

Abstract
Background:
SARS-CoV-2 pandemic has modified the cardiovascular care of ambulatory patients. The aim of this survey was to study changes in lifestyle habits, treatment adherence, and mental health status in patients with cardiometabolic disease, but no clinical evidence of COVID-19.
Methods:
A cross-sectional survey was conducted in ambulatory patients with cardiometabolic disease using paper/digital surveys. Variables investigated included socioeconomic status, physical activity, diet, tobacco use, alcohol intake, treatment discontinuation, and psychological symptoms.
Results:
A total of 4,216 patients (50.9% males, mean age 60.3 ± 15.3 years old) from 13 Spanish-speaking Latin American countries were enrolled. Among the study population, 46.4% of patients did not have contact with a healthcare provider, 31.5% reported access barriers to treatments and 17% discontinued some medication. Multivariate analysis showed that non-adherence to treatment was more prevalent in the secondary prevention group: peripheral vascular disease (OR 1.55, CI 1.08–2.24; p = 0.018), heart failure (OR 1.36, CI 1.05–1.75; p = 0.017), and coronary artery disease (OR 1.29 CI 1.04–1.60; p = 0.018). No physical activity was reported by 38% of patients. Only 15% of patients met minimum recommendations of physical activity (more than 150 minutes/week) and vegetable and fruit intake. Low/very low income (45.5%) was associated with a lower level of physical activity (p < 0.0001), less fruit and vegetables intake (p < 0.0001), more tobacco use (p < 0.001) and perception of depression (p < 0.001). Low educational level was also associated with the perception of depression (OR 1.46, CI 1.26–1.70; p < 0.01).
Conclusions:
Patients with cardiometabolic disease but without clinical evidence of COVID-19 showed significant medication non-adherence, especially in secondary prevention patients. Deterioration in lifestyle habits and appearance of depressive symptoms during the pandemic were frequent and related to socioeconomic status.
Keywords: Latin America, COVID-19 pandemic, cardiovascular disease, cardiometabolic disease, social determinants, SARS-CoV-2
Introduction
During the current COVID-19 pandemic, international organizations and national health authorities proposed a community strategy to prevent and mitigate the spread of SARS-CoV-2, and almost all countries in the world adopted social distancing measures with different degrees of restriction [1,2,3,4].
The fear of becoming infected with coronavirus, as well as the initial global public health statements urging people to stay home, led to a reduction in the number of visits and hospitalizations in patients with chronic non-communicable diseases [5,6,7]. Considering this, interest burgeoned in protocols for novel management of different pathologies [8,9,10]. This led health teams to presume that, in parallel to the COVID 19 contagion curve, there was another curve that was not being measured: one related to missed medical care in at risk populations [11].
In addition to these problems, Latin America presents a specific health issue, the impact of social determinants of health such as poverty, previously high unemployment rates, low educational level and fewer resources to combat the pandemic and its consequences [12]. These components increase the risk of social conflict and individual uncertainty with unpredictable psychological impact [13].
There is a question about the real state of affairs of patients with cardiometabolic disease but no clinical manifestation of Covid-19 in terms of lifestyle, adherence to treatments, and psychological symptoms during the pandemic [14].
Methods
The rationale and design of the CorCOVID LATAM Study was previously published [15].
Study population
The study population included patients with cardiometabolic disease being followed by a cardiologist in Spanish speaking Latin American countries. Eligible patients were those who did not have symptoms, signs, or suspicion of COVID-19. All gave their consent to answer a survey personally or by virtual platforms.
Informed consent
Patients were informed about the objective of the survey and the anonymity of their responses, and gave consent to answer it personally or by virtual platforms. Ethics approval was obtained from the Interamerican Society of Cardiology (IASC) Research Ethics Board.
Study design
A cross-sectional online survey consisting of 38 questions was developed using Google Forms (Mountain View, CA). Research staff administered the questionnaire to patients and then entered data online. In accordance with government measures to limit population mobilization, the survey was conducted either face-to-face, by phone, or by video chat, in which case informed consent was verbally taken.
The survey had seven clusters divided in two sections: 1. Questions that examine the patient’s demographic and cardiometabolic profile; 2. Questions that examine the patient’s behavior during the last 30 days. Questions contained dichotomous or multiple option answers. Answers were not forced, and respondents were permitted to select more than one response depending on the question content.
According to the World Health Organization (WHO), in its document ‘Global Recommendations on Physical Activity for Health’, physical activity is measured in minutes/week and times/week [16]. Low level of physical activity was considered as 2 times or less/week and less than 100 minutes/week, too.
Regarding fruits and vegetables consumption we measured in days/week and servings/day as per WHO. The international goals are 400 gr/day distributed in 4–5 servings/day (2 of fruit and 3 of vegetables). We considered very low intake less than three days/week and less than three servings/day.
Study distribution
The Interamerican Society of Cardiology opened the call for cardiologists of Spanish speaking Latin American countries to join as researchers on June 1st, 2020. Sixty-six investigators from 13 countries (divided in three geographic regions) applied and were approved:
Region 1 (North, Central, and Caribbean region): Costa Rica, Cuba, El Salvador, Guatemala, México, and República Dominicana.
Region 2 (Andean region): Colombia, Ecuador, Perú, and Venezuela.
Region 3 (Southern cone region): Argentina, Chile, and Paraguay.
The survey platform was open between June 15 and July 15, 2020 for the investigator team. Reminders were emailed daily to maximize the response rate, with information about the progression of the total surveys by country, as an incentive.
Statistical analysis
Data was described using means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. Independent sample t-tests were used to compare the normally distributed continuous variables, the Mann-Whitney U test was used for non-normally distributed continuous variables, and the Pearson’s chi-squared test (or the Fisher’s exact test as appropriate) for categorical variables. A P value of less than 0.05 was considered statistically significant. Multiple logistic regression models were constructed for comparisons, OR and 95% confidence intervals (CI) were provided to establish which variables are determining factors in the main negative changes observed in this population during the SARS-COV 2 outbreak. Data was collected in Google Forms. All statistical analysis was performed using Stata v. 13.1 (Stata Corp LP, USA).
Results
A total of 4429 surveys(s) were collected, 213 of which were discarded due to incomplete data, duplicate document, or non-meeting inclusion criteria. As such, 4216 were included in the database for statistical analysis distributed by regions as shown in Figure 1. The mean age of the population was 60.35 ±15.39 years old, and 2147 patients were men (50.9%).
Figure 1.

Distribution of surveyed by region.
Baseline socio-demographic characteristics are listed in Table 1.
Table 1.
Descriptive analysis of socio-demographic characteristic of the population. Categorical variables are shown as percentages with counts in parentheses.
| Baseline socio demographic profile | Baseline habits profile | ||
|---|---|---|---|
| Region of origin | Habits | ||
|
33.8% (1426) | Smoking | |
|
32.2% (1359) |
|
85.6% (3610) |
|
33.9% (1431) |
|
9.0% (381) |
| Age (years) | 60.3 (SD 15.39) |
|
3.9% (165) |
| Sex |
|
1.4% (60) | |
|
50.9% (2147) | Physical activity | |
|
49% (2069) |
|
38% (1605) |
| Education |
|
34.4% (1454) | |
|
2.2% (96) |
|
14.9% (632) |
|
19.1% (807) |
|
12.4% (525) |
|
32.1% (1355) | Physical activity Min/week | |
|
15.3% (646) |
|
44.5% (1164) |
|
31.1% (1312) |
|
31.3% (818) |
| Occupation |
|
14.2% (372) | |
|
4.6% (194) |
|
9.8% (257) |
|
18.1% (766) | Alcohol intake | |
|
19.4% (819) |
|
42.6% (1797) |
|
6.7% (284) |
|
57.3% (2419) |
|
12.1% (512) | Frequency of consumption (n = 1797) | |
|
12.5% (528) |
|
68.2% (1227) |
|
26.4% (1113) |
|
17.2% (310) |
| Income level |
|
7.7% (139) | |
|
10% (422) |
|
6% (109) |
|
35.5% (1498) |
|
0.6% (12) |
|
48.5% (2047) | Frequency of intake of fruits and vegetables | |
|
5.9% (249) |
|
7.7% (326) |
|
34.8% (1469) | ||
|
22.7% (958) | ||
|
34.7% (1463) | ||
| Daily intake of fruits and vegetables | |||
|
28.5% (1202) | ||
|
56.7% (2393) | ||
|
10.7% (451) | ||
|
2.6% (111) | ||
|
1.4% (59) | ||
Socio-economic and cardiometabolic profile
Among this population, 1920 (45.54%) belonged to the low and very low incomes group and 903 (22.4%) had primary education level or non-education.
Table 2 shows the cardiometabolic profile of the study population.
Table 2.
Descriptive analysis of cardiometabolic profile of the population. Categorical variables are shown as percentages with counts in parentheses.
| Baseline Cardiometabolic profile | |
|---|---|
| CV History | |
| Hypertension | 72.8 % (3071) |
| Dyslipidemia | 36.8 % (1555) |
| Diabetes | 21.3 % (899) |
| Coronary disease | 18.2 % (769) |
| Arrhythmias | 16.9 % (714) |
| Heart failure | 10.3 % (436) |
| Valvulopathy | 8.2 % (346) |
| Peripheral vascular disease | 4.2 % (181) |
| Cardiomyopathy | 4 % (172) |
| Stroke | 3.9 % (168) |
| Cardiac devices | 3.8 % (164) |
| Other | 2.3 % (99) |
| Last hospitalization due to a cardiovascular event | |
| Never | 51.3% (2165) |
| 2020 | 11.1% (470) |
| 2019 | 11.1% (469) |
| 2018 | 7.0% (298) |
| 2017 or earlier | 19.3% (814) |
| Number of pills taken per day | |
| Less than 4 | 67.0% (2825) |
| 5 to 8 | 27.5% (1160) |
| 9 to 12 | 4.8% (203) |
| More than 12 | 0.6% (28) |
Among risk factors, hypertension (3071/72.8%), dyslipidemia (1555/36.8%) and diabetes (899/21.3%) were the most frequent.
Coronary artery disease (CAD) (769/18.2%) and heart failure (436/10.3%) were the most prevalent secondary prevention population.
Of the population, 1391 (32.9%) took 5 or more pills daily at the time of the survey and 2258 (53.56%) had at least one contact with the health team in the last month.
Lifestyles habits
Among the total population, 2611 (62%) performed physical activity, but only 629 (14.9%) met the minimum recommendations of 150 minutes per week. Only 562 (14.7%) had the recommended daily intake of four or more servings. Finally, 1797 (42.6%) were reported as habitual drinkers and 606 (14.4%) as current smokers.
Changes during the pandemic
The major changes in self-reported lifestyle habits are shown in Table 3, classified into 4 main items: physical activity, smoking, alcohol intake, and dietary intake of fruits and vegetables.
Table 3.
Changes in lifestyle habits in the last 30 days. Behavior is expressed as percentage of affirmative answers and in brackets the number of patients involved.
| Physical activity | n (%) |
|---|---|
| Changes in physical activity (n = 2611) | |
| It has been less than in the previous months | 61.3% (1601) |
| It has been the same as in the previous months | 28.4% (742) |
| It has been more than in the previous months | 10.2% (268) |
| Have you used any app for training? | |
| Yes | 21.3% (558) |
| No | 78.6% (2053) |
| Smoking | |
| Changes in Smoking habit (n = 606) | |
| It has been less than in the previous months | 33% (200) |
| It has been the same as in the previous months | 25.7% (156) |
| It has been more than in the previous months | 17% (103) |
| Missing data | 24.2% (147) |
| Have you considered Smoking cessation? | |
| Yes | 52.3% (317) |
| Alcohol Intake | |
| Changes in alcohol intake (n = 1797) | |
| It has been less than in the previous months | 45.4% (816) |
| It has been the same as in the previous months | 34.7% (624) |
| It has been more than in the previous months | 11.3% (204) |
| Missing data | 8.5% (153) |
| Dietary intake of fruits and vegetables | |
| Changes in fruits and vegetables intake (n = 4216) | |
| It has been less than in the previous months | 27.9% (1177) |
| It has been the same as in the previous months | 49.8% (2103) |
| It has been more than in the previous months | 22.2% (936) |
➢ Physical activity and diet
Among the population who regularly perform physical activity, 1601 (61.3%) reported less volume than the previous months.
The surveyed population reported a low consumption of fruits and vegetables 1795 (42.5%) 3 or fewer days/week and 3595 (85.5%) 3 or fewer servings/day. In the preceding 30 days, vegetable and fruit intake diminished in 27.9% of the surveyed population, did not change in 49.8% and increased in 22.2% of the patients, (Figure 2).
Figure 2.
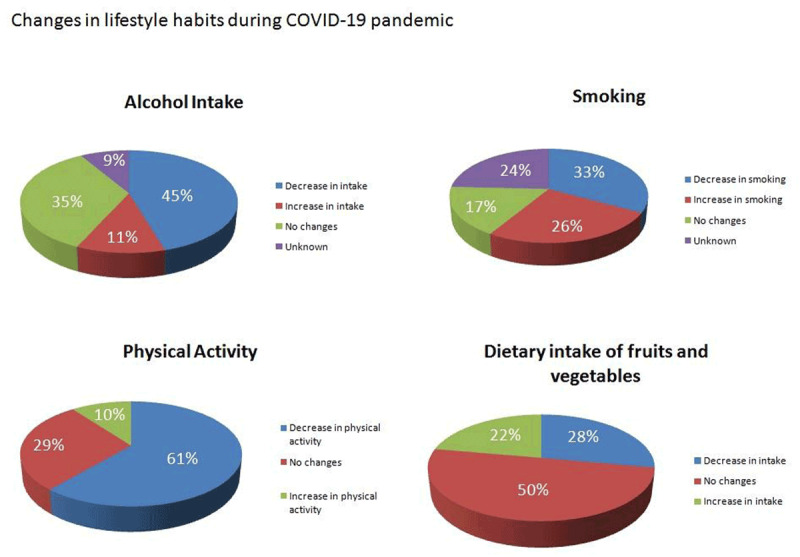
Main changes in lifestyle habits.
➢ Tobacco and Alcohol
In the current smoking population (103), 17% stated an increase in tobacco consumption but, as a positive finding, 52.3% reported they had considered quitting tobacco.
In the regular drinker population (1797), 11.3% stated they drank more, while 79% stated they drank the same or less quantity than they did before the pandemic.
Psychological symptoms
The perception of depression was reported by 1751 (41.5%) and was associated with low educational level (OR 1.46 CI 1.26–1.70; P < 0.01).
Other psychological symptoms were reported: weariness (2219/52.6%), decreased attention (1219/28.9%), sleeplessness or insomnia problems (2049/48.6%), and loss of interest in usual activities (3349/79.4%).
Univariate analysis showed an association between the perception of depression and low income (OR 0.48 CI 0.42–0.55; P < 0.001), sedentary lifestyle (OR 0.62 CI 0.54–0.70; P < 0.001), decreased food intake (OR 0.48 CI 0.43–0.57; P < 0.001) and perception of weight loss (OR 0.48 CI 0.41–0.56; P < 0.001).
Low-income was associated with a lower level of physical activity (P < 0.0001), less consumption of fruits and vegetables (P < 0.0001), more tobacco use (P < 0.001), and a higher perception of depression (P < 0.001).
Adherence to pharmacological treatments
A total of 1330 patients (31.5%) reported access barriers to pharmacological treatments, and 720 (17%) reported discontinuation of some medication (Figure 3). After applying multivariate analysis, secondary prevention status was significantly associated with this situation: peripheral disease (OR 1.55 CI 1.08–2.24; P = 0.018), heart failure (OR 1.36 CI 1.05–1.75; P = 0.017), valvular heart disease (OR 1.66 CI 1.27–2.17; P < 0.001) and CAD (OR 1.29 CI 1.04–1.60; P = 0.018).
Figure 3.
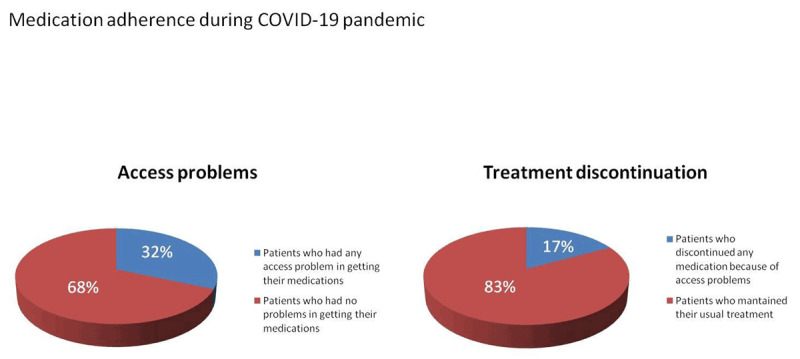
Percentage of patients who have had problems accessing some medication and patients with treatment discontinuation.
Perception of depression increased chances of discontinuing a medication (OR 2.01 CI 1.71–2.37; P < 0.001).
Details of univariate and multivariate analysis are listed in Table 4.
Table 4.
Discontinuation of medication related to numbers of pills and cardiovascular antecedents.
| Univariate Logistic | Multivariate Logistic | |||||
|---|---|---|---|---|---|---|
| OR crude | 95%CI | P value | Adjusted OR | 95%CI | P value | |
| Male sex | 0.92 | 0.78–1.08 | 0.312 | 1.01 | 0.86–1.20 | 0.819 |
| Pills per day | ||||||
| - Less than 4 | Baseline | N/A | N/A | Baseline | N/A | N/A |
| - 5–8 | 0.85 | 0.70–1.02 | 0.096 | 0.80 | 0.65–0.99 | 0.047 |
| - 9–12 | 1.19 | 0.83–1.70 | 0.335 | 1.07 | 0.73–1.59 | 0.698 |
| - More than 12 | 1.28 | 0.51–3.18 | 0.590 | 1.09 | 0.42–2.80 | 0.857 |
| Cardiovascular History | ||||||
| Stroke | 0.72 | 0.45–1.14 | 0.163 | 0.70 | 0.44–1.12 | 0.147 |
| Peripheral vascular disease | 1.54 | 1.08–2.19 | 0.015 | 1.55 | 1.08–2.24 | 0.018 |
| Coronary disease | 1.16 | 0.94–1.41 | 0.148 | 1.29 | 1.04–1.60 | 0.018 |
| Diabetes | 1.01 | 0.83–1.23 | 0.883 | 1.08 | 0.88–1.33 | 0.411 |
| Hypertension | 0.74 | 0.62–0.88 | 0.001 | 0.86 | 0.71–1.03 | 0.119 |
| Dyslipidemia | 0.81 | 0.68–0.96 | 0.016 | 0.85 | 0.71–1.02 | 0.084 |
| Heart failure | 1.44 | 1.13–1.84 | 0.003 | 1.36 | 1.05–1.75 | 0.017 |
| Cardiomyopathy | 1.49 | 1.04–2.15 | 0.029 | 1.30 | 0.89–1.91 | 0.172 |
| Valvular heart disease | 1.77 | 1.37–2.29 | <0.001 | 1.66 | 1.27–2.17 | <0.001 |
| Arrhythmias | 0.97 | 0.78–1.21 | 0.833 | 0.90 | 0.72–1.12 | 0.357 |
| Cardiac devices | 1.04 | 0.69–1.57 | 0.834 | 0.95 | 0.62–1.45 | 0.816 |
| Depression | 2.02 | 1.72–2.38 | 0.000 | 2.01 | 1.71–2.37 | <0.001 |
Discussion
The main finding of our work was to demonstrate that a significant number of patients with cardiometabolic disease showed worsening of lifestyle habits, inadequate medical follow-up, frequent discontinuation of medications, and a worrying incidence of psychological symptoms. This was particularly apparent in the secondary prevention group.
A recent editorial by Robert Brook et al. analyzed the impact of major catastrophes on cardiometabolic risk factors. The authors proposed a strategy of anticipating, not just reacting to, the possible coming of a second crisis derived from the clinical worsening of cardiometabolic patients and suggested possible tools to deal with the problem [17]. The contribution of the Cor-COVID-LATAM survey aims to further these goals.
It behooves us to consider that inadequate follow-up increases the possibility of not detecting asymptomatic or minimally symptomatic disturbances in high-risk patients. Among our surveyed cardiometabolic population, 1958 (46.4%) did not have any type of contact with a healthcare provider despite the widely spread recommendations of not neglecting the care of chronic pathology. This situation is consistent with what has already been reported in Asia and Europe [18,19].
Despite the current availability of virtual tools to guide patients in diet and physical activity, the health system was not prepared to respond adequately in a short time to reach thousands of patients [20]. Thus, only 558 (21.3%) among those who performed physical activity used web tutorials or apps. Inexperience in the use of telemedicine tools, and in many cases the non-existence of updated patient databases, increased the lack of connection between the health teams and patients with cardiometabolic disease, particularly in public health systems belonging to low and middle incomes countries [21,22,23]. The absence of adequate follow-up of patients lead to missed opportunities, such as that offered by 52.3% of active smokers, who reported that they had contemplated quitting smoking [24].
A relevant result of this study is the important number of patients discontinuing treatment. As it is well known, this increases the risk of events in a short period of time [25,26]. During the last decade, adherence to cardiovascular treatment guidelines has been a highly debated topic [27]. Some evidence has shown that patients’ self-reports usually underestimate adherence issues. The FOCUS study demonstrated that adherence falls from 68% to 50.8% when investigators add pill count to the Morisky Green Test, a short survey that evaluates adherence [28]. Based on this, it is likely that non-adherence could be greater than that reported by patients in this study.
The maintenance of cardiovascular treatment is a complex challenge with different components. Among these, access barriers emerged as a major finding as 1330 (31.5%) reported difficulties in obtaining some medication. Similarly, data from the Prospective Urban and Rural Epidemiological (PURE) Study showed that in Latin American countries, secondary prevention drugs may not be available or affordable for a large proportion of communities and households [29]. For instance, at the time of this survey, most Latin American countries did not accept digital prescription of drugs, giving rise to a new barrier to access medication given the mobility restriction measures.
Another important aspect affecting cardiometabolic patients’ treatments was the controversial information in the press and social media about some medicines (e.g.: angiotensin-converting enzyme inhibitor or angiotensin receptor blockers) as a potential gateway for the coronavirus [30,31]. Despite the immediate position statement of many cardiovascular scientific societies, including the Inter American Society of Cardiology, strongly recommending to continue cardiovascular treatments, it did not completely avoid a lack of adherence to these treatments [32].
Since the beginning of the outbreak of SARS-CoV-2, potential psychological impact was of great concern [33,34,35]. This study demonstrated a significant percentage of patients reporting psychological symptoms. Among them, the perception of depression showed an association with social determinants of health such as low-income and educational level, factors that have previously been shown to enhance cardiovascular mortality [36]. We recently published the most detailed results regarding psychological impact and 1,590 individuals (37.71%; IC95% 36.24–39.19) were considered suffering major depression independently associated with female gender (OR 1.72; 95%CI 1.40–2.11; p < 0.0001), low physical activity <100 minutes weekly (OR 1.36; 95%CI 1.10–1.67; p < 0.004), and low fruits and vegetables intake (OR 1.46; 95%CI 1.05–2.03; p < 0.024) [37]. The consequences of these neglected aspects will surely be reflected in an increase in mental disorders such as major depression and stress, which have a proven relationship with cardiovascular outcomes [38]. A recent web survey of the UK Household Longitudinal Study (UKHLS) showed that mental health deteriorated compared to pre-COVID-19 times, and the authors commented on the need to generate policies that address special populations such as women, youth, and children in order to prevent future mental illnesses [39]. Early detection and proper treatment of depression are crucial aspects to start the resilience process [40].
Limitations
Among the limitations of this study are the absence of a random sample design to achieve a better representativeness of the participating countries’ population. Even though we were able to include more than 4000 patients, this is only a partial view of the continental situation, and probably, there is high regional and local heterogeneity. However, a significant number of surveys in a short period of time has allowed us to create a snapshot that reasonably expresses the situation of cardiometabolic patients in Latin America. Another limitation is that Brazil was not included in the survey, as the survey was limited to Spanish speaking countries. Finally, the self-reported variables may lead to bias, related to the type of survey and psychological status of patients during the interview.
Conclusions
A significant proportion of the surveyed Latin American patients with cardiometabolic disease but without clinical evidence of SARS-CoV-2 infection during the ongoing COVID-19 pandemic showed a worsening of lifestyle habits, inadequate medical follow-up, frequent discontinuation of medications, particularly in the secondary prevention group, and worrying incidence of psychological symptoms. Some of them were related to low income and educational levels. These findings show the greater vulnerability of individuals living in middle-income countries during this unprecedented pandemic.
Additional Files
The additional files for this article can be found as follows:
CorCOVID Survey.
Investigators.
Competing Interests
The authors have no competing interests to declare.
References
- 1.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395: 497–506. DOI: 10.1016/S0140-6736(20)30183-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.MacIntyre CR, Wang Q. Physical distancing, face masks, and eye protection for prevention of COVID-19 [published correction appears in Lancet. 2020 Jun 5]. Lancet. 2020; 395(10242): 1950–51. DOI: 10.1016/S0140-6736(20)31183-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bauch CT, Anand M. COVID-19: When should quarantine be enforced? [published online ahead of print, 2020 May 20]. Lancet Infect Dis. 2020; S1473-3099(20)30428-X. DOI: 10.1016/S1473-3099(20)30428-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet. 2020; 395: 912–20. DOI: 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Boukhris M, Hillani A, Moroni F, et al. Cardiovascular implications of the COVID-19 Pandemic: A global perspective. Can J Cardiol. 2020; 36(7): 1068–80. DOI: 10.1016/j.cjca.2020.05.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pessoa-Amorim G, Camm CF, Gajendragadkar P, et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic: A survey by the European Society of Cardiology. Eur Heart J Qual Care Clin Outcomes. 2020; 6(3): 210–16. DOI: 10.1093/ehjqcco/qcaa046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Burki TK. Cancer care in the time of COVID-19. Lancet Oncol. 2020; 21(5): 628 DOI: 10.1016/S1470-2045(20)30201-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Korytkowski M, Antinori-Lent K, Drincic A, et al. A pragmatic approach to inpatient diabetes management during the COVID-19 pandemic. J Clin Endocrinol Metab. 2020; 105(9): dgaa342 DOI: 10.1210/clinem/dgaa342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol. 2020; 105: 104684 DOI: 10.1016/j.oraloncology.2020.104684 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bhaskar S, Bradley S, Israeli-Korn S, et al. Chronic Neurology in COVID-19 Era: Clinical Considerations and Recommendations From the REPROGRAM Consortium. Front Neurol. 2020; 11: 664 Published 2020 Jun 24. DOI: 10.3389/fneur.2020.00664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chalasani M, Nasir K, Gupta MD, Kalra A. The Covid-19 pandemic and India’s cardiovascular disease burden: Finding the right balance [published online ahead of print, 2020 May 15]. Indian J Med Ethics. 2020; V(3): 1–3. DOI: 10.20529/IJME.2020.059 [DOI] [PubMed] [Google Scholar]
- 12.Pinilla-Roncancio M. The reality of disability: Multidimensional poverty of people with disability and their families in Latin America. Disabil Health J. 2018; 11(3): 398–404. DOI: 10.1016/j.dhjo.2017.12.007 [DOI] [PubMed] [Google Scholar]
- 13.Holmes EA, O’Connor RC, Perry VH, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020; 7(6): 547–60. DOI: 10.1016/S2215-0366(20)30168-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brook RD, Levy P, Rajagopalan S. Cardiometabolic risk factor control during times of crises and beyond. Circ Cardiovasc Qual Outcomes. 2020; 13(7): e006815 DOI: 10.1161/CIRCOUTCOMES.120.006815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Santi RL, Piskorz DL, Marquez MF, et al. Impact of the pandemic on non-infected cardiometabolic patients. A survey in countries of Latin America rationale and design of CorCOVID LATAM Study [published online ahead of print, 2020 Aug 28]. CJC Open. 2020. DOI: 10.1016/j.cjco.2020.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Health Organization. Global Recommendations on Physical Activity for Health. https://www.who.int/publications/i/item/9789241599979 (Last visit 09/dec/2020). [PubMed]
- 17.Brook RD, Levy P, Rajagopalan S. Cardiometabolic risk factor control during times of crises and beyond. Circ Cardiovasc Qual Outcomes. 2020; 13(7): e006815 DOI: 10.1161/CIRCOUTCOMES.120.006815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tam CF, Cheung KS, Lam S, et al. Impact of coronavirus disease 2019 (COVID-19) outbreak on ST-segment-elevation myocardial infarction care in Hong Kong, China. Circ Cardiovasc Qual Outcomes. 2020; 13(4): e006631 DOI: 10.1161/CIRCOUTCOMES.120.006631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Huet F, Prieur C, Schurtz G, et al. One train may hide another: Acute cardiovascular diseases could be neglected because of the COVID-19 pandemic. Arch Cardiovasc Dis. 2020; 113(5): 303–07. DOI: 10.1016/j.acvd.2020.04.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.American Heart Association. Cardiovascular disease risk reduction across healthcare settings: A scientific statement from the American Heart Association [published online ahead of print, 2020 Aug 7]. Circ Cardiovasc Qual Outcomes. 2020; HCQ0000000000000094. DOI: 10.1161/HCQ.0000000000000094 [DOI] [PubMed] [Google Scholar]
- 21.Julien HM, Eberly LA, Adusumalli S. Telemedicine and the forgotten America. Circulation. 2020; 142(4): 312–14. DOI: 10.1161/CIRCULATIONAHA.120.048535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Curioso WH. Building capacity and training for digital health: Challenges and opportunities in Latin America. J Med Internet Res. 2019; 21(12): e16513 Published 2019 Dec 18. DOI: 10.2196/preprints.16513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Novillo-Ortiz D, Dumit EM, D’Agostino M, et al. Digital health in the Americas: Advances and challenges in connected health. BMJ Innov. 2018; 4(3): 123–27. DOI: 10.1136/bmjinnov-2017-000258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kowitt SD, Cornacchione Ross J, Jarman KL, et al. Tobacco quit intentions and behaviors among cigar smokers in the United States in response to COVID-19. Int J Environ Res Public Health. 2020; 17(15): 5368 Published 2020 Jul 25. DOI: 10.3390/ijerph17155368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Giral P, Neumann A, Weill A, Coste J. Cardiovascular effect of discontinuing statins for primary prevention at the age of 75 years: A nationwide population-based cohort study in France. Eur Heart J. 2019; 40(43): 3516–25. DOI: 10.1093/eurheartj/ehz458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sundström J, Hedberg J, Thuresson M, Aarskog P, Johannesen KM, Oldgren J. Low-Dose aspirin discontinuation and risk of cardiovascular events: A Swedish Nationwide, population-based cohort study. Circulation. 2017; 136(13): 1183–92. DOI: 10.1161/CIRCULATIONAHA.117.028321 [DOI] [PubMed] [Google Scholar]
- 27.Booth JN 3rd, Colantonio LD, Chen L, et al. Statin discontinuation, reinitiation, and persistence patterns among medicare beneficiaries after myocardial infarction: A cohort study. Circ Cardiovasc Qual Outcomes. 2017; 10(10): e003626 DOI: 10.1161/CIRCOUTCOMES.117.003626 [DOI] [PubMed] [Google Scholar]
- 28.Castellano JM, Sanz G, Peñalvo JL, et al. A polypill strategy to improve adherence: Results from the FOCUS project. J Am Coll Cardiol. 2014; 64(20): 2071–82. DOI: 10.1016/j.jacc.2014.08.021 [DOI] [PubMed] [Google Scholar]
- 29.Khatib R, McKee M, Shannon H, Chow C, Rangarajan S, Teo K, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries: An analysis of the PURE study data. Lancet. 2016; 387(10013): 61–9. DOI: 10.1016/S0140-6736(15)00469-9 [DOI] [PubMed] [Google Scholar]
- 30.Cannata F, Chiarito M, Reimers B, et al. Continuation versus discontinuation of ACE inhibitors or angiotensin II receptor blockers in COVID-19: Effects on blood pressure control and mortality [published online ahead of print, 2020 Jun 5]. Eur Heart J Cardiovasc Pharmacother. 2020; pvaa056. DOI: 10.1093/ehjcvp/pvaa056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Danser AHJ, Epstein M, Batlle D. Renin-Angiotensin system blockers and the COVID-19 pandemic: At present there is no evidence to abandon renin-angiotensin system blockers. Hypertension. 2020; 75(6): 1382–85. DOI: 10.1161/HYPERTENSIONAHA.120.15082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zhang X, Yu J, Pan LY, Jiang HY. ACEI/ARB use and risk of infection or severity or mortality of COVID-19: A systematic review and meta-analysis. Pharmacol Res. 2020; 158: 104927 DOI: 10.1016/j.phrs.2020.104927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020; 17(5): 1729 Published 2020 Mar 6. DOI: 10.3390/ijerph17051729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cao W, Fang Z, Hou G, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020; 287: 112934 DOI: 10.1016/j.psychres.2020.112934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lima CKT, Carvalho PMM, Lima IAAS, et al. The emotional impact of coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020; 287: 112915 DOI: 10.1016/j.psychres.2020.112915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lazzarino AI, Hamer M, Stamatakis E, Steptoe A. Low socioeconomic status and psychological distress as synergistic predictors of mortality from stroke and coronary heart disease. Psychosom Med. 2013; 75(3): 311–16. DOI: 10.1097/PSY.0b013e3182898e6d [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Piskorz D, Barragán AP, Santi RL, Vázquez G, Ortiz GS, Zambrano LR, et al. Psychological impact of the pandemic on ambulatory cardiometabolic patients without evidence of SARS-CoV-2 infection. The CorCOVID Latam Psy Study. Curr Probl Cardiol. 2020. November 2; 100737 DOI: 10.1016/j.cpcardiol.2020.100737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sumner JA, Khodneva Y, Muntner P, et al. Effects of concurrent depressive symptoms and perceived stress on cardiovascular risk in low- and high-income participants: Findings from the reasons for geographical and racial differences in stroke (REGARDS) Study. J Am Heart Assoc. 2016; 5(10): e003930 DOI: 10.1161/JAHA.116.003930 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Pierce M, Hope H, Ford T, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population [published online ahead of print, 2020 Jul 21]. Lancet Psychiatry. 2020; S2215-0366(20)30308-4. DOI: 10.1016/S2215-0366(20)30308-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lopez Santi R. The development of resilience as behavioral support for chronic disease carriers: Perspectives during COVID-19. J Electrocardiol. 2020. (In Press). DOI: 10.1016/j.jelectrocard.2020.08.018 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
CorCOVID Survey.
Investigators.