

Abstract
Objective To describe a new presentation of tears and retears of the rotator cuff, which we denominate captured rotator cuff (CRC). We also aim to evaluate it clinically and through images.
Methods We assessed retrospectively 16 patients with intraoperative diagnosis of CRC between March 2005 and September 2017; by means of imaging (radiography and magnetic resonance imaging [MRI]) and functional scores (UCLA and Constant & Murley). In images we analyzed the evolution for rotator cuff arthropathy and presence of retears. Functionally, we compared the affected side with the contralateral side and extensive lesions with nonextensive.
Results Five (31.25%) patients presented with rotator cuff arthropathy, and 10 (62.5%) with retears. Three (75%) patients with nonextensive lesions had good/excellent UCLA and Constant & Murley scores. In patients with extensive lesions, when the Constant & Murley score was evaluated, 6 (50%) presented good/excellent results, and in the UCLA score, 7 (58.3%). Comparing the affected side (Constant 74.72 points; UCLA 20 points) with the contralateral side (Constant 96.96 points; UCLA 25.63 points), there were worse functional results with statistical significance.
Conclusion The diagnosis of CRC is suspected by characteristic findings on MRI and confirmed in arthroscopy. The affected shoulders present worse functional postoperative scores.
Keywords: rotator cuff, shoulder, rupture, subacromial adhesions
Introduction
Rotator cuff (RC) injuries are among the most common upper limb orthopedic conditions. 1 The repair of these lesions was first described by Codman in 1911. 2 With the advancement and popularization of arthroscopic techniques, and improvement in the quality of imaging, postoperative complications have been more diagnosed and studied. Shoulder stiffness is one of the most common postoperative complications and is present in 4.8 to 8.7% of patients in some series. 3 4 Retear is the most common and can reach 94%, as described by Paxton et al. 5 Some factors are related to an increased risk of retear, including: lesion size, fat infiltration, muscle atrophy, age and work activity. 6 7 The clinical outcome after repair of a retear remains inconclusive. While some studies indicate poor results, others state that there is no clinically negative impact. 8 9
In 1996, Mormino et al 10 described a form of complication of open and arthroscopic repair of total and partial ruptures of the RC, calling it the “captured shoulder” (CS). The criteria for confirming the diagnosis were defined as subdeltoid adhesions of the RC, healed tendon repair and associated osteochondral lesions.
Among the patients who underwent arthroscopic surgery due to rupture of the RC, in our group, subacromial adhesions of the previously repaired tendons were verified. This feature was also identified in shoulders without previous surgery.
The purpose of the present study is to describe a new presentation of tear and retear of the RC, which we call captured rotator cuff (CRC). We also aim to evaluate it clinically and by means of images.
Materials and Methods
From March 2005 to September 2017, 16 patients had intraoperative diagnosis of CRC. These lesions were defined by the presence of complete rupture of one or more tendons of the RC associated with their adherence to the acromion. All of the cases were operated arthroscopically by the same team.
The present study included patients with a minimum follow-up of 12 months (maximum of 101 months) and surgical findings as mentioned above. Following the exclusion criteria, those with incomplete data, previous surgeries unrelated to arthroscopic repair of the RC, and with poor quality imaging, were not part of the study.
After selecting the inclusion and exclusion criteria, from a total of 4038 shoulders undergoing arthroscopic RC rupture repair, we obtained 16 patients, with a total of 16 shoulders, equivalent to 0.39%.
In the clinical evaluation, the Constant & Murley score was considered, 11 as well as the University of California at Los Angeles (UCLA) score 12 and the visual analogue scale (VAS). 13
The patients underwent on-site clinical evaluation with at least 1 year of follow-up. In those patients who were diagnosed with CRC, the radiographic study evaluated the Hamada 14 and Seebauer 15 classifications for those with RC arthropathy. On magnetic resonance imaging (MRI), postoperative healing was evaluated by the Sugaya classification 16 as: type 1) sufficient tendon thickness with low intensity homogeneous tendon; type 2) sufficient tendon thickness with high intensity area; type 3) insufficient tendon thickness with no discontinuity; type 4) presence of minor discontinuity; type 5) presence of major discontinuity.
Radiographic examinations were performed on a Siemens DR digital device (Siemens Healthcare GmbH, Erlangen, Bavaria, Germany), in true anteroposterior position, in neutral, medial rotation, lateral rotation, outlet view and simple axillary profile. The magnetic resonance exams were performed in a GE 1.5 T Signa device (General Electric Medical Systems, Milwaukee, WI, USA). The evaluation of the examinations and measurements were made by three fellows of the shoulder surgery service, with the help of a radiologist specialized in musculoskeletal radiology with more than 10 years of experience.
In five patients, we observed specific characteristics on preoperative MRI ( Figure 1 ). There is a continuity between the tendon stump and the subacromial/subdeltoid bursa to which it is thickened. The tendon stump is displaced/oriented superiorly with a liquid sheet between it and the superomedial surface of the humeral head, in this case with a maximum distance of 3.9 mm.
Fig. 1.

( A ) Continuity between the tendon stump and the subacromial bursa (black arrow). ( B ) Orientation/superior dislocation of the tendon stump (white arrow) and fluid sheet between it and the superomedial surface of the humeral head (3.92mm).
Lesions were classified as nonextensive lesion, affecting one single tendon of the RC, and extensive lesion, affecting two or more tendons 17 according to intraoperative findings. We compared the mean value of functional scores in patients with extensive and nonextensive lesions, and the affected side with the contralateral side.
The Constant & Murley score was grouped according to Boehm: 18 excellent (≥ 91), good (81–90), satisfactory (71–80), regular (61–70), or poor (≤ 60). According to Amstutz et al, 12 results found using the UCLA method can be excellent (≥ 25 points), good (18–24 points), regular (9–17 points) or poor (≤ 8 points). For the VAS measurement, numerical values between 0 and 10 were used, where 0 represents no pain, and 10 as the maximum pain felt by the patient. 13
Data were compared by statistical analysis using the chi-squared test, the Fisher exact test and paired t-test using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY, USA). The study was approved by the Ethics Committee of the responsible institution under the number CAAE 97060718.4.0000.5126.
Surgical Technique
Patient under general anesthesia and brachial plexus block, in lateral decubitus with 15° dorsal inclination, and upper limb traction affected with 30° abduction and 15° flexion. The surgical procedure begins with glenohumeral inspection through the standard posterior portal. In cases where there are lesions or signs of subluxation/dislocation of the biceps long head tendon, tenotomy with or without tenodesis is performed. The bursal space is accessed using posterior portal for visualization, lateral for instrumentation and anterior for irrigation and instrumentation. Attention should be taken at this time, because in these cases of CRC, unlike normal subacromial vision, we find the sign of “empty shoulder” ( Figure 2 ), characterized by the nonvisualization of the RC, and the impression that the optic is still positioned in the articular space. At this time, the surgeon should look for the acromial RC adhesions ( Figure 3 ). After their identification, a cleavage plane is created with the aid of a synovial shaver blade or of a periosteum detachment ( Figure 4 ). With proper release, tendon flexibility is verified ( Figure 5 ) and repair is performed with as little tension as possible ( Figure 6 ), using metal anchors and high strength synthetic wires. Acromioplasty is performed at the discretion of the shoulder based on the presence of subacromial friction signal. One of the group surgeons does not perform the procedure (13 acromioplasties). Postoperatively, the patient is placed in a sling with abduction cushion for a period between 3 weeks (lesions ≤ 2 cm) and six weeks (lesions > 2 cm). The patient is oriented to actively mobilize the elbow, wrist and fingers from the first day after surgery. The physiotherapy program with passive and self-passive exercises for range of motion gain and analgesia (ultrasound, transcutaneous electrical neurostimulation, cryotherapy) begins after removal of the sling. Isometric strengthening starts from 8 to 12 weeks and isotonic strengthening from 12 to 16 weeks depending on the size of the lesion.
Fig. 2.
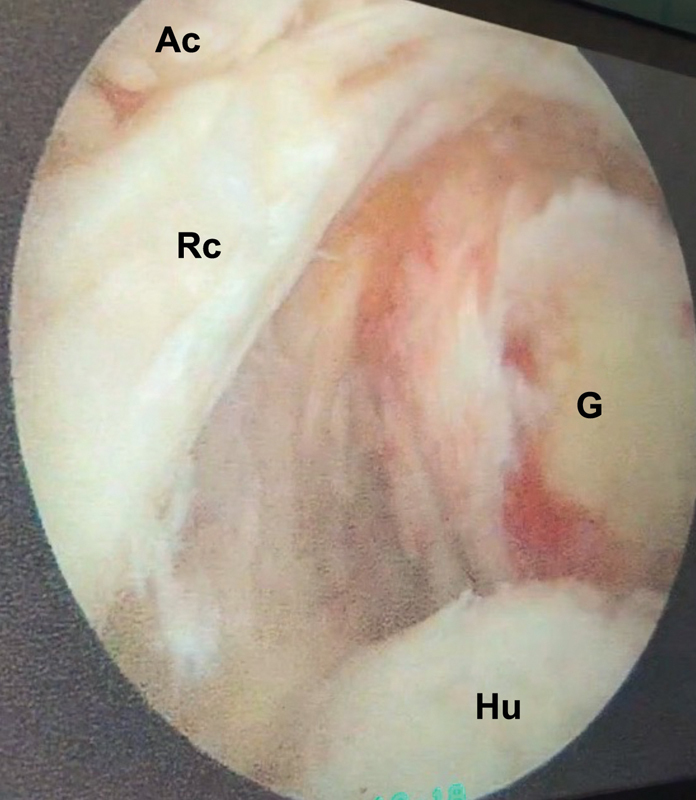
"Empty shoulder" sign. G: glenoid. Ac: acromion; RC: rotator cuff; Hu: humerus.
Fig. 3.

Adhesions between tendons of the RC and the acromion. Ac: acromion; RC: rotator cuff; Hu: humerus.
Fig. 4.

Creating cleavage plane between the acromion (Ac) and the rotator cuff (RC). Hu: humerus; SB: synovial shaver blade.
Fig. 5.

Rotator cuff released from the acromion and evaluation of tendon flexibility with Grasper instruments (G). Hu: humerus; GT: Greater tubercle.
Fig. 6.

Tendon sutured in its footprint using metal anchors (black arrows). Ac: acromion; RC: rotator cuff; GT: Greater tuber.
Results
Epidemiological and intraoperative data are presented in Table 1 .
Table 1. Epidemiological and intraoperative data.
| Mean age at surgery | 58.18 years old | Minimum: 42 Maximum: 69 |
| Gender (male/female) | 9/7 | 56,25%/43,75% |
| Affected side (right/left) | 13/3 | 81,25%/18,75% |
| Dominance (right-handed/left-handed) | 15/1 | 93,75%/6,25% |
| Type of repair | Complete | 14 (87,5%) |
| Partial | 2 (12,5%) | |
| Complementary Findings and/or Complementary Procedures | Acromioplasty | 14 (87,5%) |
| Tenotomy of LHBT | 8 (50%) | |
| Tenodesis of LHBT | 1 (6,25%) | |
| Previous tear of LHBT | 2 (12,5%) | |
| Ruptured tendons | SS | 4 (25%) |
| SS + IS | 8 (50%) | |
| SS + IS + Tm | 2 (12,5%) | |
| SS + SC | 2 (12,5%) |
Abbreviations: IS, infraspinatus; LHBT, long head biceps tendon; SC, subscapularis; SS, supraspinatus; Tm, teres minor.
Patients with extensive lesions (mean 73.4 points; 36.1 to 97.8) had a worse Constant & Murley score compared with those with nonextensive lesions (mean 78.2 points; 30.1 to 103.1); without statistical significance ( Table 2 ). Both patients undergoing partial repair had regular functional scores. Neither evolved with rotator cuff arthropathy. The 14 (87.5%) patients with total repair had good and excellent functional scores.
Table 2. Lesion extension versus Constant & Murley (Postoperative) .
| Constant | Total |
p-value
:
0.384 |
||||||
| Poor | Regular | Good | Excellent | |||||
| Lesion | Nonextensive | n | 1 | 0 | 2 | 1 | 4 | |
| % | 25.0% | 0.0% | 50.0% | 25.0% | 100.0% | |||
| Extensive | n | 1 | 5 | 5 | 1 | 12 | ||
| % | 8.3% | 41.7% | 41.7% | 8.3% | 100.0% | |||
| Total | n | 2 | 5 | 7 | 2 | 16 | ||
| % | 12.5% | 31.3% | 43.8% | 12.5% | 100.0% | |||
Chi-square test.
Patients with extensive lesions (mean 19.3 points; 8 to 30) had worse UCLA scores compared with those with nonextensive lesions (mean 23.5 points, ranging from 10 to 30) but without statistical significance ( Table 3 ).
Table 3. Postoperative UCLA versus lesion extension.
| UCLA | Total |
p-value
0.572 |
||||||
| Poor | Regular | Good | Excellent | |||||
| Lesion | Nonextensive | n | 0 | 1 | 0 | 3 | 4 | |
| % | 0.0% | 25.0% | 0.0% | 75.0% | 100.0% | |||
| Extensive | n | 2 | 3 | 2 | 5 | 12 | ||
| % | 16.7% | 25.0% | 16.7% | 41.7% | 100.0% | |||
| Total | n | 2 | 4 | 2 | 8 | 16 | ||
| % | 12.5% | 25.0% | 12.5% | 50.0% | 100.0% | |||
Chi-square test.
Patients with nonextensive lesions had a higher proportion of good and excellent Constant & Murley and UCLA scores (75% in both), compared with those with extensive injury (50% and 58.3%, respectively); without statistical significance ( p = 0.585 Constant & Murley score; p = 1.000 UCLA; Fisher exact test).
When comparing the mean Constant & Murley and UCLA scores of the affected side (74.72 and 20 points, respectively) with the contralateral side (96.96 and 25.63 points) there was worse result on the operated side, with statistical significance ( Table 4 and 5 ).
Table 4. Constant and Murley mean score of affected side versus contralateral side.
| Comparation | Mean | Standard Deviation | Mean difference | 95% CI for mean difference | p-value | |
|---|---|---|---|---|---|---|
| Affected side | 74.72 | 20.82 | −22.24 | −32.87 | −11.62 | <0.001 |
| Contralateral side | 96.96 | 12.95 | ||||
Paired T test.
Table 5. Mean UCLA score of affected side versus contralateral side.
| Comparation | Mean | Standard Deviation | Mean difference | 95% CI for mean difference | p-value | |
|---|---|---|---|---|---|---|
| Affected side | 20.00 | 8.48 | −5.63 | −9.96 | −1.29 | 0.014 |
| Contralateral side | 25.63 | 6.35 | ||||
Paired T test.
Five (31.25%) patients were diagnosed with rotator cuff arthropathy, presenting decreased acromion-humeral distance with or without acetabularization of the coracoacromial arch and glenohumeral arthrosis. ( Table 6 ).
Table 6. Radiographic classifications.
| Types | Quantity | |
|---|---|---|
| Hamada | 1 | 8 (50%) |
| 2 | 3 (18.75%) | |
| 3 | 0 | |
| 4A | 3 (18.75%) | |
| 4B | 2 (12.5%) | |
| 5 | 0 | |
| Seebauer | IA | 0 |
| IB | 2 (12.5%) | |
| IIA | 3 (18.75%) | |
| IIB | 0 |
At the review consultation, there was a decrease in VAS from 6.8 (3 to 10) to 2.7 (0 to 9).
By the Sugaya classification, we found 1 patient (6.25%) type 1, 2 (12.5%) type 2, 3 (18.7%) type 3 and 10 (62.5%) type 5. There were no patients with Sugaya type 4. Patients with extensive lesions had a higher proportion of retears when compared to those with nonextensive lesions (67 versus 50%).
Of the three patients diagnosed with primary CRC, two (one with nonextensive lesion and one with extensive lesion) had good and excellent functional scores with healed tendon (Sugaya 1 and 2). The third patient had an extensive lesion, complete repair was performed, but he presented low functional scores, evolving with RC arthropathy (Hamada 4 A).
Discussion
In the present study, evaluating 16 patients with clinical and arthroscopic CRC, we found significant differences in relation to the article described by Mormino et al, 10 in which they analyzed that all patients underwent a previous procedure of acromioplasty with repair of rotator cuff injury or partial lesion debridement. These patients presented stiffness and pain after this first procedure and were therefore submitted to a new arthroscopic approach in which the findings of the so-called CS were identified. In contrast, no patient in our sample had postoperative stiffness, and in three cases we observed CRC in patients with complete RC tear and without previous surgery.
Mormino established three diagnostic criteria for intraoperative findings: 1) healed tendon lesions; 2) subdeltoid adhesions of the RC; 3) chondral lesion in the glenoid. In our patients, we observed: 1) tendon ruptures of the RC (relapses or primary), 2) RC adhered to the acromion, and 3) sign of "empty shoulder." We did not find subdeltoid adhesions or chondral lesions associated. Due to these differences, our findings describe a pathology to which the name of CS is not reliable, so we chose to name it CRC.
It is noteworthy that certain factors may have contributed to the differences in diagnostic criteria between CS and CRC. In addition to the association between open and video surgery, the arthroscopic technique in the 1990s was still in its early stages of improvement. Contrary to what happens today, when there is more experience in arthroscopy.
Two (12.5%) patients presented preoperatively with pseudoparalysis (anterior active elevation < 90°, complete passive elevation, and absence of causative neurological or osteoarticular injury) and none had joint stiffness. Captured rotator cuff developed primarily in 3 (18.75%); of these, 1 progressed poorly, with regular UCLA and progression to RC arthropathy.
Choi et al, 6 evaluating 147 patients who underwent arthroscopic repair of medium, large and extensive RC injuries, found a mean Constant & Murley score, after repair, of 84.3 points. Kim et al, 19 in 221 RC repair arthroscopies, achieved a mean Constant & Murley score of 89.3 points and 33% of rupture. Agout et al, 20 after 10 years of follow-up, noted that among 965 shoulders with RC tears arthroscopically repaired, the mean Constant & Murley score was 77.8 points, as well as 19% of retear in nonextensive lesions, and 29.3% in extensive lesions. Collin et al, 21 in a sample of 234 patients with arthroscopic repair of extensive posterosuperior lesions, at 10 years of follow-up, found a mean Constant & Murley score of 78.5 points, 34% of retear, and 47% of new rupture after secondary repair. Miyazaki et al, 22 evaluating 163 arthroscopically operated shoulders in patients ≥ 65 years old, using the UCLA score, obtained 96.4% of good and excellent results, as well as 2.45% of retear. Godinho et al, 23 analyzing 86 shoulders after RC repair for nontraumatic (51 shoulders) and traumatic (35 shoulders) injuries, the mean modified UCLA was 33.7 points in the first group, and 32.8 points in the second. In the present study, we obtained a mean Constant & Murley score of 74.7 points, a mean UCLA of 20 points, and a retear ratio (Sugaya 5) of 62.5%. One patient (33.3%) with primary CRC, and 9 (69.27%) with secondary CRC had retear. Comparing with the literature, we believe that patients with CRC have a worse functional score, and greater likelihood of retear in both primary and secondary patients.
In a previous article of the group, 24 evaluating 100 patients (110 shoulders), the clinical outcome of the complete RC rupture repair showed a high percentage of functional recovery (Constant & Murley 83.96) when compared to the contralateral side (Constant & Murley 85.3). In contrast, in the present study, there was a worse functional result of the affected shoulders (Constant & Murley 74.71) when compared to the contralateral side (Constant & Murley 96.95), with statistical significance.
In 5 of the 16 patients diagnosed with CRC, we found the following MRI findings: 1) thickening of the subacromial/subdeltoid bursa; 2) continuity between the tendon stump and these bursa; 3) superior orientation of the tendon stump and 4) presence of a sheet of fluid between the tendon stump and the superomedial surface of the humeral head. These characteristics described above may suggest the diagnosis of CRC.
We did not find any definite cause that explains CRC; however, we think some factors may be associated with this condition. One of the functions of the biceps is to be a secondary humeral head depressant; 25 26 two patients (one of them primary) had previous rupture of the biceps. It is also known that one of the advantages of performing acromioplasty is the increase in local concentration of growth and angiogenic factors, influencing the tendon healing of the RC. 27 28 On the other hand, during acromioplasty, a bleeding bone bed is formed, conducive to possible adhesions. Fourteen patients underwent previous acromioplasty. Further studies are needed to establish and confirm the causal factors of this entity.
In the literature, we find several articles citing CS as a cause of stiffness; these authors describe that its prevention requires early rehabilitation. 3 29 30 However, to our knowledge, this is the only article describing this presentation of a lesion of the RC, the CRC.
As limitations, we had a small sample (16 patients) and did not have a control group to compare functional results.
Conclusion
Captured rotator cuff diagnosis is confirmed by arthroscopy with the following criteria: 1) empty shoulder sign; 2) rupture or retear of one or more tendons of the RC; and 3) adherence of the ruptured tendons to the acromion.
The affected shoulders have worse postoperative functional scores with statistical significance compared to the contralateral shoulder.
Magnetic resonance imaging may show superior displacement of the tendon stump, continuity of the tendon with the subacromial bursa, and a fluid sheet separating the tendon of the RC from the humeral head.
Footnotes
Conflito de Interesses Os autores declaram não haver conflito de interesses.
Referências
- 1.Chen A L, Mears S C, Hawkins R J. Orthopaedic care of the aging athlete. J Am Acad Orthop Surg. 2005;13(06):407–416. doi: 10.5435/00124635-200510000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Codman E A. Boston: Thomas Todd; 1934. Rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. The shoulder. [Google Scholar]
- 3.Brislin KJ, Field LD, Savoie FH 3rd. Complications after arthros- copic rotator cuff repair. Arthroscopy 2007;23(02):124–128 [DOI] [PubMed]
- 4.Huberty D P, Schoolfield J D, Brady P C, Vadala A P, Arrigoni P, Burkhart S S. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(08):880–890. doi: 10.1016/j.arthro.2009.01.018. [DOI] [PubMed] [Google Scholar]
- 5.Paxton E S, Teefey S A, Dahiya N, Keener J D, Yamaguchi K, Galatz L M. Clinical and radiographic outcomes of failed repairs of large or massive rotator cuff tears: minimum ten-year follow-up. J Bone Joint Surg Am. 2013;95(07):627–632. doi: 10.2106/JBJS.L.00255. [DOI] [PubMed] [Google Scholar]
- 6.Choi S, Kim M K, Kim G M, Roh Y H, Hwang I K, Kang H. Factors associated with clinical and structural outcomes after arthroscopic rotator cuff repair with a suture bridge technique in medium, large, and massive tears. J Shoulder Elbow Surg. 2014;23(11):1675–1681. doi: 10.1016/j.jse.2014.02.021. [DOI] [PubMed] [Google Scholar]
- 7.Cho N S, Lee B G, Rhee Y G. Arthroscopic rotator cuff repair using a suture bridge technique: is the repair integrity actually maintained? Am J Sports Med. 2011;39(10):2108–2116. doi: 10.1177/0363546510397171. [DOI] [PubMed] [Google Scholar]
- 8.
- 9.
- 10.Mormino M A, Gross R M, McCarthy J A. Captured shoulder: a complication of rotator cuff surgery. Arthroscopy. 1996;12(04):457–461. doi: 10.1016/s0749-8063(96)90040-7. [DOI] [PubMed] [Google Scholar]
- 11.Constant C R, Murley A H. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;(214):160–164. [PubMed] [Google Scholar]
- 12.Amstutz H C, Sew Hoy A L, Clarke I C. UCLA anatomic total shoulder arthroplasty. Clin Orthop Relat Res. 1981;(155):7–20. [PubMed] [Google Scholar]
- 13.Huskisson E C.Measurement of pain Lancet 19742(7889):1127–1131. [DOI] [PubMed] [Google Scholar]
- 14.Hamada K, Fukuda H, Mikasa M, Kobayashi Y. Roentgenographic findings in massive rotator cuff tears. A long-term observation. Clin Orthop Relat Res. 1990;(254):92–96. [PubMed] [Google Scholar]
- 15.Seebauer L. Biomecanical classification of cuff tear arthropaty [abstract]. In: Global Shoulder Society Meeting; 2003 July 17–19 Salt Lake City, UT-USA
- 16.Sugaya H, Maeda K, Matsuki K, Moriishi J. Functional and structural outcome after arthroscopic full-thickness rotator cuff repair: single-row versus dual-row fixation. Arthroscopy. 2005;21(11):1307–1316. doi: 10.1016/j.arthro.2005.08.011. [DOI] [PubMed] [Google Scholar]
- 17.Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82(04):505–515. doi: 10.2106/00004623-200004000-00006. [DOI] [PubMed] [Google Scholar]
- 18.Boehm D. Heidelberg: Springer; 2006. Valuation of the Constant score; pp. 20–21. [Google Scholar]
- 19.Kim J H, Hong I T, Ryu K J, Bong S T, Lee Y S, Kim J H. Retear rate in the late postoperative period after arthroscopic rotator cuff repair. Am J Sports Med. 2014;42(11):2606–2613. doi: 10.1177/0363546514547177. [DOI] [PubMed] [Google Scholar]
- 20.Agout C, Berhouet J, Bouju Y. Clinical and anatomic results of rotator cuff repair at 10 years depend on tear type. Knee Surg Sports Traumatol Arthrosc. 2018;26(08):2490–2497. doi: 10.1007/s00167-018-4854-1. [DOI] [PubMed] [Google Scholar]
- 21.Collin P, Colmar M, Thomazeau H. Clinical and MRI Outcomes 10 Years After Repair of Massive Posterosuperior Rotator Cuff Tears. J Bone Joint Surg Am. 2018;100(21):1854–1863. doi: 10.2106/JBJS.17.01190. [DOI] [PubMed] [Google Scholar]
- 22.Miyazaki A N, da Silva L A, Santos P D, Checchia S L, Cohen C, Giora T S. Evaluation of the results from arthroscopic surgical treatment of rotator cuff injuries in patients aged 65 years and over. Rev Bras Ortop. 2015;50(03):305–311. doi: 10.1016/j.rboe.2015.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.
- 24.Abechain J JK, Godinho G G, Matsunaga F T, Netto N A, Daou J P, Tamaoki M JS. Functional outcomes of traumatic and non-traumatic rotator cuff tears after arthroscopic repair. World J Orthop. 2017;8(08):631–637. doi: 10.5312/wjo.v8.i8.631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kido T, Itoi E, Konno N, Sano A, Urayama M, Sato K. The depressor function of biceps on the head of the humerus in shoulders with tears of the rotator cuff. J Bone Joint Surg Br. 2000;82(03):416–419. doi: 10.1302/0301-620x.82b3.10115. [DOI] [PubMed] [Google Scholar]
- 26.
- 27.Frank J M, Chahal J, Frank R M, Cole B J, Verma N N, Romeo A A. The role of acromioplasty for rotator cuff problems. Orthop Clin North Am. 2014;45(02):219–224. doi: 10.1016/j.ocl.2013.12.003. [DOI] [PubMed] [Google Scholar]
- 28.Galliera E, Randelli P, Dogliotti G. Matrix metalloproteases MMP-2 and MMP-9: are they early biomarkers of bone remodelling and healing after arthroscopic acromioplasty? Injury. 2010;41(11):1204–1207. doi: 10.1016/j.injury.2010.09.024. [DOI] [PubMed] [Google Scholar]
- 29.Millett P J, Horan M P, Maland K E, Hawkins R J. Long-term survivorship and outcomes after surgical repair of full-thickness rotator cuff tears. J Shoulder Elbow Surg. 2011;20(04):591–597. doi: 10.1016/j.jse.2010.11.019. [DOI] [PubMed] [Google Scholar]
- 30.





