

Abstract
Background
Society awards provide visibility and national recognition for physicians. Several studies have found that women were underrepresented as award recipients when compared with subspecialty workforce data. However, to our knowledge no studies have examined the gender distribution of award recipients in orthopaedic societies. Orthopaedic surgery remains among the least gender-diverse specialties in medicine. Particularly in academic practice, the increasing paucity of women with progressive rank may reflect unequal access to the currency for promotion, including national reputation and visibility. Therefore, information on orthopaedic awarding practices may help to identify and address challenges associated with recruiting, retaining, and promoting women in orthopaedics.
Questions/purposes
(1) Since the year 2000, have women orthopaedic surgeons received awards in proportion to their society membership? (2) Are the awards granted to women equally distributed across the categories of leadership, humanitarianism, education, scientific investigation, resident/fellow scientific investigation, and diversity? (3) Does the gender distribution of award recipients differ for awards bestowed through a blinded process versus an unblinded process?
Methods
Eighteen national, clinically focused orthopaedic societies in the United States were included. These societies offer a combined total of 69 awards; each award was studied from its earliest record through December 2018, resulting in a study period from 1973 to 2018. Each society provided the gender demographics of their membership in 2018. The proportion of women award recipients from 2000 to 2018 was compared with the proportion of women members in 2018 for each society. Awards were also categorized based on the six types of accomplishment they recognized (leadership, humanitarianism, education, scientific investigation, resident/fellow scientific investigation, and diversity), and whether they were granted through a blinded or unblinded selection process. Chi-square tests were used to compare the proportion of women receiving awards in various categories, and to compare the proportion of women who received awards through blinded selection processes versus unblinded selection processes.
Results
From 2000 to 2018, women received 8% (61 of 794) of all awards and represented 9% (5359 of 59,597) of all society members. Two societies had an underrepresentation of women award recipients compared with their society membership. We found that women were not represented proportionally across award categories. Women were more likely to receive a diversity award than a leadership award (odds ratio 12.0 [95% CI 3.1 to 45.7]; p < 0.001), and also more likely to receive an education award than a leadership award (OR 4.1 [95% CI 1.3 to 12.7]). From 1973 to 2018, 17 of 22 the leadership awards offered by societies have never been granted to a woman. Finally, women were more likely to receive awards bestowed through a blinded process than an unblinded process. Women earned 11% (30 of 285) of awards bestowed through a blinded award process and 6% (31 of 509) of awards bestowed through an unblinded award process (OR 1.8 [95% CI 1.1 to 3.1]; p = 0.03).
Conclusion
The percent of women award recipients was generally proportional to membership overall and in most societies. However, on a national workforce level, the proportion of women award recipients is lower than the proportion of women in academic orthopaedics, which has been reported by others to be about 13%, suggesting that women in academic orthopaedics may be underrepresented as award recipients. Additionally, women were less likely to receive leadership awards than awards of other types, which suggests that women are not being recognized as leaders in orthopaedics. Women were also more likely to receive awards granted through unblinded processes, which raises concern that there may be implicit bias in orthopaedic awarding practices.
Clinical Relevance
We encourage societies to examine the inclusiveness of their awards selection processes and to track the demographic information of award recipients over time to measure progress toward equal representation. Creating standardized award criteria, including women on selection committees, requiring the consideration of diverse nominees, and implicit bias training for selection committees may help to reduce bias in awarding practices.
Introduction
Despite efforts to improve gender parity in orthopaedic surgery, very little progress has been made over the last decade. According to physician workforce data in the United States, women comprised 4% of practicing orthopaedic surgeons in 2007, compared with 5% of practicing orthopaedic surgeons in 2017 [2, 4]. Even with efforts to recruit and support women, orthopaedics has one of the lowest proportions of women residents and fellows of any medical specialty at only 15% in 2017 [6]. In the academic practice environment, the proportion of women who are faculty members in orthopaedics is lower than in any other specialty [7]. Additionally, significant disparities exist within the orthopaedic academic promotion pipeline. Among full-time MD faculty in 2015, women comprised 16% of assistant professors, 10% of associate professors, and 7% of professors in orthopaedic surgery [5]. This phenomenon of decreasing diversity with increasing rank is known as the “leaky pipeline” [17]; at every level of promotion and advancement, women fail to progress, or “leak” from the talent pipeline. Promotion and advancement in academia depend largely on national reputation and visibility [24], raising the question of whether opportunities to achieve national recognition may be more limited for women surgeons than for men.
Awards are “external markers of professional achievement” and, as such, are important for professional visibility, promotion, and career advancement for physicians, particularly in academia [14]. Awards also reflect the characteristics and accomplishments that a group values. Therefore, the diversity of award recipients can be seen as a proxy for the inclusivity of specialty societies [21]. The gender diversity of award recipients has been studied in several medical and surgical specialties, and all have shown substantial underrepresentation of women among award recipients [19–21]. To our knowledge, gender representation in orthopaedic surgery society awards has never been studied. Given the evidence of the leaky pipeline phenomenon within academic orthopaedic promotion and advancement, information on orthopaedic awarding practices may help to identify and address one of the challenges associated with recruiting, retaining, and promoting women in orthopaedics. We aimed to comprehensively study the current and historical gender distribution of orthopaedic society award recipients, with a particular emphasis on the relationship between gender and the type of awards received, as well as the impact of blinded and unblinded selection processes.
Therefore, we asked, (1) Since the year 2000, have women orthopaedic surgeons received awards in proportion to their society membership? (2) Are the awards granted to women equally distributed across the categories of leadership, humanitarianism, education, scientific investigation, resident/fellow scientific investigation, and diversity? (3) Does the gender distribution of award recipients differ for awards bestowed through a blinded process versus an unblinded process?
Materials and Methods
Societies Studied
The American Academy of Orthopaedic Surgeons (AAOS), the American Orthopaedic Association (AOA) and all societies on the AAOS Board of Specialty Societies (AAOS BOS) with a clinical orthopaedic or diversity focus were invited to participate in this study [1]. AAOS BOS societies with a primary focus of rehabilitation, research, or musculoskeletal infection were excluded. The Ruth Jackson Orthopaedic Society was excluded because it does not grant awards. Eighteen societies met all inclusion and no exclusion criteria.
This work was deemed non-human subjects research by the institutional review board at Washington University in St. Louis, MO, USA.
Society Membership
Societies provided aggregate gender demographic information for their society members in 2018. Societies were asked to include data from all membership categories in their membership count (for example: candidate members, associate members, full members, etc.). All 18 societies responded to our request for information. Twelve societies provided aggregate gender data for their 2018 members. Three societies did not keep historical membership records and provided 2019 membership information. The Arthroscopy Association of North America organization was unable to provide membership data, so it was excluded from any analysis requiring comparisons to membership. Two societies did not track demographic information for their members and provided a list of member names.
For each list of member names provided, two coders (TC, DK) undertook a prespecified process to assign gender to each member. First, traditional naming conventions were applied when applicable; for example, a recipient with the first name “John” was coded as a man without further investigation. If the gender of the first name was ambiguous, an online search was performed using ResearchGate, LinkedIn, and/or the hospital or research department’s website. If gender could not be definitively determined after exhausting this process, then that person was excluded from the study. To establish inter-rater reliability between the two coders (TC, DK) 10% of the membership lists were cross coded to determine Cohen’s kappa. Cohen’s kappa for member gender was 0.9 indicating excellent agreement [9].
Overall in 2018, 9% (5359 of 59,597) of orthopaedic society members were women, ranging from 1% to 27% of members. In total, 4% (2315 of 61,912) of society members had an unknown gender, either because it was unknown to the society (that is, the member did not specify their gender in society records) (n = 2229), or because the member’s gender could not be determined by the coders after using the gender-coding process described above (n = 86). Less than 2% of members in each society had an unknown gender, with the exceptions of AOSSM (30%, n = 1161) and AOA (28%, n = 461).
Definition of an Award
An award was defined as an honor retrospectively given to a person for an achievement. Grants and scholarships were not included. Awards could include a monetary gift; however, an award was excluded if its purpose was to support future research, training, or professional development opportunities (such as attending a meeting, travel, or attending a course). Recipients could be self-nominated or nominated by a colleague. Awards with more than five recipients per year were excluded. All award recipients were tabulated from the earliest record of each award through December 2018. The first author was tabulated as the sole recipient of an award if it was granted for a paper or project with multiple authors.
Determination of Gender and Professional Certification
Throughout the study, gender was determined using the same process described above. Each recipient was classified as having either an MD or MD-equivalent (for example, MD, DO, or MBBS) or non-MD degree (for example, PhD, PT, OT, or RN) at the time of award designation. This was determined by looking at the award recipient’s degree in the official meeting brochure or award history on the society’s website. If the degree was not listed, we searched the internet to determine the individual’s degree. Award recipients without an MD or MD-equivalent were excluded from the analysis, given that our population of interest was orthopaedic surgeons.
Award Information
In July 2019, we queried society websites and annual meeting programs for awards information. All publicly available awards and recipients were recorded for each society. If the society website and/or meeting program did not specify a list of awards or recipients, we contacted the societies to provide data. Complete awards data were obtained for 17 of the 18 societies. The Knee Society could not provide historical data for their Chitranjan S. Ranawat MD Award, John N. Insall MD Award, and Mark B. Coventry MD Award. The earliest documented award was given in 1973, and all awards through 2018 were included.
Over the entire study period, from 1973 to 2018, 1112 award recipients were tabulated across all societies. Gender was determined for 99% (1106 of 1112) of award recipients. In total, 92% (1018 of 1106) of awards were granted to an individual with an MD equivalent, our population of interest. Of the 35 named awards, all awards were named after men.
Time Period and Rationale for Comparisons
For historical perspective, we included descriptive data for awards bestowed from 1973 to 2018. However, given that demographic changes have occurred in the field over this period, we used the 21st century (2000-2018) as a more relevant subset of time for detailed analysis. Unless clearly indicated, all measurements and analysis are from 2000 to 2018 data only.
Demographic information on the gender distribution of orthopaedic society members was only available for the year 2018. Given that the only available physician workforce data demonstrates a relative plateau in the gender distribution of orthopaedic surgeons from 2007 to 2017 [2, 4], we compared 2018 society membership data to awards data from 2000 to 2018. This period provided a large enough sample of award recipients for meaningful analysis while maintaining a reasonably accurate denominator.
In addition to society-level data, it is important to consider two denominators: the proportion of women who are practicing orthopaedic surgeons overall, and the proportion of women who practice in academic orthopaedic settings. The most recent data available shows that in 2018, women comprised 5% of practicing orthopaedic surgeons overall, and in 2015 women were 13% of full-time MD orthopaedic department faculty members [2, 3]. Although statistical calculations were not performed with these numbers, these denominators provide further context for our data because they highlight the demographics of surgeons who are eligible for awards versus the demographics of who is receiving awards on a workforce level.
Award Recognition Types
We divided all awards into six categories based on the type of accomplishment being recognized: leadership, humanitarianism, diversity, education (teaching or mentoring), scientific investigation, or resident/fellow scientific investigation (Table 1). Awards were categorized based on the description of the award provided on the society website. Societies were contacted by email or telephone to clarify if the description of the award was ambiguous.
Table 1.
Award types, definitions, and number of awards in each category from 1973-2018
| Type of award | Definition | Number of awards |
| Leadership | Recognition of major scientific advancements and lifetime achievements in the field | 22 |
| Humanitarianism | Recognition of work benefitting underserved populations | 4 |
| Diversity | Either recognition for promoting gender/racial diversity, or any recognition reserved for gender/racial minority individuals. | 3 |
| Education | Recognition for teaching and/or mentoring | 6 |
| Scientific investigation | Recognition of an exceptional/impactful paper, abstract, poster, or other work | 26 |
| Resident/fellow scientific investigation | Recognition of an exceptional/impactful paper, abstract, poster, or other work submitted by a resident or fellow | 8 |
| Total | 69 |
Award Blinding
We defined each award as blinded or unblinded based on the method of recipient selection. We examined the description of the award and application instruction on the society websites to determine whether each award was blinded or unblinded. If the description or instruction was ambiguous, we contacted the societies by email or telephone for clarification.
Outcomes
Our primary outcome was the overall proportion of women who received awards relative to their society membership. We assessed this by comparing the proportion of women award recipients (2000-2018) in each society relative to that society’s 2018 membership. Our secondary outcomes were the proportion of women recipients in each award category and the proportion of women receiving blinded awards versus those receiving unblinded awards.
Statistical Analysis
To compare the proportion of women award recipients to society membership, we calculated the % difference with 95% confidence intervals between % women award recipients and % women members, using the MedCalc software (Ostend, Belgium) comparison of proportions test [15].
We used chi-square or Fisher’s exact test to evaluate the independence of cross-tabulated counts. The results of these analyses are expressed as odds ratios with 95% CIs and associated p values. All statistical analyses were two-tailed, and a significance level of 0.05 was considered significant. These statistical tests were performed using SAS Base software version 9.4 (SAS, Cary, NC, USA).
Results
Representation of Women Among Award Recipients
Since 2000, women members were proportionately represented as society award recipients overall. Of the 12 societies with more than 25 award recipients from 2000 to 2018 and membership data available, two societies, AOSSM and POSNA, had underrepresentation of women award recipients compared with their membership. The 10 other societies had no differences between the gender distribution of their award recipients and membership (Table 2). Of awards bestowed from 2000 to 2018, women received 8% (61 of 794) of all awards, with a range of 0% to 28% between societies (Fig. 1).
Table 2.
Gender distribution of orthopaedic society awards from 2000-2018 compared with 2018 society membership
| Awards (2000-2018) | Membership (2018) | ||||||||
| Society | Number of men award recipients | Number of women award recipients | Percentage of women award recipientsa | Number of members | Number of men members | Number of women members | Percentage of women members | % difference (95% CI) | p value |
| AAHKS | 43 | 0 | 0% | 3953 | 3712 | 241 | 6% | 6% (-2 to 7) | 0.1 |
| AAHSa | 16 | 2 | 1590 | 1211 | 379 | 24% | |||
| AANAb | 54 | 11 | 17% | ||||||
| AAOS | 49 | 2 | 4% | 29,403 | 27,671 | 1732 | 6% | 2% (-7 to 5) | 0.6 |
| AOA | 33 | 1 | 3% | 1186 | 1075 | 111 | 9% | 6% (-6 to 10) | 0.2 |
| AOFAS | 34 | 5 | 13% | 2015 | 1782 | 233 | 12% | 1% (-6 to 15) | 0.8 |
| AOSSM | 183 | 6 | 3% | 2755 | 2497 | 258 | 9% | 6% (3 to 8) | < 0.01 |
| ASES | 31 | 3 | 9% | 850 | 802 | 48 | 6% | 3% (-3 to 17) | 0.4 |
| ASSH | 33 | 6 | 15% | 4553 | 3801 | 752 | 17% | 1% (-13 to 9) | 0.9 |
| Hip | 53 | 2 | 4% | 200 | 195 | 5 | 3% | 1% (-3 to 10) | 0.7 |
| JRGOSa | 14 | 3 | 571 | 416 | 155 | 27% | |||
| Kneea | 6 | 0 | 198 | 196 | 2 | 1% | |||
| LLRSa | 9 | 0 | 155 | 132 | 23 | 15% | |||
| MSTS | 21 | 8 | 28% | 344 | 284 | 60 | 17% | 10% (-4 to 29) | 0.2 |
| NASS | 52 | 2 | 4% | 7252 | 6551 | 701 | 10% | 6% (-9 to 3) | 0.1 |
| OTAa | 20 | 2 | 2410 | 2176 | 234 | 10% | |||
| POSNA | 53 | 2 | 4% | 1470 | 1130 | 340 | 23% | 19% (11 to 23) | < 0.001 |
| SOMOS | 29 | 6 | 17% | 692 | 607 | 85 | 12% | 5% (-5 to 21) | 0.4 |
The percentage of women award recipients and the percent difference are only reported for societies with more than 25 award recipients. If blank, this society had fewer than 25 award recipients from 2000 to 2018. The percent difference is calculated as the absolute difference between the percentage of women award recipients and the percentage of women members.
AANA could not provide membership demographic information; AAHKS = American Association of Hip and Knee Surgeons; AAHS = American Association for Hand Surgery; AANA = Arthroscopy Association of North America; AAOS = American Academy of Orthopaedic Surgeons; AOA = American Orthopaedic Association; AOFAS = Association of Foot and Ankle Surgeons; AOSSM = Association Orthopaedic Society for Sports Medicine; ASES = American Shoulder and Elbow Surgeons; ASSH = American Society for Surgery of the Hand; Hip = The Hip Society; JRGOS = J. Robert Gladden Orthopaedic Society; Knee = The Knee Society; LRRS = Limb Lengthening and Reconstruction Society; MSTS = Musculoskeletal Tumor Society; NASS = North American Spine Society; OTA = Orthopaedic Trauma Association; POSNA = Pediatric Orthopaedic Society of North America; SOMOS = Society of Military Orthopaedic Surgeons.
Fig. 1.

This graph shows the proportion of award recipients by gender for each orthopaedic society from 2000 to 2018. Please note that societies to the right of the black line had fewer than 25 award recipients. Denominators of 25 or less may be too small to be accurately described as proportions; AAHKS = American Association of Hip and Knee Surgeons; AANA = Arthroscopy Association of North America; AAOS = American Academy of Orthopaedic Surgeons; AOA = American Orthopaedic Association; AOFAS = Association of Foot and Ankle Surgeons; AOSSM = Association Orthopaedic Society for Sports Medicine; ASES = American Shoulder and Elbow Surgeons; ASSH = American Society for Surgery of the Hand; Hip = The Hip Society; MSTS = Musculoskeletal Tumor Society; NASS = North American Spine Society; POSNA = Pediatric Orthopaedic Society of North America; SOMOS = Society of Military Orthopaedic Surgeons; AAHS = American Association for Hand Surgery; JRGOS = J. Robert Gladden Orthopaedic Society; Knee = The Knee Society; LRRS = Limb Lengthening and Reconstruction Society; OTA = Orthopaedic Trauma Association.
To provide further context for our finding that women received 8% (61 of 794) of awards, we display this alongside recent physician workforce data, showing that women were 13% of full-time MD orthopaedic department faculty members in 2015, and 5% of practicing orthopaedic surgeons overall in 2018 (Fig. 2) [2, 3].
Fig. 2.
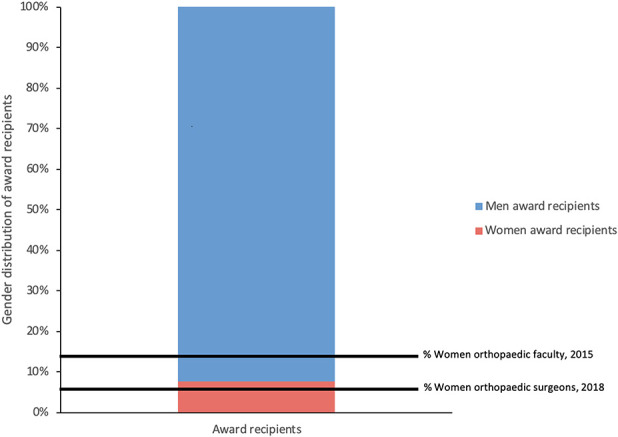
This graph shows orthopaedic award recipients from 2000 to 2018 compared with the academic orthopaedic workforce [3] and general orthopaedic workforce [2].
Considering historic data across all societies from 1973 to 2018, women received 6% (64 of 1018) of all awards (Fig. 3). Three of the 18 societies never granted an award to a woman during the entire study period.
Fig. 3.

This graph shows the names of all orthopaedic awards and the gender of award recipients from 1973 to 2018; AAHKS = American Association of Hip and Knee Surgeons; AAHS = American Association for Hand Surgery; AANA = Arthroscopy Association of North America; AAOS = American Academy of Orthopaedic Surgeons; AOA = American Orthopaedic Association; AOFAS = Association of Foot and Ankle Surgeons; AOSSM = Association Orthopaedic Society for Sports Medicine; ASES = American Shoulder and Elbow Surgeons; ASSH = American Society for Surgery of the Hand; Hip = The Hip Society; JRGOS = J. Robert Gladden Orthopaedic Society; Knee = The Knee Society; LRRS = Limb Lengthening and Reconstruction Society; MSTS = Musculoskeletal Tumor Society; NASS = North American Spine Society; OTA = Orthopaedic Trauma Association; POSNA = Pediatric Orthopaedic Society of North America; SOMOS = Society of Military Orthopaedic Surgeons.
Representation of Women in Various Award Categories
Women were not represented proportionally across award categories. From 2000 to 2018, women received 2% (7 of 300 awards) of leadership awards, 3% (1 of 39) of humanitarianism awards, 22% (4 of 18) of diversity awards, 9% (6 of 67 of education awards), 12% (33 of 278 of scientific investigation awards), and 11% (10 of 92) of resident/fellow scientific investigation awards (Fig. 4). Women were more likely to receive a diversity award than a leadership award (OR 12.0 [95% CI 3.1 to 45.7]; p < 0.001) and also were more likely to receive an education award than a leadership award (OR 4.1 [95% CI 1.3 to 12.7]).
Fig. 4.

This graph shows the proportion of orthopaedic award recipients by gender for each award type from 2000 to 2018. aOf note, there were less than 25 award recipients in the “Diversity” award category; data with a denominator of less than 25 may be too small to be accurately described as a proportion.
From 1973 to 2018, 17 of the 22 leadership awards offered by societies have never been granted to a woman.
Blinding of Awards Processes and Genders of Recipients
Women were more likely to receive awards bestowed through a blinded process than through an unblinded process. From 2000 to 2018, women earned 11% (30 of 285) of awards bestowed through a blinded award process and 6% (31 of 509) of awards bestowed through an unblinded award process (OR 1.8 [95% CI 1.1 to 3.1]; p = 0.03).
Discussion
Awards recognize achievements that are valued by a society, provide visibility to recipients, and have been described as proxies for institutional support from academic societies [21]. As such, they can function as measures of inclusion and support in surgical societies. When considering awards as proxies for institutional support, it is important to be particularly mindful of awards and award categories that show zero or nearly-zero representation of women. This “inexorable zero” has been described as “a telling symptom of hidden attitudes or hiring practices that work to exclude women or minorities from whole categories of jobs” [11]. For example, in our study, all named awards are named after men. Seventeen of 22 leadership awards have never been granted to a woman, and three societies have never granted an award to a woman in their history. Such “zero representation” situations should be assessed to understand the factors that may be barriers to inclusion. For instance, a highly prestigious award in our dataset was previously named “The Mr. [orthopaedic subspecialty] Award.” Based on the name itself, this award was inherently exclusionary. This has been changed such that the award is now named after a specific man; however, the historical name is still listed on the society website, and this award has never been granted to a woman. In this situation, more subtle exclusionary forces, such as the society's cultural perception of that award, may be a persistent barrier to women receiving it. Addressing these “inexorable zeros” represents an opportunity to improve support for women orthopaedic surgeons and encourage societies to think about awarding practices through an equity lens. Awards are important not only for personal recognition but also for career advancement because they can contribute to academic promotion and other professional opportunities. In these respects, awards can be a powerful tool for supporting recipients. Given the importance of awards in academia and the lack of prior studies investigating orthopaedic society awarding practices, we aimed to evaluate the gender distribution of orthopaedic society awards.
Limitations
This study has several limitations. First, because historical membership demographics for each society were not recorded, our study compares awardee data from 2000 to 2018 to each society’s 2018 membership. We recognize that a society’s gender distribution may have changed over this time; however, with the records available, this was the most detailed and accurate comparison possible. In addition, given the relative stability of gender demographics in orthopaedics, this approximation would likely not generate substantial inaccuracy or alter the conclusions of the study.
As members are the often the population of people who are “eligible” for society awards, society-level comparisons allow us to account for intersociety differences in the demographics of membership pools. Additionally, societies provided aggregate membership data for members of all categories, so their reported demographic data may include society members who are not orthopaedic surgeons. In order to illustrate our data outside of the society-specific context, we compared aggregate awardee data to national orthopaedic workforce data, which is consistent with prior studies of awards in medical specialties (Fig. 2) [19, 20].
Second, we do not have information on how many women applied for or were nominated for these awards, which leaves us unable to determine whether the source of underrepresentation is due to the application and nomination process or the selection process. We recommend that societies internally monitor these two components of the awarding process and intervene if there is inequity in either one. Additionally, we were interested in examining if societies that had diversity task forces, diversity programming, or diversity in their mission statement had more equitable awarding practices. However, we were unable to study this variable without information about when these statements and/or programs were implemented. Tracking the relationship between the implementation of society diversity efforts and awardee demographics could be an important outcome measure for societies to internally measure the effectiveness of diversity programming and messaging.
Finally, our study is limited by our use of gender as the only diversity variable, without discussion of intersectionality or other underrepresented populations. Diversity solely defined by gender is inadequate and does not capture the impact of other identities such as race, sexual orientation, and gender identity beyond a men/women binary.
Representation of Women Among Award Recipients
In all but two societies, women awardees were proportionately represented when compared with society membership. The proportion of women awardees is similar to the current proportion of women practicing in orthopaedics (5%); however, it is lower than the proportion of women in academic orthopaedics (13%) [2, 3]. Physicians in academic practice contexts are best poised to earn society awards because of an increased emphasis on research, education, and scholarship. In addition, awards may be more important for promotion in academic medicine than in private practice; thus, academic physicians may be more incentivized to apply for awards. When awards are compared with the gender distribution of academic orthopaedic surgeons, women are underrepresented in all award categories except for diversity. This finding has important implications for academic promotion and advancement and may contribute to the paucity of women in upper-level academic positions and the leaky pipeline phenomenon in academic orthopaedics. When Silver et al. [18–21] studied the gender diversity of awardees in several medical societies, they similarly found that women were underrepresented as award recipients when compared with the current proportion of women in academia in these fields. Collectively, these findings raise concern that women in academia are underrepresented as award recipients in several medical fields, including orthopaedics.
Although society awards are inherently important for visibility, they also serve as a surrogate for inclusion, which could not be measured within the scope of this study. In situations where women are minimally represented as society members and as award recipients, this representation is still deemed “proportional.” As such, having “proportional representation” in awards does not preclude the possibility of exclusion on the level of society membership. Exclusion often occurs unknowingly or indirectly. For example, women may be less likely to be sponsored for membership or be less likely to apply for membership if other women are not visible as members or valued as award recipients. Thus, achieving proportional representation may superficially meet diversity objectives while falling short of the larger goal, which is inclusion [16]. We encourage all societies to strive for inclusion: The state in which individuals from all backgrounds feel welcome and valued in an organization.
Representation of Women in Various Award Categories
The odds of a woman receiving a leadership award were lower than the odds of a woman winning an award in other categories, such as diversity awards or education awards. This discrepancy may result from decreased access to leadership opportunities, decreased recognition of leadership duties performed, or both. Leadership awards are the most common, and arguably the most meaningful, type of recognition bestowed by societies because they reflect the overall characteristics and accomplishments that a group values. Meta-analyses show that leadership stereotypes tend to be culturally masculine, as illustrated by the paradigm “think manager [or leader], think male” [13]. Additionally, both men and women tend to equate strong leadership with attributes typically ascribed to men, such as assertiveness [23]. These examples illustrate how implicit biases can affect our view of who is and is not a leader. To dismantle gendered schemas of leadership, everyone involved in awarding processes needs to be cognizant of their own implicit biases. On a systematic level, forming diverse review committees, implementing implicit bias training for award committee members, and creating standardized criteria for assessing nominees may help to reduce bias in awarding practices [12].
Blinding of Awards Processes and Genders of Recipients
We found that women were more likely to receive awards bestowed through blinded processes. Although to our knowledge, this has not been reported before in orthopaedics, the implications of audition and application blinding have been thoroughly studied in other fields and offer important context for our finding. For example, in a classic study of orchestra auditions, women were 50% more likely to pass preliminary selection rounds if the audition was blinded [10]. In a study of racial bias in hiring decisions, applicants with names that the authors characterized as stereotypically “black” were approximately 50% less likely to receive a call back for an interview compared to applicants with names characterized as stereotypically “white,” despite the resumes being identical [8]. Similarly in academia, in a study of identical curricula vitae (CVs), CVs with men’s names were evaluated as “hirable” more often than CVs with women’s names [22]. These findings collectively show the impact of implicit bias in selection decisions. In this context, our observation that women were more likely to receive blinded awards raises concern that implicit bias may exist in orthopaedic surgery awarding practices. We urge orthopaedic societies to examine their awarding processes for possible sources of bias and to create more equitable processes. Possible interventions are similar to those we suggested earlier, and include forming diverse review committees, implicit bias training, and adhering to standardized criteria for assessing qualifications [12].
Conclusion
We observed that overall, women orthopaedic society members are proportionately represented as award recipients. However, women were less likely to receive awards in certain categories, such as leadership, and were more likely to receive blinded as opposed to unblinded awards, raising concern about implicit bias. To create change, we encourage societies to collect and monitor the demographic information of their award recipients to promote accountability and data transparency. We also encourage societies to consider the diversity of their award selection committees, as well as establish and adhere to nonbiased criteria for award determination [12]. Additionally, societies should intentionally examine the inclusivity of their award descriptions and application criteria. Future research could examine the effectiveness of bias reducing interventions on the subsequent diversity of award recipients. With attuned selection committees, layers of accountability, and an increased focus on diversity and inclusion, society awards can more equitably recognize the accomplishments of orthopaedic surgeons.
Acknowledgments
We thank all of the orthopaedic societies who contributed data to this study. We also thank Taylor Cogsil BA, and Dongyeon J. Kim BA, for their assistance in coding the gender of society members.
Footnotes
Each author certifies that neither he nor she, nor any members of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution waived approval for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.American Academy of Orthopaedic Surgeons. Board of Specialty Societies. 2019. Available at: https://www.aaos.org/about/governance-overview/board-of-specialty-societies/. Accessed August 12, 2019.
- 2.Association of American Medical Colleges. Active Physicians by Sex and Specialty, 2017. Available at: https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-sex-and-specialty-2017. Accessed April 28, 2020.
- 3.Association of American Medical Colleges. Table 4A: Distribution of Full-Time Women MD Faculty by Department and Rank, 2015. Available at: https://www.aamc.org/system/files/reports/1/2015table4a.pdf. Accessed April 26, 2020.
- 4.Association of American Medical Colleges. Active Physicians by Sex and Specialty, 2007. Available at: https://www.aamc.org/system/files/2019-08/2008-physician-specialty-data.pdf. Accessed April 28, 2020.
- 5.Association of American Medical Colleges. Distribution of Full-Time Faculty by Department, Rank, and Gender, 2015. Available at: https://www.aamc.org/download/481182/data/2015table3.pdf. Accessed April 22, 2018.
- 6.Association of American Medical Colleges. ACGME Residents and Fellows by Sex and Specialty, 2017. Available at: https://www.aamc.org/data-reports/workforce/interactive-data/acgme-residents-and-fellows-sex-and-specialty-2017. Accessed December 12, 2019.
- 7.Association of American Medical Colleges. U.S. Medical School Faculty by Sex, Rank, and Department, 2018. Available at: https://www.aamc.org/system/files/2020-01/2018Table13.pdf. Accessed February 22, 2020.
- 8.Bertrand M, Mullainathan S. Are Emily and Greg More Employable Than Lakisha and Jamal? A Field Experiment on Labor Market Discrimination. Am Econ Rev . 2004;94:991–1013. [Google Scholar]
- 9.Cicchetti D V., Sparrow SA. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am J Ment Defic . 1981;86:127–137. [PubMed] [Google Scholar]
- 10.Goldin C, Rouse C. Orchestrating Impartiality: The Impact of “Blind” Auditions on Female Musicians. American Economic Review. 2000;90:715-741. [Google Scholar]
- 11.Huang BI. The " Inexorable Zero " Harvard Law Review. 2004; 117:1215-1235. [Google Scholar]
- 12.Isaac C, Lee B, Carnes M. Interventions that affect gender bias in hiring: A systematic review. Acad Med . 2009;84:1440–1446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Koenig AM, Eagly AH, Mitchell AA, Ristikari T. Are leader stereotypes masculine? A meta-analysis of three research paradigms. Psychol Bull . 2011;137:616–642. [DOI] [PubMed] [Google Scholar]
- 14.Lincoln AE, Pincus S, Koster JB, Leboy PS. The Matilda Effect in science: Awards and prizes in the US, 1990s and 2000s. Soc Stud.Sci. 2012;42:307–320. [DOI] [PubMed] [Google Scholar]
- 15.Comparison MedCalc. of proportions calculator. Available at: https://www.medcalc.org/calc/comparison_of_proportions.php. Accessed April 1, 2020.
- 16.Roberson QM. Disentangling the Meanings of Diversity and Inclusion in Organizations. Gr Organ Manag . 2006;31:212–236. Available at: http://journals.sagepub.com/doi/10.1177/1059601104273064. Accessed April 28, 2020. [Google Scholar]
- 17.Sexton KW, Hocking KM, Wise E, Osgood MJ, Cheung-Flynn J, Komalavilas P, Campbell KE, Dattilo JB, Brophy CM. Women in Academic Surgery: The Pipeline Is Busted. J Surg Educ . 2012;69:84–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Silver JK, Bank AM, Slocum CS, Blauwet CA, Bhatnagar S, Poorman JA, Goldstein R, Reilly JM, Zafonte RD. Women physicians underrepresented in American Academy of Neurology recognition awards. Neurology. 2018;91:e603–e614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Silver JK, Bhatnagar S, Blauwet CA, Zafonte RD, Mazwi NL, Slocum CS, Schneider JC, Tenforde AS. Female Physicians Are Underrepresented in Recognition Awards from the American Academy of Physical Medicine and Rehabilitation. PM R; 2017. [DOI] [PubMed] [Google Scholar]
- 20.Silver JK, Blauwet CA, Bhatnagar S, Slocum CS, Tenforde AS, Schneider JC, Zafonte RD, Goldstein R, Gallegos-Kearin V, Reilly JM, Mazwi NL. Women Physicians Are Underrepresented in Recognition Awards from the Association of Academic Physiatrists. Am J Phys Med Rehabil . 2018;97:34–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Silver JK, Slocum CS, Bank AM, Bhatnagar S, Blauwet CA, Poorman JA, Villablanca A, Parangi S. Where Are the Women? The Underrepresentation of Women Physicians Among Recognition Award Recipients From Medical Specialty Societies. PM R. 2017;9:804–815. [DOI] [PubMed] [Google Scholar]
- 22.Steinpreis R, Anders K, Ritzke D. The Impact of Gender on the Review of the Curricula Vitae of Job Applicants and Tenure Candidates: A National Empirical Study. Sex Roles. 1999;41. [Google Scholar]
- 23.Vial AC, Napier JL. Unnecessary frills: Communality as a nice (but expendable) trait in leaders. Front Psychol . 2018;9:1866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Washington University School of Medicine Washington University School of Medicine Appointments & Promotions Guidelines and Requirements. 2014. Available at: https://biochem.wustl.edu/data/pdfs/forms_info/APGAR.pdf. Accessed September 29, 2018.