

Recently, two articles1,2 published in China featured the application of hyperbaric oxygen therapy in patients with novel coronavirus disease 2019 (COVID-19) pneumonia. The first was a case report of a severely ill patient who was failing standard respiratory support (not intubated) and whose disease course was reversed with eight hyperbaric oxygen treatments (HBOTs) at 200 kPa/95 minutes total treatment time. The second was a more severely afflicted patient on a ventilator with acute respiratory distress syndrome whose life was saved by the application of five HBOTs. By direct voice and electronic communication with the authors/treating physicians this author has reviewed the data and treatment of four additional severely ill COVID-19 patients with bilateral ground glass opacities who were failing standard mask oxygen therapy, were treated with 3–5 HBOTs and discharged from the hospital to home. The authors reported that they have safely treated an additional 29 less severe patients with the same outcome. The five non-intubated patients had been on oxygen support for days to weeks with immediate pre-HBOT oxygen saturation levels as low as 70% on mask oxygen. With each once daily administration of HBOT the patients experienced sustained elevation of oxygen saturation and improvement in symptoms that persisted to the following morning (Figure 1). With just 3–8 HBOTs the patients were bridged through the hypoxemic crisis phase of the infection and successfully discharged from the hospital. The authors suggested that HBOT applied earlier in the disease process would prevent the deterioration that leads to the significant morbidity and mortality of COVID-19 infection.
Figure 1.
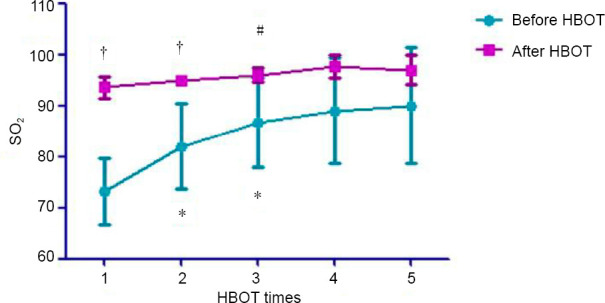
Daily mean blood oxygen saturation levels before and after each HBOT in five COVID-19 patients.
Note: Data are expressed as mean ± SD. *P < 0.05, vs. pre-first HBOT; #P < 0.05, vs. post-first HBOT; †P < 0.05, vs. pre-HBOT for that day. Figure taken online from freely available document that was identical to data provided to this author by the Chinese authors. HBOT: Hyperbaric oxygen treatments; SO2: oxygen saturation.
The application of HBOT to COVID-19 pneumonia/hypoxemia is supported by sound physiology and Henry's Law. Henry's Law is the basis for the normal exchange of gases in our lungs. It states that the concentration in a liquid (pulmonary blood) of an interfacing gas (oxygen in the alveoli of the lungs) is proportional to the pressure of the interfacing gas. Final oxygen uptake and binding to hemoglobin in pulmonary capillary red blood cells is dependent on the diffusion of dissolved oxygen from alveolar wall→pulmonary interstitium→capillary wall→blood plasma→red blood cell membrane→red blood cell cytoplasm→hemoglobin. Interference with this process at any point results in decreased oxygen-hemoglobin binding. In COVID-19 pneumonia patients the barrier to diffusion is in the alveoli (inflammatory exudate-pneumonia) and inflamed interstitium. Standard therapy is to exploit Henry's Law by increasing the pressure of oxygen in the alveoli (increasing the fractional inspired oxygen concentration): nasal cannula→venti-mask→non-rebreather mask→endotracheal intubation. As the pneumonitis and hypoxemia progress standard therapy cannot penetrate the diffusion barriers in the lungs because they are limited by ambient pressure. In addition, it cannot treat the accumulating oxygen debt and intense pulmonary and systemic inflammatory reaction. The options are to bypass the lungs with extracorporeal membrane oxygenation (ECMO) or surmount the limits to dissolution of oxygen in tissue and the barriers to oxygen diffusion by further exploiting Henry's Law with HBOT and increased pressure above ambient pressure.
Through Henry's Law HBOT enhances multiple stages in the above process by increasing: 1) the dissolving of oxygen in the alveolar and inflammatory barrier, 2) the diffusion rate of oxygen, 3) the diffusion distance of oxygen, 4) the dissolution of oxygen in blood plasma, 5) the oxygen saturation of hemoglobin in red blood cells, and 6) the delivery of oxygen to the microcirculation and tissue. The net result is a reversal of the downward spiral of COVID-19 patients. The elevation of systemic levels of oxygen with HBOT has been traditionally misunderstood in terms of respiratory metabolite effects with a transient hyperoxemia that dissipates once the patient leaves the chamber. However, for 358 years, and especially in the modern era (1960 to present), permanent and later trophic effects of HBOT have been documented with both single and repetitive HBOT.3 One of the mechanisms of action was recently elucidated as epigenetic modulation through direct effects of hydrostatic pressure and hyperoxia of gene expression/suppression of over 40% of the protein-coding genes in the human genome. The largest clusters of upregulated genes are the growth, repair, cell signaling, and anti-inflammatory genes, and the largest clusters of down-regulated genes are the pro-inflammatory genes and those that control programmed cell death. A single HBOT has been shown in multiple studies to have dramatic persisting effects on disease pathophysiology, especially inflammation, its ubiquitous acute form, reperfusion injury (e.g., carbon monoxide poisoning, necrotizing infection, resuscitation, and others), and extreme form acute respiratory distress syndrome,4 and on reversing the lethal oxygen debt from cardiac arrest.3 In the Chinese COVID-19 patients HBOT was likely treating pulmonary and systemic hypoxia, inflammation, other pulmonary pathophysiologic targets, reversing oxygen debt, and modulating gene expression both acutely and durably as evidenced by the patient's sustained improvement with each daily HBOT.
The strength of these five cases is reinforced by historical precedence. Unwittingly, the Chinese physicians replicated an historical experience with HBOT in a near identical pulmonary viral pandemic, the Spanish flu pandemic of 1918. Dr. Orval Cunningham of Kansas City, USA applied hyperbaric oxygen therapy (pressure and oxygen) to a moribund cyanotic Spanish flu patient with agonal breathing who experienced the same dramatic reversal of his disease that the Chinese physicians witnessed. He used the near-identical pressure, 1.6 ATA (1 ATA = 101.32 kPa), and number of treatments, but less oxygen.5
While HBOT treatment of these patients was life-saving the authors carefully explained their infection control procedures for the hyperbaric department and chambers. None of their staff became infected with the treatment of 35 COVID-19 patients while healthcare worker transmission has accounted for significant numbers of hospitalized patients in both China and the USA. Strict infection control must be practiced to deliver this therapy or hyperbaric chambers will act as disease vectors and amplify the spread of coronavirus through cross-contamination of healthcare workers and other patients.
In conclusion, preliminary evidence from China strongly suggests that based on the immutable science of HBOT and recent clinical application to deteriorating severely hypoxemic COVID-19 pneumonia patients HBOT has significant potential to impact the COVID-19 pandemic.
Dr. Harch has a consulting company that consults on hyperbaric medicine, renders expert opinions, and provides longterm care to his patients by installing hyperbaric chambers in his patients' homes.
Footnotes
Copyright license agreement:
The Copyright License Agreement has been signed by the author before publication.
Plagiarism check: Checked twice by iThenticate.
Peer review: Externally peer reviewed.
REFERENCES
- 1.Zhong X, Tao X, Tang Y, Chen R. The outcomes of hyperbaric oxygen therapy to retrieve hypoxemia of severe novel coronavirus pneumonia: first case report. Zhonghua Hanghai Yixue yu Gaoqiya Yixue Zazhi? 2020 doi: 10.3760/cma.j.issn.1009-6906.2020.0001. [Google Scholar]
- 2.Zhong XL, Niu XQ, Tao XL, Chen RY, Liang Y, Tang YC. The first case of HBOT in critically ill endotracheal intubation patient with COVID-19. Beijing, China: Novel Coronavirus Pneumonia Research Network Sharing Platform of China Association for Science and Technology; 2020. [Google Scholar]
- 3.Jain KK. Textbook of Hyperbaric Medicine. 6th ed. Cham, Switzerland: Springer; 2017. [Google Scholar]
- 4.Rogatsky GG, Shifrin EG, Mayevsky A. Acute respiratory distress syndrome in patients after blunt thoracic trauma: the influence of hyperbaric oxygen therapy. Adv Exp Med Biol. 2003;540:77–85. doi: 10.1007/978-1-4757-6125-2_12. [DOI] [PubMed] [Google Scholar]
- 5.Sellers LM. The fallibility of the forrestian principle.“semper primus pervenio maxima cum VI”. Laryngoscope. 1964;74:613–633. doi: 10.1288/00005537-196405000-00001. [DOI] [PubMed] [Google Scholar]