

Abstract
Introduction
Foldable hydrophobic acrylic intraocular lenses (IOLs) are prone to develop a long-term postoperative material change called glistenings. The aim of this study was to investigate the changes in the predisposition for glistening formation in one type of hydrophobic acrylic IOL material from its introduction to the present day.
Methods
In a laboratory setup, an in vitro model was used to induce glistenings in hydrophobic acrylic IOLs manufactured by one company (Alcon, Fort Worth, TX, USA) in different years: 23 1990s-manufacture hydrophobic acrylic three-piece IOLs (MA30BA/MA60AC) that were explanted in 1996 and 1997, and five of each of the newer AcrySof IOL models (MA60AC, SA60AT, TFNT00 and SN60WF) from 2014 to 2017. Furthermore, five Clareon (SY60WF) IOLs were put through the same accelerated aging procedure. The number of microvacuoles per square millimeter (MV/mm2) was determined in the central part of each IOL optic and compared between the groups.
Results
The mean number of MV was highest in the 1990s-manufacture Alcon acrylic IOLs, with 1289 (± 738) MV/mm2. The number decreased to 650 (± 101), 192 (± 105), 175 (± 112) and 47 (± 26) for MA60AC, SA60AT, TFNT00 and SN60WF, respectively. The lowest count was obtained in the Clareon group, with 1 (± 1) MV/mm2.
Conclusions
A high number of glistenings was induced in the explanted IOLs from the 1990s. The propensity for glistening formation decreased considerably after that decade and now in current use. Even though in vitro glistening formation in today’s AcrySof material was low, the Clareon material was essentially glistenings-free.
Keywords: Accelerated aging, Biomaterial stability, Glistenings, IOL material history, IOL pathology
Key Summary Points
| Why carry out this study? |
| Foldable hydrophobic acrylic intraocular lenses (IOLs) are prone to develop a long-term postoperative material change called glistenings. |
| We induced glistenings in vitro in hydrophobic acrylic IOLs from different years to find changes in the tendency to develop this pathology and estimate its current clinical importance. |
| We hypothesized that the tendency to glistening formation in the studied IOL material has decreased from the 1990s until today. |
| What was learned from the study? |
| The number of glistenings was highest in the 1990s-manufacture IOLs, with 1289 MV/mm2, and decreased to 650, 192, 175, 47 and 1 MV/mm2 for the MA60AC, SA60AT, TFNT00, SN60WF and Clareon, respectively. |
| Even though glistening formation in today’s AcrySof material was low, the Clareon material was essentially glistenings-free. |
Digital Features
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.13483104.
Introduction
The first Alcon acrylic intraocular lens (IOL) (Alcon Laboratories Inc., Fort Worth, TX, USA) was implanted by Richard Packard in Windsor, England, on December 14, 1990, and market release of the first model, the three-piece MA60AL, was in 1995. Clinical studies on a single-piece model started in 1997 and were completed in 1999, with approval and release of the single-piece Acrysof SA30AL in 2000 [1, 2] (R. Packard, personal communication with GUA, August 2020; W. Graham, personal communication with GUA, August 2020). The Acrysof material is described as a random copolymer of 2-phenylethyl acrylate and 2-phenylethyl methacrylate with a cross-linking diacrylate benzotriazole derivative (bondable) in a three-dimensional network. In the multipiece model MA60AL, the optic is entirely Acrysof, and the two haptics in the modified C style design are made of monofilament (blue-colored) polymethylmethacrylate (PMMA). Since the 1990s, Alcon acrylic IOLs have become increasingly popular throughout the world. Today, there are other different hydrophobic IOL materials, and Alcon introduced lenses made of a new hydrophobic acrylic material (called Clareon) in 2017 (Table 1).
Table 1.
The developmental history of Alcon’s acrylic lenses [1, 2] (R. Packard, personal communication with GUA, August 2020; W. Graham, personal communication with GUA, August 2020)
| Year | Development event |
|---|---|
| 1990 | First implantations of the MA60AL multipiece Acrysof IOL in Windsor, UK, and New Orleans, LA, USA, on December 14 (surgeons: Packard and Brint, respectively) |
| 1991–1992 | MA60AL: European Core Study and parallel FDA clinical study |
| 1994 | Multipiece MA60AL model approvals: CE mark (notified body TUV) and FDA pre-market approval |
| 1995 |
Development of Acrysof single-piece design Problems with “Acrysert” pack and glistenings lead to product withdrawal in the USA |
| 1997 | Single-piece clinical studies start |
| 1999 | Single-piece clinical studies completed |
| 2000 | Single-piece Acrysof approval and market release |
| 2001 | New variations of one-piece for smaller incision injection |
| 2003 | “Yellow” Acrysof Natural available. Multifocal Acrysof ReSTOR launched outside the USA. Trials on Acrysof toric and Wavefront IOLs begin |
| 2005 | Launch of Acrysof toric and IQ lenses |
| 2007 | Acrysof Aspheric ReSTOR+ 3.0 launched in Europe |
| 2010 | Acrysof Aspheric ReSTOR Toric launched in Europe |
| 2012 | Acrysof Aspheric ReSTOR+ 2.5 launched in Europe |
| 2013 | Thomes & Callaghan report on improved manufacturing process—improvements to minimize glistenings |
| 2015 | Acrysof PanOptix launched outside the USA |
| 2017 | Clareon introduced in Europe |
Shortly after the introduction of foldable hydrophobic acrylic IOLs, clinicians observed in slit-lamp examination a long-term postoperative material change—the appearance in some lenses of small glittering inclusions within the IOL optic, calling them glistenings [3]. These are 1–20 µm fluid-filled microvacuoles (MV), and it was observed that they can appear in all lenses made from hydrophobic acrylic material, including Acrysof [4–7]. They become visible as small vacuoles consisting of water that form within the IOL polymer chains surrounding it [8]. These microvacuoles are detectable to the clinical observer, because the refractive index of the water (1.333) in the MV contrasts with that of the polymer (1.55 for the AcrySof material). Another type of a hydration-related material change in hydrophobic acrylic IOLs is subsurface nanoglistenings (SSNGs). They appear as a whitish band in the subsurface area of the IOL. Small vacuoles with diameters from less than 200 nm located up to 120 μm below the surface of the IOL have been identified to be the source of this IOL pathology [9].
Numerous factors have been suggested to promote glistening formation [6, 10]. The impact of glistenings on patients’ visual function lies mainly in increased intraocular light scattering, which is linearly dependent of the number and size of MV [5]. While different experimental setups have been developed to create this material change in vitro and simulate an accelerated aging process, one approach that involves alternating heating and cooling has been shown to create valid and repeatable results simulating the IOL aging within the human eye [5, 11, 12]. Since these initial observations, IOL manufacturers have aimed to reduce the tendency toward glistenings by improving the lens production processes [11]. Nevertheless, material changes such as these glistenings in hydrophobic IOLs remain a discussion topic in the current literature, including quantification of glistenings, assessing their clinical importance and preventing them [13–15].
In the present study, we aimed to induce glistenings in explanted IOLs made from 1990s-manufacture Alcon acrylic IOLs, quantify them and compare the numbers with glistenings generated in the same manufacturer’s hydrophobic acrylic IOLs from recent years and the present day.
Methods
Intraocular Lenses
A single type of hydrophobic acrylic IOL material, manufactured by one company (Alcon, Fort Worth, TX, USA), was studied in the laboratory for different years of manufacture. The first group of lenses consisted of 23 IOLs made in the 1990s, MA30BA and MA60AC, all of which had been explanted and sent to the David J. Apple Laboratory for Ocular Pathology between 1996 and 1997. In six (26%) cases, the IOLs were explanted due to IOL (sub-)luxation, in three (13%) cases due to intraocular infection, in two (9%) due to incorrect refraction, and in one (4%) due to an intraoperative complication; in 11 (48%) cases the reason for explantation could not be definitely confirmed. The second group was five AcrySof IOLs each of the models MA60AC, SA60AT, TFNT00 and SN60WF made in the years 2014 to 2017. Additionally, five lenses made from the company’s most recent hydrophobic acrylic IOL material (Clareon) were studied.
Glistening Induction and Evaluation
Glistening induction and image acquisition and analysis were performed according to a well-established protocol for accelerated IOL aging which we fully described in previous publications [5, 11–13].
Each lens was held in small glass vials containing 20 ml of 0.9% sodium chloride solution, and the vials were kept in a water bath at 45 °C ± 1 °C for 24 h. The temperature was reduced to 37 °C ± 1 °C for 2.5 h before image acquisition. Each IOL was mounted on a heated stage at 37 °C for optical microscopy and a photographic record. A 14-fold magnification was selected to center the IOL on a grid, before a photograph of the central IOL optic was taken in 90-fold magnification [12]. ImageJ (1.49v) software was used to obtain the glistening number [12, 25]. The number of glistenings was given in mean microvacuoles per square millimeter (MV/mm2) (± SD) and compared to the modified clinical (Miyata) glistening grading system, with grade 0 (< 50 MVs/mm2), grade 1 (50–100 MVs/mm2), grade 2 (100–200 MVs/mm2) and grade 3 (> 200 MVs/mm2) [16].
The group of explanted IOLs, sent to the laboratory in 1996 and 1997, had been stored in plastic containers in dry state since the time of acquisition. Prior to the experiment, the explanted IOLs were evaluated for the presence of any glistenings that might have developed before the accelerated aging procedure. The IOLs from later years were purchased and stored as recommended by the manufacturer until the time of the experiment.
Compliance with Ethics and Statistical Analysis
This article is based on analyses of IOLs and does not contain any studies with human participants or animals performed by any of the authors. Statistical analysis was performed using SPSS (IBM SPSS Statistics, version 22). Descriptive statistics included the mean number of MVs/mm2 (± standard deviation) for all lenses of each group. Glistening number was compared between the groups using the Kruskal–Wallis test. A P value less than 0.05 was considered statistically significant.
Results
A high number of glistenings was induced in the 1990s-manufacture Alcon acrylic IOLs, whereas the number of glistenings was less in lenses from later years (Fig. 1). The 1990s IOLs showed few glistenings prior to the accelerated aging, with a mean number of 36 (± 26) MV/mm2. The mean number of MV/mm2 (± SD) in the 1990s-manufacture IOLs after accelerated aging increased to 1289 (± 738) MV/mm2. That number almost halved in the lenses from 2014 with 650 (± 101) and continued to decrease from 192 (± 105), 175 (± 112) to 47 (± 26) over the course of the years 2015, 2016 and 2017, respectively, P < 0.01. The average number of glistenings in the Clareon IOLs (from 2017) was 1 (± 1) (Fig. 2). Compared to the modified clinical (Miyata) glistening grading system, mean number of MV in AcrySof IOLs can be classified as Miyata 3 until 2014. Glistenings decreased to grade 2 in 2015 and 2016 and reached grade 0 in 2017, as the Clareon IOLs [16].
Fig. 1.

Overview images of different AcrySof intraocular lenses (IOLs) after the same in vitro glistening induction procedure in 14-fold magnification. The three-piece AcrySof IOL upper left was explanted in 1996 and developed a large number of microvacuoles, giving the whole optic a whitish appearance. The AcrySof IOLs from later years show a decreasing number of microvacuoles
Fig. 2.
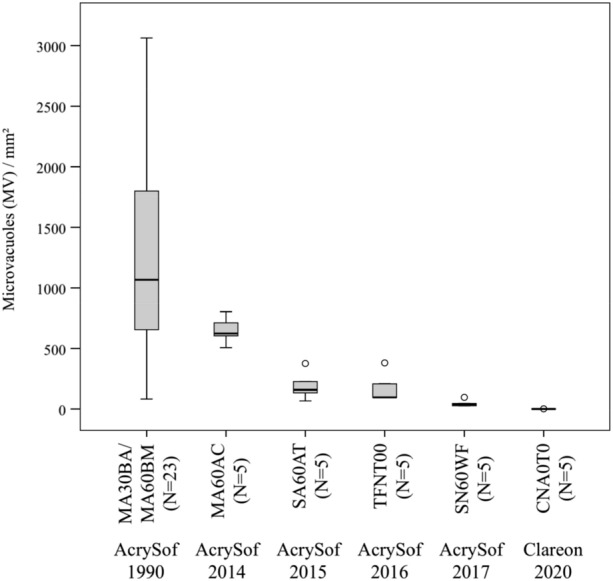
Number of microvacuoles induced in vitro in each intraocular lens (IOL) group from different years and production lines. The mean glistening number and range was highest in the explanted AcrySof IOLs from the 1990s. The number was decreased in AcrySof IOLs from subsequent years. Using the same accelerated aging procedure, almost no microvacuoles could be induced in lenses from Clareon material
Discussion
During his professional career, Prof. David J Apple MD (1941–2011) collected autopsy enucleated pseudophakic eyes as well as explant IOLs for his research on IOL pathology and improving the safety and efficacy of these devices. The specimens were sent to his laboratory by hundreds of reporting ophthalmologists and by pathologist-staff at eye banks. In 2012, these records were transferred from his estate to Heidelberg in Germany. This historical archive has now over 23,000 specimens, which include many files that still hold the explanted IOL, including several specimens of the first explants of the 1990s-manufacture Alcon foldable hydrophobic acrylic IOLs.
We used a well-established laboratory method to induce glistenings in 23 of the explanted Alcon acrylic IOLs from the 1990s and compared the results with the glistenings we could induce in Alcon acrylic lenses made in 2014–2017. Our results showed a reduction in the tendency to glistening formation in this material from the 1990s to today. Even though an improvement has been observed before clinically, no study quantified the differences in glistening formation between lenses produced over such a long period of time in one specific hydrophobic acrylic material and using a single standardized experimental method.
Several factors were suspected to influence the tendency towards glistening formation, including IOL-related factors like the lens copolymer composition, manufacturing process, packaging and dioptric power of the IOL, as well as intraocular environmental factors like changes in temperature, alterations to the equilibrium water content, breakdown of blood-aqueous barrier and postoperative inflammation [10].
After the ophthalmic community had raised concerns about glistenings, manufacturers aimed to address this issue by changing different steps of the IOL manufacturing and the handling of the lenses.
The first IOL was made of a rigid hydrophobic acrylic: PMMA [17]. Following the introduction of phacoemulsification and with an accompanying trend towards smaller and smaller incisions in cataract surgery, IOL manufacturers sought to make foldable hydrophobic acrylic IOLs that could be folded with forceps, or injected, through a small incision. The first foldable lenses, including the Alcon acrylic models, were quite rigid at room temperature and had to be heated in a water bath to soften the lens for folding and placing into the IOL injector [2]. As our study demonstrates, changes in the temperature of an IOL can provoke glistening formation within the lens material, especially in the early acrylic IOLs. The Alcon company claims to have improved the manufacturing process by adjusting environmental controls, equipment, polymer formulation, cast molding and curing operations. Furthermore, the process controls have been tightened [11]. As one very early example, the material was softened so that there was no longer a need to heat the lens prior to implantation. In the first studies about the reasons behind glistening formation, it was believed to be related to the IOL packaging [18]. This led to a voluntary withdrawal of all lenses packed in the AcryPak system. Later, however, glistenings also appeared in IOLs stored in the wagon-wheel system, suggesting that there have to be other factors causing the material change [19].
There are two main theories suggested explaining the driving force behind the formation of fluid-filled vacuoles within the IOL in the patient’s eye [10].
The first theory claims that temperature changes cause the formation of glistenings. A heating process leads to increased water absorption, and after the temperature decreases, the resulting surplus of water gathers in voids within the polymer network, creating microvacuoles [10]. Kato et al. supported this theory by demonstrating that the temperature of the ocular surface decreases approximately 7 °C when the outer temperature decreases from 45 °C to 0 °C [8]. Glistening formation from this mechanism would depend mainly on the copolymer composition of the IOL, since the material glass transition temperature would have the greatest influence. IOL materials are made from different components of acrylate monomers, chromophores and cross-linking agents. Early hydrophobic acrylic IOLs were composed of materials that resulted in low equilibrium water content (EWC)—as low as 0.1–0.5% in the AcrySof material, which is composed of the monomers phenylethyl acrylate (PEA) and phenylethyl methacrylate (PEMA), cross-linked with butanediol diacrylate (BDDA). One way of reducing the tendency towards glistening formation that has been used by manufacturers in recent times is to increase the EWC by including monomers with a higher number of hydrophilic groups [20]. As one example, in the EnVista IOL (Bausch and Lomb, New York, USA) the copolymer consists of 40% poly(ethylene glycol) phenyl ether acrylate, 30% hydroxyethyl methacrylate (HEMA) and 26% styrene, cross-linked by ethylene glycol dimethacrylate (4%)—collectively called PHS copolymer. This composition leads to an EWC of about 4% and shows a low tendency towards formation of glistenings [21]. Changing the polymer composition accordingly seems to be effective in reducing the tendency towards glistening formation, as also seen in the current study in the Clareon material, which had the lowest number of microvacuoles of 1 MV/mm2 among all tested lenses. In the Clareon, one of the monomers of the AcrySof, PEMA, was replaced with HEMA, which increased the EWC of the material under in vivo conditions to around 1.5% [14].
The second theory suggests that glistenings develop in vivo because of small hydrophilic impurities within a hydrophobic IOL material that lead to a dynamic osmotic pressure within the material, causing an influx of water into the polymer, which ultimately creates cavitation and an accumulating number of fluid-filled MV. This cavitation mechanism was first put forward by a study of Saylor et al., who were able to create glistenings in vitro by reducing the osmolarity of the external solution from 300 to 0 mM without changing the temperature. The authors came to the conclusion that oligomeric species generated during polymerization of the material are most likely responsible for the pathology [22]. The Alcon company keeps secret the details about the changes to the manufacturing and packaging process of their hydrophobic acrylic IOL that lead to the reduction in the tendency for glistening formation. Thomes and Callaghan (employees of Alcon Research, Ltd.) presented in 2013 a study showing that a much higher amount of glistenings could be created in AcrySof IOLs made in 2003 compared to lenses made in 2012 [11]. They found an 87% decrease in the mean MV density in lenses manufactured in 2012 compared to those from 2003 [11]. In accordance with their findings, our results show a statistically and clinically significant reduction in the number of glistenings inducible in Alcon acrylic IOLs made in the 1990s compared to AcrySof IOLs made in 2017. Additionally, our study covers a much longer period of over 25 years and includes the company’s most recent polymer formulation, the Clareon, for comparison.
Previous studies have demonstrated that glistenings have a limited effect on visual acuity, but rather lead to additional intraocular light scattering that might cause glare symptoms [5, 6, 13]. A model was recently introduced for calculating the amount of stray light that is additionally introduced to the eye by glistenings: stray light parameter = 0.0046 × glistenings number per mm2 [deg2/sr] [5]. Using this formula, one can estimate the amount of stray light created by the different lens groups from the present study. The mean number of MV of 1289 found in the lenses from the 1990s would result in a stray light increase of 5.9 deg2/sr, which is 2.4-fold higher than the amount induced by a 20-year-old lens (2.5 deg2/sr) [23]. In comparison, light scattering from AcrySof (manufactured in 2017) and Clareon IOLs falls well below the level of a clear crystalline lens.
In an early prospective clinical study on glistenings, Miyata et al. studied eyes implanted with Alcon acrylic IOLs in 1997 and 1998. They proposed a clinical grading system (as described in the methods section of this manuscript) to quantify this material pathology. During the follow-up period of 5–20 months, the authors found a glistenings grade of 1 or higher in 57% of their cases. During a 6-month follow-up of the cases with glistenings, they developed to grade 3 in one third of the cases after 2–3 months [16]. A more recent clinical study from 2017 used a different clinical grading system and found glistenings numbers similar to Miyata grade 1 or higher in 53 and 75% of the cases 2 and 3 years after implantation of the SN60WF AcrySof IOLs, respectively [24]. Our study suggests a major decrease in the propensity for glistening formation in the Alcon acrylic material, but in accordance with recent clinical observations, the material change could still be induced even in the most recent AcrySof IOLs—and would translate to a grade of almost 1 on the clinical Miyata scale. The Clareon material was found to be essentially glistenings-free after the same accelerated-aging procedure was applied. Single microvacuoles counted in these lenses might even be considered as the background noise of the image analysis.
Our study has some limitations. One confounding factor is that, prior to our study, the 1990s IOLs were inside living eyes before we started the accelerated aging. In some of the 1990s cases, not all of the case-related information, such as the reason for explantation, could be definitely confirmed, so we could not include this data. Due to the limited resolution of light microscopy, it was not possible to evaluate SSNG in this study, as this would require more complex analysis methods, like cryogenic focused ion beam scanning electron microscopy [9]. Another limitation is caused by the fact that, through its history, Alcon manufactured its acrylic IOLs in several locations in the USA and Ireland, and we cannot exclude that testing IOLs from different manufacturing sites would change our results. Furthermore, the lack of a longitudinal observation is a limitation, and we cannot exclude a potential change in glistening number over time. Nevertheless, we believe that our study provides useful information and allows the interesting conclusion—reassuring to clinicians—that glistenings are less common in the Alcon lenses made with modern manufacturing techniques.
Conclusion
We demonstrated that a high number of glistenings could be induced in foldable hydrophobic acrylic IOLs explanted in the late 1990s. The inducible number was reduced in the more recent AcrySof material, and the propensity for glistenings formation decreased considerably, while the Clareon material was found to be essentially glistenings-free.
Acknowledgements
Funding
The David J. Apple International Laboratory for Ocular Pathology receives funding from the Klaus Tschira Stiftung, Heidelberg, Germany, which had no role in the design or conduct of this research. T. Yildirim is funded by the Physician-Scientist Program of the Heidelberg University, Faculty of Medicine. The journal’s Rapid Service Fee was funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authorship Contributions
Qiang Wang and Timur M. Yildirim contributed equally to this work.
Disclosures
Timur M. Yildirim, Qiang Wang, Grzegorz Łabuz, S. Schickhardt, Patrick R. Merz, Hyeck-Soo Son, Donald J. Munro and Elfriede Friedmann have nothing to disclose. Ramin Khoramnia and Gerd U. Auffarth report grants, personal fees, non-financial support and consulting fees from Johnson&Johnson and Alcon; grants, personal fees and non-financial support from Carl Zeiss Meditec, Hoya, Kowa, Oculentis/Teleon, Rayner, Santen and Sifi; grants and personal fees from Biotech; and grants from Acufocus, Contamac and Physiol, outside the submitted work.
Compliance with Ethics Guidelines
This article is based on analyses of IOLs and does not contain any studies with human participants or animals performed by any of the authors.
Data Availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Contributor Information
Qiang Wang, Email: 443798074@qq.com.
Timur M. Yildirim, Email: timur.yildirim@med.uni-heidelberg.de
Sonja K. Schickhardt, Email: sonja.schickhardt@med.uni-heidelberg.de
Grzegorz Łabuz, Email: g.labuz@hotmail.com.
Ramin Khoramnia, Email: ramin.khoramnia@med.uni-heidelberg.de.
Patrick R. Merz, Email: Patrick.Merz@med.uni-heidelberg.de
Hyeck-Soo Son, Email: HyeckSoo.Son@med.uni-heidelberg.de.
Donald J. Munro, Email: donald.munro@djapplelab.com
Elfriede Friedmann, Email: friedmann@mathematik.uni-kassel.de.
Gerd U. Auffarth, Email: gerd.auffarth@med.uni-heidelberg.de
References
- 1.Apple DJ, Escobar-Gomez M, Zaugg B, Kleinmann G, Borkenstein AF. Modern cataract surgery: unfinished business and unanswered questions. Surv Ophthalmol. 2011;56(6 Suppl):S3–53. doi: 10.1016/j.survophthal.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 2.Mehdorn E, Hunold W, Auffarth G. Erste Erfahrungen mit einer neuen faltbaren Acryllinse (Acrysof) Berlin, Heidelberg: Kongreß der Deutschsprachigen Gesellschaft für Intraokularlinsen Implantation; 1993. [Google Scholar]
- 3.Dhaliwal DK, Mamalis N, Olson RJ, et al. Visual significance of glistenings seen in the AcrySof intraocular lens. J Cataract Refract Surg. 1996;22(4):452–457. doi: 10.1016/S0886-3350(96)80041-1. [DOI] [PubMed] [Google Scholar]
- 4.Miyata A, Yaguchi S. Equilibrium water content and glistenings in acrylic intraocular lenses. J Cataract Refract Surg. 2004;30(8):1768–1772. doi: 10.1016/j.jcrs.2003.12.038. [DOI] [PubMed] [Google Scholar]
- 5.Łabuz G, Knebel D, Auffarth GU, et al. Glistening formation and light scattering in six hydrophobic-acrylic intraocular lenses. Am J Ophthalmol. 2018;196:112–120. doi: 10.1016/j.ajo.2018.08.032. [DOI] [PubMed] [Google Scholar]
- 6.Łabuz G, Reus NJ, van den Berg TJ. Straylight from glistenings in intraocular lenses: In vitro study. J Cataract Refract Surg. 2017;43(1):102–108. doi: 10.1016/j.jcrs.2016.10.027. [DOI] [PubMed] [Google Scholar]
- 7.Ninel Z, Gregori TSS, Mamalis N, Olson RJ. In vitro comparison of glistening formation among hydrophobic acrylic intraocular lenses. J Cataract Refract Surg. 2002;22:4–56. doi: 10.1016/s0886-3350(02)01224-5. [DOI] [PubMed] [Google Scholar]
- 8.Kato K, Nishida M, Yamane H, Nakamae K, Tagami Y, Tetsumoto K. Glistening formation in an AcrySof lens initiated by spinodal decomposition of the polymer network by temperature change. J Cataract Refract Surg. 2001;27(9):1493–1498. doi: 10.1016/S0886-3350(01)00895-1. [DOI] [PubMed] [Google Scholar]
- 9.Ong MD, Callaghan TA, Pei R, Karakelle M. Etiology of surface light scattering on hydrophobic acrylic intraocular lenses. J Cataract Refract Surg. 2012;38(10):1833–1844. doi: 10.1016/j.jcrs.2012.05.043. [DOI] [PubMed] [Google Scholar]
- 10.Werner L. Glistenings and surface light scattering in intraocular lenses. J Cataract Refract Surg. 2010;36(8):1398–1420. doi: 10.1016/j.jcrs.2010.06.003. [DOI] [PubMed] [Google Scholar]
- 11.Thomes BE, Callaghan TA. Evaluation of in vitro glistening formation in hydrophobic acrylic intraocular lenses. Clin Ophthalmol (Auckland, NZ) 2013;7:1529–1534. doi: 10.2147/OPTH.S44208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yildirim TM, Fang H, Schickhardt SK, Wang Q, Merz PR, Auffarth GU. Glistening formation in a new hydrophobic acrylic intraocular lens. BMC Ophthalmol. 2020;20(1):186. doi: 10.1186/s12886-020-01430-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Weindler JN, Łabuz G, Yildirim TM, Tandogan T, Khoramnia R, Auffarth GU. The impact of glistenings on the optical quality of a hydrophobic acrylic intraocular lens. J Cataract Refract Surg. 2019;45(7):1020–1025. doi: 10.1016/j.jcrs.2019.01.025. [DOI] [PubMed] [Google Scholar]
- 14.Oshika T, Fujita Y, Inamura M, Miyata K. Mid-term and long-term clinical assessments of a new 1-piece hydrophobic acrylic IOL with hydroxyethyl methacrylate. J Cataract Refract Surg. 2020;46(5):682–687. doi: 10.1097/j.jcrs.0000000000000142. [DOI] [PubMed] [Google Scholar]
- 15.Borghesi S, Colciago S, Zeri F, Scialdone A, Tavazzi S. In vitro glistening formation in IOLs: automated method for assessing the volumetric density and depth distribution of microvacuoles. J Cataract Refract Surg. 2020;46(8):1178–1183. doi: 10.1097/j.jcrs.0000000000000272. [DOI] [PubMed] [Google Scholar]
- 16.Miyata A, Uchida N, Nakajima K, Yaguchi S. Clinical and experimental observation of glistening in acrylic intraocular lenses. Jpn J Ophthalmol. 2001;45(6):564–569. doi: 10.1016/S0021-5155(01)00429-4. [DOI] [PubMed] [Google Scholar]
- 17.Ridley H. Intra-ocular acrylic lenses; a recent development in the surgery of cataract. Br J Ophthalmol. 1952;36(3):113–122. doi: 10.1136/bjo.36.3.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Omar O, Pirayesh A, Mamalis N, Olson RJ. In vitro analysis of AcrySof intraocular lens glistenings in AcryPak and wagon wheel packaging. J Cataract Refract Surg. 1998;24(1):107–113. doi: 10.1016/S0886-3350(98)80082-5. [DOI] [PubMed] [Google Scholar]
- 19.Gregori NZ, Spencer TS, Mamalis N, Olson RJ. In vitro comparison of glistening formation among hydrophobic acrylic intraocular lenses(1) J Cataract Refract Surg. 2002;28(7):1262–1268. doi: 10.1016/S0886-3350(02)01224-5. [DOI] [PubMed] [Google Scholar]
- 20.Mentak K (2013) Inventor; Key Medical Technologies, Inc., San Ramon, CA (US), assignee. Method of making ophthalmic devices and components thereof from hydrophobic acrylic (HA) polymers with reduced or eliminated glistenings. CA
- 21.Tetz M, Jorgensen MR. New hydrophobic IOL materials and understanding the science of glistenings. Curr Eye Res. 2015;40(10):969–981. doi: 10.3109/02713683.2014.978476. [DOI] [PubMed] [Google Scholar]
- 22.Saylor DM, Coleman Richardson D, Dair BJ, Pollack SK. Osmotic cavitation of elastomeric intraocular lenses. Acta Biomater. 2010;6(3):1090–1098. doi: 10.1016/j.actbio.2009.08.030. [DOI] [PubMed] [Google Scholar]
- 23.van den Berg TJ. Analysis of intraocular straylight, especially in relation to age. Optom Vis Sci. 1995;72(2):52–59. doi: 10.1097/00006324-199502000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Johansson B. Glistenings, anterior/posterior capsular opacification and incidence of Nd:YAG laser treatments with two aspheric hydrophobic acrylic intraocular lenses - a long-term intra-individual study. Acta Ophthalmol. 2017;95(7):671–677. doi: 10.1111/aos.13444. [DOI] [PubMed] [Google Scholar]
- 25.Rasband W. ImageJ; Image Processing and Analysis in Java. Bethesda, Maryland, Research Services Branch, National Institutes of Health, Bethesda. Available at: http://rsb.info.nih.gov/ij/. (Accessed 20 May 2020)
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.