconstructed using a local flap. The local flap was used by making a rectangular incision in front of the auricle and rolling it into a cylindrical shape. We named this flap a square screw flap.
Results
The patient was discharged 1 week after surgery without complications.
Conclusions
This method is considered to be useful for reconstruction of the ear canal with a small defect.
Keywords: external auditory canal cancer, external auditory canal reconstruction, pedicled flap, reconstruction after tumor excision, square screw flap
1. INTRODUCTION
Free flaps, skin grafts, and local flaps are required for reconstruction of the ear canal after surgery for tumors, trauma, burns, malformations, and inflammation. Particularly in case of cancer, the tissue defect area after tumor removal is large, and it is difficult to perform wound closure by simple suturing as a reconstructive method. Therefore, it is common to use a pedicle flap containing tissue to maintain blood flow or a free flap reconstruction method that requires postoperative intensive care.
Di Benedetto et al reported the snail flap technique, which creates a local flap for reconstruction after tumor excision for cancers of the ear canal with less tissue invasion and loss. 1 Since this method pulls the facial skin, a large skin incision is required in the neck, which poses a risk of facial neuropathy after surgery and problems with surface adjustment after suturing; however, early discharge and good epithelialization are expected following the procedure.
In this study, we have further improved the skin incision of the snail flap method; we devised a local flap that reconstructs the external auditory canal by forming a cylindrical flap in front of the auricle. This modification—which we refer to as the square screw flap—serves to reduce the risk of facial nerve damage.
We report the usefulness of this new flap by discussing a case of squamous cell carcinoma invading the external auditory meatus, where the tumor was excised and the external auditory meatus was reconstructed using the square screw flap.
Written consent was obtained from the patient.
2. CASE PRESENTATION
An 80‐year‐old woman presented to our clinic with chief complaints of hearing loss and right earache. One month prior to presentation, the patient experienced discomfort in the right ear and a popping sound appeared; therefore, she visited an otolaryngologist. A tumor was found in the right external auditory canal, and she was referred to our hospital for close examination and treatment.
On physical examination, an ulcerative mass of about 1 cm was identified in the anterior wall of the external auditory canal with no apparent infiltration of the tympanic membrane; however, the mass was attached to the tympanic membrane. No regional lymphadenopathy was observed on palpation. Computed tomography showed a tumor on the anterior wall of the external auditory canal and bone erosion.
A biopsy was performed on this tumor at the outpatient clinic where pathological diagnosis revealed the tumor to be squamous cell carcinoma.
Specifically, the patient was diagnosed with T2N0M0 cancer of the anterior wall of the external auditory canal based on the Pittsburgh classification. 2
As a preoperative plan of the line of the resection of the tumor, considering the possibility of infiltrating the anterior wall of the external auditory canal, the anterior margin is the anterior wall of the external auditory canal, the posterior margin is the external auditory canal skin, and the deep margin is the tympanic membrane. The tumor was planned to be removed. A local flap was used to reconstruct the defect.
The patient underwent total right external ear canal resection with reconstruction of the ear canal by a local pedicled flap. An incision was made posterior to the auricle, and the posterior wall of the external auditory canal was peeled from the bone to enter the middle ear cavity and transect the ossicle. A skin incision was made to include the right tragus in the anterior direction, the temporomandibular joint fossa was entered, and part of the joint capsule was excised. The tumor was excised from the anterior wall of the external auditory canal by cutting open the upper and lower parts of the bone with a drill (Figure 1A). After resection of the tumor, intraoperative frozen sections were taken to check the negative surgical margin of the anterior deep area.
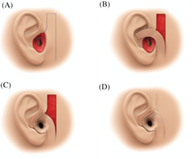
FIGURE 1.

A, After resection of the external auditory canal tumor. B, Skin incision design. C, A local flap is raised. D, After reconstruction of the external auditory canal
A rectangular flap was raised in front of the ipsilateral auricle to reconstruct the tissue defect by excision (Figures 1B and 2A).
FIGURE 2.

Intraoperative photograph. A, Skin incision designed in front of the auricle. B, A rectangular flap is raised. C, The flap is formed into a cylindrical shape. D, The donor site is simply sutured. E, Findings 6 months after surgery
The caudal part of the flap was the pedicle of the flap, and the flap parallel to the mandibular branch was raised with a square shape with a width of 2 cm and a length of 7 cm (Figures 1C and 2B).The flap was raised in the dermal layer and formed into a cylindrical shape. The distal end of the anterior edge and the center were sutured with a 5 to 0 absorbent thread so as to form a cylindrical shape. It was reconstructed into an external auditory canal (Figure 2C).The distal portion of the flap was sutured to the outer edge of the residual ear canal. The local flap donor site was closed with a simple suture (Figures 1D and 2D). Gelfoam and gauze were placed in the wound for 2 weeks after surgery.
One week after the operation, she was discharged from the hospital without complications.
Postoperative pathological examination revealed no tumor component in the anterior or posterior margin. Squamous cell carcinoma was found in the subepithelium of the deep margin, but no neoplastic lesions were found in the intraoperative deep margin or histopathological tissues of the middle ear mucosa. We judged that the margin was positive and performed additional radiation of 50 Gy to the ear canal postoperatively.
The findings 6 months after the surgery are shown (Figure 2E).
Postoperative audiometry was performed and the pure tone average of air conduction hearing of four frequencies of 500, 1000, 1000, and 2000 Hz was 55 dB with an air‐bone gap of 42.5 dB.
The patient was followed up for 15 months after the operation. No recurrence was observed, and the patient continues to be in good condition.
3. CONSIDERATION
Malignant tumors of the external auditory canal are extremely rare, with a prevalence rate of 1 to 6 in 1 million per year. 3 When a tumor develops deep in the external auditory canal, it is often difficult to evaluate deep margins intraoperatively; therefore, a large excision is often performed, resulting in a large tissue defect. Therefore, free flaps are often used for reconstruction. Functional reconstruction in most cases is not performed, especially in advanced cancer.
On the other hand, early malignant tumors of the external auditory canal, which are confined to the external auditory canal, have a favorable prognosis, and complete resection can be expected to cure the tumor. However, the external auditory canal is in the temporal bone, and hard tissues such as the temporomandibular joint and temporal bone exist in peripheral tissues after the external auditory canal resection, and it is difficult to perform a simple suture because a dead space remains.
Reconstruction methods for exposed bone surfaces after tumor resection include split‐thickness skin grafts, local pedicled flaps, and vascularized free flaps. Both methods have postoperative problems due to conductive hearing loss associated with epithelialization and spontaneous closure of the reconstructed external auditory canal. Among these three reconstruction methods, skin grafts can have difficulty in epithelializing after the operation without frequent postoperative care. Although the technique of skin grafting is easy, the transplanted skin rarely engrafts on the bone surface, and the hospitalization period is prolonged or frequent visits to an outpatient clinic are necessary due to treatment for the external auditory canal. 4 Reconstruction with the temporal fascia also requires time for epithelialization. In addition, malignant tumors of the external auditory canal are often treated with postoperative radiation therapy, so if epithelialization is prolonged, the effect of radiation therapy will cause further delay in healing, resulting in a decrease in the patient's quality of life (QOL) and requiring long‐term outpatient visits, as observed in many instances.
When a free flap with a vascular pedicle is used, a surgical operation on another site is required to collect the graft. Therefore, the surgical procedure becomes complicated and the operation time prolonged. Furthermore, it takes time to stabilize the wound site, which often leads to extension of the hospital stay. In addition, the initiation of radiation therapy requires stabilization of the wound site, thereby delaying radiation therapy. Therefore, it is applicable only when there is significant tissue loss and when reconstruction is difficult with the other two methods.
On the other hand, local pedicled flaps can often solve the aforementioned problems, such as skin graft failure, technical aspects of vascularized free flaps, and delayed radiation therapy due to postoperative wound healing. Although they have advantages, they are only indicated for external auditory canal cancers of size T1 or T2. A flap is defined as “valve‐shaped skin or a subcutaneous soft tissue mass with its own circulation.” 5 Flaps include the initial flaps that are used without specifying the feeding blood vessels, myocutaneous flaps to which muscles and fascia are attached, fascia flaps obtained by removing the muscles from the muscle flaps, and perforator flaps that also exclude the fascia. 6 McGregor 7 proposed a simple classification that indicates flap blood circulation: the axial pattern flap and the random pattern flap. The axial pattern flap has an artery with a relatively large blood vessel diameter that runs under the skin parallel to the skin surface over a long distance (direct cutaneous artery), and the one without such an artery is a random pattern flap.
Various methods have been reported for a local flap for external auditory canal cancer, including a snail flap elevated in the shape of a triangular pyramid with a width of 2.5 cm and a length of 6 cm, a method using tissue of the concha of the ear as reconstruction material, and a posterior ear flap using the skin at the back of the ear as a bipedicle flap, among others. 1 , 8 , 9 All of these are classified as random pattern flaps as they do not have direct cutaneous arteries. The random pattern flap is nourished by the blood flow through the skin and subcutaneous vascular network. As blood circulation in the random pattern flap is unstable compared with the axial pattern flap, a long random pattern flap is not possible. When raising the random pattern flap, it is necessary to design it according to the height‐width ratio. The height‐width ratio is the ratio of the flap base width to the flap length that can be safely lifted by a random pattern flap and is set to approximately 1:2; however, a long flap can be made with a 1:3 to 1:4 ratio in the facial region where blood flow is sufficient. 10
In this study, we modified the snail flap and reconstructed the external auditory canal using the local flap of the anterior ear in a case of external auditory canal cancer with little invasion of surrounding tissues (temporal bone). We made a rectangular incision with a width of 1.5 cm and a length of 4.5 cm as shown in the figure on the skin in front of the auricle (Figure 2A) and then rounded the rectangle into a cylinder (Figure 2B,C) to reconstruct the external auditory canal, which we termed a square screw flap.
The advantages of this method are that, compared to the snail flap, there are fewer new incisions because the skin near the wound is used, the surgical operation is simple, and epithelialization is faster; therefore, the hospital stay can be shortened. In patients with a thick beard, a snail flap makes the surgical site difficult to observe due to the effect of hair growth in the reconstructed external auditory canal, and hair removal is required. However, with this method, since the hairless part in front of the auricle is used, hair removal is not required. On the other hand, this method is not suitable for reconstruction in cases of extensive resection: only T1 or T2 cases by the Pittsburgh classification with less infiltration of the temporal bone are indicated for this method. Furthermore, the flap of the anterior part of the ear used in this method is a random pattern flap, and it can be used in the same method as a local flap normally would.
As reported by Di Benedetto et al, 1 the patency of the external auditory canal can be expected by placing a silicon stent for 2 months after surgery. On the other hand, the snail flap is not suitable for cases where the subcutaneous fat is thick and skin tension is strong. We considered that this method is also not suitable for these cases.
Local flaps are a good indication for elderly patients who want to avoid long‐term hospitalization. In particular, men with dark beards and cases with a history of surgery on the neck and a scar on the upper part of the flap are not good candidates for the snail flap, but would be good candidates for this method, instead.
On the other hand, we consider that there is no indication for this method in the case of large defects, including auricle resection.
The advantage of this reconstruction method is that it can maintain the QOL of older adults by shortening hospital stays and simplifying the procedure. In addition, since it is a simple procedure, the operator does not need additional skills or training. Although the number of cases is still small, there is ample room to consider the application of this method considering that our patient, an 80‐year‐old woman, was discharged 1 week after surgery for external auditory canal squamous cell carcinoma. We aim to conduct a study with more patients in the future to evaluate the advantages of this method more accurately.
4. SUMMARY
We experienced a case of reconstruction of the external auditory canal after resection of squamous cell carcinoma invading the external auditory canal. After excision of the tumor, the skin in front of the auricle was incised into a rectangle, and a square screw flap was used to reconstruct the external auditory canal.
We consider this method to be suitable for cases of early T1 or T2 cancers by the Pittsburgh classification, in which local excision of the anterior ear can compensate for the excision defect. On the other hand, we consider thick subcutaneous fat and strong skin tension to be maladaptive for this method.
We considered this method to be a useful external auditory canal reconstruction method that aims for early discharge without delaying postoperative radiotherapy as it is simpler and requires lesser treatment than other reconstruction methods.
CONFLICT OF INTEREST
The authors declare no potential conflict of interest.
Anazawa U, Omura K, Nishijima Y, Aoki K, Kojima H, Tanaka Y. External auditory canal reconstruction with inferior pedicled square screw flap from the preauricular area after resection of external auditory canal cancer. Laryngoscope Investigative Otolaryngology. 2021;6:77–80. 10.1002/lio2.505
BIBLIOGRAPHY
- 1. Di Benedetto G, Pierangeli M, Zura G, Bertani A. Reconstruction of the external auditory canal with a laterocervical twisted flap (snail flap). Plast Reconstr Surg. 1997;99:1745‐1748. [PubMed] [Google Scholar]
- 2. Moody SA, Hirsch BE, Myers EN. Squamous cell carcinoma of the external auditory canal: an evaluation of a staging system. Am J Otol. 2000;21:582‐588. [PubMed] [Google Scholar]
- 3. Lobo D, Llorente JL, Suárez C. Squamous cell carcinoma of the external auditory canal. Skull Base. 2008;18:167‐172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Daisuke S, Atsushi S. A skin graft technique for reconstructing full‐thickness scalp defects. Jpn J Surg Wound Care. 2016;7:118‐123. [Google Scholar]
- 5. Toshiharu M. Hiben toha. Keiseigeka Tiryoushugi Zennsho In: Kiyonori H, Motohiro N, Shinichi H, Shigehiko K, Kensuke K, Jo K, eds. Keiseigeka no kihonshugi 2. Kokuseido: Tokyo; 2017. 74 p (in Japanese). [Google Scholar]
- 6. Toshiharu M. Hiben no Bunrui. Keiseigeka Tiryoushugi Zennsho In: Kiyonori H, Motohiro N, Shinichi H, Shigehiko K, Kensuke K, Jo K, eds. Keiseigeka no kihonshugi 2. Tokyo: Kokuseido; 2017:75‐86 (in Japanese). [Google Scholar]
- 7. McGregor IA, Morgan G. Axial and random pattern flaps. Br J Plast Surg. 1973;26:202‐213. [DOI] [PubMed] [Google Scholar]
- 8. Botting AM, Alkadhi A. External auditory canal and tragal reconstruction following tumor excision: a novel method. Plast Reconstr Surg. 2006;117:2510‐2511. [DOI] [PubMed] [Google Scholar]
- 9. Koji N, Hiroaki S, Seiichiro K. Reconstruction of the wall of the external auditory meatus by the postauricular flap after lateral temporal bone resection. Pract Otol (Kyoto). 2008;101:340‐341. [Google Scholar]
- 10. Takashi N. Theory and practice turbulent axis vasa vasorum type flap of the flap (random pattern flap) and the main shaft vegetative vascular type flap (Axial pattern flap ). Plast Surg. 2012;55:S 100‐S104. (in Japanese). [Google Scholar]