

A 54-year-old man with no previous history presented with a 4-month history of progressive exertional dizziness associated with chest pain and dyspnoea. The patient had no syncope, palpitations, orthopnoea, or paroxysmal nocturnal dyspnoea. His blood pressure was 139/71 mmHg and his heart rate was 80 beats per minute. Lung auscultation revealed normal vesicular breathing with bilateral equal air entry and no added sounds. Cardiac examination revealed a normal S1 and S2 with a grade III diastolic murmur heard at the location of the aortic valve. The electrocardiogram revealed a normal sinus rhythm and increased R-wave amplitude in precordial leads V3–V6, which is consistent with left ventricular hypertrophy. Transthoracic echocardiography suspected aortic regurgitation, but due to poor image quality, he was referred for transoesophageal echocardiography (TOE). TOE showed a pentacuspid aortic valve (PAV), with moderately severe aortic insufficiency and non-coaptation leaflets during diastole (Figure 1 and Supplementary material online, Images and Videos S1–S4). It also revealed left ventricular hypertrophy with a mass of 312 g and an ejection fraction of 55%. Additional TOE findings are listed in Table 1. Coronary angiography revealed normal coronary arteries. The patient underwent aortic valve replacement due to the valvular findings and the presence of cardiac symptoms (chest pain and dyspnoea). Due to patient preference, valve replacement was done using a 24 mm ATS AP360 supra-annular mechanical valve. The PAV was confirmed intraoperatively. He recovered without complications and discharged on the 6th day post-operatively. Upon follow-up, patient remained asymptomatic and echocardiography showed a well seated prosthetic valve with normal occlude motion and mean gradient across valve 8 mmHg. PAV is rarely seen and reported in clinical practice; with the first case reported in 1923 by Simonds J.P. Since then, there have been at least eight reported cases to our knowledge.1–3 The main complaint of progressively worsening exertional dizziness, as seen in this case, was not reported before.
Figure 1.
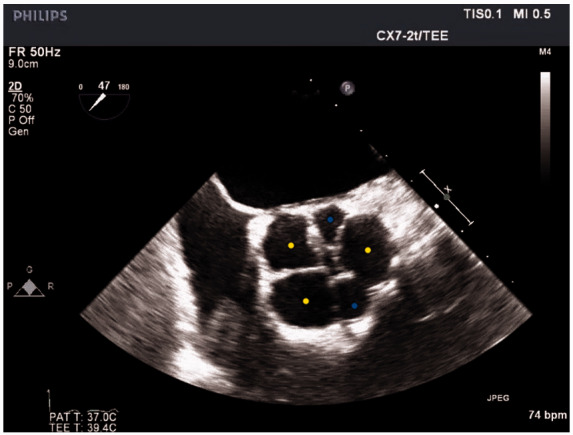
Transoesophageal echocardiography image of the pentacuspid aortic valve, short-axis view. Transoesophageal echocardiogram was performed on Phillips IE 33 system (Phillips medicalvsystems, USA) with S7-2t transoesophageal echocardiography transducer. This shows mid-oesophageal short-axis view in diastolic frame at the level of aortic with unequal sized pentacusps. There are three large cusps of equal size (marked yellow) and two relatively small sized cusps (marked blue). There is a central regurgitant orifice in diastole.
Table 1.
Transoesophageal echocardiography findings and aortic valve insufficiency quantification
| Left ventricular internal systolic dimension | 40 mm |
| Left ventricular internal diastolic dimension | 56 mm |
| Interventricual septal thickness | 13.1 mm |
| Left ventricular posterior wall thickness | 12.8 mm |
| Jet width to left ventricular outflow tract ratio | 65% |
| Pressure half time (limited accuracy due to coexistent diastolic dysfunction) | 400 ms |
| Vena contracta | 9.8 mm |
| Effective regurgitant orifice area | 0.35 cm2 |
| Regurgitant volume | 51 mL |
| Ejection fraction | 55% |
| Left ventricular outflow tract | 25.7 mm |
| Sinus of Valsalva | 35.2 mm |
| Sinotubular junction | 31 mm |
| Proximal ascending aorta | 37 mm |
| Mid-ascending aorta | 37.3 mm |
Supplementary material
Supplementary material is available at European Heart Journal - Case Reports online.
Supplementary Material
Acknowledgements
We would like to thank the patient and his family who allowed the case to be shared with the medical community. We hope that he enjoys a long, healthy and a happy life. We also thank Dr Vinayak Vadgaonkar for his continued support and assistance in helping us with this case report.
Ethical consent: Ethical consult for publication was obtained from the ethical committee of the Mohammed bin Khalifa bin Salman Al-Khalifa Cardiac Center & Bahrain Defense Force Hospital, Kingdom of Bahrain.
Consent: The author/s confirm that written consent for submission and publication of this case report including image(s) and associated text has been obtained from the patient in line with COPE guidance.
Conflict of interest: All authors declare that they have no conflict of interest.
Funding: None.
References
- 1. Tutarel O. The pentacuspid aortic valve. Ann Thorac Surg 2011;91:646. [DOI] [PubMed] [Google Scholar]
- 2. Kuroki H, Hirooka K, Ohnuki M.. Pentacuspid aortic valve causing severe aortic regurgitation. J Thorac Cardiovasc Surg 2012;143:e11–e12. [DOI] [PubMed] [Google Scholar]
- 3. Ozyilmaz S, Akgul O, Guzeltas A, Ozyilmaz I.. Diagnosis of pentacuspid aortic valve with severe regurgitation using three-dimensional transesophageal echocardiography. Echocardiography 2014;32:393–394. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.