

Key Points
Question
When does the clinical benefit of dapagliflozin emerge in patients with heart failure with reduced ejection fraction, and what is the magnitude as a function of proximity to prior heart failure hospitalization?
Findings
In this secondary analysis of a randomized clinical trial, dapagliflozin rapidly reduced the risk of cardiovascular death or worsening heart failure, with a sustained statistically significant benefit as soon as 28 days. Patients with a more recent heart failure hospitalization were at particularly high risk and experienced robust relative and absolute risk reductions.
Meaning
In this study, there was a rapid reduction in risk of cardiovascular death or worsening heart failure when dapagliflozin was initiated in patients with heart failure with reduced ejection fraction, with particularly large absolute risk reductions in patients with a more recent heart failure hospitalization.
This secondary analysis of a randomized clinical trial examines the timing of the onset of clinical benefit with dapagliflozin and its magnitude as a function of proximity to prior heart failure hospitalization in patients with chronic heart failure with reduced ejection fraction.
Abstract
Importance
Dapagliflozin has been shown to reduce the risk of cardiovascular death or worsening heart failure (HF) in patients with chronic HF and reduced ejection fraction (HFrEF). However, clinical inertia often underlies deferred initiation of effective therapies.
Objective
To examine timing of onset of clinical benefit with dapagliflozin and magnitude as a function of proximity to prior HF hospitalization.
Design, Setting, and Participants
This is a secondary analysis of a completed multinational trial. The Dapagliflozin and Prevention of Adverse-Outcomes in Heart Failure trial was a double-blind, placebo-controlled randomized clinical trial of dapagliflozin in patients with chronic HFrEF (n = 4744). From February 2017 to August 2018, the study enrolled patients in New York Heart Association classes II through IV and with left ventricular ejection fraction of 40% or less; the median (range) follow-up time was 18.2 (0-27.8) months. Hazard ratios (HRs) were calculated for the primary efficacy outcome with dapagliflozin vs placebo by time following randomization. Efficacy and safety of dapagliflozin were assessed according to the timing of the most recent HF hospitalization prior to trial enrollment.
Exposures
None.
Main Outcomes and Measures
Composite of cardiovascular death or worsening HF.
Results
A total of 4744 patients were included (1109 women [23.4%]; mean [SD] age, 66.3 [10.9] years). The reduction in the primary outcome with dapagliflozin was rapidly apparent, with a sustained statistically significant benefit by 28 days after randomization (HR at 28 days, 0.51 [95% CI, 0.28-0.94]; P = .03). A total of 2251 patients (47.4%) had been previously hospitalized for HF, and 1301 (27.4%) had been hospitalized within 12 months prior to enrollment. Among patients treated with placebo, there was a stepwise gradient of risk for the primary outcome according to timing of most recent HF hospitalization, with 2-year Kaplan-Meier rates of 21.1%, 25.3%, and 33.8% (adjusted P = .003) for patients with a prior HF hospitalization never, more than 12 months ago, and 12 or fewer months ago, respectively. Across these subgroups, dapagliflozin reduced the relative risk of the primary outcome by 16% (HR, 0.84 [95% CI, 0.69-1.01]), 27% (HR, 0.73 [95% CI, 0.54-0.99]), and 36% (HR, 0.64 [95% CI, 0.51-0.80]), respectively (P = .07 for trend). Accordingly, patients with a more recent HF hospitalization tended to experience greater absolute risk reductions with dapagliflozin at 2 years: 2.1% (95% CI, −1.9% to 6.1%), 4.1% (95% CI, −3.6% to 11.7%), and 9.9% (95% CI, 3.3%-16.5%), respectively (P = .05 for trend).
Conclusions and Relevance
In this study, treatment with dapagliflozin was associated with rapid reduction in the risk of cardiovascular death or worsening HF, with a sustained statistically significant benefit emerging very early after randomization. Patients with a more recent HF hospitalization were at particularly high risk and experienced greater relative and absolute risk reductions with dapagliflozin.
Trial Registration
ClinicalTrials.gov Identifier NCT03036124
Introduction
In the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) trial, treatment with the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin, added to other guideline-directed medical therapy, reduced the risk of worsening heart failure (HF) events and cardiovascular death in patients with HF with reduced ejection fraction (HFrEF) (hazard ratio [HR], 0.74; 95% CI, 0.65-0.85; P < .001).1 With many different therapeutic options available for patients with HFrEF, clinical inertia often underlies deferred initiation of additional beneficial therapy, which ultimately leads to preventable adverse HF events.2 To frame these potential lost opportunities with respect to dapagliflozin, we examined the timing of onset of clinical benefit with dapagliflozin in the DAPA-HF trial.
In addition, hospitalization for worsening HF is a prognostically significant event in the clinical course of a patient with chronic HF.3,4 Beyond the substantial consequence of inpatient admissions for patient quality of life, HF hospitalization identifies patients who are at high risk for subsequent disease progression, requirement for advanced therapies, and cardiovascular death.3,4 Because of their elevated risk profile, patients who have been hospitalized for HF represent an important target population for reducing overall HF morbidity and mortality.5 Although DAPA-HF excluded patients who were in the midst of an HF hospitalization, nearly half of the patients enrolled in the DAPA-HF trial had been previously hospitalized for HF.1 We therefore also examined whether the risk of clinical events and response to dapagliflozin varied as a function of proximity to the last reported HF hospitalization.
Methods
Study Population
The design and primary results of the DAPA-HF trial have been previously reported.1,6 Briefly, DAPA-HF was a multinational, double-blind, placebo-controlled randomized clinical trial in patients with HFrEF (n = 4744), conducted between February 2017 and August 2018, that evaluated the efficacy and safety of dapagliflozin, 10 mg daily, compared with a matching placebo, over a median (range) follow-up of 18.2 (0-27.8) months. The ethics committee at each of the 410 participating institutions (in 20 countries) approved the protocol, and all patients provided written informed consent.
The trial included patients with New York Heart Association (NYHA) functional classes II through IV and left ventricular ejection fraction (LVEF) of 40% or less who in the view of the investigators were optimally treated with pharmacological and device therapy for HFrEF according to local guidelines. Study participants were also required to have an N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentration of 600 pg/mL or more, or 400 pg/mL or more if hospitalized for HF within the previous 12 months. Patients with atrial fibrillation or atrial flutter were required to have an NT-proBNP concentration of 900 pg/mL or more, irrespective of prior history of HF hospitalization. Patients were excluded from participation in the trial if they were currently hospitalized for acute decompensated HF or had been hospitalized for HF within 4 weeks of trial enrollment. Other key exclusion criteria included symptoms of hypotension or systolic blood pressure less than 95 mm Hg, estimated glomerular filtration rate less than 30 mL/min/1.73 m2 (or rapidly declining kidney function), type 1 diabetes, and another condition likely to prevent patient participation in the trial or significantly limit life expectancy. A full list of exclusion criteria is provided in a previously published article on the design.6
For the present analysis, patients were categorized according to the timing of the most recent HF hospitalization relative to trial enrollment. This information was captured categorically in the case record form, and patients were classified as having been hospitalized for HF within the last 12 months, more than 12 months prior to enrollment, or never.
Efficacy and Safety Outcomes
The primary efficacy outcome in the trial was the composite of an episode of worsening HF (an unplanned hospital admission or urgent HF visit resulting in intravenous therapy for HF) or cardiovascular death, whichever occurred first. For the present analysis, we also assessed the individual components of worsening HF episode (a hospitalization for HF or urgent HF visit) and cardiovascular death. All outcomes were adjudicated centrally by a clinical events committee blinded to treatment group assignment using established definitions as part of the conduct of the trial. Source documents were reviewed to establish dates of events. For the present analysis, we assessed the following safety outcomes, which were prespecified in the DAPA-HF trial: serious adverse events, adverse events associated with the discontinuation of study treatment, and adverse events of interest associated with volume depletion and kidney adverse events.
Statistical Analyses
Baseline characteristics were summarized according to the timing of the most recent HF hospitalization relative to trial enrollment. Categorical variables are reported as counts and percentages, and continuous variables as means and SDs or as medians and interquartile ranges (IQRs), as appropriate. Differences between groups were evaluated with the χ2 test for categorical variables and analysis of variance or the Kruskal-Wallis test for continuous variables, as appropriate.
To explore the timing of onset of the clinical benefit of dapagliflozin vs placebo, we calculated the hazard ratios (HRs) and 95% CIs for the treatment effect of dapagliflozin vs placebo on the primary efficacy outcome, with the data set truncated and iteratively reanalyzed in incremental cuts at each day following randomization. These data were plotted over time using locally weighted scatterplot smoothing (LOWESS). Analogous plots were created for each of the components of the primary efficacy outcome (ie, cardiovascular death and worsening HF).
The rates of the efficacy outcomes across categories defined by timing of the most recent HF hospitalization in patients in the placebo arm were calculated using 2-year Kaplan-Meier failure estimates and compared using the log-rank test. We evaluated the association between timing from prior HF hospitalization and risk of the efficacy outcomes using multivariable Cox proportional hazards regression analysis, adjusting for variables of a priori clinical interest (age, sex, race, LVEF, baseline NT-proBNP concentration, and NYHA class).
We used Cox regression analysis to calculate HRs for the treatment effect of dapagliflozin compared with placebo, 95% CIs, and 2-sided P values for each of the efficacy outcomes across categories defined by timing of the most recent HF hospitalization. To assess the trend in HR for the primary efficacy outcome by timing of the most recent HF hospitalization, we used an inverse-variance weighted least-squares model. To compare absolute differences in the treatment effect of dapagliflozin vs placebo according to timing of the most recent HF hospitalization, we calculated the absolute risk reduction (ARR) by subtracting the Kaplan-Meier event rates for the primary efficacy end point at 2 years in patients treated with dapagliflozin from those of patients treated with placebo across each subgroup. To assess the trend in ARR for the primary efficacy end point, we used an inverse-variance weighted least-squares model, regressing ARR on ordinal categories defined by the timing of the most recent HF hospitalization. All analyses were performed based on intention-to-treat status, with diabetes status (a randomization stratification factor in the DAPA-HF trial) as a covariate. Statistical analyses were performed in Stata version 16.0 (StataCorp) and SAS version 9.4 (SAS Institute). All P values were 2 sided, and a P value less than .05 was considered statistically significant.
Results
Among the 4744 patients in the DAPA-HF trial, 1109 (23.4%) were women. The mean (SD) age was 66.3 (10.9) years.
Timing of Onset of Clinical Benefit of Dapagliflozin
A reduction in the risk of the primary efficacy outcome of worsening HF event or cardiovascular death was rapidly apparent, as demonstrated by the early separation of the Kaplan-Meier curves. Specifically, the statistical significance of this benefit (ie, nominal P < .05) was sustained by 28 days after randomization (HR at 28 days, 0.51 [95% CI, 0.28-0.94]; P = .03; Figure 1, A and B), after which the upper confidence boundary of the HR remained below unity for the remainder of the trial. A similar pattern of early and consistent benefit was observed for the individual components of the primary efficacy outcome (worsening heart failure: HR at 28 days, 0.48 [95% CI, 0.23-0.94], HR at end of study, 0.70 [95% CI, 0.59-0.83]; cardiovascular death: HR at 28 days, 0.87 [95% CI, 0.31-2.41]; HR at end of study, 0.82 [95% CI, 0.69-0.98]; Figure 1, C and D).
Figure 1. Hazard Ratios (HRs) by Day Postrandomization.
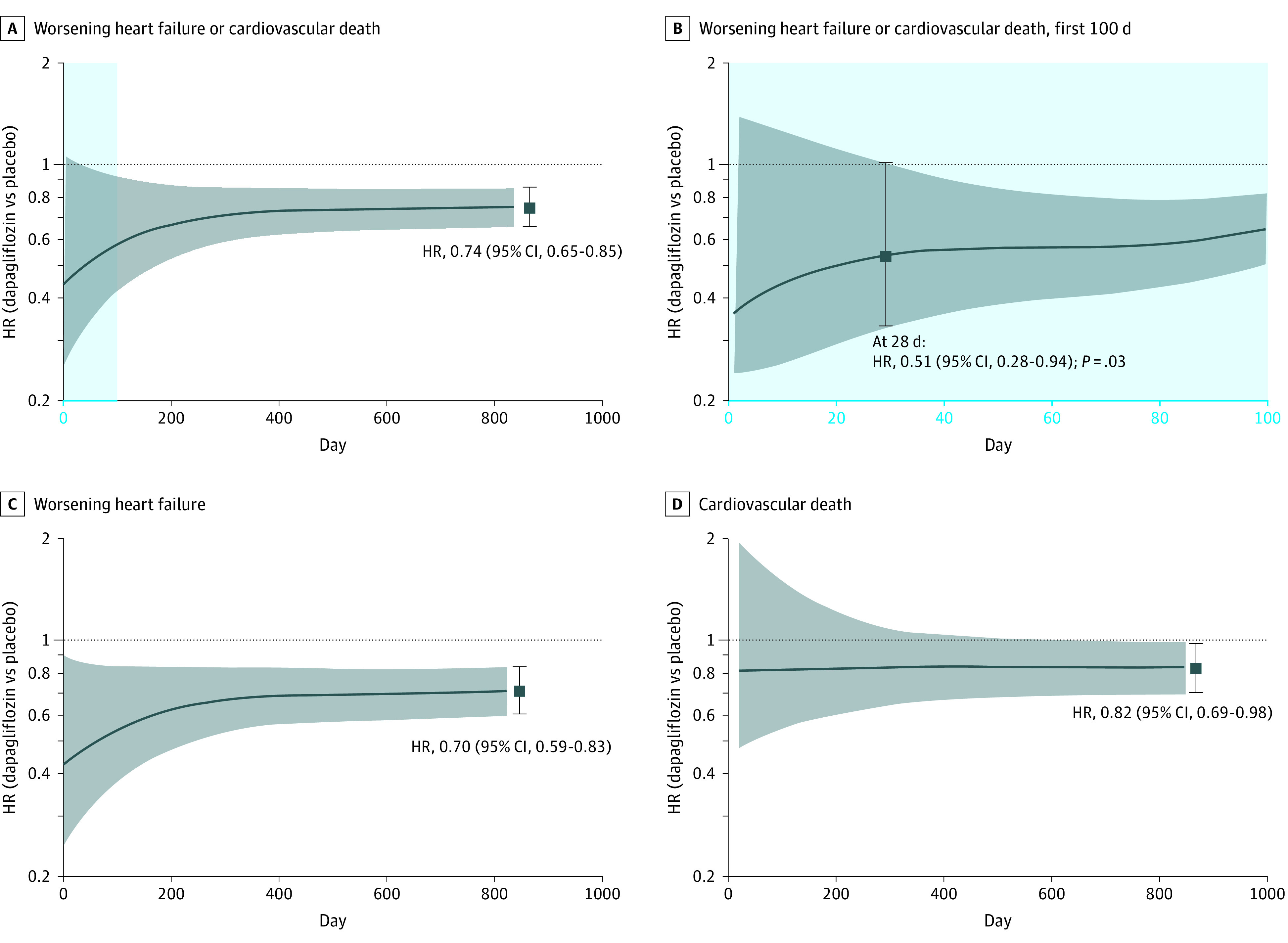
A, Dapagliflozin vs placebo for the primary efficacy outcome; B, dapagliflozin vs placebo for the primary efficacy outcome in the first 100 days; C and D, the individual components of worsening heart failure (C) and cardiovascular death (D). The HRs and 95% CIs observed at the end of the trial for each outcome are provided as a point of reference.1 A reduction in the risk of the primary efficacy outcome of cardiovascular death or worsening heart failure event was statistically significant by 4 weeks after randomization (HR at 28 days, 0.51 [95% CI, 0.28-0.94]; P = .03).
Characteristics by Most Recent HF Hospitalization
Of the 4744 patients, 2251 patients (47.4%) had been previously hospitalized for HF, and 1301 (27.4%) had been so within the 12 months prior to enrollment. Patients who had been hospitalized for HF within 12 months of trial enrollment were less likely to be White (those with no prior hospitalization, 1861 of 2493 [74.7%] vs those hospitalized >12 months ago, 612 of 950 [64.4%] vs those hospitalized in ≤12 months, 860 of 1301 [66.2%]; P < .001), more likely to have more symptomatic disease based on a higher proportion with symptoms in NYHA class III (those with no prior hospitalization, 788 [31.6%] vs those hospitalized >12 months ago, 236 [24.8%] vs those hospitalized in ≤12 months, 474 [36.4%]) or class IV (those with no prior hospitalization, 12 [0.5%] vs those hospitalized >12 months ago, 6 [0.6%] vs those hospitalized in ≤12 months, 25 [1.9%]; P < .001), and more likely to be receiving a diuretic (those with no prior hospitalization, 2028 [81.3%] vs those hospitalized >12 months ago, 833 [87.7%] vs those hospitalized in ≤12 months, 1147 [88.2%]; P < .001) (Table 1).
Table 1. Baseline Characteristics by Timing of Most Recent Heart Failure (HF) Hospitalization Relative to Trial Enrollmenta.
| Characteristic | Participants, No. (%) | P value | |||
|---|---|---|---|---|---|
| Full trial cohort (N = 4744) | Timing of HF hospitalization relative to enrollment | ||||
| Never (n = 2493) | >12 Mo (n = 950) | ≤12 Mo (n = 1301) | |||
| Age, mean (SD), y | 66.3 (10.9) | 66.7 (10.7) | 66.9 (10.3) | 65.2 (11.5) | <.001 |
| Female | 1109 (23.4) | 591 (23.7) | 215 (22.6) | 303 (23.3) | .80 |
| White race | 3333 (70.3) | 1861 (74.7) | 612 (64.4) | 860 (66.2) | <.001 |
| BMI, mean (SD) | 28.2 (5.9) | 28.3 (6.0) | 28.0 (5.7) | 28.0 (5.9) | .09 |
| NYHA class at enrollment | |||||
| II | 3203 (67.5) | 1693 (67.9) | 708 (74.5) | 802 (61.6) | <.001 |
| III | 1498 (31.6) | 788 (31.6) | 236 (24.8) | 474 (36.4) | |
| IV | 43 (0.9) | 12 (0.5) | 6 (0.6) | 25 (1.9) | |
| Baseline LVEF, mean (SD), % | 31.1 (6.8) | 31.3 (6.7) | 30.6 (6.8) | 30.9 (6.9) | .009 |
| Baseline NT-proBNP, median (IQR), pg/mL | 1437 (857-2650) | 1400 (852-2481) | 1526 (957-2597) | 1486 (791-2968) | .09 |
| Main causative mechanism of HF | |||||
| Ischemic | 2674 (56.4) | 1442 (57.8) | 529 (55.7) | 703 (54.0) | .03 |
| Nonischemic | 1687 (35.6) | 840 (33.7) | 358 (37.7) | 489 (37.6) | |
| Unknown | 383 (8.1) | 211 (8.5) | 63 (6.6) | 109 (8.4) | |
| Baseline eGFR <60 mL/min/1.73 m2 | 1926 (40.6) | 975 (39.1) | 418 (44.1) | 533 (41.0) | .03 |
| Baseline HF medications | |||||
| Diuretic | 4008 (84.5) | 2028 (81.3) | 833 (87.7) | 1147 (88.2) | <.001 |
| ACEI | 2661 (56.1) | 1390 (55.8) | 515 (54.2) | 756 (58.1) | .16 |
| ARB | 1307 (27.6) | 704 (28.2) | 265 (27.9) | 338 (26.0) | .32 |
| ARNI | 508 (10.7) | 298 (12.0) | 99 (10.4) | 111 (8.5) | .005 |
| β-Blocker | 4558 (96.1) | 2388 (95.8) | 921 (96.9) | 1249 (96.0) | .29 |
| MRA | 3370 (71.0) | 1754 (70.4) | 653 (68.7) | 963 (74.0) | .01 |
| Digoxin | 887 (18.7) | 412 (16.5) | 206 (21.7) | 269 (20.7) | <.001 |
| Atrial fibrillation | 1818 (38.3) | 924 (37.1) | 400 (42.1) | 494 (38.0) | .02 |
| ICD at enrollment | 1242 (26.2) | 688 (27.6) | 296 (31.2) | 258 (19.8) | <.001 |
| CRT at enrollment | 354 (7.5) | 166 (6.7) | 92 (9.7) | 96 (7.4) | .01 |
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor–neprilysin inhibitor; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); CRT, cardiac resynchronization therapy; eGFR, estimated glomerular filtration rate; ICD, implantable cardioverter-defibrillator; IQR, interquartile range; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association.
Categorical variables are shown as counts and percentages. Continuous variables are shown as mean (SD) or median (IQR) values.
Clinical Risk by Timing of Most Recent HF Hospitalization
In the placebo arm, there was a stepwise gradient of risk for the primary efficacy outcome of cardiovascular death or worsening HF event according to timing of the most recent HF hospitalization, ranging from a 2-year Kaplan-Meier event rate of 21.1% in patients with no prior history of HF hospitalization, 25.3% in those with an HF hospitalization more than 1 year prior to enrollment, and 33.8% in those with an HF hospitalization within 12 months of trial enrollment (P = .04 for trend) (Figure 2). This risk gradient remained significant after adjusting for age, sex, race, LVEF, baseline NT-proBNP concentration, and NYHA class (compared with patients never hospitalized for HF, adjusted HRs were 1.08 [95% CI, 0.90-1.29] and 1.30 [95% CI, 1.12-1.51] for those hospitalized >12 months ago and ≤12 months ago, respectively; P = .003) (Table 2). The risk difference appeared to be driven by an increased risk of worsening HF (compared with patients never hospitalized for HF, adjusted HRs were 1.19 [95% CI, 0.95-1.49] and 1.56 [95% CI, 1.29-1.88] for those hospitalized >12 months ago and ≤12 months ago, respectively) rather than cardiovascular death (compared with patients never hospitalized for HF, adjusted HRs were 1.01 [95% CI, 0.80-1.29] and 0.98 [95% CI, 0.80-1.21] for those hospitalized >12 months ago and ≤12 months ago, respectively).
Figure 2. Cumulative Incidence of Cardiovascular Death or Worsening Heart Failure Event at 2 Years by Timing of Most Recent Heart Failure Hospitalization Relative to Trial Enrollment.

There was a stepwise gradient of risk for the primary efficacy outcome of cardiovascular death or worsening heart failure event according to timing of the most recent heart failure hospitalization. This risk gradient remained significant after adjusting for age, sex, race, left ventricular ejection fraction, baseline N-terminal pro-B-type natriuretic peptide concentration, and New York Heart Association class (compared with patients never hospitalized for HF, adjusted hazard ratios were 1.08 [95% CI, 0.90-1.29] and 1.30 [95% CI, 1.12-1.51] for those hospitalized >12 months ago and ≤12 months ago, respectively; P = .003).
Table 2. Clinical Events and Treatment Effect by Timing of Most Recent Heart Failure (HF) Hospitalization Relative to Trial Enrollmenta.
| Most recent HF hospitalization | Events, No. | Patients, No. | Placebo arm | Dapagliflozin arm incidence rate per 100 patient-years (95% CI) | Treatment effect hazard ratio (95% CI)b | ||
|---|---|---|---|---|---|---|---|
| Incidence rate per 100 patient-years (95% CI) | Unadjusted hazard ratio (95% CI) | Adjusted hazard ratio (95% CI) | |||||
| Primary efficacy end point | |||||||
| Never | 414 | 2493 | 13.1 (11.5-15.0) | 1 [Reference] | 1 [Reference] | 11.0 (9.5-12.7) | 0.84 (0.69-1.01) |
| >12 mo | 173 | 950 | 15.2 (12.5-18.6) | 1.07 (0.89-1.27) | 1.08 (0.90-1.29) | 11.0 (8.8-13.8) | 0.73 (0.54-0.99) |
| ≤12 mo | 301 | 1301 | 21.6 (11.6-25.0) | 1.45 (1.25-1.68) | 1.30 (1.12-1.51) | 13.8 (11.6-16.6) | 0.64 (0.51-0.80) |
| Worsening HF episodec | |||||||
| Never | 241 | 2493 | 8.2 (6.9-9.7) | 1 [Reference] | 1 [Reference] | 5.9 (4.8-7.1) | 0.72 (0.56-0.93) |
| >12 mo | 112 | 950 | 9.4 (7.3-12.1) | 1.18 (0.95-1.48) | 1.19 (0.95-1.49) | 6.9 (5.8-9.9) | 0.80 (0.55-1.16) |
| ≤12 mo | 210 | 1301 | 15.0 (12.6-17.9) | 1.73 (1.44-2.08) | 1.56 (1.29-1.88) | 9.6 (7.8-12.0) | 0.64 (0.48-0.84) |
| Cardiovascular death | |||||||
| Never | 253 | 2493 | 7.4 (6.2-8.7) | 1 [Reference] | 1 [Reference] | 6.7 (5.6-8.0) | 0.91 (0.71-1.16) |
| >12 mo | 97 | 950 | 8.1 (6.2-10.6) | 0.98 (0.77-1.23) | 1.01 (0.80-1.29) | 5.9 (4.3-7.9) | 0.74 (0.49-1.11) |
| ≤12 mo | 150 | 1301 | 9.2 (7.4-11.4) | 1.14 (0.93-1.40) | 0.98 (0.80-1.21) | 7.0 (5.5-8.9) | 0.76 (0.55-1.05) |
Both models include randomized treatment as a factor and are stratified by baseline diabetes status. Adjusted hazard ratios are adjusted for age, sex, race, left ventricular ejection fraction, baseline N-terminal pro-B-type natriuretic peptide concentration, and New York Heart Association class.
Dapagliflozin vs placebo.
Hospitalization for HF or an urgent HF visit.
Efficacy and Safety of Dapagliflozin
Dapagliflozin reduced the relative risk of the primary outcome by 16% (HR, 0.84 [95% CI, 0.69-1.01]) in patients with no prior history of HF hospitalization, 27% (HR, 0.73 [95% CI, 0.54-0.99]) in those with an HF hospitalization more than 1 year prior to enrollment, and 36% (HR, 0.64 [95% CI, 0.51-0.81]) in those with an HF hospitalization within 12 months of trial enrollment (P = .07 for trend for HR) (Table 2). These relative risk reductions, coupled with the higher baseline risk, led to correspondingly greater ARRs at 2 years across the groups: 2.1% (95% CI, −1.9% to 6.1%), 4.1% (95% CI, −3.6% to 11.7%), and 9.9% (95% CI, 3.3%-16.5%), respectively (P = .05 for trend for ARR) (Figure 3). This pattern was consistent in patients with and without type 2 diabetes (eTable 1 in the Supplement). There was no excess in risk of any of the prespecified adverse events with dapagliflozin vs placebo within any of these subgroups (eTable 2 in the Supplement).
Figure 3. Treatment Effect of Dapagliflozin on the Primary Composite Outcome by Timing of Most Recent Heart Failure (HF) Hospitalization Relative to Trial Enrollment.
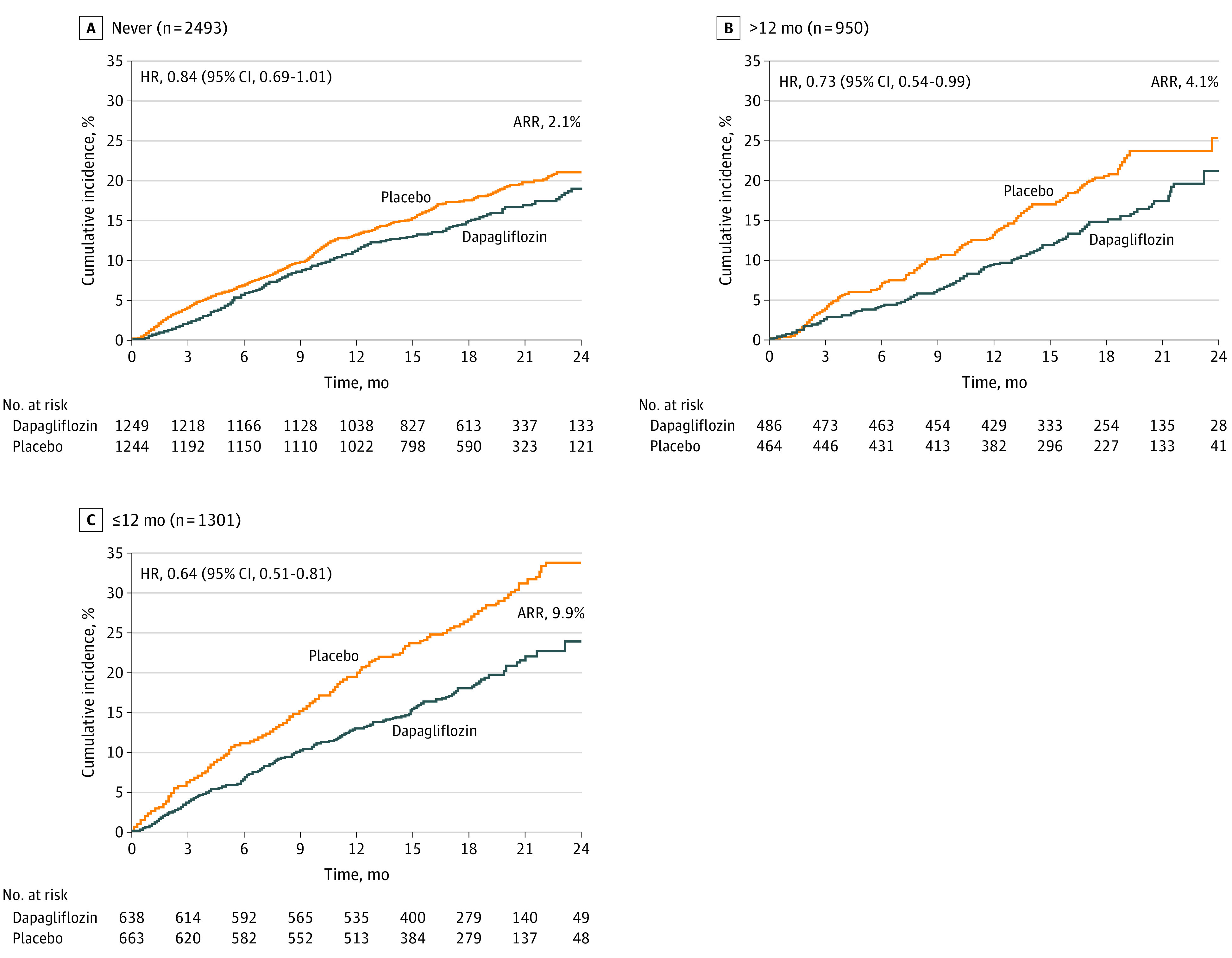
Patients with a more recent hospitalization for HF experienced robust relative and absolute risk reductions in the primary efficacy outcome of cardiovascular death or worsening heart failure. ARR indicates absolute risk reduction; HR, hazard ratio.
Discussion
In this analysis from the DAPA-HF trial, we found that the clinical benefit of dapagliflozin for reducing the risk of cardiovascular death or worsening HF was rapidly apparent, with a sustained statistically significant benefit as soon as 4 weeks after randomization. These data are consistent with the findings from the Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction (EMPEROR-Reduced) trial, in which there was a sustained statistically significant benefit of empagliflozin on the primary efficacy end point at 34 days after randomization,7 and they underscore the opportunity for early clinical benefit when initiating dapagliflozin use in patients with chronic HFrEF. In addition, we found that proximity to prior HF hospitalization was associated with an increased risk of worsening HF or cardiovascular death, as well as with a gradient of absolute treatment benefit from dapagliflozin. In view of the emphasis that guidelines place on optimizing treatment approaches to improve outcomes following HF hospitalization,5 these data suggest that optimizing guideline-directed medical therapy with SGLT2 inhibition is beneficial in all patients with chronic, symptomatic HFrEF and may be particularly helpful with respect to ARR in those with a more recent hospitalization for worsening HF.
Overcoming Clinical Inertia
The rapid time to clinical benefit highlights the risk of delaying initiation of dapagliflozin in patients with HFrEF, a chronic, progressive disease with an insidious course that is often undertreated. Despite an extensive evidence base from clinical trials and clear guidelines from cardiovascular professional societies, use of comprehensive medical therapies for the treatment of HFrEF remains woefully suboptimal in clinical practice, and most patients are treated only with renin-angiotensin system inhibitors and β-blockers.2 In addition to an expanded focus on implementation science, improved messaging to clinicians and patients may be critical to promote faster and more widespread adoption of these highly efficacious therapies. Similarly, awareness that the benefits of dapagliflozin are realized very early after initiating therapy, as demonstrated in this analysis, may underscore the urgency of doing so.
Timing of Clinical Benefit From SGLT2 Inhibition
The rapid time to clinical benefit from dapagliflozin in patients with chronic HFrEF also raises important questions about the mechanisms by which SGLT2 inhibition prevents worsening HF and cardiovascular death, an area of intense interest and investigation. For many cardiovascular therapies, there is a delay between initiation of treatment and benefit on cardiovascular outcomes that depends on the mechanism of action and underlying pathobiological state. For example, the benefit of lipid-lowering therapies for preventing complications of atherosclerotic cardiovascular disease is generally not realized for 6 to 12 months, owing to the time necessary to alter atherosclerotic plaque composition and, in turn, decrease atherothrombotic events. In contrast, the immediate clinical outcome of dapagliflozin use in patients with chronic HFrEF may implicate early physiologic changes, including direct hemodynamic and decongestive effects, as key drivers of the drug’s early benefit.
In support of this hypothesis, a small placebo-controlled randomized clinical trial of the SGLT2 inhibitor empagliflozin in patients with acute HF demonstrated that SGLT2 inhibition leads to increased urinary output and a more negative fluid balance in the days following initiation of therapy.8 Similarly, a recent mechanistic study of empagliflozin in ambulatory patients with chronic HF demonstrated that treatment with SGLT2 inhibitors results in early and substantial natriuresis and plasma volume contraction.9
Importantly, though, the apparent magnitude of clinical benefit with SGLT2 inhibitors is greater than one would expect from direct hemodynamic and decongestive effects alone; therefore, it is likely that other mechanisms play an important role. The same mechanistic study also showed that, in contrast with the pattern observed with other diuretics, empagliflozin-mediated natriuresis did not result in neurohormonal activation, which may, in part, account for its favorable cardiovascular profile.9 Furthermore, mediation analyses from other SGLT2 inhibitor trial cohorts have identified hematocrit increase as a potential mediator of the treatment benefit of SGLT2 inhibitors.10,11 Although this physiologic change may partly reflect plasma volume contraction, it may also be caused by early and sustained increases in erythropoietin,12 which may in turn be a marker for other cardioprotective biological processes.
Prior HF Hospitalization and Benefit of Dapagliflozin
Consistent with prior studies, our analysis demonstrates that HF hospitalization is an important indicator of risk in patients with chronic HFrEF. Furthermore, these data suggest that timing of prior HF hospitalization may identify patients who are likely to derive a greater absolute treatment benefit from SGLT2 inhibition. Although the mechanisms by which dapagliflozin prevents worsening HF and cardiovascular death remain incompletely understood, it is plausible that the hemodynamic and decongestive benefits of SGLT2 inhibition may be more pronounced in patients who are prone to acute decompensation, a condition that is characterized by clinically overt congestion. Regardless of the mechanism, these data suggest that patients with chronic, symptomatic HFrEF benefit from SGLT2 inhibition and those who have been more recently hospitalized for HF experience especially large ARRs of cardiovascular death or hospitalization for HF with dapagliflozin.
Limitations
There are several limitations of this analysis that deserve mention. First, this was a post hoc analysis of a clinical trial; therefore, these data should be considered hypothesis generating and are most directly relevant to patients who meet the trial enrollment criteria. Second, the confidence limits surrounding the HR estimates in the LOWESS plot are a function of the number of primary efficacy outcomes, which in turn depends on the trial sample size. It should therefore be acknowledged that the time to statistical significance of the clinical benefit may be a consequence not only of the pharmacodynamic effects of dapagliflozin but also the trial design. Third, the timing of the most recent HF hospitalization relative to trial enrollment was captured in categorical bins in the case record form, so a more granular assessment of clinical risk and treatment benefit as a function of proximity to prior HF hospitalization was not possible. Finally, the DAPA-HF trial excluded patients who were in the midst of an HF hospitalization or who had been hospitalized for HF within the preceding 4 weeks. Therefore, these data should not be interpreted as providing evidence for the efficacy or safety of dapagliflozin during HF hospitalization or in the vulnerable immediate posthospitalization period, when patients may be more susceptible to therapy-associated complications because of active modulation of diuretic therapy, fluctuating kidney function, and concomitant dose adjustment of neurohormonal antagonists. This is the focus of ongoing clinical trials evaluating in-hospital initiation of dapagliflozin (NCT04363697) and empagliflozin (NCT04157751) in patients hospitalized for acute HF.
Conclusions
In patients with chronic HFrEF, dapagliflozin rapidly reduced the risk of cardiovascular death or worsening HF, with a sustained statistically significant benefit emerging very early after randomization. Patients in closer proximity to a prior HF hospitalization were not only at high risk for recurrent events, but also experienced robust relative risk reductions and ARRs when treated with dapagliflozin. Taken together, these data highlight the opportunity for rapid clinical benefit when initiating dapagliflozin in all patients with chronic HFrEF and the particularly large ARRs that can be realized with prompt initiation of therapy in patients who have recently been hospitalized for HF.
eTable 1. Effect of dapagliflozin on the primary efficacy outcome by timing of most recent heart failure hospitalization in relation to trial enrollment in patients with and without type 2 diabetes mellitus.
eTable 2. Adverse events by timing of most recent heart failure hospitalization in relation to trial enrollment.
References
- 1.McMurray JJV, Solomon SD, Inzucchi SE, et al. ; DAPA-HF Trial Committees and Investigators . Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008. doi: 10.1056/NEJMoa1911303 [DOI] [PubMed] [Google Scholar]
- 2.Greene SJ, Butler J, Albert NM, et al. Medical therapy for heart failure with reduced ejection fraction: the CHAMP-HF Registry. J Am Coll Cardiol. 2018;72(4):351-366. doi: 10.1016/j.jacc.2018.04.070 [DOI] [PubMed] [Google Scholar]
- 3.Solomon SD, Dobson J, Pocock S, et al. ; Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) Investigators . Influence of nonfatal hospitalization for heart failure on subsequent mortality in patients with chronic heart failure. Circulation. 2007;116(13):1482-1487. doi: 10.1161/CIRCULATIONAHA.107.696906 [DOI] [PubMed] [Google Scholar]
- 4.Bello NA, Claggett B, Desai AS, et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ Heart Fail. 2014;7(4):590-595. doi: 10.1161/CIRCHEARTFAILURE.113.001281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161. doi: 10.1161/CIR.0000000000000509 [DOI] [PubMed] [Google Scholar]
- 6.McMurray JJV, DeMets DL, Inzucchi SE, et al. ; DAPA-HF Committees and Investigators . A trial to evaluate the effect of the sodium-glucose co-transporter 2 inhibitor dapagliflozin on morbidity and mortality in patients with heart failure and reduced left ventricular ejection fraction (DAPA-HF). Eur J Heart Fail. 2019;21(5):665-675. doi: 10.1002/ejhf.1432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Packer M, Anker SD, Butler J, et al. ; EMPEROR-Reduced Trial Committees and Investigators . Effect of empagliflozin on the clinical stability of patients with heart failure and a reduced ejection fraction: the EMPEROR-reduced trial. Circulation. Published October 21, 2020. doi: 10.1161/CIRCULATIONAHA.120.051783 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Damman K, Beusekamp JC, Boorsma EM, et al. Randomized, double-blind, placebo-controlled, multicentre pilot study on the effects of empagliflozin on clinical outcomes in patients with acute decompensated heart failure (EMPA-RESPONSE-AHF). Eur J Heart Fail. 2020;22(4):713-722. doi: 10.1002/ejhf.1713 [DOI] [PubMed] [Google Scholar]
- 9.Griffin M, Rao VS, Ivey-Miranda J, et al. Empagliflozin in heart failure: diuretic and cardiorenal effects. Circulation. 2020;142(11):1028-1039. doi: 10.1161/CIRCULATIONAHA.120.045691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Inzucchi SE, Zinman B, Fitchett D, et al. How does empagliflozin reduce cardiovascular mortality? insights from a mediation analysis of the EMPA-REG OUTCOME trial. Diabetes Care. 2018;41(2):356-363. doi: 10.2337/dc17-1096 [DOI] [PubMed] [Google Scholar]
- 11.Li J, Woodward M, Perkovic V, et al. Mediators of the effects of canagliflozin on heart failure in patients with type 2 diabetes. JACC Heart Fail. 2020;8(1):57-66. doi: 10.1016/j.jchf.2019.08.004 [DOI] [PubMed] [Google Scholar]
- 12.Mazer CD, Hare GMT, Connelly PW, et al. Effect of empagliflozin on erythropoietin levels, iron stores, and red blood cell morphology in patients with type 2 diabetes mellitus and coronary artery disease. Circulation. 2020;141(8):704-707. doi: 10.1161/CIRCULATIONAHA.119.044235 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Effect of dapagliflozin on the primary efficacy outcome by timing of most recent heart failure hospitalization in relation to trial enrollment in patients with and without type 2 diabetes mellitus.
eTable 2. Adverse events by timing of most recent heart failure hospitalization in relation to trial enrollment.