

Abstract
Background
Wound healing is a complex and dynamic process. Healing of acute and chronic wounds can be impaired by patient factors (that is, comorbidities) and/or wound factors (that is, infection). Regenerative medicine products, such as autologous/homologous platelet-rich plasma gel, may speed up the healing process. Autologous/homologous platelet-rich plasma is an advanced wound therapy used for hard-to-heal acute and chronic wounds. The cytokines and growth factors contained in platelet-rich plasma play a crucial role in the healing process.
Case presentation
A 61-year-old Caucasian male patient, suffering from mental retardation following meningitis, with a transplanted kidney due to prior renal impairment, and under immunosuppressant therapy, was submitted to aneurysmectomy of his proximal left forearm arteriovenous fistula. A few days later, the patient came to our attention with substantial blood loss from the surgical site. The wound presented no signs of healing, and after fistula reparation and considering persistent infection of the surgical site (by methicillin-resistant Staphylococcus aureus), surgeons decided for second-intention healing. To favor healing, 10 mL homologous platelet concentrate gel was sequentially applied. After each application, wound was covered with nonadherent antiseptic dressing. After only seven applications of homologous platelet concentrate gel, wound completely recovered and no amputation was necessary.
Conclusions
Topical application of homologous platelet-rich plasma gel in healing wound shows beneficial results in wound size reduction and induces granulation tissue formation. Platelet-rich plasma could be a safe and cost-effective treatment for managing the cutaneous wound healing process to shorten the recovery period and thereby improve patient quality of life.
Keywords: Regenerative medicine, Skin flap, Surgery, Wound healing
Background
Wound healing is a complex and dynamic process. Healing of acute and chronic wounds can become impaired by patient factors (that is, comorbidities) and/or wound factors (that is, infection). Regenerative medicine products, such as autologous/homologous platelet-rich plasma (PRP) gel, may speed up the healing process [1]. Autologous/homologous PRP is an advanced wound therapy used in hard-to-heal acute and chronic wounds. The cytokines and growth factors contained in PRP play a crucial role in the healing process.
Skin flap may help closure but can be affected by nonhealing skin ulcers. These ulcers are often slow healing and unresponsive to traditional treatments; consequently, the patient’s quality of life and prognosis may be severely affected [2]. To heal wounds resulting from skin transposition, local application of heterologous platelet-rich gel (PRG) has already been attempted [3], and its efficacy demonstrated in both in vitro and in vivo models [4]. The great potential of platelet-based gel has already been discussed by several authors [5–8]. Platelet-derived growth factors are involved in tissue regeneration and formation of new vessels that could improve skin flap survival [9]. The reported case is in line with the Surgical Case Report (SCARE) criteria [10].
Case presentation
A 61-year-old Caucasian male patient came to our department complaining of two large venous aneurysms on his left cephalic and basilic veins. The patient suffered from end-stage renal disease and underwent right kidney transplantation and brachiocephalic arteriovenous fistula (AVF) creation, 10 and 13 years before admission, respectively. The patient was poorly collaborative due to his cognitive retardation, likely linkable to an improperly treated meningitis during childhood. He was also affected by hypertension and colonic diverticulosis. Five years before admission, deep vein thrombosis of the upper and lower limbs was reported. Interestingly, the patient followed an immunosuppressive therapy with everolimus, prednisone, and mycophenolate mofetil. He also took atenolol, ramipril, and amlodipin to control blood pressure, and clopidogrel with subcutaneous enoxaparin in relation to his medical history of hypercoagulation. Physical examination showed a 6 × 4 cm2 swelling of the proximal left forearm, with no alterations of the covering skin. Thrill was present at palpation. Auscultation revealed VI/VI Levine systolic–diastolic bruit. Before intervention, informed consent was obtained from the patient’s legal representative and, only subsequently, was he premedicated with intravenous cephazoline 1 g, administered one hour before skin incision. Surgery was performed under local anesthesia by means of mepivacaine 2%. A 10-cm incision was necessary to expose the fistula and the two outflow vein dilations. Cephalic vein aneurysm measured 5 cm in length and 3 cm in transverse diameter, whereas the basilic vein aneurysmatic dilation was 3 cm long and 2 cm wide (Fig. 1; Additional file 1: Video 1). After AVF closure and cephalic vein aneurysmectomy, the breach of the artery wall was closed with a 5-0 polypropylene suture. Basilic vein aneurysm was then excised, and the two vascular stumps were approached with a 5-0 polypropylene suture (Fig. 2; Additional file 2: Video 2). The patient was discharged after two days without complications. Twenty days later, the patient came back to our attention with substantial blood loss from the surgical site (Fig. 3). The left forearm was edematous, and the perilesional skin showed signs of inflammation. The wound was not healed, and substance loss measured about 10 cm in transverse diameter. Blood loss was stopped by means of a tourniquet; intravenous administration of ceftriaxone 2 g was carried out, and the patient was immediately conducted to the operating room. Intraoperative examination revealed purulent fluid collection at the surgical site and a huge perivascular clot. Artery appeared inflamed and avascular. Debridement of the site caused substantial blood loss from proximal radial artery, close to the brachial artery bifurcation. After a failed attempt at vascular wall suture, considering the persistent infection of the surgical site (and the subsequent impossibility to use a vascular graft) and testing the patency of the ulnar artery, the radial artery was tied and completely closed. The area was cleared and, due to retracted skin margins, second-intention healing was chosen to restore normal local conditions (Fig. 4). The surgical site was treated with povidone iodine and covered with sterile gauzes. Daily medications were carried out for the next 2 weeks. After surgery, the patient showed low hemoglobin blood levels, requiring blood transfusion. To favor healing, 14 days later, 10 mL homologous (due to constantly low blood hemoglobin levels) platelet concentrate gel was applied. After application, wound was covered with a nonadherent dressing. Before the procedure, wound swab was performed. Methicillin-resistant Staphylococcus aureus (MRSA) colonies were detected, but no specific antibiotic therapy was established.
Fig. 1.
Left forearm. Intraoperative picture showing two aneurysms. The distal one is a cephalic vein aneurysm measuring 5 cm in length and 3 cm in transverse diameter; the proximal aneurysm represents the basilic vein aneurysmatic dilation (3 × 2 cm2)
Fig. 2.

Left forearm. Intraoperative picture of the postoperative result. After AVF closure and cephalic vein aneurysmectomy, the breach of the artery wall was closed with a 5-0 polypropylene suture. Basilic vein aneurysm was then excised, and the two vascular stumps were approached with a 5-0 polypropylene suture
Fig. 3.

Left upper limb, 20 days after aneurysmectomy. The left forearm was edematous, and the perilesional skin showed signs of inflammation. The wound was not healed, and substance loss measured about 10 cm in transverse diameter. Blood loss was stopped by means of a tourniquet
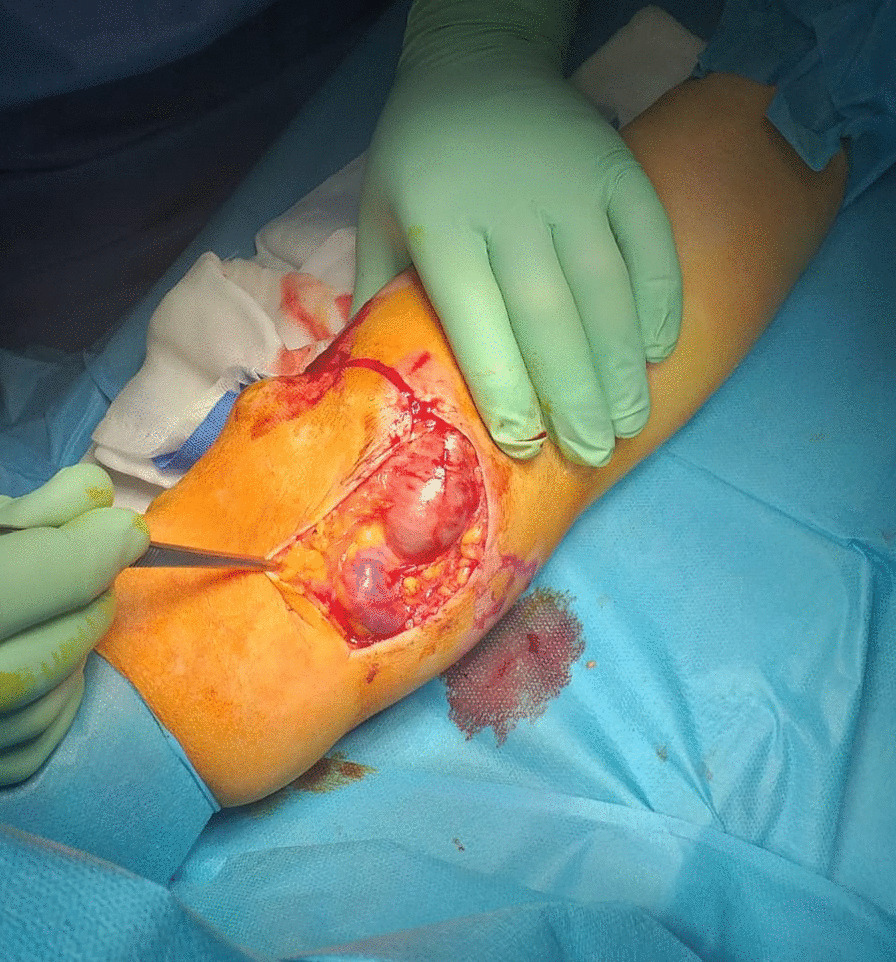
Fig. 4.

Left forearm. Surgical site soon after curettage and radial artery ligation. Loss of substance measures 6 × 4 cm2
To prepare platelet concentrate gel, a unit of apheresis platelets from a type 0 periodic donor was used. The unit was aliquoted into 10 minibags of 20 mL each, and stored at a controlled temperature of –40 °C. Whenever a medication was performed, one minibag was thawed, divided into 10 dry tubes, and centrifuged at high speed (3500 rpm) for 5 minutes to obtain a platelet pellet stratified at the bottom of each tube. Once the supernatant plasma (rich in anticoagulant) was removed, the pellet was suspended in 10 cc of type AB virus-inactivated plasma (universal plasma donor). To allow gelling of the platelet concentrate, the Plateltex Act® kit was used. The full preparation of PRP gel took around 30 min.
Medications were performed once a week (as successfully attempted in other work [1]), for 7 weeks. Before applying the PRG, the wound was prepared by surgical debridement as required to remove any dead tissue and hyperkeratotic skin, then cleaned each time with saline solution. After application, the wound was covered with nonadherent antiseptic dressing. A few layers of sterile gauze and noncompressible bandages were positioned on the region of interest. Clinical evaluation of the outcome of treatment included assessment of the size of the ulcer and degree of wound healing. Percentage of reduction was calculated using the following equation: (wound dimensions before treatment − wound dimensions after treatment)/wound dimensions before treatment × 100.
After only seven applications of homologous platelet concentrate gel, wound completely recovered and no invasive surgical procedures were necessary. One week after the first application, the first granulation spots appeared (Fig. 5). At the second week, the wound measured 5 cm in transverse diameter and was 3 cm wide (Fig. 6). One week later, wound debridement showed that the granulation tissue covered the whole loss of substance (Fig. 7) and wound edges appeared narrower (4.5 × 1.5 cm2). Five weeks after the first PRG application, the wound measured 3.5 × 0.7 cm2 (Fig. 8). After 2 months, the wound was completely recovered (Fig. 9). There were no complications recorded in the study (Additional Files 1 and 2).
Fig. 5.

Left forearm. Skin wound 1 week after first treatment with PRG. First granulation spots appeared
Fig. 6.
Left forearm. Skin wound at second control, before second PRG application. Loss of substance measures 5 × 3 cm2
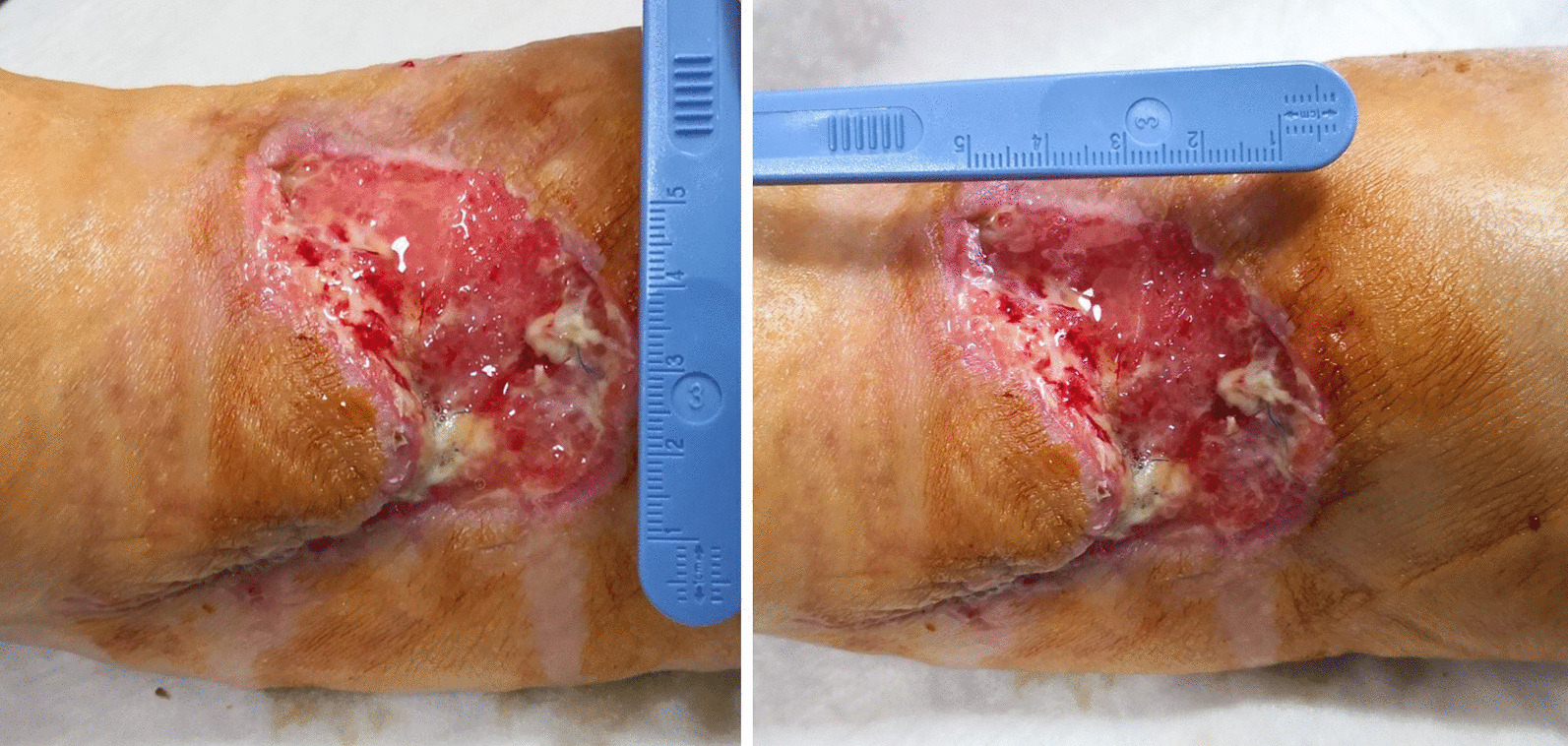
Fig. 7.

Left forearm skin wound. At third control (before third PRP application), the loss of substance measured 4.5 cm in transverse diameter and was 1.5 wide
Fig. 8.

Left forearm. Skin wound 9 weeks after surgery. The loss of substance was 3.5 × 0.7 cm2. No signs of bacterial infection are present
Fig. 9.

Left forearm 2 months after first application of PRG and 10 weeks after surgery. Complete recovery of the site is showed
Discussion and conclusions
Satisfactory results have also been achieved on uremic and diabetic patients suffering from diabetic ulcers, with ulcer healing and a reduction of disease-associated morbidity and decreased healthcare costs [11]. Our experience confirmed the utility of PRG for wound healing, particularly in a patient suffering from systemic sclerosis [1].
Several studies on the clinical use of PRP have already been conducted. Most of the literature ranges from dental medicine [12] to maxillofacial surgery [13], from dermatology and esthetic medicine [14, 15], to orthopedics and sports medicine [16], and even neurology [17]. PRP is also a promising therapeutic tool for the treatment of chronic mucositis [18] and for diabetic foot and leg ulcers [19]. In addition, PRP not only enhances the rate of wound healing but also reduces the neurological and neuropathic pain associated with injuries [20, 21]. Use of autologous platelet concentrates accelerates healing in dental implant surgery, orthopedic surgery, muscle and tendon repair, skin ulcers, hole repair in eye surgery, and cardiac surgery [22]. All these therapeutic properties are possible because platelet blood products are rich in growth factors and cytokines that stimulate and accelerate the wound healing process. In their literature review, Zamani and colleagues well described all the biological properties of PRG and its clinical application [6]. Platelets have great potential to act in the three different processes involved in wound healing: inflammation, cell proliferation, and extracellular matrix remodeling. The content of their granules (neurotransmitters, enzymes, cytokines, growth factors, and chemokines) stimulates wound reparation, increasing reepithelialization, contraction, and neovascularization. Platelets alone contain whatever is necessary for wound repair, and PRG guarantees the right amount of chemical signals to favor tissue regeneration. Furthermore, the presence of several enzymes (including lysozyme) exerts effective antimicrobial action [23].
Importantly, the preparation of PRG is cost-effective and relatively time-saving [24]. Furthermore, PRG is relatively safe, with few side effects or complications, mainly related to hypersensitivity [25, 26].
A randomized clinical trial conducted by Elsaid et al. assessed the role of PRP gel on clean nonhealing diabetic foot ulcer. Those authors reported that 25% of treated patients achieved complete healing versus none of the control group (regular dressing with saline). In total, only 8.3% of the patients treated with PRG did not show any response to treatment [27]. Another recent randomized controlled trial by Raynis et al. compared the effectiveness of autologous PRP gel in the treatment of hard-to-heal leg ulcers with existing conventional treatment, revealing that 25.71% of the autologous PRP group and 17.64% of control group had ulcers completely reepithelialized (p > 0.05). Wound size reduction was 52.35% in the autologous PRP group and 33.36% in the control group (p = 0.003). The autologous PRP group showed superiority over conventional treatment in wound bed coverage with granulation (p = 0.001) [28]. In the presented case, complete wound healing was achieved after only 6 weeks.
The percentage of reduction in the horizontal and longitudinal dimensions of the wound was 100%. This may reflect the growth-promoting effect of PRP gel.
Interestingly, despite the recorded presence of MRSA, use of PRG allowed to control surgical-site bacterial colonization without antibiotic therapy, as already reported by several authors [29, 30].
Complicated skin wounds represent an increasingly hard challenge. To date, diabetes and long-standing diseases have implied an aggressive surgical approach in most cases, with large curettages or even amputations. Regenerative medicine has offered several alternatives to invasive approaches, but is generally experimental and often very expensive. So far, PRP gel has been employed as a possible remedy to loss of substance in several branches of medicine. Unfortunately, experiences are limited and there is not extensive clinical use. With this work, the effectiveness of platelet concentrate gel in repairing challenging skin loss of substance is underlined once more. Importantly, this is one of the few cases of a large skin wound (about 10 cm in maximum diameter) treated with weekly application of PRP gel, without skin graft covering. Restitutio ad integrum was complete and autonomous (second intention) in less than 2 months, without abnormal scarring outcomes. Noninvasive procedures should always be chosen, especially in cases like the presented one in which the patient is not totally compliant. Importantly, the procedure was cost-effective and easy to perform. Furthermore, the antimicrobial properties of PRP against various microorganisms enable the potential use of PRP gel as an alternative to conventional antibiotics.
Supplementary Information
Additional file 1. Left forearm. Intraoperative video showing an aneurysm of the cephalic vein (upper) and an aneurysm of the the basilic vein (lower).
Additional file 2. Left forearm. Intraoperative video of the postoperative result. After AVF closure and cephalic vein aneurysmectomy, the breach of the artery wall was closed with a 5-0 polypropylene suture. Basilic vein aneurysm was then excised and the two vascular stumps were approached with a 5-0 polypropylene suture.
Acknowledgements
Not applicable.
Abbreviations
- PRP
Platelet-rich plasma
- PRG
Platelet-rich gel
- SCARE
Surgical case report
- AVF
Arteriovenous fistula
- MRSA
Methicillin-resistant Staphylococcus aureus
Authors' contributions
V.D.P. and G.D. designed and wrote the manuscript. V.D.P., S.R., S.F., A.G., and G.M. were involved in diagnosis and treatment. G.M. and A.I.L.M. participated in literature review and data analysis, and gave the final approval. All authors read and approved the final manuscript.
Funding
There is no funding.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Ethics approval and consent to participate
This study was conducted in accordance with the fundamental principles of the Declaration of Helsinki.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1186/s13256-020-02649-6.
References
- 1.Buscemi S, De Luca S, Fazzotta S, Lo Monte AI. Platelet-rich gel for the adjuvant treatment of wound healing of transposed flap for arteriovenous fistula in systemic scleroderma. J Vasc Access. 2017;18:e33–e34. doi: 10.5301/jva.5000640. [DOI] [PubMed] [Google Scholar]
- 2.Giuggioli D, Colaci M, Manfredi A, Mariano M, Ferri C. Platelet gel in the treatment of severe scleroderma skin ulcers. Rheumatol Int. 2012;32:2929–2932. doi: 10.1007/s00296-011-2038-0. [DOI] [PubMed] [Google Scholar]
- 3.Abegão KG, Bracale BN, Delfim IG, et al. Effects of heterologous platelet-rich plasma gel on standardized dermal wound healing in rabbits. Acta Cir Bras. 2015;30:209–215. doi: 10.1590/S0102-865020150030000008. [DOI] [PubMed] [Google Scholar]
- 4.Lacci KM, Dardik A. Platelet-rich plasma: support for its use in wound healing. Yale J Biol Med. 2010;83:1–9. [PMC free article] [PubMed] [Google Scholar]
- 5.Piccin A, Di Pierro AM, Canzian L, Primerano M, Corvetta D, Negri G, Mazzoleni G, Gastl G, Steurer M, Gentilini I, Eisendle K, Fontanella F. Platelet gel: a new therapeutic tool with great potential. Blood Transfus. 2017;15:333–340. doi: 10.2450/2016.0038-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zamani M, Yaghoubi Y, Movassaghpour A, Shakouri K, Mehdizadeh A, Pishgahi A, Yousefi M. Novel therapeutic approaches in utilizing platelet lysate in regenerative medicine: are we ready for clinical use? J Cell Physiol. 2019;234:17172–17186. doi: 10.1002/jcp.28496. [DOI] [PubMed] [Google Scholar]
- 7.De Pascale MR, Sommese L, Casamassimi A, Napoli C. Platelet derivatives in regenerative medicine: an update. Transfus Med Rev. 2015;29:52–61. doi: 10.1016/j.tmrv.2014.11.001. [DOI] [PubMed] [Google Scholar]
- 8.Everts PA, Knape JT, Weibrich G, Schönberger JP, Hoffmann J, Overdevest EP, Box HA, van Zundert A. Platelet-rich plasma and platelet gel: a review. J Extra Corpor Technol. 2006;38:174–187. [PMC free article] [PubMed] [Google Scholar]
- 9.Hersant B, La Padula S, SidAhmed-Mezi M, Rodriguez AM, Meningaud JP. Use of platelet-rich plasma (PRP) in microsurgery. J Stomatol Oral Maxillofac Surg. 2017;118:236–237. doi: 10.1016/j.jormas.2017.05.009. [DOI] [PubMed] [Google Scholar]
- 10.Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, Orgill DP, For the SCARE Group The SCARE 2018 Statement: Updating Consensus Surgical CAse REport (SCARE) Guidelines. International Journal of Surgery. 2018;60:132–136. doi: 10.1016/j.ijsu.2018.10.028. [DOI] [PubMed] [Google Scholar]
- 11.Li L, Chen D, Wang C, et al. Autologous platelet-rich gel for treatment of diabetic chronic refractory cutaneous ulcers: a prospective, randomized clinical trial. Wound Repair Regen. 2015;23:495–505. doi: 10.1111/wrr.12294. [DOI] [PubMed] [Google Scholar]
- 12.Anitua E. Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants. 1999;14:529–535. [PubMed] [Google Scholar]
- 13.Piccin A, Di Pierro AM, Tagnin M, et al. Healing of a soft tissue wound of the neck and jaw osteoradionecrosis using platelet gel. Regen Med. 2016;11:459–463. doi: 10.2217/rme-2016-0031. [DOI] [PubMed] [Google Scholar]
- 14.Arshdeep, Kumaran MS. Platelet-rich plasma in dermatology: boon or a bane? Indian J Dermatol Venereol Lepro 2014;80:5–14. [DOI] [PubMed]
- 15.Piccin A, Di Pierro AM, Corvetta D, Canzian L, Gentilini I, Primerano M, Tupini C, Mercuri E, Negri G, Mazzoleni G, Fontanella F. Severe skin radiodermatitis fully healed with the use of platelet gel and a hyperbaric chamber. Blood Transfus. 2016;14:552–554. doi: 10.2450/2015.0191-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McCarrel TM, Mall NA, Lee AS, et al. Considerations for the use of platelet-rich plasma in orthopedics. Sports Med. 2014;44:1025–1036. doi: 10.1007/s40279-014-0195-5. [DOI] [PubMed] [Google Scholar]
- 17.Ye F, Li H, Qiao G, et al. Platelet-rich plasma gel in combination with Schwann cells for repair of sciatic nerve injury. Neural Regen Res. 2012;7:2286–2292. doi: 10.3969/j.issn.1673-5374.2012.29.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Caramella CM, Sandri G, Rossi S, et al. New therapeutic platforms for the treatment of epithelial and cutaneous lesions. Curr Drug Deliv. 2013;10:18–31. doi: 10.2174/1567201811310010005. [DOI] [PubMed] [Google Scholar]
- 19.Mehrannia M, Vaezi M, Yousefshahi F, et al. Platelet rich plasma for treatment of nonhealing diabetic foot ulcers: a case report. Can J Diabetes. 2014;38:5–8. doi: 10.1016/j.jcjd.2013.08.271. [DOI] [PubMed] [Google Scholar]
- 20.Kuffler DP. Platelet-rich plasma and the elimination of neuropathic pain. Mol Neurobiol. 2013;48:315–332. doi: 10.1007/s12035-013-8494-7. [DOI] [PubMed] [Google Scholar]
- 21.Kuffler DP. Platelet-rich plasma promotes axon regeneration, wound healing, and pain reduction: fact or fiction. Mol Neurobiol. 2015;52:990–1014. doi: 10.1007/s12035-015-9251-x. [DOI] [PubMed] [Google Scholar]
- 22.Nurden AT, Nurden P, Sanchez M, et al. Platelets and wound healing. Front Biosci. 2008;13:3532–3548. doi: 10.2741/2947. [DOI] [PubMed] [Google Scholar]
- 23.de Oliveira BGRB, de Oliveira FP, Teixeira LA, de Paula GR, de Oliveira BC, Pires BMFB. Epidermal growth factor vs platelet-rich plasma: activity against chronic wound microbiota. Int Wound J. 2019;16:1408–1415. doi: 10.1111/iwj.13205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ribeiro APL, Oliveira BGRB. Production cost of autologous platelet rich plasma gel. Rev Lat Am Enfermagem. 2019;27:e3221. doi: 10.1590/1518-8345.3265.3221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Latalski M, Walczyk A, Fatyga M, Rutz E, Szponder T, Bielecki T, Danielewicz A. Allergic reaction to platelet-rich plasma (PRP): case report. Medicine (Baltimore). 2019;98:e14702. doi: 10.1097/MD.0000000000014702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Senet P, Bon FX, Benbunan M, et al. Randomized trial and local biological effect of autologous platelets used as adjuvant therapy for chronic venous leg ulcers. J Vasc Surg. 2003;38:1342–1348. doi: 10.1016/S0741-5214(03)00908-X. [DOI] [PubMed] [Google Scholar]
- 27.Elsaid A, El-Said M, Emile S, Youssef M, Khafagy W, Elshobaky A. Randomized controlled trial on autologous Platelet-Rich Plasma versus saline dressing in treatment of non-healing diabetic foot ulcers. World J Surg. 2020;44:1294–1301. doi: 10.1007/s00268-019-05316-0. [DOI] [PubMed] [Google Scholar]
- 28.Rainys D, Cepas A, Dambrauskaite K, Nedzelskiene I, Rimdeika R. Effectiveness of autologous platelet-rich plasma gel in the treatment of hard-to-heal leg ulcers: a randomised control trial. J Wound Care. 2019;28:658–667. doi: 10.12968/jowc.2019.28.10.658. [DOI] [PubMed] [Google Scholar]
- 29.Farghali HA, AbdElKader NA, AbuBakr HO, Aljuaydi SH, Khattab MS, Elhelw R, Elhariri M. Antimicrobial action of autologous platelet-rich plasma on MRSA-infected skin wounds in dogs. Sci Rep. 2019;9:12722. doi: 10.1038/s41598-019-48657-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Çetinkaya RA, Yenilmez E, Petrone P, Yılmaz S, Bektöre B, Şimsek B, Kula Atik T, Özyurt M, Ünlü A. Platelet-rich plasma as an additional therapeutic option for infected wounds with multi-drug resistant bacteria: in vitro antibacterial activity study. Eur J Trauma Emerg Surg. 2019;45:555–565. doi: 10.1007/s00068-018-0957-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Left forearm. Intraoperative video showing an aneurysm of the cephalic vein (upper) and an aneurysm of the the basilic vein (lower).
Additional file 2. Left forearm. Intraoperative video of the postoperative result. After AVF closure and cephalic vein aneurysmectomy, the breach of the artery wall was closed with a 5-0 polypropylene suture. Basilic vein aneurysm was then excised and the two vascular stumps were approached with a 5-0 polypropylene suture.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.