

Supplemental Digital Content is available in the text.
Purpose
The aim of this scoping review is to understand the motivations for the creation of global medical curricula, summarize methods that have been used to create these curricula, and understand the perceived premises for the creation of these curricula.
Method
In 2018, the authors used a comprehensive search strategy to identify papers on existing efforts to create global medical curricula published from 1998 to March 29, 2018, in the following databases: MEDLINE; MEDLINE Epub Ahead of Print, In-Process, and Other Non-Indexed Citations; Embase; Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; PsycINFO; CINAHL; ERIC; Scopus; African Index Medicus; and LILACS. There were no language restrictions. Two independent researchers applied the inclusion and exclusion criteria. Demographic data were abstracted from publications and summarized. The stated purposes, methods used for the development, stated motivations, and reported challenges of curricula were coded.
Results
Of the 18,684 publications initially identified, 137 met inclusion criteria. The most common stated purposes for creating curricula were to define speciality-specific standards (50, 30%), to harmonize training standards (38, 23%), and to improve the quality or safety of training (31, 19%). The most common challenges were intercountry variation (including differences in health care systems, the operationalization of medical training, and sociocultural differences; 27, 20%), curricular implementation (20, 15%), and the need for a multistakeholder approach (6, 4%). Most curricula were developed by a social group (e.g., committee; 30, 45%) or Delphi or modified Delphi process (22, 33%).
Conclusions
The challenges of intercountry variation, the need for a multistakeholder approach, and curricular implementation need to be considered if concerns about curricular relevance are to be addressed. These challenges undoubtedly impact the uptake of global medical curricula and can only be addressed by explicit efforts to make curricula applicable to the realities of diverse health care settings.
Medical education is faced with mounting calls to develop global curricula for training.1,2 These calls run in parallel with overall globalization developments in the field of health care, including an increasing number of pandemics, the rise of noncommunicable diseases, and increased focus on the social determinants of health.3 However, the real-world implications of global medical curricula—for example, local applicability, implementation, and impact—are not well understood.4 Further, the influence of such curricula on reproducing the dominance of the Western biomedical model is a concern to scholars following the loss of Indigenous and context-specific health practices.5,6 In addition, the fit of these curricula within the local medical health care system is a potential challenge given the diversity of health care globally. This is important to understand as outdated or ill-suited curricula can lead to gaps in clinical care.7
The calls for global standards in medical education, including curricula, originate from influential educational entities such as the World Federation for Medical Education (WFME) and the World Health Organization’s Institute for International Medical Education (IIME). The WFME, founded in 1972, is an international body that aims to promote quality improvement in medical education and has a current focus on accreditation and maintaining the World Directory of Medical Schools.1 The WFME has developed and disseminated standards along the continuum of medical education from undergraduate to continuing medical education.8 The WFME also provides a curriculum development framework that can be modified locally. The IIME, founded in 1999, has the goal of developing global minimal essential requirements for physicians around the world.2
At a regional level, Europe has several initiatives to harmonize higher education training standards, including the Bologna Process9 and the European Credit Transfer and Accumulation System (ECTS). The ECTS addresses training in all higher education disciplines and aims to facilitate the recognition of the training done in each individual country in Europe across the whole of Europe so as to promote quality training and the free movement of people.10 However, the ECTS does not specify certain curricular requirements. Specific to medical education, there is the European Union of Medical Specialists (UEMS), which represents over 50 medical disciplines and 37 countries in Europe. The mission of the UEMS is to “[set] standards for high quality healthcare practice that are transmitted to the Authorities and Institutions of the [European Union] and the National Medical Associations stimulating and encouraging them to implement its recommendations.”11 Collectively, these internationally recognized organizations in education (WFME, IIME, and UEMS) have, over the past 2 decades, made efforts to accomplish their goal of identifying global standards in medical education, including producing global curricula.
The impetus for creating global curricula in medical education is multifactorial. They are purported to have benefits, including improving the quality of training, promoting individual freedoms by allowing for the free movement of people, and mitigating gaps in the health workforce.12 However, the development of curricular content is a social process that involves individuals with diverse values, histories, cultures, and varying levels of power.13 While there are many reasons to embark on the creation and revision of medical curricula, the most persuasive argument is often providing better education and by extension better patient care. It has also been proposed that curriculum development and renewal can be an opportunity for building strategic networks and bringing people and ideas together.13 This type of social networking is appealing if it promotes the sharing and integration of knowledge and technologies from different sectors and is a source of positive growth for all parties. However, proposing curricular solutions to address global challenges in medical education is mired in power dynamics and requires reflection and humility14 given the diversity of perspectives and local contexts represented in such discussions. Global medical curricula are vulnerable to being overly specific in their articulation of requirements, akin to a shopping list of competencies, which can dampen aspirations for innovation and excellence.15 In addition, global medical curricula may lack a critical understanding of local cultural and/or historical norms, which are critical to the delivery of health care and therefore to medical training.14
In a previous publication, we identified a preponderance of Western authors in the field of global oncology curricula, suggesting the dominance of the Western perspective in global medical curricula in this discipline.16 It is not known if the dominance of the Western perspective is occurring in global medical curricula in other disciplines outside of oncology. Understanding the stated purposes and stakeholder voices represented in the construction of existing global medical curricula may yield insights into strengths and gaps to inform future curricular efforts of this kind. Therefore, the aim of this scoping review is to understand the stated purposes for, motivations for, and challenges in the creation of global curricula; to summarize the methods that have been used to create these curricula; and to understand the perceived premises for the creation of these curricula. We also aim to consider how the stated purposes for global medical curricula are aligned with the methods used to create them, including considering the different sociopolitical voices of those who participated in the development of the curricula.
Method
We conducted a scoping review to understand and summarize existing efforts to create global medical curricula using the 5-step methodology of Arksey and O’Malley.17 We selected a scoping review methodology as it would allow a systematic mapping of the existing work in global medical curricula (including the articulation of trends), facilitate comparisons among curricula, and identify gaps in curricula.18 The research team, including an information specialist (R.F.), constructed a comprehensive search strategy that was peer-reviewed by additional information specialists before beginning the search. See Supplemental Digital Appendix 1 (at http://links.lww.com/ACADMED/A893) for the final search strategy. The following databases were searched to identify relevant papers published between 1998 and March 29, 2018: MEDLINE; MEDLINE Epub Ahead of Print, In-Process, and Other Non-Indexed Citations; Embase; Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; PsycINFO; CINAHL; ERIC; Scopus; African Index Medicus; and LILACS (results given in Spanish). Where available, both medial subject headings (MeSH) and keywords were used to maximize search results and account for global linguistic variations. The search terms included facult*, educat*, graduat*, postgraduat*, residen*, fellow*, or clerkship* for medical education; curricul*, program*, train*, core*, or standard* for curriculum; and global*, universal*, multinational*, or worldwide* for global. There were no language restrictions. The time span of 1998–2018 was selected based on a previous study16 in which it was found that there was a proliferation of global medical curricula efforts in the last 20 years.
Inclusion and exclusion criteria and selection process
Inclusion and exclusion criteria were applied by 2 independent researchers (M.G. and M.B.). We resolved any disagreements through discussion by the 2 researchers until a consensus regarding inclusion or exclusion was reached. We included publications if they were peer-reviewed, focused on physicians and related to any phase of medical education (e.g., undergraduate, postgraduate, continuing medical education), and if they contained a global or regional (> 1 country) curricula or discussed the concept of global, regional, or core curricula. Publications were excluded if they were intended for nonphysician professions, focused on patient or caregiver education, were curricula on global health, were surveys of practice, or were on the topic of international medical graduates (IMGs).
We first screened all publications for inclusion by their title and then reviewed their abstracts. Finally, we reviewed the full text of all remaining publications.
Data abstraction and analysis
The following data were extracted by M.G. and M.B. from each publication: publication year, publication language, medical specialty that was the topic or focus of the publication, phase of medical training referred to in the publication (e.g., postgraduate), number of authors on the publication, and the countries (which were used to determine geographic regions) of the authors on the publication. If present in the publications, the stated purposes for creating global medical curricula were recorded. For this analysis, purpose was defined as an explicit statement in the publication regarding the reason for creating the global medical curricula. For publications that were actual curricular documents, the methods used to develop the curricula were also recorded. Descriptive statistics were used to summarize these demographic data.
As part of our analysis, we also sought to understand if there was transmission of Western ideologies through the development and implementation of global medical curricula. To do this, the current scoping review builds on our previous research.16 That is, in past work, we found that exploring the methods taken in the development of curricula could yield important information on the power relations between resource-rich and resource-poor countries. Thus, to capture the purposes for and methods used in developing curricula, we coded publications deductively to ascertain the stated purposes and methods used for the development of curricula, as well as the stated motivations (theoretical benefits or driving factors) and reported challenges of curricula. We also coded for geographic area of participating curriculum developers (i.e., the authors). Taken together, the data we coded for allowed us to capture patterns related to power relations at play in the development of the curricula. We believe this type of analysis, currently absent in the literature, will advance current approaches to developing global medical curricula because it makes gaps in representation visible and helps to foreground potential unintended consequences of promoting global curricula.
A subset of articles was initially coded by M.G. The coding approach and structure were reviewed and discussed by most of the authors (M.G., J.F., E.W.D., M.A.M., J.P.) until coding was consolidated into core areas of focus by mutual agreement. The data were then reanalyzed and summarized by M.G. and M.B. The coding was completed using NVivo software, version 11 (QSR International Pty Ltd., Melbourne, Victoria, Australia). Following coding of the entire dataset, the analysis and interpretation of results were refined through multiple research meetings between M.G. and most of the other authors (J.F., E.W.D., M.A.M., J.P.).
Results
The initial search resulted in 18,684 publications (see Figure 1). After the removal of duplicates, title screening, and abstract review, 312 articles remained and underwent full-text review. Of these 312 articles, 137 met inclusion criteria and were included in our analysis.4,9,10,15,19–151
Figure 1.
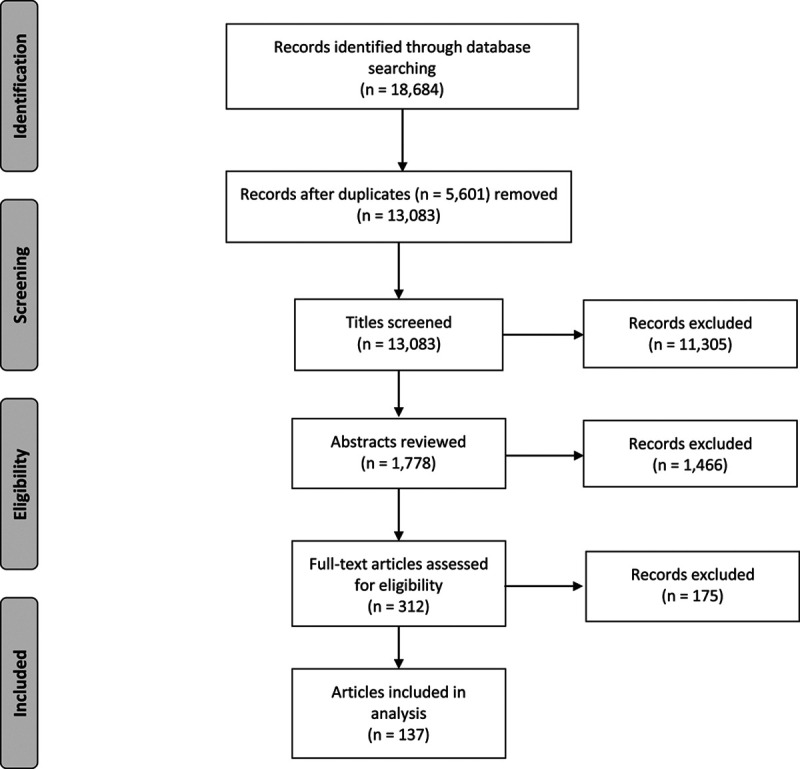
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)165 flow diagram showing the selection process used in a 2018 scoping review aimed at understanding and summarizing existing efforts to create global medical curricula.
Publication demographics
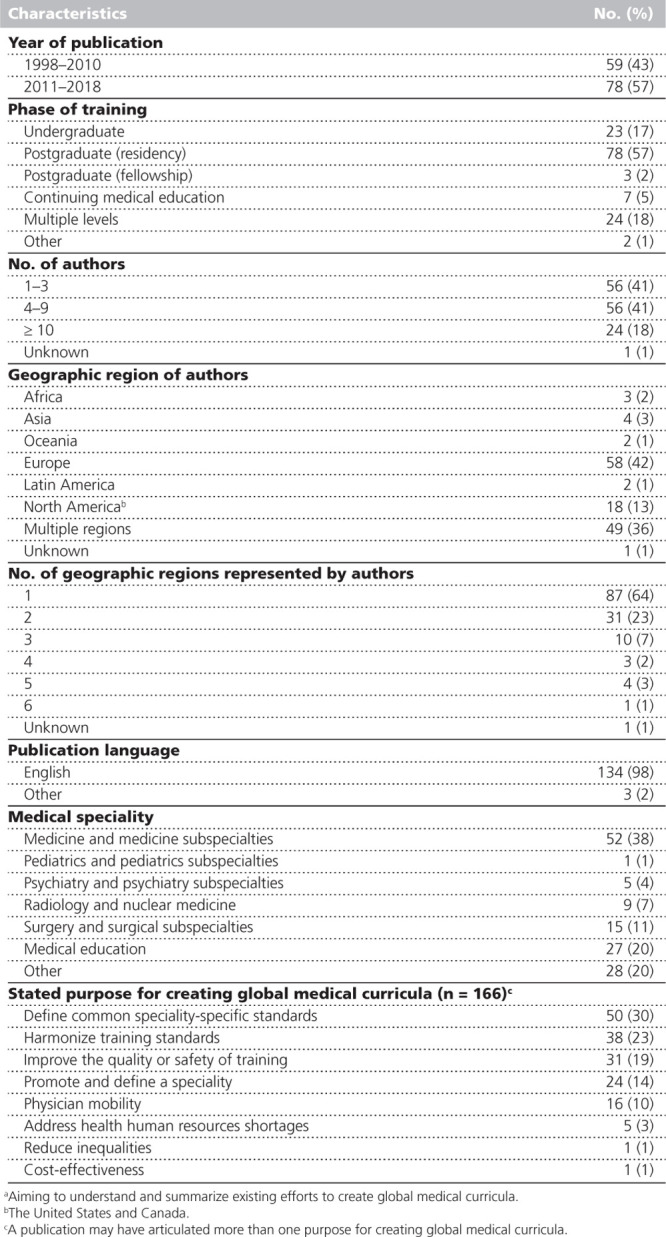
The geographic region of authors was most frequently Europe (58, 42%), followed by North America (the United States and Canada; 18, 13%; see Table 1). Additionally, many publications (49, 36%) had authors from multiple regions. Most articles (134, 98%) were published in English. The mean number of authors on publications was 8 (range = 1–145; data not shown). Seventy-eight (57%) articles were published between 2011 and 2018, and most (81, 59%) were focused on postgraduate medical education (i.e., residency [78, 57%] and fellowship [3, 2%]). Medicine and medicine subspecialties were the most common medical speciality represented, accounting for 52 (38%) publications.
Table 1.
Demographic Characteristics of Included Articles (n = 137) From a 2018 Scoping Reviewa
Stated purposes for global medical curricula
A publication may have articulated more than one purpose for creating global medical curricula. Thus, we identified 166 purpose statements in the 137 publications. The most common explicitly stated purposes for creating global medical curricula were to define common speciality-specific standards (50, 30%), to harmonize training standards (38, 23%), and to improve the quality or safety of training (31, 19%; see Table 1).
Challenges with global medical curricula
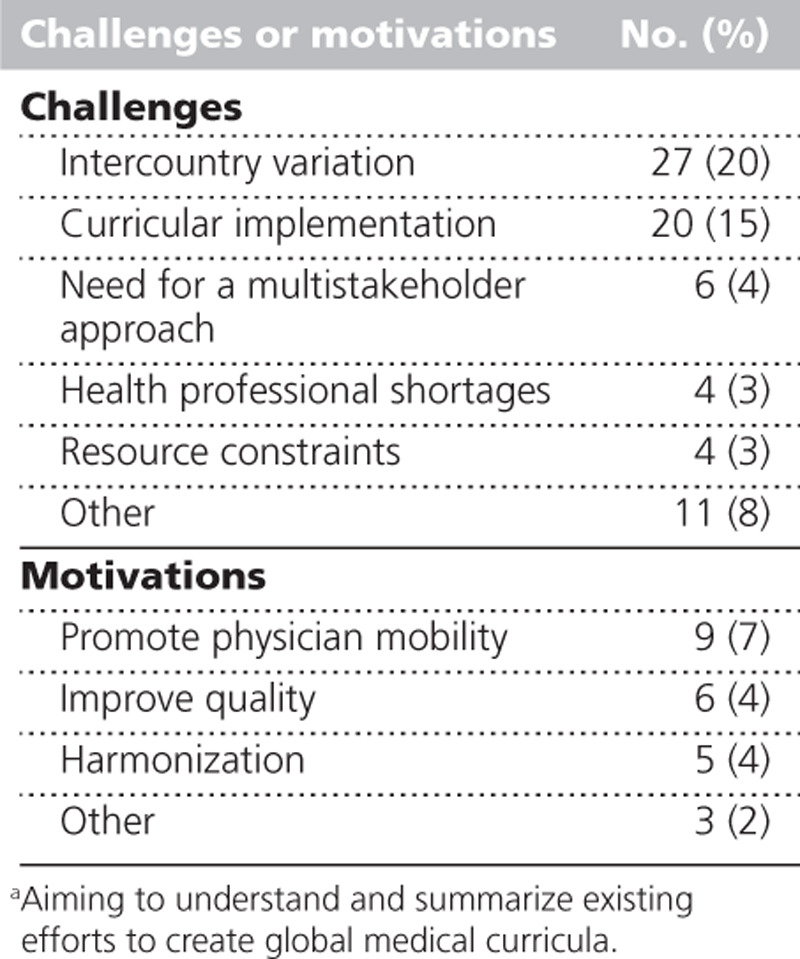
The most common challenges articulated in the publications were intercountry variation (27, 20%), curricular implementation (20, 15%), and the need for a multistakeholder approach (6, 4%; see Table 2). In addition, each publication that discussed curricular implementation as a challenge (20, 15%) also offered recommendations on implementing global medical curricula.
Table 2.
Challenges and Motivations Associated With Global Medical Curricula as Articulated in Included Articles (n = 137) From a 2018 Scoping Reviewa
How intercountry variation impacts global medical curricula was captured in 3 main areas. The first was differences in health care systems. For example, the concept of the link between the content of the curricula and the health system in one document was articulated as “[curricular content] is not only depend[ent] on national traditions, but mainly on the way neurology is practiced and how health system structures are used.”142 The other 2 main areas within intercountry variation were the operationalization of medical training (including the duration of training37) and sociocultural differences (including “widespread cultural and religious diversities and positioning of the doctor within society”85).
Intercountry variation was sometimes presented as a positive and sometimes as a negative challenge. For example, Hodges and colleagues propose “that it is time to study and embrace differences and discontinuities in goals, practices and values that underpin medical competence in different countries”91 (positive challenge), while Khanam and Chowdhury view this as a limitation on achieving uniformity, stating “medical curricul[a] [differ] greatly worldwide in their content, thus, levels of professional competenc[i]es acquired by graduates of medical schools varies across the globe. Consequently, it becomes difficult to get [a] uniform global physician”94 (negative challenge). Finally, intercountry variation and the tension between global and local priorities were identified as factors in the success of global curricula implementation. It was, for example, argued that “development of these training programs is multifaceted and must take into account the specific needs of the recipient country in order to be successful.”72
Among recommendations for implementing global medical curricula, the most frequent recommendation was about the need for local adaptation to facilitate implementation. Authors who have made global medical curricula implementation recommendations have articulated that “flexibility has to be important, otherwise parts of Europe may be unable to offer training”78 in alignment with the proposed curricula and that implementation of “training standards and curricula in local contexts will be best guided by regionally determined policies in regard to some key implementation issues.”129 Similarly, the role of global medical curricula was described as a road map in one article: “A core syllabus should not dictate when or how the content is to be delivered. Its value is simply to provide a helpful roadmap for related educational journeys.”38 Other implementation recommendations included having the appropriate assessment tools to evaluate educational outcomes; the need to address the tension between the priorities of academic institutes and the health care system131; and the need to address barriers to implementation, including financial, political, and cultural barriers (e.g., “initially, the implementation of the project of [a] universal medical curriculum will face lots of cultural, political and sociological difficulties”85). These considerations also apply to the next challenge—the need for a multistakeholder approach.
The need for a multistakeholder approach challenged the dominant paradigm of using a social group or the Delphi or modified Delphi process as the most appropriate methods for developing global medical curricula. However, in this scoping review, the majority of curricula were created using these methods (see below and Table 3). Authors advocating for a multistakeholder approach propose that “expert consensus alone is not the most appropriate way to define the professional competencies required for clinical practice”106 and question whether “[there is] a more accurate way of capturing competency beyond expert consensus.”138 They allude to the need to extend these consultations beyond the expert core to other stakeholders, including those who would be implementing the curricula locally.
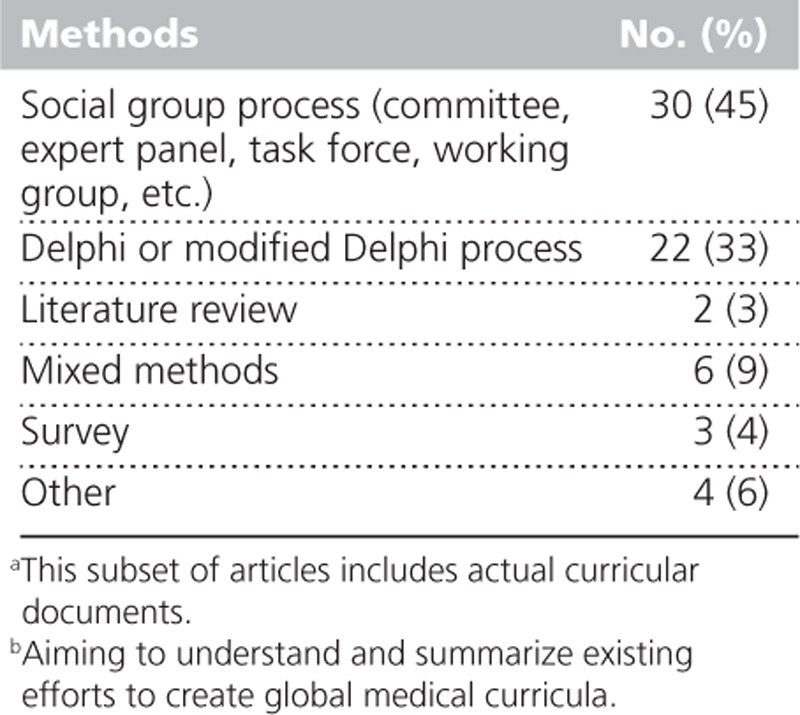
Table 3.
Methods Used for the Creation of Global Medical Curricula From 67a (of 137) Included Articles in a 2018 Scoping Reviewb
Incongruence between Western priorities and local priorities,85,91,122,149 suppression of traditional approaches,91 and reducing diversity91 were also challenges that were identified in the publications. Hodges and colleagues have articulated that “a risk of reduction of diversity and a suppression of traditional knowledge or approaches, by dominant groups or countries …”91 exists and that “while there are quite distinct cultural aspects to medicine, medical education tends to be blind to these differences and act as a ‘culture of no culture.’”91 They also argued for critical reflection during the curriculum design process to determine what perspectives are present in the consensus processes and whether certain competency areas are underrepresented due to this tension between the universal and diversity. Authors have argued that programs should counter Western dominance by “tak[ing] into consideration the socioeconomic and cultural framework of the local community when designing curricula”122 and by being mindful that there may be “incompatible cultural attitudes like individualism, difficulty in getting involved in discussions, and [an] exaggerated tendency to be outspoken in some of their [non-West] students”85 when moving discussions and curricula from Western to non-Western contexts.
Motivations for creating global medical curricula
In addition to the explicitly stated purposes for creating global medical curricula, publications also described theoretical benefits or driving factors for creating global medical curricula, which we coded as motivations.
The most frequently cited motivation behind creating global medical curricula was promoting physician mobility (9, 7%; see Table 2). Authors felt global medical curricula made movement to different areas easier by assisting regulatory bodies in credentialing physicians in different regions, as exemplified in the following excerpt: “The certification or credentialing of vascular and endovascular surgeons who have all achieved the expected competencies agreed to internationally allows regulatory bodies to develop consistent approaches between countries.”76
Improving quality (6, 4%) was the next most frequently cited motivation for creating global medical curricula. The quality narrative focused on the quality of patient care, the quality of the training programs, or the role of quality training in realizing high-quality patient care. For example, Besso and colleagues noted that “harmonizing educational outcomes and strengthening processes of training and accreditation … enhances the quality of care [trainees] provide worldwide.”43 Others described the role of these curricula in “meeting [the] demands of the public for guarantees of graduate competence and cost-effectiveness of their training.”38
Methods for developing global medical curricula
A subset of the 137 publications were actual curricular documents (67, 49%). These 67 publications were analyzed to determine what methods were used for their creation. The most common methods used were a social group process (such as a committee or expert panel; 30, 45%) or a Delphi or modified Delphi process (22, 33%; see Table 3).
Discussion
In this scoping review, we found that the majority of publications on global medical curricula efforts originate from Western geographic regions, namely Europe and North America (the United States and Canada). This is an important finding as a predominance of Western discourse in the literature on global medical curricula may suppress important views from non-Western stakeholders. This, in turn, may limit the utility of these curricula and contribute to an ongoing imbalance between curricular content and health system needs.7 We have described the challenges associated with global medical curricula that were articulated in the included articles, which included intercountry variation, the need for a multistakeholder approach, and curricular implementation.
The usefulness of global medical curricula once they have been implemented has not been assessed.4 It has been recommended that global medical curricula should be developed in consultation and collaboration with those stakeholders who will ultimately implement the curricula. In addition, Bandaranayake states that the need to maintain societal relevance should take precedence over standardization.38 These are significant challenges, and further studies to improve both the understanding of and approach to the development and implementation of global medical curricula are needed. Our findings do suggest an awareness of the need for diversity of input and the importance of engaging the stakeholders who will be implementing the curricula. However, international standards, despite efforts to mitigate this in the planning stage, can still reflect Western standards152 and whether diversifying stakeholder input alone will be enough to mitigate this problem is uncertain. An important example of the concern over Western values driving the standardization movement is articulated in an article on the Educational Commission for Foreign Medical Graduates (ECFMG) policy that states that beginning in 2023, IMGs must have graduated from a formally accredited medical school to receive ECFMG certification.153 As the article notes, this policy has the potential to impact the physician workforce not only in the United States, where they may see a decrease in IMGs, but also in other countries where they may have an increase in IMG applicants as well as in home countries where they may retain a greater number of physicians.153 This also raises concerns about Western accreditation standards and the global–local tensions that arise.154 Could a move to meet these international accreditation standards create a mismatch with local needs? This is of particular concern in countries or regions where clinical practice or the type of technology available are significantly different from clinical practice or the type of technology available in countries or regions that are setting the standards. In addition, it is challenging to demonstrate that international accreditation equates to higher-quality patient care in the United States or in the country in which an individual was training.153
A global approach to medical education is challenging. The process of consensus and standardization may be susceptible to influence by individuals’ conflicts of interest, political pressures, and differences between how educational activities are reported versus how they are actually delivered in a country.155 Our work has elucidated similar concerns with respect to global medical curricula development, namely political and sociocultural challenges. An additional challenge in global approaches to education is that there are regional variations as to what is considered a high priority. For example, humanism in medicine is a growing priority in Western contexts.120 In other regions, moral duties, such as responsibility, receive priority.156 The essential consideration of social, cultural, and health care system factors86 in developing local training content needs to be addressed in global medical curricula.
The main motivation for creating global medical curricula identified in this scoping review was to promote physician mobility. This reflects the discourse on the internationalization of medicine and medical education.157 The internationalization of medicine is a driving factor behind the need for global standards, and physician mobility is a core element of the internationalization of medicine.38 However, while physician mobility may promote individual freedoms, it may also lead to increased maldistribution of health care workers.158 The movement of physicians from low- or middle-income countries to high-income countries can create severe physician shortages and drive declines in the physician-to-population ratio in low- or middle-income countries.10 Mechanisms to accurately monitor and model the global health workforce are challenging but will be integral to determining the impact, positive or negative, of promoting greater physician mobility.
Global medical education standards, such as those articulated by the WFME, emphasize certain priorities, including a foundation in the biomedical sciences, which could perpetuate Western medical priorities.159 In turn, these priorities may be reflected in the global medical curricula identified in this scoping review, as none referred to traditional medicine or engaging traditional healers in care. Instead of focusing on traditional medicine, the social science priorities articulated by the WFME recommend focusing on professionalism, as well as legal and ethical responsibilities,159 and an analysis of humanism in global oncology curricula also identified this emphasis on professionalism.160 Despite the importance of traditional medicine in global contexts,161,162 we were not able to identify content in the existing global medical curricula that addresses traditional medicine, Indigenous health care treatments, or their integration into care in global contexts.
In addition, another point of consideration in the development of global medical curricula is that different areas of the globe have access to widely varying levels of technology. How this is manifest and the degree of impact it has in different specialties is likely variable. Radiation oncology, a subspecialty field of oncology that is heavily reliant on complex technology, provides an illustrative example. In a global radiation oncology curriculum published by the International Atomic Energy Agency (IAEA), the IAEA describes 3 skill levels that range from mandatory (level 1 and 2) to desirable (level 3).163 These levels reflect varying access to technology. However, one questions if there is a preferable approach to addressing variable access to technology in curriculum design. One may argue curricula should be adapted to suit whatever level of technology is available in a given local context, as in the IAEA global radiation oncology curriculum, while others may promote education based on whatever the most state-of-the-art technology is even if there is no local access to it. This latter approach may facilitate the referral of patients to higher-resource settings (e.g., the referral of Canadian cancer patients to the United States for proton beam therapy164) or may give clinicians a foundation for advocating for new resources in their setting. This complex intersection of globalization and technology would benefit from additional study and exploration.
The most common methods used to create the global medical curricula in this study were social group and Delphi processes. These methods are reflective of recommendations in the literature.157 Without data on the success of curricular implementation and the degree of adoption of curricula, however, we cannot provide recommendations as to which methods may produce superior results. Nevertheless, given the recommendations to engage diverse stakeholders in global curriculum development, using mixed methods may be necessary. Only 9% of the actual curricular documents identified in this scoping review applied a mixed methods approach. The limitations of social group and Delphi processes include a reductionist approach and tension between a desire for standardization and valuing diversity.85,105,138 Thus, it is important to be mindful that social group and Delphi processes do not methodologically lend themselves to preserving diversity, particularly if the perspectives medical educators hope to incorporate in global medical curricula are those of minority experts.
This scoping review has several limitations. We were not able to determine the degree to which an increase in multiregional perspectives in the development of global medical curricula would result in real-world improvements in local curricular implementation. Answering this question would be better explored through a qualitative approach. Through analysis of the included publications alone, we could not ascertain each stakeholder’s degree of engagement in the development of these curricula. This is an important limitation as it has been stated that failing to engage those who implement the curricula will result in a failure of the curricula to be applied in practice.38 To address this concern, future studies should include observations of global medical curricula development meetings and stakeholder interviews. In addition, all of the authors of this scoping review have a Western background, and this may have influenced our interpretation of the data. Our findings show that there is a Western–non-Western distinction that is made in the literature; however, this distinction is likely overly simplistic and future research and future global medical curricula development efforts should be more sensitive to the diversity within and across Western and non-Western contexts. We were not able to ascertain a single definition of global or regional with respect to medical curricula in the published literature. As such, with a desire to be comprehensive, we used an inclusive definition of global or regional as > 1 country in this scoping review. While this approach fostered inclusivity, an alternate definition may produce different results. A final consideration, as with all reviews, is that we may not have captured all possible publications on this topic.
Conclusions
Facilitating physician mobility and improving quality were the main motivations articulated for the creation of global medical curricula. However, as this scoping review has revealed, the challenges of intercountry variation, the need for a multistakeholder approach, and curricular implementation need to be considered if medical education is to address concerns about the relevance of these curricula. These challenges undoubtedly impact the uptake of global medical curricula and can only be addressed by explicit efforts to make these curricula applicable to the realities of diverse health care settings.
Acknowledgments:
The authors thank Naa Kwarley Quartey and Eleni Giannopoulos for their assistance in formatting and copy editing the paper.
Supplementary Material
Footnotes
Supplemental digital content for this article is available at http://links.lww.com/ACADMED/A893.
Funding/Support: None reported.
Other disclosures: None reported.
Ethical approval: Reported as not applicable.
References
- 1.World Federation for Medical Education. World Directory of Medical Schools. https://wfme.org/world-directory. Accessed March 10, 2020
- 2.Global Health Workforce Alliance. The Institute for International Medical Education. https://www.who.int/workforcealliance/members_partners/member_list/iime/en. Accessed March 10, 2020
- 3.McMichael AJ. Globalization, climate change, and human health. N Engl J Med. 2013; 368:1335–1343 [DOI] [PubMed] [Google Scholar]
- 4.Patel S, Jagsi R, Cook N, Hughes-Davies L, Parkinson C. The International Core Literature Consensus (ICLC): An alternative curriculum for oncologists. J Cancer Educ. 2011; 26:420–426 [DOI] [PubMed] [Google Scholar]
- 5.Hartzband P, Groopman J. Keeping the patient in the equation—Humanism and health care reform. N Engl J Med. 2009; 361:554–555 [DOI] [PubMed] [Google Scholar]
- 6.Whitehead C. Scientist or science-stuffed? Discourses of science in North American medical education. Med Educ. 2013; 47:26–32 [DOI] [PubMed] [Google Scholar]
- 7.Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. Lancet. 2010; 376:1923–1958 [DOI] [PubMed] [Google Scholar]
- 8.World Federation for Medical Education. About. https://wfme.org/about-wfme. Accessed March 10, 2020
- 9.Patrício M, Harden RM. The Bologna Process—A global vision for the future of medical education. Med Teach. 2010; 32:305–315 [DOI] [PubMed] [Google Scholar]
- 10.Harden RM. International medical education and future directions: A global perspective. Acad Med. 2006; 81(12 suppl):S22–S29 [DOI] [PubMed] [Google Scholar]
- 11.European Union of Medical Specialists. Presentation. https://www.uems.eu/about-us/presentation. Accessed March 10, 2020
- 12.Spring J. Globalization of Education: An Introduction. 2nd edNew York, NY: Routledge; 2014 [Google Scholar]
- 13.Blackmore P, Kandiko CB. Strategic Curriculum Change: Global Trends in Universities. 1st edLondon, UK: Routledge; 2012 [Google Scholar]
- 14.Anderson K, Raza D, Philpott J. Exploring the hidden curriculum of global health. Soc Med. 2014; 8:143–146 [Google Scholar]
- 15.Bion J, Rothen HU. Models for intensive care training. A European perspective. Am J Respir Crit Care Med. 2014; 189:256–262 [DOI] [PubMed] [Google Scholar]
- 16.Giuliani M, Frambach J, Broadhurst M, et al. A critical review of representation in the development of global oncology curricula and the influence of neocolonialism. BMC Med Educ. 2020; 20:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. 2005; 8:19, 32 [Google Scholar]
- 18.Martimianakis MA, Michalec B, Lam J, Cartmill C, Taylor JS, Hafferty FW. Humanism, the hidden curriculum, and educational reform: A scoping review and thematic analysis. Acad Med. 2015; 90(11 suppl):S5, S13 [DOI] [PubMed] [Google Scholar]
- 19.Abdullah F, Troedsson H, Cherian M. The World Health Organization program for emergency surgical, obstetric, and anesthetic care: From Mongolia to the future. Arch Surg. 2011; 146:620–623 [DOI] [PubMed] [Google Scholar]
- 20.Adleman J, Gillan C, Caissie A, et al. Development of a quality and safety competency curriculum for radiation oncology residency: An international Delphi study. Int J Radiat Oncol Biol Phys. 2017; 98:428–437 [DOI] [PubMed] [Google Scholar]
- 21.Afolabi B, Olapade-Olaopa EO. International training in medical education—The FAIMER institute 2002 fellowship experience. Afr J Med Med Sci. 2006; 35:59–67 [PubMed] [Google Scholar]
- 22.Ahmed K, Khan R, Mottrie A, et al. Development of a standardised training curriculum for robotic surgery: A consensus statement from an international multidisciplinary group of experts. BJU Int. 2015; 116:93–101 [DOI] [PubMed] [Google Scholar]
- 23.Ahmed K, Patel S, Aydin A, et al. European Association of Urology Section of Urolithiasis (EULIS) consensus statement on simulation, training, and assessment in urolithiasis. Eur Urol Focus. 2018; 4:614–620 [DOI] [PubMed] [Google Scholar]
- 24.Alahuhta S, Mellin-Olsen J, Blunnie WP, Knape JT; Section and Board of Anaesthesiology, European Union of Medical Specialists. Charter on continuing medical education/continuing professional development approved by the UEMS Specialist Section and European Board of Anaesthesiology. Eur J Anaesthesiol. 2007; 24:483–485 [DOI] [PubMed] [Google Scholar]
- 25.Almeida MJ. Perspective on South America: The Latin American contribution to the world movement in medical education. Med Educ. 2001; 35:796–799 [DOI] [PubMed] [Google Scholar]
- 26.Amor B. What competence does a rheumatologist need?: An international perspective. Ann Rheum Dis. 2000; 59:580–582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.European Union of Medical Specialists. Chapter 6, Charter on training of medical specialists in the EU. Requirements for specialty radiotherapy. Radiother Oncol. 2004; 70:115–116 [DOI] [PubMed] [Google Scholar]
- 28.Antonaci F, Láinez JM, Diener HC, et al. ; European Headache Federation. Guidelines for the organization of headache education in Europe: The headache school. Funct Neurol. 2005; 20:89–93 [PubMed] [Google Scholar]
- 29.Arafat R, Askitopoulou H, Della Corte F, Jakubaszko J, Sabbe M. Core curriculum in emergency medicine. Eur J Anaesthesiol. 2008; 25:690–691 [DOI] [PubMed] [Google Scholar]
- 30.Are C, Berman RS, Wyld L, Cummings C, Lecoq C, Audisio RA. Global curriculum in surgical oncology. Ann Surg Oncol. 2016; 23:1782–1795 [DOI] [PubMed] [Google Scholar]
- 31.Are C, Yanala U, Malhotra G, et al. Global curriculum in research literacy for the surgical oncologist. Ann Surg Oncol. 2018; 25:604–616 [DOI] [PubMed] [Google Scholar]
- 32.Artigas A, Pelosi P, Dellweg D, et al. ; ERS Educational Task Force on Respiratory Critical Care HERMES. Respiratory critical care HERMES syllabus: Defining competencies for respiratory doctors. Eur Respir J. 2012; 39:1294–1297 [DOI] [PubMed] [Google Scholar]
- 33.Artigas A, Vassilakopoulos T, Brochard L, et al. Respiratory critical care HERMES: A European core syllabus in respiratory critical care medicine. Breathe. 2012; 8:216–229 [Google Scholar]
- 34.Avgerinos ED, Koupidis SA, Filippou DK. Impact of the European Union enlargement on health professionals and health care systems. Health Policy. 2004; 69:403–408 [DOI] [PubMed] [Google Scholar]
- 35.Ayu AP, El-Guebaly N, Schellekens A, et al. Core addiction medicine competencies for doctors: An international consultation on training. Subst Abus. 2017; 38:483–487 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bachmann C, Abramovitch H, Barbu CG, et al. A European consensus on learning objectives for a core communication curriculum in health care professions. Patient Educ Couns. 2013; 93:18–26 [DOI] [PubMed] [Google Scholar]
- 37.Balch CM, Poston GJ. Training a new generation of surgical oncologists worldwide. Lancet Oncol. 2016; 17:700–701 [DOI] [PubMed] [Google Scholar]
- 38.Bandaranayake R. The concept and practicability of a core curriculum in basic medical education. Med Teach. 2000; 22:560–563 [DOI] [PubMed] [Google Scholar]
- 39.Bayram J, Rosborough S, Bartels S, et al. Core curricular elements for fellowship training in international emergency medicine. Acad Emerg Med. 2010; 17:748–757 [DOI] [PubMed] [Google Scholar]
- 40.Bellou A, Conroy SP, Graham CA. The European curriculum for geriatric emergency medicine. Eur J Emerg Med. 2016; 23:239. [DOI] [PubMed] [Google Scholar]
- 41.Berberat PO, de Wit NJ, Bockhorn M, Lundell L, Drenth JP. Training innovations in gastroenterology and educational resources: A new vision of gastrointestinal education across Europe. Eur J Gastroenterol Hepatol. 2010; 22:1393–1396 [DOI] [PubMed] [Google Scholar]
- 42.Berman AC. Anatomy of curriculum: Digging to the core. Anat Sci Educ. 2014; 7:326–328 [DOI] [PubMed] [Google Scholar]
- 43.Besso J, Bhagwanjee S, Takezawa J, Prayag S, Moreno R. A global view of education and training in critical care medicine. Crit Care Clin. 2006; 22:539–46, x [DOI] [PubMed] [Google Scholar]
- 44.CoBaTrICE Collaboration. International standards for programmes of training in intensive care medicine in Europe. Intensive Care Med. 2011; 37:385–393 [DOI] [PubMed] [Google Scholar]
- 45.Bode CO, Nwawolo CC, Giwa-Osagie OF. Surgical education at the West African College of Surgeons. World J Surg. 2008; 32:2162–2166 [DOI] [PubMed] [Google Scholar]
- 46.Bolon B, Barale-Thomas E, Bradley A, et al. International recommendations for training future toxicologic pathologists participating in regulatory-type, nonclinical toxicity studies. J Toxicol Pathol. 2010; 23:171–181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Breipohl W, Johansson C, Hansis M, et al. Undergraduate medical education: Tendencies and requirements in a rapidly developing Europe. Folia Med (Plovdiv). 2000; 42:5–16 [PubMed] [Google Scholar]
- 48.Brinkman DJ, Tichelaar J, Schutte T, et al. ; Working Group Research on CPT Education of the European Association for Clinical Pharmacology and Therapeutics (EACPT). Essential competencies in prescribing: A first European cross-sectional study among 895 final-year medical students. Clin Pharmacol Ther. 2017; 101:281–289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Brunelli A, Falcoz PE, D’Amico T, et al. European guidelines on structure and qualification of general thoracic surgery. Eur J Cardiothorac Surg. 2014; 45:779–786 [DOI] [PubMed] [Google Scholar]
- 50.Bundred P, Gibbs T. Medical migration and Africa: An unwanted legacy of educational change. Med Teach. 2007; 29:893–896 [DOI] [PubMed] [Google Scholar]
- 51.Burkhardt JK, Zinn PO, Bozinov O, Colen RR, Bertalanffy H, Kasper EM. Neurosurgical education in Europe and the United States of America. Neurosurg Rev. 2010; 33:409–417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Buth J, Harris PL, Maurer PC, Nachbur B, van Urk H. Harmonization of vascular surgical training in Europe. A task for the European Board of Vascular Surgery (EBVS). Cardiovasc Surg. 2000; 8:98–103 [DOI] [PubMed] [Google Scholar]
- 53.Carracedo A, Giardina E, Mosquera-Miguel A, Manzo L, Alvarez-Iglesias V, Schneider PM. Making progress in education: The EUROFORGEN master degree pilot project in forensic genetics. Forensic Sci Int Genet. 2017; 28:e12–e13 [DOI] [PubMed] [Google Scholar]
- 54.Chan MK, de Camps Meschino D, Dath D, et al. Collaborating internationally on physician leadership development: Why now? Leadersh Health Serv (Bradf Engl). 2016; 29:231–239 [DOI] [PubMed] [Google Scholar]
- 55.Chuang LT, Randall TC, Denny L, et al. Sister society meeting on global education development and collaboration: Meeting report. Int J Gynecol Cancer. 2016; 26:1186–1188 [DOI] [PubMed] [Google Scholar]
- 56.Ciottone GR, Old A, Nicholas S, Anderson PD. Implementation of an emergency and disaster medical response training network in the Commonwealth of Independent States. J Emerg Med. 2005; 29:221–229 [DOI] [PubMed] [Google Scholar]
- 57.Cohen H, Saenz R, de Almeida Troncon LE, Lizarzabal M, Olano C. Gastroenterology training in Latin America. World J Gastroenterol. 2011; 17:2283–2287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Copeland C, Fisher J, Teodorczuk A. Development of an international undergraduate curriculum for delirium using a modified delphi process. Age Ageing. 2018; 47:131–137 [DOI] [PubMed] [Google Scholar]
- 59.Institute for International Medical Education Core Committee. Global minimum essential requirements in medical education. Med Teach. 2002; 24:130–135 [DOI] [PubMed] [Google Scholar]
- 60.Costa A, Van Hemelryck F, Aparicio A, et al. Continuing medical education in Europe: Towards a harmonised system. Eur J Cancer. 2010; 46:2340–2343 [DOI] [PubMed] [Google Scholar]
- 61.Cumming A, Ross M. The tuning project for medicine—Learning outcomes for undergraduate medical education in Europe. Med Teach. 2007; 29:636–641 [DOI] [PubMed] [Google Scholar]
- 62.Cuocolo A, Milcinski M, Bischof Delaloy A; European Board of Nuclear Medicine. Syllabus for postgraduate specialisation in nuclear medicine. 2006/07 update. Eur J Nucl Med Mol Imaging. 2009; 36:551–554 [DOI] [PubMed] [Google Scholar]
- 63.Da Silva JA, Faarvang KL, Bandilla K, Woolf AD; UEMS Section and Board of Rheumatology. UEMS charter on the training of rheumatologists in Europe. Ann Rheum Dis. 2008; 67:555–558 [DOI] [PubMed] [Google Scholar]
- 64.Danziger-Isakov L, Allen U, Englund J, et al. ; American Society of Transplantation, Pediatric Infectious Diseases Society, and International Pediatric Transplant Association. Recommended curriculum for training in pediatric transplant infectious diseases. J Pediatric Infect Dis Soc. 2015; 4:4–10 [DOI] [PubMed] [Google Scholar]
- 65.De Korvin G, Delarque A. Physical and rehabilitation medicine section and board of the European Union of Medical Specialists. Community context; history of European medical organizations; actions under way. Ann Phys Rehabil Med. 2009; 52:594–607 [DOI] [PubMed] [Google Scholar]
- 66.De Lange S, Van Aken H, Burchardi H; European Society of Intensive Care Medicine; Multidisciplinary Joint Committee of Intensive Care Medicine of the European Union of Medical Specialists. European Society of Intensive Care Medicine statement: Intensive care medicine in Europe—Structure, organisation and training guidelines of the Multidisciplinary Joint Committee of Intensive Care Medicine (MJCICM) of the European Union of Medical Specialists (UEMS). Intensive Care Med. 2002; 28:1505–1511 [DOI] [PubMed] [Google Scholar]
- 67.De Robertis E, McAdoo J, Pagni R, Knape JT. Core curriculum in emergency medicine integrated in the specialty of anaesthesiology. Eur J Anaesthesiol. 2007; 24:987–990 [DOI] [PubMed] [Google Scholar]
- 68.Dequeker J, Rasker JJ, Woolf AD. Educational issues in rheumatology. Baillieres Best Pract Res Clin Rheumatol. 2000; 14:715–729 [DOI] [PubMed] [Google Scholar]
- 69.Dickenson DL, Parker MJ. The European Biomedical Ethics Practitioner Education Project: An experiential approach to philosophy and ethics in health care education. Med Health Care Philos. 1999; 2:231–237 [DOI] [PubMed] [Google Scholar]
- 70.Dittrich C, Kosty M, Jezdic S, et al. ESMO/ASCO recommendations for a global curriculum in medical oncology edition 2016. ESMO Open. 2016; 1:e000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Dittrich C, Stiefel F, Kiss A, Dizon DS. Reply to the letter to the editor ‘Integrating communication as a core skill in the global curriculum for medical oncology’ by Horlait. et al. Ann Oncol. 2017; 28:905–906 [DOI] [PubMed] [Google Scholar]
- 72.Dubowitz G, Evans FM. Developing a curriculum for anaesthesia training in low- and middle-income countries. Best Pract Res Clin Anaesthesiol. 2012; 26:17–21 [DOI] [PubMed] [Google Scholar]
- 73.Elliott CG, Barst RJ, Seeger W, et al. Worldwide physician education and training in pulmonary hypertension: Pulmonary vascular disease: The global perspective. Chest. 2010; 137(suppl 6):85S–94S [DOI] [PubMed] [Google Scholar]
- 74.Faarvang KL, da Silva JA. Competencies in rheumatology: A European framework. Best Pract Res Clin Rheumatol. 2009; 23:145–160 [DOI] [PubMed] [Google Scholar]
- 75.Fahrer R, Jorge MR, Ruiz P. Addressing psychiatric education in Latin America: Challenges and opportunities. Int Rev Psychiatry. 2010; 22:378–381 [DOI] [PubMed] [Google Scholar]
- 76.Fitridge R, Quigley F, Vicaretti M. Should we develop a core international curriculum for vascular and endovascular surgery? Eur J Vasc Endovasc Surg. 2010; 39(suppl 1):S10–S14 [DOI] [PubMed] [Google Scholar]
- 77.Francis N, Penna M, Mackenzie H, Carter F, Hompes R; International TaTME Educational Collaborative Group. Consensus on structured training curriculum for transanal total mesorectal excision (TaTME). Surg Endosc. 2017; 31:2711–2719 [DOI] [PubMed] [Google Scholar]
- 78.Gappa M, Paton J, Baraldi E, et al. Paediatric HERMES: Update of the European training syllabus for paediatric respiratory medicine. Eur Respir J. 2009; 33:464–465 [DOI] [PubMed] [Google Scholar]
- 79.García de Leonardo C, Ruiz-Moral R, Caballero F, et al. A Latin American, Portuguese and Spanish consensus on a core communication curriculum for undergraduate medical education. BMC Med Educ. 2016; 16:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Garofalo M, Aggarwal R. Competency-based medical education and assessment of training: Review of selected national obstetrics and gynaecology curricula. J Obstet Gynaecol Can. 2017; 39:534–544 [DOI] [PubMed] [Google Scholar]
- 81.Gimelli A, Neglia D, Schindler TH, Cosyns B, Lancellotti P, Kitsiou A. Nuclear cardiology core syllabus of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging. 2015; 16:349–350 [DOI] [PubMed] [Google Scholar]
- 82.Giuliani ME, Gillan C, Milne RA, Uchino M, Millar BA, Catton P. Determining an imaging literacy curriculum for radiation oncologists: An international Delphi study. Int J Radiat Oncol Biol Phys. 2014; 88:961–966 [DOI] [PubMed] [Google Scholar]
- 83.Goligher EC, Ferguson ND, Kenny LP. Core competency in mechanical ventilation: Development of educational objectives using the Delphi technique. Crit Care Med. 2012; 40:2828–2832 [DOI] [PubMed] [Google Scholar]
- 84.Gordon M, Baker P, Catchpole K, Darbyshire D, Schocken D. Devising a consensus definition and framework for non-technical skills in healthcare to support educational design: A modified Delphi study. Med Teach. 2015; 37:572–577 [DOI] [PubMed] [Google Scholar]
- 85.Gukas ID. Global paradigm shift in medical education: Issues of concern for Africa. Med Teach. 2007; 29:887–892 [DOI] [PubMed] [Google Scholar]
- 86.Hamdy H. The problem and goals are global, the solutions are local: Revisiting quality measurements and the role of the private sector in global health professions education. Acad Med. 2017; 92:1082–1085 [DOI] [PubMed] [Google Scholar]
- 87.Hansen HH, Bajorin DF, Muss HB, Purkalne G, Schrijvers D, Stahel R; ESMO/ASCO Task Force on Global Curriculum in Medical Oncology. Recommendations for a global core curriculum in medical oncology. Ann Oncol. 2004; 15:1603–1612 [DOI] [PubMed] [Google Scholar]
- 88.Heidbuchel H, Papadakis M, Panhuyzen-Goedkoop N, et al. ; Sports Cardiology Section of European Association for Cardiovascular Prevention and Rehabilitation (EACPR) of European Society of Cardiology (ESC). Position paper: Proposal for a core curriculum for a European sports cardiology qualification. Eur J Prev Cardiol. 2013; 20:889–903 [DOI] [PubMed] [Google Scholar]
- 89.Heitkamp DE, Johnson KS, Suh RD, et al. Sustaining change in radiology education: The need for universal curricula. J Am Coll Radiol. 2017; 14:804–807 [DOI] [PubMed] [Google Scholar]
- 90.Hobgood C, Anantharaman V, Bandiera G, et al. ; Core Curriculum and Education Committee for the International Federation for Emergency Medicine. International Federation for Emergency Medicine model curriculum for emergency medicine specialists. Emerg Med Australas. 2011; 23:541–553 [DOI] [PubMed] [Google Scholar]
- 91.Hodges BD, Maniate JM, Martimianakis MA, Alsuwaidan M, Segouin C. Cracks and crevices: Globalization discourse and medical education. Med Teach. 2009; 31:910–917 [DOI] [PubMed] [Google Scholar]
- 92.International Federation of Medical Students’ Associations; European Medical Students’ Association. Hilgers J, De Roos P. European core curriculum—The students’ perspective, Bristol, UK, 10 July 2006. Med Teach. 2007; 29:270–275 [DOI] [PubMed] [Google Scholar]
- 93.Kelly AM, Mullan PB. Designing a curriculum for professionalism and ethics within radiology: Identifying challenges and expectations. Acad Radiol. 2018; 25:610–618 [DOI] [PubMed] [Google Scholar]
- 94.Khanam NN, Chowdhury AA. Globalization of medical education curriculum. Bangladesh J Obstet Gynaecol. 2015; 30:37–42 [Google Scholar]
- 95.Lalloo D, Demou E, Kiran S, Cloeren M, Mendes R, Macdonald EB. International perspective on common core competencies for occupational physicians: A modified Delphi study. Occup Environ Med. 2016; 73:452–458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Lappin DW, Cannata-Andia JB; UEMS Section in Nephrology. Updated programme for harmonization of training in nephrology in the European Union. Clin Kidney J. 2013; 6:116–121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Lee AG, Golnik KC, Tso MO, Spivey B, Miller K, Gauthier TM. The International Council of Ophthalmology: Vision for ophthalmic education in an interdependent world. Am J Ophthalmol. 2012; 154:620–624.e2 [DOI] [PubMed] [Google Scholar]
- 98.Leinster S. Standards in medical education in the European Union. Med Teach. 2003; 25:507–509 [DOI] [PubMed] [Google Scholar]
- 99.Leslie K. The globalization of training in adolescent health and medicine: One size does not fit all. Int J Adolesc Med Health. 2016; 28:279–283 [DOI] [PubMed] [Google Scholar]
- 100.Macerollo A, Struhal W, Sellner J. Harmonization of European neurology education: The junior doctor’s perspective. Neurology. 2013; 81:1626–1629 [DOI] [PubMed] [Google Scholar]
- 101.Makoul G, Schofield T. Communication teaching and assessment in medical education: An international consensus statement. Netherlands Institute of Primary Health Care. Patient Educ Couns. 1999; 37:191–195 [DOI] [PubMed] [Google Scholar]
- 102.Masud T, Blundell A, Gordon AL, et al. European undergraduate curriculum in geriatric medicine developed using an international modified Delphi technique. Age Ageing. 2014; 43:695–702 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Mayberry JF. The development of medical education in Eastern Europe during the 20th century and the emergence of ‘English parallel’ courses. Scott Med J. 2013; 58:46–52 [DOI] [PubMed] [Google Scholar]
- 104.McKendrick MW; European Union of Medical Specialties. The European Union of Medical Specialties core training curriculum in infectious diseases: Overview of national systems and distribution of specialists. Clin Microbiol Infect. 2005; 11(suppl 1):28–32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.McLintock C, Pabinger I, Bauer KA, et al. International Society on Thrombosis and Haemostasis core curriculum project: Core competencies in clinical thrombosis and hemostasis. J Thromb Haemost. 2016; 14:3–27 [DOI] [PubMed] [Google Scholar]
- 106.McLintock C, Ross M. International Society on Thrombosis and Haemostasis core curriculum project: Core competencies in clinical thrombosis and hemostasis: Reply. J Thromb Haemost. 2016; 14:1318–1319 [DOI] [PubMed] [Google Scholar]
- 107.Meert A-P, Noël J-L, Boffetta P, et al. Thoracic oncology HERMES: A European syllabus towards a harmonised education and training of thoracic oncology specialists. Breathe. 2013; 9:381–392 [Google Scholar]
- 108.Mitchell S, Rohde G. Introducing an updated international ERS syllabus for postgraduate training 2017: Setting standards for training and certification in respiratory medicine. Breathe (Sheff). 2017; 13:e53–e55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Moxham B, McHanwell S, Plaisant O, Pais D. A core syllabus for the teaching of neuroanatomy to medical students. Clin Anat. 2015; 28:706–716 [DOI] [PubMed] [Google Scholar]
- 110.Moxham BJ, Plaisant O, Smith CF, Pawlina W, McHanwell S. An approach toward the development of core syllabuses for the anatomical sciences. Anat Sci Educ. 2014; 7:302–311 [DOI] [PubMed] [Google Scholar]
- 111.Naredi P, Audisio RA, Taylor I. Why do we need a core curriculum in surgical oncology in Europe? Surg Oncol. 2008; 17:267–269 [DOI] [PubMed] [Google Scholar]
- 112.Nieman K, Achenbach S, Pugliese F, Cosyns B, Lancellotti P, Kitsiou A. Cardiac computed tomography core syllabus of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging. 2015; 16:351–352 [DOI] [PubMed] [Google Scholar]
- 113.Norrby SR, Carbon C. Report of working group 3: Specialist training and continuing medical education/professional development in the infection disciplines. Clin Microbiol Infect. 2005; 11(suppl 1):46–49 [DOI] [PubMed] [Google Scholar]
- 114.Oduntan OA, Mashige KP, Kio FE, Boadi-Kusi SB. Optometric education in Africa: Historical perspectives and challenges. Optom Vis Sci. 2014; 91:359–365 [DOI] [PubMed] [Google Scholar]
- 115.Okel J, Okpechi IG, Qarni B, et al. Nephrology training curriculum and implications for optimal kidney care in the developing world. Clin Nephrol. 2016; 86:110–113 [DOI] [PubMed] [Google Scholar]
- 116.Oktay C. International Federation for Emergency Medicine model curriculum for emergency medicine specialists. Turkish J Emerg Med. 2011; 11:91–93 [DOI] [PubMed] [Google Scholar]
- 117.Palange P, Noel JL, Simonds AK. The European Respiratory Society: Future directions in medical education. Eur Respir J. 2011; 38:498–499 [DOI] [PubMed] [Google Scholar]
- 118.Pantano P, Chollet F, Paulson O, et al. ; European Federation of Neurological Societies Task Force of Neuroimaging in Neurology Curricula in Europe. EFNS Task Force on Teaching of Neuroimaging in Neurology Curricula in Europe: Present status and recommendations for the future. Eur J Neurol. 2001; 8:541–548 [DOI] [PubMed] [Google Scholar]
- 119.International Task Force on Opthalmic Education of Medical Students; International Council of Opthalmology. Principles and guidelines of a curriculum for ophthalmic education of medical students. Klin Monbl Augenheilkd. 2006; 223(suppl 5):S1–S19 [DOI] [PubMed] [Google Scholar]
- 120.Pfeiffer S, Chen Y, Tsai D. Progress integrating medical humanities into medical education: A global overview. Curr Opin Psychiatry. 2016; 29:298–301 [DOI] [PubMed] [Google Scholar]
- 121.Pfenninger EG, Domres BD, Stahl W, Bauer A, Houser CM, Himmelseher S. Medical student disaster medicine education: The development of an educational resource. Int J Emerg Med. 2010; 3:9–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Phadke K, Bagga A. Training in pediatric nephrology for developing countries. Pediatr Nephrol. 2005; 20:1205–1207 [DOI] [PubMed] [Google Scholar]
- 123.Pineda C, Reginato AM, Flores V, et al. ; Pan-American League of Associations for Rheumatology (PANLAR) Ultrasound Study Group. Pan-American League of Associations for Rheumatology (PANLAR) recommendations and guidelines for musculoskeletal ultrasound training in the Americas for rheumatologists. J Clin Rheumatol. 2010; 16:113–118 [DOI] [PubMed] [Google Scholar]
- 124.Prigent A, Huic D, Costa DC. Syllabus for postgraduate specialization in nuclear medicine—2011/2012 update: Nuclear medicine training in the European Union. Eur J Nucl Med Mol Imaging. 2012; 39:739–743 [DOI] [PubMed] [Google Scholar]
- 125.Prigent A, Hustinx R, Costa DC, et al. Nuclear medicine training in the European Union: 2015 update. Eur J Nucl Med Mol Imaging. 2016; 43:583–596 [DOI] [PubMed] [Google Scholar]
- 126.Rehani B, Brown I, Dandekar S, et al. Radiology education in Africa: Analysis of results from 13 African countries. J Am Coll Radiol. 2017; 14:247–252 [DOI] [PubMed] [Google Scholar]
- 127.Reisman Y, Eardley I, Porst H; Multidisciplinary Joint Committee on Sexual Medicine (MJCSM). New developments in education and training in sexual medicine. J Sex Med. 2013; 10:918–923 [DOI] [PubMed] [Google Scholar]
- 128.Sachdev P. Core curriculum in neuropsychiatry of the International Neuropsychiatric Association. Miyoshi K, Morimura Y, Maeda K, eds. In: Neuropsychiatric Disorders. Tokyo, Japan: Springer Japan; 2010317–346 [Google Scholar]
- 129.Salmon M, Landes M, Hunchak C, et al. Getting it right the first time: Defining regionally relevant training curricula and provider core competencies for point-of-care ultrasound education on the African continent. Ann Emerg Med. 2017; 69:218–226 [DOI] [PubMed] [Google Scholar]
- 130.San Luis TO, Jr, Vinjamuri S. Challenges of developing a pan-Asian curriculum: Lessons for global nuclear medicine training. Nucl Med Commun. 2012; 33:1119–1121 [DOI] [PubMed] [Google Scholar]
- 131.Schwarz MR, Wojtczak A. Global minimum essential requirements: A road towards competence-oriented medical education. Med Teach. 2002; 24:125–129 [DOI] [PubMed] [Google Scholar]
- 132.European Union of Medical Specialists Section and Board of Anaesthesiology. Carlsson C, Keld D, et al. Education and training in anaesthesia—Revised guidelines by the European Board of Anaesthesiology, Reanimation and Intensive Care. Eur J Anaesthesiol. 2008; 25:528–530 [DOI] [PubMed] [Google Scholar]
- 133.Sefton AJ. New approaches to medical education: An international perspective. Med Princ Pract. 2004; 13:239–248 [DOI] [PubMed] [Google Scholar]
- 134.Silva H, Bühler F, Maillet B, et al. Continuing medical education and professional development in the European Union. Pharm Med. 2012; 26:223–233 [Google Scholar]
- 135.Silva H, Stonier P, Buhler F, et al. Core competencies for pharmaceutical physicians and drug development scientists. Front Pharmacol. 2013; 4:105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Simpson P. Training, assessment and accreditation in anaesthesiology and the implications for the European Union. Eur J Anaesthesiol. 2003; 20:679–681 [DOI] [PubMed] [Google Scholar]
- 137.Singh P, Aggarwal R, Zevin B, Grantcharov T, Darzi A. A global Delphi consensus study on defining and measuring quality in surgical training. J Am Coll Surg. 2014; 219:346–353 [DOI] [PubMed] [Google Scholar]
- 138.Skeith L, Rodger MA, Lee AY, Kahn SR, Bates SM, Gonsalves C. International Society on Thrombosis and Haemostasis core curriculum project: Core competencies in clinical thrombosis and hemostasis: Comment. J Thromb Haemost. 2016; 14:1316–1317 [DOI] [PubMed] [Google Scholar]
- 139.Skirton H, Lewis C, Kent A, Coviello DA; Members of Eurogentest Unit 6 and ESHG Education Committee. Genetic education and the challenge of genomic medicine: Development of core competences to support preparation of health professionals in Europe. Eur J Hum Genet. 2010; 18:972–977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Soldatos C, Mavreas V, Kaprinis G, et al. Inter-university harmonization of undergraduate and graduate education in psychiatry. Consensus statement of the Hellenic College of Academic Psychiatry. Arch Hellenic Med. 2006; 23:379–392 [Google Scholar]
- 141.Spiwak R, Lett R, Rwanyuma L, Logsetty S. Creation of a standardized burn course for low income countries: Meeting local needs. Burns. 2014; 40:1292–1299 [DOI] [PubMed] [Google Scholar]
- 142.Struhal W, Mellgren SI, Grisold W. Three important steps to European neurology harmonization: Core curriculum, visitation program, European board examination. Eur J Neurol. 2013; 20:e101–e104 [DOI] [PubMed] [Google Scholar]
- 143.Tabin N, Mitchell S, O’Connell E, Stolz D, Rohde G. Update of the ERS international adult respiratory medicine syllabus for postgraduate training. Breathe (Sheff). 2018; 14:19–28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Tandeter H, Carelli F, Timonen M, et al. A ‘minimal core curriculum’ for family medicine in undergraduate medical education: A European Delphi survey among EURACT representatives. Eur J Gen Pract. 2011; 17:217–220 [DOI] [PubMed] [Google Scholar]
- 145.Tolba RH, Czigány Z, Osorio Lujan S, et al. Defining standards in experimental microsurgical training: Recommendations of the European Society for Surgical Research (ESSR) and the International Society for Experimental Microsurgery (ISEM). Eur Surg Res. 2017; 58:246–262 [DOI] [PubMed] [Google Scholar]
- 146.Tötsch M, Cuvelier C, Vass L, Fassina A; UEMS Section/Board of Pathology Meeting in Paris 2012. The UEMS Section/Board of pathology, chapter 6: Requirement for recognition of postgraduate training in pathology: A presentation of the Paris document. Cytopathology. 2012; 23:295–299 [DOI] [PubMed] [Google Scholar]
- 147.Tubbs RS, Sorenson EP, Sharma A, et al. The development of a core syllabus for the teaching of head and neck anatomy to medical students. Clin Anat. 2014; 27:321–330 [DOI] [PubMed] [Google Scholar]
- 148.Turner S, Seel M, Trotter T, et al. Defining a leader role curriculum for radiation oncology: A global Delphi consensus study. Radiother Oncol. 2017; 123:331–336 [DOI] [PubMed] [Google Scholar]
- 149.Van Gessel EF, Ostergard HT, Niemi-Murola L. Harmonisation of anaesthesiology training in Europe. Best Pract Res Clin Anaesthesiol. 2012; 26:55–67 [DOI] [PubMed] [Google Scholar]
- 150.Woolf AD. Specialist training in rheumatology in Europe. Rheumatology (Oxford). 2002; 41:1062–1066 [DOI] [PubMed] [Google Scholar]
- 151.Bion JF, Barrett H; CoBaTrICE Collaboration. Development of core competencies for an international training programme in intensive care medicine. Intensive Care Med. 2006; 32:1371–1383 [DOI] [PubMed] [Google Scholar]
- 152.Bandaranayake RC. Implementing change in medical education in developing countries. Med Teach. 1989; 11:39–45 [DOI] [PubMed] [Google Scholar]
- 153.Tackett S. Examining the Educational Commission for Foreign Medical Graduates announcement requiring medical school accreditation beginning in 2023. Acad Med. 2019; 94:943–949 [DOI] [PubMed] [Google Scholar]
- 154.Ho MJ, Abbas J, Ahn D, Lai CW, Nara N, Shaw K. The “glocalization” of medical school accreditation: Case studies from Taiwan, South Korea, and Japan. Acad Med. 2017; 92:1715–1722 [DOI] [PubMed] [Google Scholar]
- 155.Lindgren S, Karle H. Social accountability of medical education: Aspects on global accreditation. Med Teach. 2011; 33:667–672 [DOI] [PubMed] [Google Scholar]
- 156.Kim S, Choi S. The medical professionalism of Korean physicians: Present and future. BMC Med Ethics. 2015; 16:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Harden RM, Davis MH. AMEE medical education guide no. 5. The core curriculum with options or special study modules. Med Teach. 1995; 17:125–148 [Google Scholar]
- 158.Salafsky B, Glasser M, Ha J. Addressing issues of maldistribution of health care workers. Ann Acad Med Singapore. 2005; 34:520–526 [PubMed] [Google Scholar]
- 159.Maccarrick G. A practical guide to using the World Federation for Medical Education standards. WFME 2: Educational program. Ir J Med Sci. 2010; 179:489–491 [DOI] [PubMed] [Google Scholar]
- 160.Giuliani ME, Martimianakis MA, Papadakos J, Broadhurst M, Driessen E, Frambach J. Humanism in global oncology curricula: An emerging priority. J Clin Oncol. 2019; 37(suppl 15):10505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.World Health OrganizationWHO Traditional Medicine Strategy: 2014-2023Geneva, Switzerland: World Health Organization; 2013https://www.who.int/medicines/publications/traditional/trm_strategy14_23/en/. Accessed June 11, 2020 [Google Scholar]
- 162.Gall A, Leske S, Adams J, et al. Traditional and complementary medicine use among Indigenous cancer patients in Australia, Canada, New Zealand, and the United States: A systematic review. Integr Cancer Ther. 2018; 17:568–581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.International Atomic Energy AgencyIAEA Syllabus for the Education and Training of Radiation OncologistsVienna, Austria: International Atomic Energy Agency; 2009https://www-pub.iaea.org/MTCD/Publications/PDF/TCS-36_web.pdf. Accessed March 11, 2020 [Google Scholar]
- 164.Tsang DS, Patel S. Proton beam therapy for cancer. CMAJ. 2019; 191:E664–E666 [DOI] [PMC free article] [PubMed] [Google Scholar]
Reference cited in Figure 1 only
- 165.Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009; 6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.