

Key Points
Question
What are the treatment outcomes and adverse effects of surgical interventions for patients with vitiligo?
Findings
In this systematic review and meta-analysis that included 117 unique studies and 8776 unique patients, the rates of repigmentation above 90% and above 50% after a single session of all surgical interventions were 52.69% and 81.01%, respectively.
Meaning
These findings suggest that surgical intervention can be an effective and safe option for managing refractory stable vitiligo; selection of appropriate patients in terms of disease stability and suitable surgical procedure is important.
This systematic review and meta-analysis investigates the treatment response of different surgical modalities in patients with vitiligo.
Abstract
Importance
Surgical interventions are a key part of the therapeutic arsenal, especially in refractory and stable vitiligo. Comparison of treatment outcomes between the different surgical procedures and their respective adverse effects has not been adequately studied.
Objective
To investigate the reported treatment response following different surgical modalities in patients with vitiligo.
Data Sources
A comprehensive search of the MEDLINE, Embase, Web of Science, and Cochrane Library databases from the date of database inception to April 18, 2020, was conducted. The key search terms used were vitiligo, surgery, autologous, transplantation, punch, suction blister, and graft.
Study Selection
Of 1365 studies initially identified, the full texts of 358 articles were assessed for eligibility. A total of 117 studies were identified in which punch grafting (n = 19), thin skin grafting (n = 10), suction blister grafting (n = 29), noncultured epidermal cell suspension (n = 45), follicular cell suspension (n = 9), and cultured epidermal cell suspension (n = 17) were used.
Data Extraction and Synthesis
Three reviewers independently extracted data on study design, patients, intervention characteristics, and outcomes. Random effects meta-analyses using generic inverse-variance weighting were performed.
Main Outcomes and Measures
The primary outcomes were the rates of greater than 90%, 75%, and 50% repigmentation response. These rates were calculated by dividing the number of participants in an individual study who showed the corresponding repigmentation by the total number of participants who completed the study. The secondary outcomes were the factors associated with treatment response to the surgical intervention.
Results
Among the 117 unique studies and 8776 unique patients included in the analysis, rate of repigmentation of greater than 90% for surgical interventions was 52.69% (95% CI, 46.87%-58.50%) and 45.76% (95% CI, 30.67%-60.85%) for punch grafting, 72.08% (95% CI, 54.26%-89.89%) for thin skin grafting, 61.68% (95% CI, 47.44%-75.92%) for suction blister grafting, 47.51% (95% CI, 37.00%-58.03%) for noncultured epidermal cell suspension, 36.24% (95% CI, 18.92%-53.57%) for noncultured follicular cell suspension, and 56.82% (95% CI, 48.93%-64.71%) for cultured epidermal cell suspension. The rate of repigmentation of greater than 50% after any surgical intervention was 81.01% (95% CI, 78.18%-83.84%). In meta-regression analyses, the treatment response was associated with patient age (estimated slope, −1.1418), subtype of vitiligo (estimated slope, 0.3047), and anatomical sites (estimated slope, −0.4050).
Conclusions and Relevance
The findings of this systematic review and meta-analysis suggest that surgical intervention can be an effective option for refractory stable vitiligo. An appropriate procedure should be recommended based on patient age, site and size of the lesion, and costs.
Introduction
Vitiligo is a skin disease characterized by the chronic loss of functional melanocytes. The disease deeply affects quality of life in these individuals, and treatment options remain limited.1,2 Medical treatments in vitiligo include phototherapy, topical corticosteroids, topical calcineurin inhibitors, and combination therapies. However, recent systematic reviews3,4,5 have shown that these treatments provide only partial repigmentation in most treated individuals. Surgical interventions are an alternative therapeutic option in patients with stable vitiligo that is resistant to conventional medical approaches.6
Since thin split-thickness skin grafting was first reported to successfully repigment vitiliginous patches in 1947, various surgical methods have been developed for the treatment of vitiligo, including transplant and grafting techniques.7 However, the efficacy and safety of these surgical interventions has not recently been investigated systematically. In the present study, we performed a systematic review and meta-analysis of all relevant prospective and retrospective studies to estimate the treatment responses following each type of surgical intervention for vitiligo.
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline and reviewed and approved by the institutional review board of St Vincent’s Hospital, Seoul, Korea. The study was registered with PROSPERO, an international database of prospectively registered systematic reviews.8
Databases
We performed a comprehensive search using predefined search terms (eTable 1 in the Supplement) in the MEDLINE, Embase, Web of Science, and Cochrane Library databases from inception to April 18, 2020. The main search terms were autologous, melanocyte, surgery, suspension, transplantation, transplant, graft, grafting, blister, punch, thin, split thickness, and vitiligo. All prospective and retrospective studies were included with no language restriction, and the reference lists in relevant review articles were scanned manually as well. All articles identified by this search were screened independently by 3 reviewers for study eligibility and data extraction (H.J.J., R.W.L., and S.H.K.).
Study Selection
Study selection was based on the following inclusion criteria: (1) prospective and retrospective studies; (2) participants of all age groups with a diagnosis of vitiligo; (3) at least 1 surgical intervention group; (4) at least 10 participants in each treatment arm, regardless of the dropout rate; (5) outcomes measured based on all vitiligo lesions on the patient’s whole body or each target patch; and (6) outcomes measured according to the percentage of repigmentation. Exclusion criteria consisted of the following: (1) not a clinical study; (2) outcomes measured according to criteria other than percentage of repigmentation; (3) other intervention or combination with other intervention; (4) more than a single session of surgery; and (5) the inability to contact the corresponding authors.
Three reviewers (H.J.J., R.W.L., and S.H.K.) independently identified relevant articles by searching titles and abstracts. If the abstract did not provide enough information to determine inclusion or exclusion of the study, the reviewers performed a full-text evaluation to determine eligibility. The reviewers compared the results, and discrepancies were resolved through discussion.
Data Extraction and Outcome Measures
For the meta-analysis, the 3 independent reviewers extracted the following predefined variables: authors, country, year of publication, study type, numbers of treated patients or lesions, treatment protocols, and outcome. We performed data extraction in duplicate, and any discrepancies were resolved by consensus.
Treatment Response Following Surgical Interventions and Safety Profiles
The outcome of repigmentation was evaluated as greater than 90%, greater than 75%, and greater than 50%. The treatment response rates were calculated as the number of participants or lesions who achieved the corresponding degree of repigmentation divided by the total number of participants or lesions who completed the individual study. Patients with unstable vitiligo, piebaldism, or other types of leukoderma were excluded from the analysis, whenever possible. We investigated all reported adverse events for each surgical intervention in the included studies.
Meta-regression of Age, Vitiligo Subtype, and Body Sites
Meta-regression was performed to investigate factors associated with the achievement of greater than 90% repigmentation. Selective moderating variables, such as the type of surgical intervention, age, vitiligo subtype, and the body site were investigated for that purpose. We collected the mean age of patients, proportion of segmental vitiligo, and proportion of treated lesions on the acral and joint areas in the enrolled participants for each study, whenever this was possible.
Statistical Analysis
The rates of the corresponding treatment responses of the included studies were pooled by generic inverse variance weighting and were combined using a random-effects model. In each subgroup analysis, heterogeneity was assessed using the Cochran Q test and I2 value. Influence of variables on the outcome were analyzed using meta-regression. Publication bias was evaluated using the contoured funnel plot (eFigure 1 in the Supplement). Statistical analyses were conducted using R software, version 3.6.1 (R Foundation for Statistical Computing) with the metagen and metafor packages. Two-sided P < .05 indicated significance.
Results
Search Results
We initially identified 1365 records through database searching; 656 duplicates were removed and 351 were deleted after reviewing the titles and abstracts (Figure 1). A total of 358 full-text articles were assessed for eligibility, of which 241 were excluded for the following reasons: (1) not a clinical study (n = 23); (2) less than 10 participants included (n = 61); (3) abstract only or not enough information about the methods (n = 31); (4) outcomes measured according to criteria other than percentage of repigmentation (n = 61); (5) not a single-session surgery (n = 16); (6) other intervention used with surgery (n = 7); (7) duplicated studies (n = 14); and (8) the inability to reach corresponding authors at least twice by email (n = 28). The remaining 117 studies fulfilled the inclusion criteria and were included in the final analysis.
Figure 1. Flow Diagram Showing Identification of Eligible Studies.

Characteristics of Included Studies
We analyzed a total of 117 unique studies with 8776 unique patients (eTable 1 in the Supplement), including 19 studies9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27 with 1631 patients in the punch grafting group, 10 studies15,20,28,29,30,31,32,33,34,35 with 718 patients in the thin skin grafting group, 29 studies10,24,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62 with 2652 patients in the suction blister grafting group, 45 studies21,51,56,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104 with 2209 patients in the noncultured epidermal cell suspension (NCES) group, 9 studies75,87,93,105,106,107,108,109,110 with 185 patients in the noncultured follicular cell suspension (NCFS) group, and 17 studies56,81,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125 with 1381 patients in the cultured epidermal cell suspension (CES) group; 11 studies included more than 1 procedure type. The median follow-up duration was 7 (range, 2-108) months. The Methodological Index for Non-randomized Studies126 criteria scoring was used to assess the methodological quality for included studies (eTable 2 in the Supplement).
Treatment Response Following Surgical Intervention and Meta-regression
Overall, the rate of repigmentation achieved by patients after 1 session of any surgical intervention included greater than 90% in 52.69% (95% CI, 46.87%-58.50%) in 106 studies with 6586 patients (I2 = 97.2%) (eFigure 2 in the Supplement); greater than 75% in 64.72% (95% CI, 59.52%-69.92%) in 100 studies with 3400 patients (I2 = 95.7%); and greater than 50% in 81.01% (95% CI, 78.18%-83.84%) in 92 studies with 5462 patients (I2 = 90.7%). According to the surgical intervention type, greater than 90% repigmentation was achieved in 72.08% (95% CI, 54.26%-89.89%) of patients undergoing thin skin grafting (670 patients in 8 studies20,28,29,30,31,32,33,35), 61.68% (95% CI, 47.44%-75.92%) of patients undergoing suction blister grafting (2349 patients in 21 studies36,37,38,39,40,41,42,46,47,48,49,50,51,52,54,55,56,58,59,60,61), 56.82% (95% CI, 48.93%-64.71%) of patients undergoing CES (1138 patients in 14 studies56,111,112,113,114,115,116,117,118,119,120,121,122,123), 47.51% (95% CI, 37.00%-58.03%) of patients undergoing NCES (907 patients in 29 studies51,56,63,64,65,66,69,70,71,75,76,77,79,82,83,85,87,89,91,93,94,95,96,97,98,100,101,102,103), 45.76% (95% CI, 30.67%-60.85%) of patients undergoing punch grafting (1354 patients in 11 studies9,11,12,13,14,16,17,19,20,23,26), and 36.24% (95% CI, 18.92%-53.57%) of patients undergoing NCFS (160 patients in 8 studies75,87,93,105,106,107,109,110) after 1 session of each surgery (eFigure 2 in the Supplement and Table 1). In our meta-regression analysis, for greater than 90% repigmentation, the estimate of the slopes for mean age of patients was −1.1418 (P = .02); for the proportion of segmental vitiligo, 0.3047 (P = .01); and for the proportion of treated lesions on the acral and joint areas, −0.4050 (P = .002) (Figure 2).
Table 1. Summary of Findings for Surgical Interventions for Vitiligo.
| Intervention | Treatment response rate, % (95% CI) | Included studies | ||
|---|---|---|---|---|
| >90% Repigmentation | >75% Repigmentation | >50% Repigmentation | ||
| Punch grafting | 45.76 (30.67-60.85) | 56.78 (45.35-68.22) | 71.02 (62.23-79.80) | 1631 Patients in 19 studies9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27 |
| Thin skin grafting | 72.08 (54.26-89.89) | 76.17 (54.77-97.57) | 83.06 (71.47-94.65) | 718 Patients in 10 studies15,20,28,29,30,31,32,33,34,35 |
| Suction blister grafting | 61.68 (47.44-75.92) | 75.69 (68.09-83.39) | 88.85 (82.47-95.23) | 2652 Patients in 29 studies10,24,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62 |
| Noncultured epidermal cell suspension | 47.51 (37.00-58.03) | 63.42 (55.21-71.62) | 77.47 (70.90-84.05) | 2209 Patients in 45 studies21,51,56,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104 |
| Noncultured follicular cell suspension | 36.24 (18.92-53.57) | 53.25 (34.81-71.69) | 78.73 (65.86-91.60) | 185 Patients in 9 studies75,87,93,105,106,107,108,109,110 |
| Cultured epidermal cell suspension | 56.82 (48.93-64.71) | 70.73 (51.49-89.98) | 84.72 (80.67-88.77) | 1381 Patients in 17 studies56,81,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125 |
| All | 52.69 (46.87-58.50) | 64.72 (59.52-69.92) | 81.01 (78.18-83.84) | 8776 Patients in 117 studies9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125 |
Figure 2. Summary of Treatment Response Following Surgical Interventions for Vitiligo .
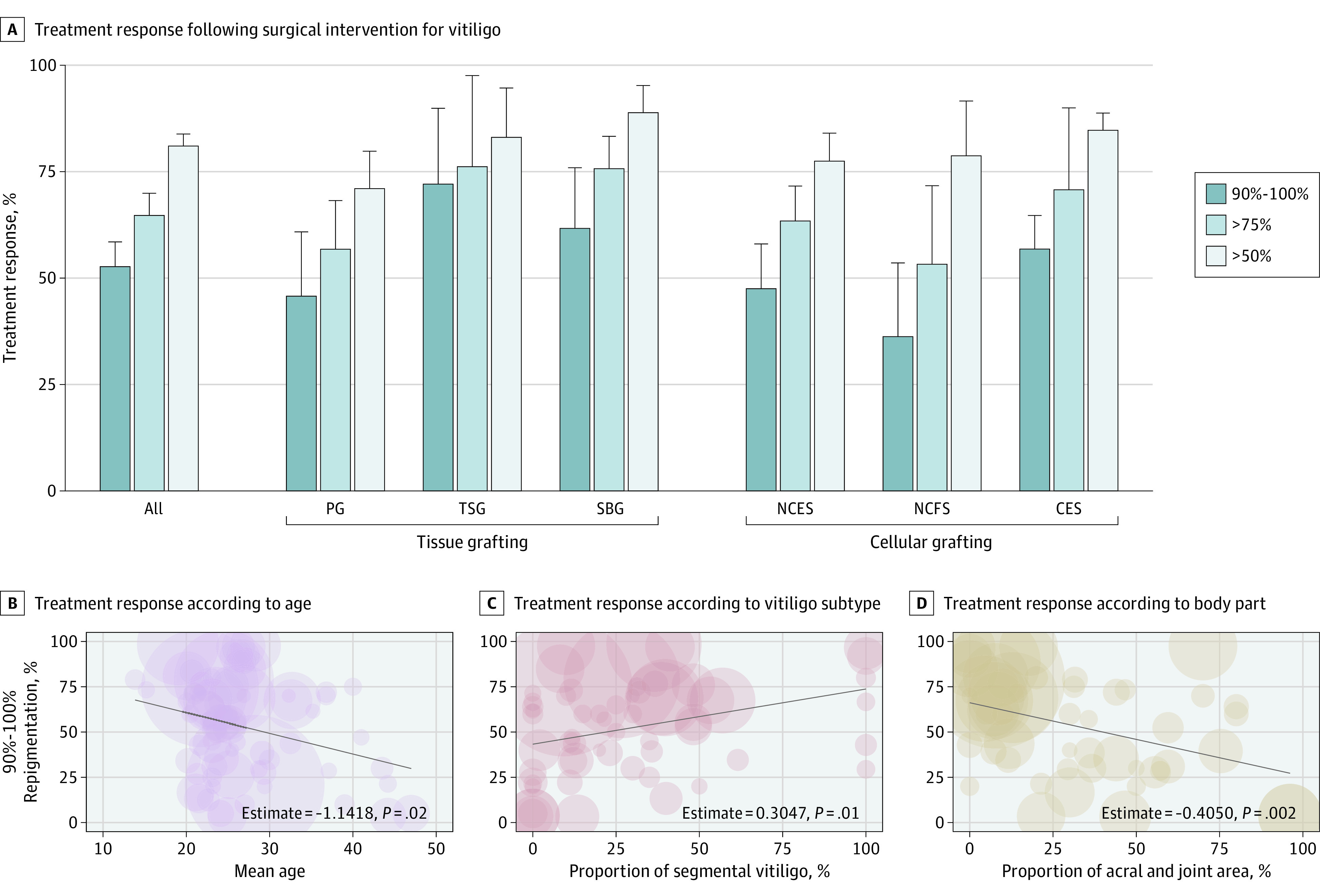
CES indicates cultured epidermal cell suspension; NCES, noncultured epidermal cell suspension; and NCFS, noncultured follicular cell suspension.
Safety of Each Surgical Intervention
The occurrence of adverse events was reported in 56 studies. Common adverse events included pain, hyperpigmentation at the recipient site, and hypopigmentation at the donor site regardless of the type of the procedure. In punch grafting, cobblestone appearance, milia, and color mismatch were the most common and critical adverse events.9,10,11,12,13,15,16,17,18,20,22,23,24,26,27 In suction blister grafting, perigraft halo, variegated appearance, and color mismatch were frequently reported.10,24,36,37,38,40,43,45,46,48,49,50,54,55,57,60 Thin skin grafting was associated with graft contracture, overhanging margin, wrinkles over the graft surface, and perigraft halo.15,20,28,29,30,31,33,34,35 In cellular grafting techniques, pain, discomfort, and burning sensation were more commonly reported when compared with tissue grafting,84,104 which was likely owing to multiple injections of local anesthetic performed over a large area in the former. Mottled pigmentation, marginal halo, and scarring were also reported in all the evaluated surgical interventions. Koebner phenomenon at the donor site or disease progression was reported in several studies as well,9,13,36,37,40,49,54,65,96,114,115 indicating a need for carefully assessing disease stability before performing surgery (Table 2).
Table 2. Common Adverse Events of Surgical Interventions.
| Intervention | Adverse events |
|---|---|
| Punch grafting | Recipient site: cobblestone appearance, variegated appearance, polka dots, color mismatch, infection, perilesional halo, insufficient repigmentation, hyperpigmentation |
| Donor site: Koebner phenomenon, scarring, infection | |
| Thin skin grafting | Recipient site: perigraft halo, milia, hypertrophic scarring, graft displacement, overhanging margin, partial graft loss, wrinkles over the graft surface, hyperpigmentation, reactivation or progression |
| Donor site: pain, hypertrophic scarring, hyperpigmentation, infection | |
| Suction blister grafting | Recipient site: hyperpigmentation, hypertrophic scar, perigraft halo, infection, color mismatch, reactivation or progression |
| Donor site: Koebner phenomenon, hyperpigmentation | |
| Noncultured epidermal cell suspension | Recipient site: color mismatch, hyperpigmentation, marginal halo, infection, mottled pigmentation, burning pain and discomfort |
| Donor site: Koebner phenomenon, infection, hypertrophic scar, hyperpigmentation | |
| Noncultured follicular cell suspension | Recipient site: color mismatch, hyperpigmentation, infection, pruritus, xerosis |
| Donor site: hyperpigmentation, hypertrophic scar, infection | |
| Cultured epidermal cell suspension | Recipient site: marginal halo, burning pain and pruritus |
Discussion
Surgical interventions are essential for the management of refractory stable vitiligo, which can be classified into tissue grafting and cellular grafting according to the nature of the grafts. Tissue grafting, including thin skin grafting, suction blister grafting, and punch grafting, has been traditionally performed for a long time, whereas cellular grafting has made a great advance in recent years. For many reasons, including ease of use and safety, NCES has greatly contributed to the reduced costs of surgical interventions for vitiligo, globally. A systematic review on surgical interventions for vitiligo was published in 2013,127 and the present study further includes all the articles published since then and derives the response rate for each surgical method.
In the present study, we systematically reviewed the treatment response following different types of surgical interventions for vitiligo, including punch grafting (19 studies), thin skin grafting (10 studies), suction blister grafting (29 studies), NCES (45 studies), NCFS (9 studies), and CES (17 studies). In meta-analysis, regardless of the type of intervention, 52.69% of the patients achieved greater than 90% repigmentation after a single surgical procedure. However, when evaluating this specific outcome according to the type of intervention, the highest response rate (for >90% repigmentation) was achieved in patients undergoing thin skin grafting (72.08%), followed by suction blister grafting (61.68%), CES (56.82%), NCES (47.51%), punch grafting (45.76%), and NCFS (36.24%).
The oldest reported surgical procedure performed in patients with vitiligo, thin skin grafting, encompasses all methods of transplanting ultrathin or thin skin grafts measuring 0.125 to 0.275 mm harvested using a manual or electronic dermatome.128 Various modifications have been added to the initially published method such as Thiersch,129 smash,130 and flit-top20 grafting. However, this technique is difficult to use on a large surface area and requires experienced skill to harvest the graft with a constant thickness.
Because thin skin grafting commonly leads to uneven pigmentation and scarring of the donor site, a surgical method to precisely harvest the epidermal graft has been attempted.131 Suction blister grafting, first described by Falabella132 in 1971, has decreased the risk of scarring of the donor site by raising subepidermal blisters with clear noninflammatory transudate and low suction pressures maintained for sufficient periods. It is safe and effective for vitiligo on junctional areas or curved areas such as lips or eyelids.133 Several studies46,58,61 reported that 87% to 90% of the lip vitiligo and 85.7% of vitiligo on the nipple and areolar showed complete repigmentation after suction blister grafting at 6 to 24 months.
Punch grafting is another well-established surgical method in vitiligo. Several motorized punch grafting devices have been put on the market in recent years, making this method more convenient and cost-effective with increased favorable outcomes.23 Moreover, repeated procedures can be easily performed in an outpatient setting. Despite the low overall treatment response following punch grafting shown in our meta-analysis, recent studies describe motorized micropunch grafting has a greatly increased response rate and reduced cobblestone appearance.23,134
Transplant of NCES is the most commonly performed cellular grafting technique for vitiligo. The procedure can treat large areas covering a ratio of donor to recipient of as much as 1:10. However, processing of the grafts is time-consuming, and the procedure itself is lengthy. In our study, greater than 90% repigmentation was achieved in 47.51%, and greater than 75% repigmentation was achieved in 63.42% after 1 session of NCES, which is slightly less than the previously reported success rate.63 Of note, treatment outcome in NCES is strongly related to the experience and skill of the surgeon and proper processing of the cell suspension. The initially reported method135 has undergone several modifications over time to improve repigmentation rates. For example, the use of hyaluronic acid instead of the patient’s serum was added to increase the viscosity and facilitate adherence of the cell suspension grafts.65 Furthermore, oral pulse betamethasone therapy started as early as 2 months after initial NCES procedure has been shown to enhance repigmentation in patients who underwent additional transplant.136
The hair follicle is an attractive reservoir, given its high density of melanocytes and melanocyte stem cells; however, NCFS was shown to be inferior to other surgical interventions in our study. Singh et al75 reported that greater than 90% repigmentation was observed in 83% of the NCES group and 65% of the NCFS group. The success rate of cellular grafting can be optimized as demonstrated in another randomized controlled study87 in which the combination of NCES and NCFS improved repigmentation rates compared with NCES alone (76% vs 57%).
Cultured epidermal cell suspension has been performed to expand the amount of autologous cell suspensions, allowing for wider graft areas. Cultured melanocytes at a density of 70 000 to 100 000 melanocytes/cm2 are transplanted to an area covering as much as 500 cm2. Hong et al116 reported that CES could provide the highest donor-to-recipient ratio to 1:60. However, melanocyte culture is time-consuming and costly and requires a laboratory specialized in cell culture and a highly stimulatory media.111 Basic fibroblast growth factor is an effective and safe media commonly used,137 but long-term safety of melanoma risk remains to be addressed.138
In our meta-regression analyses, successful outcome (>90% repigmentation) was associated with younger age, segmental vitiligo, and nonacral area (P < .05 for all). Therefore, selection of appropriate candidates would be a critical factor when considering the surgical intervention of vitiligo.
Phototherapy may also play an adjuvant role in surgical interventions for vitiligo by stimulating melanocyte spreading, inhibiting T lymphocytes, and suppressing the various cytokines to create a favorable environment for the transplanted melanocytes. Several studies reported narrow-band UV-B phototherapy before and after CES-accelerated repigmentation121 and adjuvant narrow-band UV-B phototherapy after NCES-enhanced repigmentation.97 In our study, subgroup analysis according to adjuvant phototherapy showed no significant difference in repigmentation rates. The large heterogeneity of these studies may limit the interpretation of the results; thus, randomized clinical trials to estimate the effect of adjuvant phototherapy are necessary.
The assessment of disease stability is critical when selecting appropriate candidates for surgical interventions in patients with vitiligo. Evaluation with digital photographs during a 12-month period in addition to a scoring system such as the Vitiligo Area Scoring Index139 or the Vitiligo European Task Force140 assessment score is recommended.141 However, many studies were performed before the publication of these recommendations, and a great heterogeneity of definition of the length of stability was observed ranging from 3 to 12 months. The most commonly used scoring system, the Vitiligo Disease Activity Score,142 could also lead to recall bias. As a result, Koebner phenomenon at the donor site after surgery was commonly reported. This reflects how the adequate assessment of disease stability would be essential when considering surgical options; therefore, test grafting or patient-reported Vitiligo Noticeability Scale scores143 could be useful options because they are quick, simple, and readily interpreted in the outpatient clinic.28
Long-term treatment outcomes are also an important aspect for patients deciding to undergo surgical treatments. Patients expect not only repigmentation but also maintenance of gained repigmentation, expectations that were validated by international e-Delphi consensus.144 However, vitiligo often recurs after successful repigmentation, and prospective studies reporting the long-term outcome in surgical interventions are lacking. Fongers et al17 reported that at least 65% repigmentation was maintained in 51% and 89% of the patients with vitiligo vulgaris and segmental vitiligo, respectively, after several sessions of punch grafting (mean follow-up, 5.2 years). Al-Mutairi et al30 reported that the thin skin grafting with adjuvant excimer laser treatment led to long-lasting repigmentation for as long as 4 years. Jin et al49 observed that repigmentation significantly decreased over time, especially starting from 2 years after epidermal grafting. Altalhab et al88 reported that 103 of 553 patients who underwent a single session of melanocyte-keratinocyte transplant (18.6%) showed a relapse after 6-year follow-up; focal and segmental vitiligo showed a significantly lower recurrence rate.
Each surgical intervention for vitiligo has advantages and disadvantages. Therefore, the appropriate procedure should be recommended based on the patient’s age, economic status, the location and extent of vitiligo, and the facilities available at the clinic. Because complete repigmentation is rarely achieved after 1 session, multiple sessions are necessary to improve treatment outcome and patient satisfaction. Lesions of large areas can first be treated by cellular grafting, followed by tissue grafting for smaller remaining areas.145
Limitations
Our systematic review has limitations. First, there was considerable heterogeneity in study designs, demographic information, and protocols regarding preoperative and postoperative procedures. In particular, we observed a great heterogeneity of definition of outcome measures because the studies were published before the international consensus was reached. Repigmentation has currently reached consensus to use percentage of repigmentation quartiles, including 0 to 25%, 26% to 50%, 51% to 79%, and 80% to 100%.146 Second, limited evidence was available from randomized clinical trials or systematic reviews. Last, because the outcome of surgical interventions largely depends on the skill and experience of the clinician, actual outcomes may vary among the studies.
Conclusions
The findings of this systematic review and meta-analysis confirm that surgical interventions are essential for the management of refractory stable vitiligo. Maximizing treatment outcomes requires the selection of appropriate patients in terms of disease stability and suitable surgical technique. In the future, we should categorize patients for the surgical procedure that is performed. Consensus among physicians should also be reached on preoperative evaluations and postoperative assessments.
eTable 1. Clinical Characteristics of Studies Included in This Meta-analysis
eTable 2. Methodological Index for Nonrandomized Studies (MINORS) Criteria Scoring for Included Studies
eFigure 1. Contoured Funnel Plot of >90% Repigmentation Rate
eFigure 2. Treatment Response (>90% Repigmentation) of Surgical Interventions in Patients With Vitiligo
eReferences.
References
- 1.Rodrigues M, Ezzedine K, Hamzavi I, Pandya AG, Harris JE; Vitiligo Working Group . New discoveries in the pathogenesis and classification of vitiligo. J Am Acad Dermatol. 2017;77(1):1-13. doi: 10.1016/j.jaad.2016.10.048 [DOI] [PubMed] [Google Scholar]
- 2.Bae JM, Lee SC, Kim TH, et al. Factors affecting quality of life in patients with vitiligo: a nationwide study. Br J Dermatol. 2018;178(1):238-244. doi: 10.1111/bjd.15560 [DOI] [PubMed] [Google Scholar]
- 3.Ezzedine K, Whitton M, Pinart M. Interventions for vitiligo. JAMA. 2016;316(16):1708-1709. doi: 10.1001/jama.2016.12399 [DOI] [PubMed] [Google Scholar]
- 4.Bae JM, Jung HM, Hong BY, et al. Phototherapy for vitiligo: a systematic review and meta-analysis. JAMA Dermatol. 2017;153(7):666-674. doi: 10.1001/jamadermatol.2017.0002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lee JH, Kwon HS, Jung HM, et al. Treatment outcomes of topical calcineurin inhibitor therapy for patients with vitiligo: a systematic review and meta-analysis. JAMA Dermatol. 2019;155(8):929-938. doi: 10.1001/jamadermatol.2019.0696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Holla AP, Parsad D. Vitiligo surgery: its evolution as a definite treatment in the stable vitiligo. G Ital Dermatol Venereol. 2010;145(1):79-88. [PubMed] [Google Scholar]
- 7.Khunger N, Kathuria SD, Ramesh V. Tissue grafts in vitiligo surgery—past, present, and future. Indian J Dermatol. 2009;54(2):150-158. doi: 10.4103/0019-5154.53196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.National Institute for Health Research. Treatment outcomes of surgical treatments for vitiligo: systematic review and meta-analysis. CRD42020186777. Accessed April 18, 2020. https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=186777
- 9.Boersma BR, Westerhof W, Bos JD. Repigmentation in vitiligo vulgaris by autologous minigrafting: results in nineteen patients. J Am Acad Dermatol. 1995;33(6):990-995. doi: 10.1016/0190-9622(95)90292-9 [DOI] [PubMed] [Google Scholar]
- 10.Gupta S, Jain VK, Saraswat PK. Suction blister epidermal grafting versus punch skin grafting in recalcitrant and stable vitiligo. Dermatol Surg. 1999;25(12):955-958. doi: 10.1046/j.1524-4725.1999.99069.x [DOI] [PubMed] [Google Scholar]
- 11.Malakar S, Dhar S. Treatment of stable and recalcitrant vitiligo by autologous miniature punch grafting: a prospective study of 1,000 patients. Dermatology. 1999;198(2):133-139. doi: 10.1159/000018089 [DOI] [PubMed] [Google Scholar]
- 12.Sarkar R, Mehta SD, Kanwar AJ. Repigmentation after autologous miniature punch grafting in segmental vitiligo in North Indian patients. J Dermatol. 2001;28(10):540-546. doi: 10.1111/j.1346-8138.2001.tb00027.x [DOI] [PubMed] [Google Scholar]
- 13.Hallaji Z, Daneshpazhooh M, Rezai-Khiabanloo S. Successful treatment of vitiligo with punch graft followed by outdoor topical psoralen plus ultraviolet a radiation. Arch Iranian Med. 2003;6(2):86-90. [Google Scholar]
- 14.Ghorpade A. Use of tissue glue for punch grafting in vitiligo—a preliminary report. Indian J Dermatol Venereol Leprol. 2004;70(3):159-161. [PubMed] [Google Scholar]
- 15.Khandpur S, Sharma VK, Manchanda Y. Comparison of minipunch grafting versus split-skin grafting in chronic stable vitiligo. Dermatol Surg. 2005;31(4):436-441. doi: 10.1097/00042728-200504000-00010 [DOI] [PubMed] [Google Scholar]
- 16.Masood Q, Majid I, Hassan I, Khan D. Miniature punch grafting in recalcitrant vitiligo. JK Pract. 2005;12(2):81-82. [Google Scholar]
- 17.Fongers A, Wolkerstorfer A, Nieuweboer-Krobotova L, Krawczyk P, Tóth GG, van der Veen JP. Long-term results of 2-mm punch grafting in patients with vitiligo vulgaris and segmental vitiligo: effect of disease activity. Br J Dermatol. 2009;161(5):1105-1111. doi: 10.1111/j.1365-2133.2009.09367.x [DOI] [PubMed] [Google Scholar]
- 18.Feetham HJ, Chan JL, Pandya AG. Characterization of clinical response in patients with vitiligo undergoing autologous epidermal punch grafting. Dermatol Surg. 2012;38(1):14-19. doi: 10.1111/j.1524-4725.2011.02171.x [DOI] [PubMed] [Google Scholar]
- 19.Linthorst Homan MW, Spuls PI, Nieuweboer-Krobotova L, et al. A randomized comparison of excimer laser versus narrow-band ultraviolet B phototherapy after punch grafting in stable vitiligo patients. J Eur Acad Dermatol Venereol. 2012;26(6):690-695. doi: 10.1111/j.1468-3083.2011.04147.x [DOI] [PubMed] [Google Scholar]
- 20.Sharma S, Garg VK, Sarkar R, Relhan V. Comparative study of flip-top transplantation and punch grafting in stable vitiligo. Dermatol Surg. 2013;39(9):1376-1384. doi: 10.1111/dsu.12263 [DOI] [PubMed] [Google Scholar]
- 21.Kumar R, Singh SK, Gupta AK, Patel PK, Chhachhi H, Patel RK. Comparative study of efficacy of non-cultured melanocyte transfer technique and punch grafting technique in the management of stable vitiligo. J Evolution Med Dent Sci. 2015;4(102):16754-16758. doi: 10.14260/jemds/2015/2509 [DOI] [Google Scholar]
- 22.Mohamed Mohamed EE, Younes AK, Osmand A, Mohamed R, Makki M, Younis M. Punch graft versus follicular hair transplantation in the treatment of stable vitiligo. J Cosmet Laser Ther. 2017;19(5):290-293. doi: 10.1080/14764172.2017.1303170 [DOI] [PubMed] [Google Scholar]
- 23.Bae JM, Lee JH, Kwon HS, Kim J, Kim DS. Motorized 0.8-mm micropunch grafting for refractory vitiligo: a retrospective study of 230 cases. J Am Acad Dermatol. 2018;79(4):720-727.e1. doi: 10.1016/j.jaad.2018.06.016 [DOI] [PubMed] [Google Scholar]
- 24.Ezz-Eldawla R, Abu El-Hamd M, Saied SM, Hassanien SH. A comparative study between suction blistering graft, mini punch graft, and hair follicle transplant in treatment of patients with stable vitiligo. J Dermatolog Treat. 2019;30(5):492-497. doi: 10.1080/09546634.2018.1528329 [DOI] [PubMed] [Google Scholar]
- 25.Zhao T, Ye Z, Gao T, Li S, Li C.. Mini-punch grafting for the treatment of refractory and stable vitiligo. J Invest Dermatol. 2019;139(5):S97. doi: 10.1016/j.jid.2019.03.638 [DOI] [Google Scholar]
- 26.Anbar T, Abd El Raheem T, Bassiouny DA, et al. Value of silicone gel in prevention of cobblestoning following punch minigrafting in vitiligo. J Dermatolog Treat. Published online April 13, 2020. [DOI] [PubMed] [Google Scholar]
- 27.Kim DS, Ju HJ, Lee HN, et al. Skin seeding technique with 0.5-mm micropunch grafting for vitiligo irrespective of the epidermal-dermal orientation: animal and clinical studies. J Dermatol. 2020;47(7):749-754. doi: 10.1111/1346-8138.15390 [DOI] [PubMed] [Google Scholar]
- 28.Agrawal K, Agrawal A. Vitiligo: repigmentation with dermabrasion and thin split-thickness skin graft. Dermatol Surg. 1995;21(4):295-300. doi: 10.1111/j.1524-4725.1995.tb00176.x [DOI] [PubMed] [Google Scholar]
- 29.Kahn AM, Cohen MJ. Repigmentation in vitiligo patients: melanocyte transfer via ultra-thin grafts. Dermatol Surg. 1998;24(3):365-367. doi: 10.1111/j.1524-4725.1998.tb04168.x [DOI] [PubMed] [Google Scholar]
- 30.Al-Mutairi N, Manchanda Y, Al-Doukhi A, Al-Haddad A. Long-term results of split-skin grafting in combination with excimer laser for stable vitiligo. Dermatol Surg. 2010;36(4):499-505. doi: 10.1111/j.1524-4725.2010.01477.x [DOI] [PubMed] [Google Scholar]
- 31.Majid I, Imran S. Ultrathin split-thickness skin grafting followed by narrowband UVB therapy for stable vitiligo: an effective and cosmetically satisfying treatment option. Indian J Dermatol Venereol Leprol. 2012;78(2):159-164. doi: 10.4103/0378-6323.93632 [DOI] [PubMed] [Google Scholar]
- 32.Sheth VM, Currimbhoy SD, Feetham HJ, et al. Efficacy of narrowband ultraviolet B versus excimer radiation in repigmenting vitiligo after minigrafting on the distal arms. J Am Acad Dermatol. 2012;67(2):318-320. doi: 10.1016/j.jaad.2012.02.045 [DOI] [PubMed] [Google Scholar]
- 33.Majid I. Ultra-thin skin grafting in resistant stable vitiligo: factors affecting the treatment outcome. Pigment Cell Melanoma Res. 2014;27(5):988. [Google Scholar]
- 34.Sankara RK, Rao DS, Ramachandra BV, Srinivasulu G, Lakshmi NB. A study of split thickness skin graft technique in stable acral vitiligo. J Evolution Med Dental Sci. 2016;5(30):1581-1585. doi: 10.14260/jemds/2016/372 [DOI] [Google Scholar]
- 35.Majid I, Imran S. Ultrathin skin grafting in resistant stable vitiligo: a follow-up study of 8 years in 370 patients. Dermatol Surg. 2017;43(2):218-225. doi: 10.1097/DSS.0000000000000969 [DOI] [PubMed] [Google Scholar]
- 36.Hatchome N, Kato T, Tagami H. Therapeutic success of epidermal grafting in generalized vitiligo is limited by the Koebner phenomenon. J Am Acad Dermatol. 1990;22(1):87-91. doi: 10.1016/0190-9622(90)70013-8 [DOI] [PubMed] [Google Scholar]
- 37.Hann SK, Im S, Bong HW, Park YK. Treatment of stable vitiligo with autologous epidermal grafting and PUVA. J Am Acad Dermatol. 1995;32(6):943-948. doi: 10.1016/0190-9622(95)91329-7 [DOI] [PubMed] [Google Scholar]
- 38.Na GY. Autologous suction blister grafting for the treatment of vitiligo. Ann Dermatol. 1996;8(1):19-24. doi: 10.5021/ad.1996.8.1.19 [DOI] [Google Scholar]
- 39.Suga Y, Butt KI, Takimoto R, Fujioka N, Yamada H, Ogawa H. Successful treatment of vitiligo with PUVA-pigmented autologous epidermal grafting. Int J Dermatol. 1996;35(7):518-522. doi: 10.1111/j.1365-4362.1996.tb01673.x [DOI] [PubMed] [Google Scholar]
- 40.Kim HY, Kang KY. Epidermal grafts for treatment of stable and progressive vitiligo. J Am Acad Dermatol. 1999;40(3):412-417. doi: 10.1016/S0190-9622(99)70490-1 [DOI] [PubMed] [Google Scholar]
- 41.Lim JT. Repigmentation of vitiligo with autologous blister-induced epidermal grafts. Ann Acad Med Singap. 1999;28(6):824-828. [PubMed] [Google Scholar]
- 42.Gupta S, Kumar B. Epidermal grafting for vitiligo in adolescents. Pediatr Dermatol. 2002;19(2):159-162. doi: 10.1046/j.1525-1470.2002.00035.x [DOI] [PubMed] [Google Scholar]
- 43.Gupta S, Kumar B. Epidermal grafting in vitiligo: influence of age, site of lesion, and type of disease on outcome. J Am Acad Dermatol. 2003;49(1):99-104. doi: 10.1067/mjd.2003.415 [DOI] [PubMed] [Google Scholar]
- 44.Kim SE, Kim JR, Kim TH. The comparative study of the epidermal graft by suction blister between simple and complicated cases of vitiligo. Korean J Dermatol. 2003;41(6):716-721. [Google Scholar]
- 45.Cho WI, Kim JE, Seo SJ, Hong CK. The effect of autologous epidermal grafting in the treatment of intractable vitiligo. Korean J Dermatol. 2005;43(4):455-461. [Google Scholar]
- 46.Gupta S, Goel A, Kanwar AJ, Kumar B. Autologous melanocyte transfer via epidermal grafts for lip vitiligo. Int J Dermatol. 2006;45(6):747-750. doi: 10.1111/j.1365-4632.2006.02694.x [DOI] [PubMed] [Google Scholar]
- 47.Hasegawa T, Suga Y, Ikejima A, et al. Suction blister grafting with CO(2) laser resurfacing of the graft recipient site for vitiligo. J Dermatol. 2007;34(7):490-492. doi: 10.1111/j.1346-8138.2007.00317.x [DOI] [PubMed] [Google Scholar]
- 48.Babu A, Thappa DM, Jaisankar TJ. Punch grafting versus suction blister epidermal grafting in the treatment of stable lip vitiligo. Dermatol Surg. 2008;34(2):166-178. doi: 10.1097/00042728-200802000-00005 [DOI] [PubMed] [Google Scholar]
- 49.Jin Y, Xu A, Wang P, Song X, Liu X. Long-term follow-up and correlated factors of vitiligo following autologous epidermal transplantation. Cutis. 2011;87(3):137-141. [PubMed] [Google Scholar]
- 50.Li J, Fu WW, Zheng ZZ, Zhang QQ, Xu Y, Fang L. Suction blister epidermal grafting using a modified suction method in the treatment of stable vitiligo: a retrospective study. Dermatol Surg. 2011;37(7):999-1006. doi: 10.1111/j.1524-4725.2011.01966.x [DOI] [PubMed] [Google Scholar]
- 51.Budania A, Parsad D, Kanwar AJ, Dogra S. Comparison between autologous noncultured epidermal cell suspension and suction blister epidermal grafting in stable vitiligo: a randomized study. Br J Dermatol. 2012;167(6):1295-1301. doi: 10.1111/bjd.12007 [DOI] [PubMed] [Google Scholar]
- 52.Maleki M, Banihashemi M, Sanjari V. Efficacy of suction blister epidermal graft without phototherapy for locally stable and resistant vitiligo. Indian J Dermatol. 2012;57(4):282-284. doi: 10.4103/0019-5154.97669 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rao A, Gupta S, Dinda AK, et al. Study of clinical, biochemical and immunological factors determining stability of disease in patients with generalized vitiligo undergoing melanocyte transplantation. Br J Dermatol. 2012;166(6):1230-1236. doi: 10.1111/j.1365-2133.2012.10886.x [DOI] [PubMed] [Google Scholar]
- 54.Lu N, Xu A, Wu X. Follow-up study of vitiligo patients treated with autologous epidermal sheet transplants. J Dermatolog Treat. 2014;25(3):200-204. doi: 10.3109/09546634.2012.671912 [DOI] [PubMed] [Google Scholar]
- 55.Ashique KT, Kaliyadan F. Long-term follow-up and donor site changes evaluation in suction blister epidermal grafting done for stable vitiligo: a retrospective study. Indian J Dermatol. 2015;60(4):369-372. doi: 10.4103/0019-5154.160482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bao H, Hong W, Fu L, Wei X, Qian G, Xu A. Blister roof grafting, cultured melanocytes transplantation and non-cultured epidermal cell suspension transplantation in treating stable vitiligo: a mutual self-control study. J Dermatolog Treat. 2015;26(6):571-574. doi: 10.3109/09546634.2015.1034068 [DOI] [PubMed] [Google Scholar]
- 57.Ebrahimi A, Radmanesh M, Kavoussi H. Recipient site preparation for epidermal graft in stable vitiligo by a special fraise. An Bras Dermatol. 2015;90(1):55-60. doi: 10.1590/abd1806-4841.20153205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Shin D, Oh SH, Hann SK. Vitiligo involving the nipple and areola: a good indication for epidermal grafting. Dermatol Surg. 2016;42(4):565-568. doi: 10.1097/DSS.0000000000000666 [DOI] [PubMed] [Google Scholar]
- 59.Ravi SS, Chittoory SS. Suction blister grafting—still a useful modality for treatment of resistant and stable vitiligo. J Evolution Med Dental Sci. 2017;6(80):5668-5673. doi: 10.14260/jemds/2017/1229 [DOI] [Google Scholar]
- 60.Iwanowski T, Szlązak P, Rustowska A, Sokołowska-Wojdyło M. Efficacy of suction blister epidermal grafting with concomitant phototherapy in vitiligo treatment. Postepy Dermatol Alergol. 2018;35(6):592-598. doi: 10.5114/pdia.2017.71257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Kar BR, Raj C. Suction blister epidermal grafting for vitiligo involving angles of lip: experience of 112 patients. J Cutan Aesthet Surg. 2018;11(1):13-19. doi: 10.4103/JCAS.JCAS_111_15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Khan R, Sharma A, Bhushan A, Basnet B, Sharma VK, Gupta S. Relationship between α-melanocyte stimulating hormone levels and therapeutic outcome of melanocyte transplantation and phototherapy in non-segmental patients with vitiligo: a prospective study. Australas J Dermatol. 2018;59(4):e315-e318. doi: 10.1111/ajd.12769 [DOI] [PubMed] [Google Scholar]
- 63.van Geel N, Ongenae K, De Mil M, Haeghen YV, Vervaet C, Naeyaert JM. Double-blind placebo-controlled study of autologous transplanted epidermal cell suspensions for repigmenting vitiligo. Arch Dermatol. 2004;140(10):1203-1208. doi: 10.1001/archderm.140.10.1203 [DOI] [PubMed] [Google Scholar]
- 64.Pandya V, Parmar KS, Shah BJ, Bilimoria FE. A study of autologous melanocyte transfer in treatment of stable vitiligo. Indian J Dermatol Venereol Leprol. 2005;71(6):393-397. doi: 10.4103/0378-6323.18942 [DOI] [PubMed] [Google Scholar]
- 65.van Geel N, Ongenae K, Vander Haeghen Y, Vervaet C, Naeyaert JM. Subjective and objective evaluation of noncultured epidermal cellular grafting for repigmenting vitiligo. Dermatology. 2006;213(1):23-29. doi: 10.1159/000092833 [DOI] [PubMed] [Google Scholar]
- 66.Mulekar SV, Al Issa A, Al Eisa A. Treatment of vitiligo on difficult-to-treat sites using autologous noncultured cellular grafting. Dermatol Surg. 2009;35(1):66-71. [DOI] [PubMed] [Google Scholar]
- 67.Malhotra SK, Puri KJPS, Singh S. Non-cultured epidermal cell suspension-a simpler solution for a complex disease vitiligo. Pigment Cell Melanoma Res. 2010;23(3):462. [Google Scholar]
- 68.Holla AP, Kumar R, Parsad D, Kanwar AJ, Mehta SD. Role of wound bed nutrition in non cultured epidermal suspension transplantation in vitiligo. Pigment Cell Melanoma Res. 2011;24(4):835. [Google Scholar]
- 69.Paul M. Autologous non-cultured basal cell-enriched epidermal cell suspension transplantation in vitiligo: Indian experience. J Cutan Aesthet Surg. 2011;4(1):23-28. doi: 10.4103/0974-2077.79183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Sahni K, Parsad D, Kanwar AJ. Noncultured epidermal suspension transplantation for the treatment of stable vitiligo in children and adolescents. Clin Exp Dermatol. 2011;36(6):607-612. doi: 10.1111/j.1365-2230.2011.04065.x [DOI] [PubMed] [Google Scholar]
- 71.Sahni K, Parsad D, Kanwar AJ, Mehta SD. Autologous noncultured melanocyte transplantation for stable vitiligo: can suspending autologous melanocytes in the patients’ own serum improve repigmentation and patient satisfaction? Dermatol Surg. 2011;37(2):176-182. doi: 10.1111/j.1524-4725.2010.01847.x [DOI] [PubMed] [Google Scholar]
- 72.Gimenez-Azcarate A, Bernad I, Irarrazaval I, Lera M, Redondo P. Double-blind, randomized, intraindividually controlled clinical trial to evaluate the efficacy of autologous melanocyte cell transplant using amniotic membrane as a scaffold in the treatment of stable vitiligo. J Am Acad Dermatol. 2013;68(4):AB189. [Google Scholar]
- 73.Holla AP. Short-duration cold trypsinization as a novel method in noncultured epidermal suspension transplantation in stable vitiligo. Br J Dermatol. 2013;169:67-68.24098902 [Google Scholar]
- 74.Holla AP, Sahni K, Kumar R, Parsad D, Kanwar A, Mehta SD. Acral vitiligo and lesions over joints treated with non-cultured epidermal cell suspension transplantation. Clin Exp Dermatol. 2013;38(4):332-337. doi: 10.1111/ced.12040 [DOI] [PubMed] [Google Scholar]
- 75.Singh C, Parsad D, Kanwar AJ, Dogra S, Kumar R. Comparison between autologous noncultured extracted hair follicle outer root sheath cell suspension and autologous noncultured epidermal cell suspension in the treatment of stable vitiligo: a randomized study. Br J Dermatol. 2013;169(2):287-293. doi: 10.1111/bjd.12325 [DOI] [PubMed] [Google Scholar]
- 76.Bassiouny D, El-Zawahry BM, Esmat S, et al. Effect of procedural-related variables on melanocytekeratinocye suspension transplantation in stable vitiligo: a clinical and immunohistochemical study. Pigment Cell Melanoma Res. 2014;27(5):903. [Google Scholar]
- 77.Budania A, Khunger N. Non cultured epidermal cell suspension for stable vitiligo from lab to dermatologists clinic: an oversimplification or a real possibility. Pigment Cell Melanoma Res. 2014;27(5):985-986. [Google Scholar]
- 78.Holla AP. Combined cell suspension transplantation in stable vitiligo. Br J Dermatol. 2014;171:69.24484293 [Google Scholar]
- 79.Razmi MT, Parsad D, Kumaran SM. Transplantation of autologous noncultured extracted hair follicle outer root sheath cell and autologus noncultured epidermal cell suspension in combination as a novel method in vitiligo surgery. Pigment Cell Melanoma Res. 2014;27(5):903-904. [Google Scholar]
- 80.Holla AP. Recombinant protease for cell separation as a safer alternate to trypsin in noncultured epidermal suspension transplantation in stable vitiligo. Br J Dermatol. 2015;173:105-106. [Google Scholar]
- 81.Verma G, Varkhande SR, Kar HK, Rani R. Evaluation of repigmentation with cultured melanocyte transplantation (CMT) compared with non-cultured epidermal cell transplantation in vitiligo at 12th week reveals better repigmentation with CMT. J Invest Dermatol. 2015;135(10):2533-2535. doi: 10.1038/jid.2015.178 [DOI] [PubMed] [Google Scholar]
- 82.Bassiouny D, ElZawahry B, Esmat S, et al. Autologous melanocyte-keratinocyte suspension in NSV: is supplementation of the suspension medium beneficial. Pigment Cell Melanoma Res. 2017;30(5):e3-. [Google Scholar]
- 83.El-Zawahry BM, Esmat S, Bassiouny D, et al. Effect of procedural-related variables on melanocyte-keratinocyte suspension transplantation in nonsegmental stable vitiligo: a clinical and immunocytochemical study. Dermatol Surg. 2017;43(2):226-235. doi: 10.1097/DSS.0000000000000962 [DOI] [PubMed] [Google Scholar]
- 84.Kachhawa D, Rao P, Kalla G. Simplified non-cultured non-trypsinised epidermal cell graft technique followed by psoralen and ultraviolet a light therapy for stable vitiligo. J Cutan Aesthet Surg. 2017;10(2):81-85. doi: 10.4103/JCAS.JCAS_119_16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Liu Z, Li W, Zeng A, et al. Is suction blister epidermal grafting a simple and reliable way to screen patients with large area vitiligo for ReCell treatment? J Invest Dermatol. 2017;137(10):S197. doi: 10.1016/j.jid.2017.07.124 [DOI] [Google Scholar]
- 86.Mutalik S, Shah S, Sidwadkar V, Khoja M. Efficacy of cyclosporine after autologous noncultured melanocyte transplantation in localized stable vitiligo—a pilot, open label, comparative study. Dermatol Surg. 2017;43(11):1339-1347. doi: 10.1097/DSS.0000000000001190 [DOI] [PubMed] [Google Scholar]
- 87.Razmi T M, Kumar R, Rani S, Kumaran SM, Tanwar S, Parsad D. Combination of follicular and epidermal cell suspension as a novel surgical approach in difficult-to-treat vitiligo: a randomized clinical trial. JAMA Dermatol. 2018;154(3):301-308. doi: 10.1001/jamadermatol.2017.5795 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Altalhab S, AlJasser MI, Mulekar SV, et al. Six-year follow-up of vitiligo patients successfully treated with autologous non-cultured melanocyte-keratinocyte transplantation. J Eur Acad Dermatol Venereol. 2019;33(6):1172-1176. doi: 10.1111/jdv.15411 [DOI] [PubMed] [Google Scholar]
- 89.Awasti S, Vinay K, Thakur V, et al. Comparison of efficacy of cold trypsinization versus warm trypsinization in preparation of autologous non-cultured epidermal cell suspension for treatment of stable vitiligo. J Eur Acad Dermatol Venereol. 2019;33(6):e237-e239. doi: 10.1111/jdv.15502 [DOI] [PubMed] [Google Scholar]
- 90.Chuah SY, Thng STG. The role of in vivo reflectance confocal microscopy in assessing the stability of vitiligo vulgaris prior to cellular grafting. Skin Res Technol. 2019;25(2):245-247. doi: 10.1111/srt.12638 [DOI] [PubMed] [Google Scholar]
- 91.Garg S, Dosapaty N, Arora AK. Laser ablation of the recipient area with platelet-rich plasma-enriched epidermal suspension transplant in vitiligo surgery: a pilot study. Dermatol Surg. 2019;45(1):83-89. doi: 10.1097/DSS.0000000000001641 [DOI] [PubMed] [Google Scholar]
- 92.Gupta S, Relhan V, Garg VK, Sahoo B. Autologous noncultured melanocyte-keratinocyte transplantation in stable vitiligo: a randomized comparative study of recipient site preparation by two techniques. Indian J Dermatol Venereol Leprol. 2019;85(1):32-38. [DOI] [PubMed] [Google Scholar]
- 93.Hamza AM, Hussein TM, Shakshouk HAR. Noncultured extracted hair follicle outer root sheath cell suspension versus noncultured epidermal cell suspension in the treatment of stable vitiligo. J Cutan Aesthet Surg. 2019;12(2):105-111. doi: 10.4103/JCAS.JCAS_136_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Liu B, Chen HH, Liu ZH, et al. The clinical efficacy of treatment using the autologous non-cultured epidermal cell suspension technique for stable vitiligo in 41 patients. J Dermatolog Treat. 2021;32(1):90-94. doi: 10.1080/09546634.2019.1619657 [DOI] [PubMed] [Google Scholar]
- 95.Mrigpuri S, Razmi T M, Sendhil Kumaran M, Vinay K, Srivastava N, Parsad D. Four compartment method as an efficacious and simplified technique for autologous non-cultured epidermal cell suspension preparation in vitiligo surgery: a randomized, active-controlled study. J Eur Acad Dermatol Venereol. 2019;33(1):185-190. doi: 10.1111/jdv.15234 [DOI] [PubMed] [Google Scholar]
- 96.Parambath N, Sharma VK, Parihar AS, Sahni K, Gupta S. Use of platelet-rich plasma to suspend noncultured epidermal cell suspension improves repigmentation after autologous transplantation in stable vitiligo: a double-blind randomized controlled trial. Int J Dermatol. 2019;58(4):472-476. doi: 10.1111/ijd.14286 [DOI] [PubMed] [Google Scholar]
- 97.Tawfik YM, Abd Elazim NE, Abdel-Motaleb AA, Mohammed RAA, Tohamy AMA. The effect of NB-UVB on noncultured melanocyte and keratinocyte transplantation in treatment of generalized vitiligo using two different donor-to-recipient ratios. J Cosmet Dermatol. 2019;18(2):638-646. doi: 10.1111/jocd.12759 [DOI] [PubMed] [Google Scholar]
- 98.Thakur V, Kumar S, Kumaran MS, Kaushik H, Srivastava N, Parsad D. Efficacy of transplantation of combination of noncultured dermal and epidermal cell suspension vs epidermal cell suspension alone in vitiligo: a randomized clinical trial. JAMA Dermatol. 2019;155(2):204-210. doi: 10.1001/jamadermatol.2018.4919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Tovar-Garza A, Hinojosa JA, Hynan LS, Pandya AG. Noncultured epidermal suspension grafting using suction blisters as donor tissue for vitiligo. J Am Acad Dermatol. 2019;80(4):1152-1154. doi: 10.1016/j.jaad.2018.10.041 [DOI] [PubMed] [Google Scholar]
- 100.Vachiramon V, Triyangkulsri K, Saengwimol D, Chanprapaph K. Outcome of repeated use of donor site for noncultured epidermal cellular grafting in stable vitiligo: a retrospective study. Biomed Res Int. 2019;2019:7623607. doi: 10.1155/2019/7623607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Anbar TS, El-Ammawi TS, Mohammed SS, Abdel-Rahman AT. Noncultured epidermal suspensions obtained from partial-thickness epidermal cuts and suction blister roofs for vitiligo treatment: a prospective comparative study. J Cosmet Dermatol. Published online January 30, 2020. doi: 10.1111/jocd.13312 [DOI] [PubMed] [Google Scholar]
- 102.Esmat S, Bassiouny D, Saleh MA, et al. Studying the effect of adding growth factors to the autologous melanocyte keratinocyte suspension in segmental vitiligo. Dermatol Ther. 2020;33(3):e13368. doi: 10.1111/dth.13368 [DOI] [PubMed] [Google Scholar]
- 103.Kumar S, Vinay K, Parsad D, et al. Comparison of recipient-site preparation by electrofulguration-assisted manual dermabrasion versus conventional manual dermabrasion in non-cultured epidermal cell suspension procedure for stable vitiligo: an open-label comparison study. J Eur Acad Dermatol Venereol. 2020;34(7):e337-e339. doi: 10.1111/jdv.16313 [DOI] [PubMed] [Google Scholar]
- 104.Rasheed HM, Esmat SM, Hegazy RA, et al. Effect of different methods of trypsinization on cell viability and clinical outcome in vitiligo patients undergoing noncultured epidermal cellular suspension. Dermatol Surg. 2020;46(10):1307-1314. doi: 10.1097/DSS.0000000000002329 [DOI] [PubMed] [Google Scholar]
- 105.Mohanty S, Kumar A, Dhawan J, Sreenivas V, Gupta S. Noncultured extracted hair follicle outer root sheath cell suspension for transplantation in vitiligo. Br J Dermatol. 2011;164(6):1241-1246. doi: 10.1111/j.1365-2133.2011.10234.x [DOI] [PubMed] [Google Scholar]
- 106.Vinay K, Dogra S, Parsad D, et al. Clinical and treatment characteristics determining therapeutic outcome in patients undergoing autologous non-cultured outer root sheath hair follicle cell suspension for treatment of stable vitiligo. J Eur Acad Dermatol Venereol. 2015;29(1):31-37. doi: 10.1111/jdv.12426 [DOI] [PubMed] [Google Scholar]
- 107.Shah AN, Marfatia RK, Saikia SS. A study of noncultured extracted hair follicle outer root sheath cell suspension for transplantation in vitiligo. Int J Trichology. 2016;8(2):67-72. doi: 10.4103/0974-7753.188042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Kumar P, Bhari N, Tembhre MK, et al. Study of efficacy and safety of noncultured, extracted follicular outer root sheath cell suspension transplantation in the management of stable vitiligo. Int J Dermatol. 2018;57(2):245-249. doi: 10.1111/ijd.13759 [DOI] [PubMed] [Google Scholar]
- 109.Shi HX, Zhang RZ, Xu B, et al. Experimental study and clinical observations of autologous hair follicle cell transplants to treat stable vitiligo. Indian J Dermatol Venereol Leprol. 2020;86(2):124-133. doi: 10.4103/ijdvl.IJDVL_261_18 [DOI] [PubMed] [Google Scholar]
- 110.Thakur DS, Kumar S, Kumaran MS, Srivastava N, Parsad D. Comparison of follicular unit extraction vs. plucking of hair follicles as technique of harvesting hair follicles in non-cultured hair follicular cell suspension in vitiligo. J Eur Acad Dermatol Venereol. 2020;34(1):e34-e36. doi: 10.1111/jdv.15888 [DOI] [PubMed] [Google Scholar]
- 111.Löntz W, Olsson MJ, Moellmann G, Lerner AB. Pigment cell transplantation for treatment of vitiligo: a progress report. J Am Acad Dermatol. 1994;30(4):591-597. doi: 10.1016/S0190-9622(94)70067-2 [DOI] [PubMed] [Google Scholar]
- 112.Olsson MJ, Juhlin L. Transplantation of melanocytes in vitiligo. Br J Dermatol. 1995;132(4):587-591. doi: 10.1111/j.1365-2133.1995.tb08715.x [DOI] [PubMed] [Google Scholar]
- 113.Chen YF, Chang JS, Yang PY, Hung CM, Huang MH, Hu DN. Transplant of cultured autologous pure melanocytes after laser-abrasion for the treatment of segmental vitiligo. J Dermatol. 2000;27(7):434-439. doi: 10.1111/j.1346-8138.2000.tb02201.x [DOI] [PubMed] [Google Scholar]
- 114.Guerra L, Capurro S, Melchi F, et al. Treatment of “stable” vitiligo by Timedsurgery and transplantation of cultured epidermal autografts. Arch Dermatol. 2000;136(11):1380-1389. doi: 10.1001/archderm.136.11.1380 [DOI] [PubMed] [Google Scholar]
- 115.Chen YF, Yang PY, Hu DN, Kuo FS, Hung CS, Hung CM. Treatment of vitiligo by transplantation of cultured pure melanocyte suspension: analysis of 120 cases. J Am Acad Dermatol. 2004;51(1):68-74. doi: 10.1016/j.jaad.2003.12.013 [DOI] [PubMed] [Google Scholar]
- 116.Hong WS, Hu DN, Qian GP, McCormick SA, Xu AE. Ratio of size of recipient and donor areas in treatment of vitiligo by autologous cultured melanocyte transplantation. Br J Dermatol. 2011;165(3):520-525. doi: 10.1111/j.1365-2133.2011.10398.x [DOI] [PubMed] [Google Scholar]
- 117.Ghosh D, Kuchroo P, Viswanathan C, et al. Efficacy and safety of autologous cultured melanocytes delivered on poly (DL-lactic acid) film: a prospective, open-label, randomized, multicenter study. Dermatol Surg. 2012;38(12):1981-1990. doi: 10.1111/dsu.12000 [DOI] [PubMed] [Google Scholar]
- 118.Wei XD, Fu LF, Hong WS, Qian GP, Xu AE. Transplantation of autologous melanocytes for the treatment of vitiligo in children: a retrospective analysis of 124 cases. J Dermatol. 2012;39:221-222. [Google Scholar]
- 119.Zhou MN, Zhang ZQ, Wu JL, et al. Dermal mesenchymal stem cells (DMSCs) inhibit skin-homing CD8+ T cell activity, a determining factor of vitiligo patients’ autologous melanocytes transplantation efficiency. PLoS One. 2013;8(4):e60254. doi: 10.1371/journal.pone.0060254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Li J, Xu J, Fu W, Wu W, Chen S, Uyama T. Confocal laser scanning microscope is a valuable method to evaluate effectiveness of autologous cultured epidermal sheet for the treatment of stable vitiligo. J Dermatol. 2014;41:102.24438148 [Google Scholar]
- 121.Zhang DM, Hong WS, Fu LF, Wei XD, Xu AE. A randomized controlled study of the effects of different modalities of narrow-band ultraviolet B therapy on the outcome of cultured autologous melanocytes transplantation in treating vitiligo. Dermatol Surg. 2014;40(4):420-426. doi: 10.1111/dsu.12444 [DOI] [PubMed] [Google Scholar]
- 122.Wu XG, Hong WS, Xu A. GM-CSF: a possible prognostic serum biomarker of vitiligo patients’ considered for transplantation treatment with cultured autologous melanocytes: a pilot study. J Eur Acad Dermatol Venereol. 2016;30(8):1409-1411. doi: 10.1111/jdv.13256 [DOI] [PubMed] [Google Scholar]
- 123.Wu KJ, Tang LY, Li J, et al. Modified technique of cultured epithelial cells transplantation on facial segmental vitiligo. J Craniofac Surg. 2017;28(6):1462-1467. doi: 10.1097/SCS.0000000000003834 [DOI] [PubMed] [Google Scholar]
- 124.Zhu MC, Ma HY, Zhan Z, Liu CG, Luo W, Zhao G. Detection of auto antibodies and transplantation of cultured autologous melanocytes for the treatment of vitiligo. Exp Ther Med. 2017;13(1):23-28. doi: 10.3892/etm.2016.3949 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Lin J, Chen S, Li J, et al. The treatment of acral vitiligo with autologous cultured epidermal grafts. J Invest Dermatol. 2018;138(5):S212. doi: 10.1016/j.jid.2018.03.1264 29246800 [DOI] [Google Scholar]
- 126.Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712-716. doi: 10.1046/j.1445-2197.2003.02748.x [DOI] [PubMed] [Google Scholar]
- 127.Mulekar SV, Isedeh P. Surgical interventions for vitiligo: an evidence-based review. Br J Dermatol. 2013;169(suppl 3):57-66. doi: 10.1111/bjd.12532 [DOI] [PubMed] [Google Scholar]
- 128.Sonthalia S, Kachhawa D. Jodhpur Technique. StatPearls Publishing LLC; 2020. [PubMed] [Google Scholar]
- 129.Awad SS. Repigmentation of poliosis after epithelial grafting for vitiligo. Dermatol Surg. 2013;39(3, pt 1):406-411. doi: 10.1111/dsu.12082 [DOI] [PubMed] [Google Scholar]
- 130.Krishnan A, Kar S. Smashed skin grafting or smash grafting—a novel method of vitiligo surgery. Int J Dermatol. 2012;51(10):1242-1247. doi: 10.1111/j.1365-4632.2012.05513.x [DOI] [PubMed] [Google Scholar]
- 131.Kiistala U. Suction blister device for separation of viable epidermis from dermis. J Invest Dermatol. 1968;50(2):129-137. doi: 10.1038/jid.1968.15 [DOI] [PubMed] [Google Scholar]
- 132.Falabella R. Epidermal grafting: an original technique and its application in achromic and granulating areas. Arch Dermatol. 1971;104(6):592-600. doi: 10.1001/archderm.1971.04000240016002 [DOI] [PubMed] [Google Scholar]
- 133.Nanda S, Relhan V, Grover C, Reddy BS. Suction blister epidermal grafting for management of eyelid vitiligo: special considerations. Dermatol Surg. 2006;32(3):387-391. doi: 10.1111/j.1524-4725.2006.32078.x [DOI] [PubMed] [Google Scholar]
- 134.Bae JM, Kim J, Kim DS. Skin seeding technique using 0.8-mm motorized punch for refractory vitiligo. Pigment Cell Melanoma Res. 2017;30(5):e130-e131. [Google Scholar]
- 135.Gauthier Y, Surleve-Bazeille JE. Autologous grafting with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol. 1992;26(2, pt 1):191-194. doi: 10.1016/0190-9622(92)70024-A [DOI] [PubMed] [Google Scholar]
- 136.Mulekar SV. Stable vitiligo treated by a combination of low-dose oral pulse betamethasone and autologous, noncultured melanocyte-keratinocyte cell transplantation. Dermatol Surg. 2006;32(4):536-541. [DOI] [PubMed] [Google Scholar]
- 137.Chen YF, Yang PY, Hung CM, Hu DN. Transplantation of autologous cultured melanocytes for treatment of large segmental vitiligo. J Am Acad Dermatol. 2001;44(3):543-545. doi: 10.1067/mjd.2001.110658 [DOI] [PubMed] [Google Scholar]
- 138.Shih IM, Herlyn M. Role of growth factors and their receptors in the development and progression of melanoma. J Invest Dermatol. 1993;100(2)(suppl):196S-203S. doi: 10.1038/jid.1993.76 [DOI] [PubMed] [Google Scholar]
- 139.Hamzavi I, Jain H, McLean D, Shapiro J, Zeng H, Lui H. Parametric modeling of narrowband UV-B phototherapy for vitiligo using a novel quantitative tool: the Vitiligo Area Scoring Index. Arch Dermatol. 2004;140(6):677-683. doi: 10.1001/archderm.140.6.677 [DOI] [PubMed] [Google Scholar]
- 140.Taïeb A, Picardo M; VETF Members . The definition and assessment of vitiligo: a consensus report of the Vitiligo European Task Force. Pigment Cell Res. 2007;20(1):27-35. doi: 10.1111/j.1600-0749.2006.00355.x [DOI] [PubMed] [Google Scholar]
- 141.Ezzedine K, Lim HW, Suzuki T, et al. ; Vitiligo Global Issue Consensus Conference Panelists . Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25(3):E1-E13. doi: 10.1111/j.1755-148X.2012.00997.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Njoo MD, Das PK, Bos JD, Westerhof W. Association of the Köbner phenomenon with disease activity and therapeutic responsiveness in vitiligo vulgaris. Arch Dermatol. 1999;135(4):407-413. doi: 10.1001/archderm.135.4.407 [DOI] [PubMed] [Google Scholar]
- 143.Batchelor JM, Tan W, Tour S, Yong A, Montgomery AA, Thomas KS. Validation of the Vitiligo Noticeability Scale: a patient-reported outcome measure of vitiligo treatment success. Br J Dermatol. 2016;174(2):386-394. doi: 10.1111/bjd.14208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Eleftheriadou V, Thomas K, van Geel N, et al. ; Vitiligo Global Issues Consensus Group . Developing core outcome set for vitiligo clinical trials: international e-Delphi consensus. Pigment Cell Melanoma Res. 2015;28(3):363-369. doi: 10.1111/pcmr.12354 [DOI] [PubMed] [Google Scholar]
- 145.Bae JM, Ju HJ, Lee RW, et al. Micropunch grafting as an adjuvant for noncultured melanocyte-keratinocyte transplantation for refractory vitiligo. J Am Acad Dermatol. 2020;82(6):1548-1550. doi: 10.1016/j.jaad.2020.03.003 [DOI] [PubMed] [Google Scholar]
- 146.Eleftheriadou V, Hamzavi I, Pandya AG, et al. International Initiative for Outcomes (INFO) for vitiligo: workshops with patients with vitiligo on repigmentation. Br J Dermatol. 2019;180(3):574-579. doi: 10.1111/bjd.17013 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Clinical Characteristics of Studies Included in This Meta-analysis
eTable 2. Methodological Index for Nonrandomized Studies (MINORS) Criteria Scoring for Included Studies
eFigure 1. Contoured Funnel Plot of >90% Repigmentation Rate
eFigure 2. Treatment Response (>90% Repigmentation) of Surgical Interventions in Patients With Vitiligo
eReferences.