

Abstract
OBJECTIVES
Brandt-Daroff exercises (BDEs) are commonly used as an at-home treatment for posterior canalithiasis, but their efficacy in the treatment of benign paroxysmal positional vertigo (BPPV) of the horizontal canal (HC-BPPV) has not been previously studied. Using biomechanical model simulation, we investigated modifications that may optimize BDE use for HC-BPPV treatment.
MATERIALS and METHODS
The BPPV Viewer, a three-dimensional model of the human labyrinth, was used to analyze BDE for HC-BPPV treatment. While moving the model through sequential BDE positions, the expected position of otoliths was demonstrated. Treatment steps were adjusted to maximize otolith movement around the canal circumference without compromising otolith repositioning into the semicircular duct’s anterior arm. All adjustments were integrated into lateral modified BDEs (LMBDEs) presented here.
RESULTS
By implementing several modifications, BDE can effectively treat HC-BPPV. Model simulation indicates tilting the head 20° upward in the lateral position, instead of 45° specified by the original technique, which significantly increases displacement of otoliths originating from the horizontal duct’s anterior and intermediate segments. LMBDE can be performed as a direct two-step sequence without pausing in the upright position before switching sides. If the affected ear is known, positioning the head 45° below horizontal on the unaffected side as a third treatment step can promote actual canal evacuation. These treatment enhancements increase circumferential otolith movement around the canal and may promote horizontal canal evacuation.
CONCLUSION
LMBDEs are a modification of BDE that may increase their effectiveness for use in patients with HC-BPPV. This safe treatment adjunct between office visits may promote long-term symptom reduction.
Keywords: Benign paroxysmal positional vertigo, vertigo, otorhinolaryngological diseases, physical therapy techniques
INTRODUCTION
Benign paroxysmal positional vertigo (BPPV), the most common vertiginous disorder, occurs when otoliths normally embedded in the utricle become dislodged and migrate into one of the semicircular ducts of the membranous labyrinth. This results in inappropriate gravity sensitivity in the affected semicircular duct and a false sense of spinning associated with changes in head position.[1] Owing to its dependent positioning when recumbent, otoliths most commonly enter the posterior semicircular duct. Horizontal semicircular canalithiasis is the second most common variant of BPPV and accounts for 3% to 30% of cases.[2–7] Horizontal canal BPPV (HC-BPPV) is characterized by horizontal nystagmus that is provoked by rotating the head in the supine position.[8,9]
Horizontal canal BPPV (HC-BPPV) can be divided into two subgroups based on the resting position of the otoliths in the horizontal duct, the anatomy of which is detailed in Figure 1. The majority of otoliths reside in the intermediate segment, resulting in geotropic disease. During a supine roll test, geotropic nystagmus beats toward the undermost ear and is more intense on the affected side. Contrarily, in a minority of cases, the loose otoliths reside in the anterior segment of the duct, resulting in apogeotropic disease. Apogeotropic horizontal nystagmus is transient and less intense lying on the affected side and long-lasting on the unaffected side in which position debris rests on the cupula.[10,11] This variant of horizontal canalithiasis in which debris is confined to the anterior segment of the canal closest to the cupula is sometimes confused with horizontal cupulolithiasis in which a long-lasting apogeotropic horizontal nystagmus is present in both right and left head positions.
Figure 1.
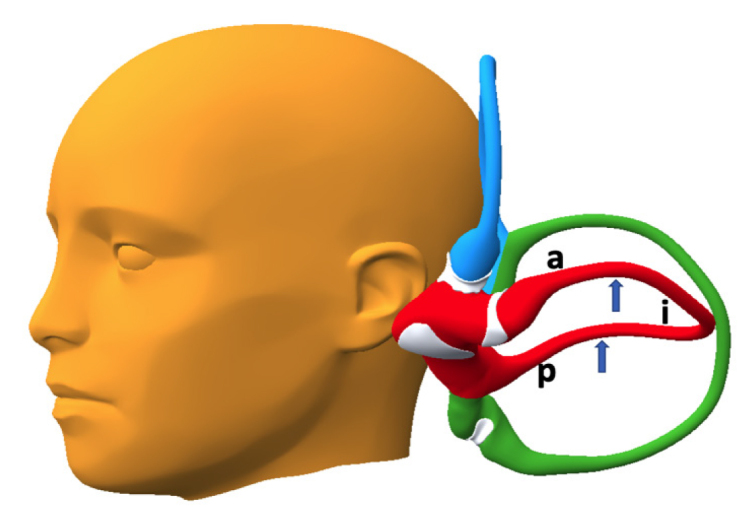
Segmentation of the lateral semicircular duct. The horizontal semicircular duct may be divided into three segments created by the bent toroid configuration of the duct. The anterior and posterior inflections of the horizontal semicircular duct are indicated (arrows). The inflections divide the duct into an anterior segment (a), an intermediate segment (i), and a posterior segment (p). The anterior segment (a) is bounded by the crista and cupula at one end and the anterior inflection (arrow) at the other. The intermediate segment (i), between the anterior and posterior inflections (arrows), is the longest. The posterior segment (p), between the posterior inflection (arrow) and the utricle, is downsloping and self-empties.
Over the last 30 years, several clinician-guided treatment maneuvers have been developed and revised to treat symptoms of HC-BPPV. The earliest treatments date back to the 1990s[12–14] and include the barbeque roll, described in a different variation by Baloh and Lempert[15,16]; the forced prolonged position[17]; the barrel roll[18]; the Gufoni[19]; and the Vannucchi-Asprella maneuvers.[20] More recent HC-BPPV treatments include the quick repositioning maneuver in 2015.[21]
Despite these advancements, patients with HC-BPPV have demonstrated higher recurrence rates,[22] uncovering the opportunity for treatment expansion. Given that HC-BPPV can be a challenging problem that does not resolve with in-office treatment alone, one solution may be the addition of self-performed maneuvers between office visits. At-home maneuvers have been well studied for posterior canalithiasis, with Brandt-Daroff exercises (BDEs) being the most commonly recommended. The addition of BDE is more effective than in-office treatment alone and may be equivalent to in-office treatment with long-term follow-up.[23–27] Although BDEs do not physically have the ability to displace otoliths from the posterior canal, mechanistically they work through dissolution and dispersion of debris and habituation of the pathologic response resulting from back-and-forth movement 90–120° around the duct circumference. The underlying presumption is that the greater the displacement, the more effective the exercise will be. The degree to which BDE may improve horizontal canalithiasis has never been studied. Using a biomechanical model, we sought modifications that would maximize otolith movement in the horizontal duct to promote dissolution, dispersion, habituation, and possibly repositioning of otolithic debris back to the utricular sac. We present lateral modified BDEs (LMBDEs) as a new treatment for HC-BPPV.
MATERIALS AND METHODS
The BPPV Viewer (BPPVViewer.com), a three-dimensional (3D) biomechanical model of the human labyrinth system designed for the study of BPPV, was used to analyze BDEs in the treatment of horizontal canalithiasis. This model, as previously reported by Teixido et al.,[28] was created from axial histological sections of a human labyrinth by following the same technique as reported by Wang et al.[29] for the creation of the Downloadable Virtual Model of the Temporal Bone. The histological sections were imaged with high-resolution scanning and integrated into Amira 5.2.2. (Thermo Fisher Scientific Inc., OR, USA), This reconstructed labyrinth was cloned for the contralateral side. Both labyrinths were positioned carefully in relation to a 3D surface map of a human skull. Virtual, mobile markers for otoliths were created to visualize the expected dependent position of the otolith in a given head position.
Using the model’s gravity function, the expected position of otoliths was demonstrated while moving the model through sequential positions of the BDEs. These steps were adjusted individually and systematically to identify a sequence that would accomplish three goals: first, to transfer any otoliths in the anterior segment of the horizontal duct to the intermediate segment; second, to maximize otolith movement around the circumference of the horizontal duct during maneuver repetitions; and, third, to promote canal emptying into the utricle. These techniques were also adjusted to maximize patient safety as an at-home self-performed technique by ensuring no patients with geotropic HC-BPPV convert to apogeotropic disease. Numerous trials and elimination of unnecessary positions allowed us to identify a modified sequence that is efficient, safe, and effective.
All technique adjustments were integrated into the LMBDE presented here. Image screenshots from the model demonstrating positioning were taken for the publication of this article.
RESULTS
Brandt-Daroff Exercises (BDEs), conventionally used for posterior canalithiasis, can be optimized for safe and effective treatment of horizontal canalithiasis if several modifications are implemented. Simulation of BDEs with the model revealed only 90° of movement of horizontal canal otoliths around the horizontal semicircular duct. This may account for the limited efficacy of standard BDEs for the treatment of horizontal canalithiasis. Analysis with the model revealed potential enhancements and treatment predicaments that can compromise the effectiveness of the maneuver that are not evident without model analysis. These results are best presented in a hierarchy of priority necessary to arrive at a single best solution for patients with both geotropic and apogeotropic variants of horizontal canalithiasis.
Discovery of Head Rotation Resulting in Minimum Risk of Increased Symptoms
It is important that no patient converts from geotropic to apogeotropic horizontal canalithiasis and experiences increased symptoms while performing a home maneuver. If a patient with geotropic horizontal canalithiasis descended on the affected ear with the nose turned below horizontal as described earlier, the horizontal canalith mass is predicted to move forward into the anterior arm of the canal when the patient reverses positions, causing apogeotropic disease. However, if the patient descends on the affected ear and the head does not turn below horizontal, no harm is done. It is crucial that a home maneuver performed by a naïve patient cannot make the problem worse, so we modified our maneuver with the head 20° above horizontal for assurance that the geotropic patient does not mistakenly convert to apogeotropic disease.
Discovery of Head Rotation That Effectively Treats Patients with Apogeotropic Canalithiasis
When the head is turned 20° up from the horizontal position, anterior limb (apogeotropic) horizontal canalithiasis was reliably converted to geotropic horizontal canalithiasis. If the same patient reclines first to the unaffected side, the otolith mass stayed trapped, but was seen to be liberated to the middle segment of the horizontal duct at the next repetition of the maneuver.
Discovery of Head Rotation Resulting in Maximum Displacement
With the head tilted 45° upward in the lateral position as specified by the original Brandt-Daroff technique, the horizontal canal otolith mass demonstrated 90° of movement around the circumference of the canal and no possibility of evacuating the horizontal canal. With the head facing forward in the lateral position, a full 180° of movement was achieved and even provoked canal emptying for patients with geotropic disease, but this positioning did not facilitate migration of otoliths from the anterior segment of the duct to the middle segment for those patients with apogeotropic disease. This compromised efficacy in a subset of patients is unacceptable in a universal maneuver. With our modified technique, the upward head tilt was reduced to 20° above horizontal in the lateral position. This angulation promoted conversion of apogeotropic to geotropic disease (moves otoliths present in the anterior segment to the middle segment of the duct) and resulted in increased otolith movement from 90° to 140° around the circumference of the canal in all patients with horizontal canalithiasis (Figure 2).
Figure 2.
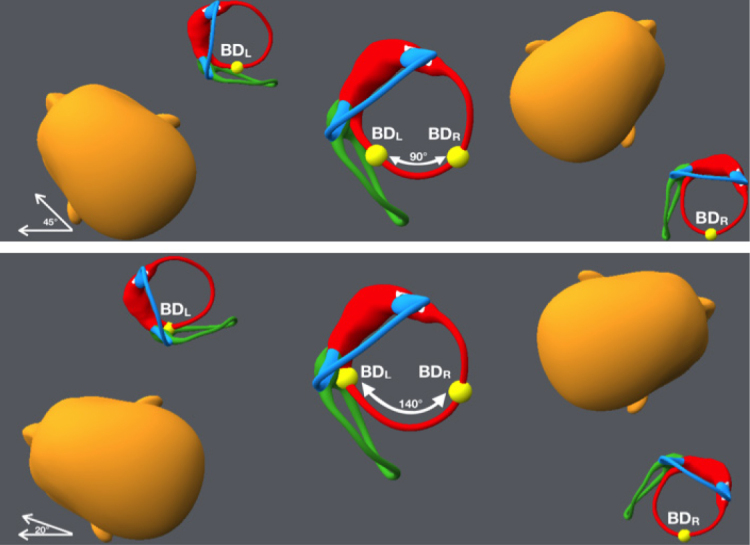
Arch of otolith movement from standard Brandt-Daroff exercises (BDEs) compared with our lateral modified BDEs (LMBDE). Top: Otolith movement from standard BDEs designed for posterior canalithiasis with head 45° above horizontal in the lateral position. Between left (BDL) and right lateral Brandt-Daroff positions (BDR), the otolith moved approximately 90° around the circumference of the horizontal canal. Bottom: Otolith movement from the LMBDE performed with head 20° above horizontal in the lateral position. Between left (BDL) and right lateral Brandt-Daroff positions (BDR), the otolith moved approximately 140° around the circumference of the horizontal canal.
Elimination of Unnecessary Positions
Stopping in the upright position in each repetition halts otolith movement, which has no perceivable advantage in this treatment, so this position was eliminated. Performing our modified exercises as two consecutive movements with the head 20° above horizontal in the lateral position was arrived at as the most efficient, safe, and effective solution for all patients. This simple two-step treatment sequence is depicted in Figure 3.
Figure 3.
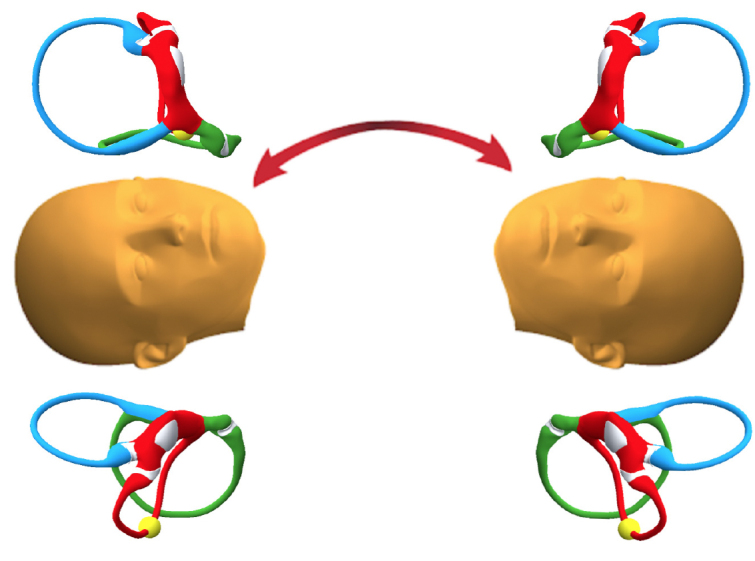
Lateral modified Brandt-Daroff exercises (LMBDEs): a simple two-step sequence for left or right-sided HC-BPPV. The treatment sequence consists of two positions performed in alternation with the head rotated 20° upward from horizontal in the lateral positions.
Enhanced Treatment in Patients Whose Side of Disease Is Known
This technique was further optimized to allow canal emptying in patients in whom the side of disease is known by placing the head 45° below horizontal on the unaffected side as a third treatment movement. This both increased the movement of the otolith around the circumference of the canal and even promoted evacuation of the horizontal canal in the uppermost ear. However, the usefulness of this modification requires clear knowledge of the affected ear and could create worse problems for patients if they unknowingly descend on the affected side. This will work for apogeotropic and geotropic horizontal canalithiasis (Figures 4 and 5).
Figure 4.

Lateral modified Brandt-Daroff exercises (LMBDEs): a three-step sequence for left-sided HC-BPPV. Treatment of (apogeotropic or geotropic) left-sided disease with additional treatment step, turning the head 45° downward when on the right, to promote horizontal canal emptying. To be sure an apogeotropic case is cured and not perpetuated on the left, the head turn should happen only as a third position as seen above. Left: Three treatment steps for left-sided HC-BPPV. Right: Otolith movement around the circumference of the horizontal duct in each of the three treatment positions shown from an inferior axial view.
Figure 5.

Lateral modified Brandt-Daroff exercises (LMBDEs): a three-step sequence for right-sided HC-BPPV. Treatment of (apogeotropic or geotropic) right-sided disease with additional treatment step, turning the head 45° downward when on the left, to promote horizontal canal emptying. To be sure an apogeotropic case is cured and not perpetuated on the right, the head turn should happen only as a third position as seen above. Left: Three treatment steps for right-sided HC-BPPV. Right: Otolith movement around the circumference of the horizontal duct in each of the three treatment positions shown from an inferior axial view.
DISCUSSION
Brandt-Daroff Exercises (BDEs) date back to 1980 when Brandt and Daroff published their manuscript.[30] Originally devised as an inpatient treatment, BDEs involved patients lying lateral recumbent on the provocative side with the head 45° above horizontal until vertigo resided, sitting upright for 30 seconds, and then lying lateral recumbent on the opposite side with the head 45° above horizontal for another 30 seconds. This sequence was repeated every three hours and stopped after two consecutive vertigo-free days.[30] In their original study, 66 of the 67 patients (98.5%) treated with BDEs achieved complete relief of the positional vertigo within 3 to 14 days, with most requiring 7 to 10 days.[30] Over time, BDEs have transformed into predominantly outpatient treatment, and they are one of the most commonly recommended treatments for patients to perform at home. There are numerous studies supporting their effectiveness for the treatment of BPPV.[23–27] In a study comparing the effectiveness of treatment with the Epley maneuver alone or combined with at-home BDEs in between sessions, Desai et al.[26] found that the patients who also performed the BDEs had better symptom resolution and independence after one month. However, these studies have been limited to posterior canalithiasis, and the use of BDEs for the treatment of BPPV in other canals has not been studied.
Continuous modifications and refinements characterize the history of the treatment of BPPV and have led to enhanced treatment efficacy. Although the treatment of horizontal canalithiasis has significantly advanced over the last 30 years, it still lags behind that of posterior canalithiasis. Patients with HC-BPPV have been shown to have higher recurrence rates[22]; thus, treatment aimed at reducing recurrence and improving long-term patient outcomes is crucial.
With its highly realistic anatomy and mobility features, it is reasonable to believe our biomechanical model analysis presents a useful solution to the advancement of horizontal canalithiasis treatment. We ensured all predicted gross otolith movements are similar to head position changes that produce observable eye movements in clinical practice. The model analysis shows that standard BDEs, with the head 45° upward from horizontal in the horizontal position, results in a limited degree of movement around the circumference of the horizontal canal. This maximum of 90° displacement is at the low range of displacements expected in the same exercises for posterior canalithiasis and may explain the generally accepted perception that BDEs are not effective for treatment of horizontal canalithiasis.
Adjusting the head rotation to remain at 20° above horizontal and eliminating the need to stop in the upright position when switching sides can both improve predicted otolith movement and simplicity of the BDEs for this group of patients. This simple two-step at-home maneuver can be performed safely by any novice patient, without regard to the affected ear or type of disease. Although determining the affected side is often not a problem for experienced practitioners, it cannot always be determined by all clinicians who see this very common ailment. Nevertheless, this simple non-ear specific treatment option can still be used.
Our analysis demonstrates the LMBDE will reliably convert apogeotropic to geotropic disease. This is similar to the supine roll test that converts apogeotropic canalithiasis to geotropic.
As an efficacious treatment for both geotropic and apogeotropic horizontal canalithiasis, we also presented the option of incorporating an additional treatment step, which entailed rotating the head 45° below horizontal on the unaffected side if it is known. The addition of this third step essentially incorporates the Gufoni maneuver, which has been shown to reliably empty the horizontal canal into the repeated exercise. However, we recommend reserving this treatment for experienced practitioners whose patients did not find success with our simple two-step technique.
CONCLUSION
Lateral Modified Brandt-Daroff Exercises (LMBDEs) are a modification of BDEs that can increase their effectiveness for use in patients with all horizontal canalithiasis and may be a safe and useful treatment adjunct between office visits to increase long-term symptom reduction. Analysis with the 3D model predicts efficacy over standard BDEs for horizontal canal BPPV; however, these results should be confirmed with controlled clinical patient analysis, which is currently being initiated at our institution.
MAIN POINTS.
Lateral Modified Brandt-Daroff Exercises (LMBDEs) are a modification of Brandt-Daroff Exercises (BDEs) that may increase their effectiveness for use in patients with horizontal canal benign paroxysmal positional vertigo (HC-BPPV.)
LMBDEs primarily involve two alterations; adjusting the head rotation to remain at 20° above horizontal and eliminating the need to stop in the upright position when switching sides can both improve predicted otolith movement and simplicity of the BDEs.
Our simple two-step at-home maneuver can be performed safely by any novice patient, without regard to the affected ear or type of disease.
As an efficacious treatment for both geotropic and apogeotropic horizontal canalithiasis, clinicians may also use our three-step ear specific maneuver, which entailed an additional step rotating the head 45° below horizontal on the unaffected side if it is known.
With its highly realistic anatomy and mobility features, it is reasonable to believe our biomechanical model analysis presents a useful solution to the advancement of horizontal canalithiasis treatment; however, these results should be confirmed with controlled clinical patient analysis, which is currently being initiated at our institution.
Footnotes
This study was presented at the 145th Annual Meeting of the American Neurological Association, October 5, 2020, Virtual Meeting.
Ethics Committee Approval: N/A.
Informed Consent: N/A.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – M.T., L.E.M., R.C.; Design – M.T., L.E.M.; Supervision - M.T., R.C.; Resource - M.T.; Materials - M.T., L.E.M.; Data Collection and/or Processing - L.E.M., R.C.; Analysis and/or Interpretation - L.E.M., R.C.; Literature Search - L.E.M.; Writing - L.E.M., M.T., R.C.; Critical Reviews - L.E.M., M.T., R.C.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol. 1979;8:151. [PubMed] [Google Scholar]
- 2.Korres S, et al. Occurrence of semicircular canal involvement in Benign Paroxysmal Positional Vertigo. Otol Neurotol. 2002;23:926–32. doi: 10.1097/00129492-200211000-00019. [DOI] [PubMed] [Google Scholar]
- 3.Hornibrook J. Horizontal canal benign positional vertigo. Ann Otol Rhinol Laryngol. 2004;113:721–5. doi: 10.1177/000348940411300908. [DOI] [PubMed] [Google Scholar]
- 4.Caruso G, Nuti D. Epidemiological data from 2270 PPV patients. Audiological Med. 2005;3:7–11. doi: 10.1080/16513860510028310. [DOI] [Google Scholar]
- 5.Cakir BO, Ercan I, Cakir ZA, Civelek S, Sayin I, Turgut S. What is the true incidence of horizontal semicircular canal benign paroxysmal positional vertigo? Otolaryngol Head Neck Surg. 2006;134:451–4. doi: 10.1016/j.otohns.2005.07.045. [DOI] [PubMed] [Google Scholar]
- 6.Uno A, Moriwaki K, Kato T, Nagai M, Sakata Y. Clinical features of benign paroxysmal positional vertigo. Nippon Jibiinkoka Gakkai Kaiho. 2001;104:9–16. doi: 10.3950/jibiinkoka.104.9. [DOI] [PubMed] [Google Scholar]
- 7.Nuti D, Mandala M, Salerni L. Lateral canal paroxysmal positional vertigo revisited. Ann N Y Acad Sci. 2009;1164:316–23. doi: 10.1111/j.1749-6632.2008.03720.x. [DOI] [PubMed] [Google Scholar]
- 8.Cipparrone L, Corridi G, Pagnini P. Cupulolitiasi. In: Dufour A, editor. V° giornata Italiana di Nistagmografia Clinica. Boots-Formenti. Milano; Italy: 1985. pp. 36–53. [Google Scholar]
- 9.McClure J. Horizontal canal BPV. J Otolaryngol. 1985;14:30–5. [PubMed] [Google Scholar]
- 10.White JA, Coale KD, Catalano PJ, Oas JG. Diagnosis and Management of Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo. Otolaryngol Head Neck Surg. 2005;133:278–84. doi: 10.1016/j.otohns.2005.03.080. [DOI] [PubMed] [Google Scholar]
- 11.Maia FZE. New treatment strategy for apogeotropic horizontal canal benign paroxysmal positional vertigo. Audiol Res. 2016;6:163. doi: 10.4081/audiores.2016.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pagnini P, Nuti D, Vannucchi P. Benign paroxysmal vertigo of the horizontal canal. ORL J Otorhinolaryngol Relat Spec. 1989;51:161–70. doi: 10.1159/000276052. [DOI] [PubMed] [Google Scholar]
- 13.Pagnini P, Vannucchi P, Nuti D. Le nystagmus apogéotropique dans la vertige paroxystique positionelle bénin du canal sémicirculaire horizontal. La Revue d’Otoneurologie Française. 1994;12:304–7. [Google Scholar]
- 14.Nuti D, Vannucchi P, Pagnini P. Benign paroxysmal vertigo of the horizontal canal: a form of canalolithiasis with variable clinical features. J Vestib Res. 1996;6:173–84. doi: 10.1016/0957-4271(95)02010-1. [DOI] [PubMed] [Google Scholar]
- 15.Baloh RW. Reply to the letter by Lempert: horizontal benign positional vertigo. Neurology. 1994;44:2214. doi: 10.1212/WNL.44.11.2214. [DOI] [PubMed] [Google Scholar]
- 16.Lempert T, Ttiel-Wilck K. A positional maneuver for treatment of horizontal-canal benign positional vertigo. Laryngoscope. 1996;106:476–8. doi: 10.1097/00005537-199604000-00015. [DOI] [PubMed] [Google Scholar]
- 17.Vannucchi P, Giannoni B, Pagnini P. Treatment of lateral semicircular canal benign paroxysmal positional vertigo. J Vest Res. 1997;7:1–6. doi: 10.1016/S0957-4271(96)00112-7. [DOI] [PubMed] [Google Scholar]
- 18.Epley JM. Caveats in particle repositioning for treatment of canalithiasis. Operative Tech. Otolaryngol Head Neck Surg. 1997;8:68–76. doi: 10.1016/S1043-1810(97)80005-X. [DOI] [Google Scholar]
- 19.Gufoni M, Mastrosimone L. Trattamento con manovra di riposizionamento per la canalolitiasi orizzontale. Acta Otorhinolaringol Ital. 1998;18:363–7. [PubMed] [Google Scholar]
- 20.Vannucchi P, Asprella Libonati G, Gufoni M. The Physical Treatment of Lateral Semicircular CanalCanalolithiasis. Audiol Med. 2005;3:52–6. doi: 10.1080/16513860510029445. [DOI] [Google Scholar]
- 21.Li J, Guo P, Tian S, Li K, Zhang H. Quick repositioning maneuver for horizontal semicircular canal benign paroxysmal positional vertigo. J Otol. 2015;10:115–7. doi: 10.1016/j.joto.2015.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sakaida M, Takeuchi K, Ishinaga H, Adachi M, Majima Y. Long-term outcome of benign paroxysmal positional vertigo. Neurology. 2003;60:1532–4. doi: 10.1212/01.WNL.0000061477.03862.4D. [DOI] [PubMed] [Google Scholar]
- 23.Banfield GK, Wood C, Knight J. Does vestibular habituation still have a place in the treatment of benign paroxysmal positional vertigo? J Laryngol Otol. 2000;114:501–5. doi: 10.1258/0022215001906237. [DOI] [PubMed] [Google Scholar]
- 24.Cohen HS, Kimball KT. Effectiveness of treatments for BPPV of the posterior canal. Otol Neurotol. 2005;26:1034–40. doi: 10.1097/01.mao.0000185044.31276.59. [DOI] [PubMed] [Google Scholar]
- 25.Haripriya S, Ajith S, Babu Roshan PS, Faisal CkM. Comparison of Epley Maneuver and Brandt-Daroff Exercises on Short-Term Posterior Canal Benign Paroxysmal Positional Vertigo - Related Quality of Life. Indian J Physiother Occup Ther. 2014;8:109–13. doi: 10.5958/0973-5674.2014.00366.9. [DOI] [Google Scholar]
- 26.Desai DS, Chauhan AS, Trivedi MN. Role of Modified Epley’S Maneuver and Brandt-Daroff Exercises in Treatment of Posterior Canal Bppv: A Comparative Study. Int J Physiother Res. 2015;3:1059–64. doi: 10.16965/ijpr.2015.137. [DOI] [Google Scholar]
- 27.Cetin YS, Ozmen OA, Demir UL, Kasapoglu F, Basut O, Coskun H. Comparison of the effectiveness of Brandt-Daroff Vestibular training and Epley Canalith repositioning maneuver in benign Paroxysmal positional vertigo long term result: A randomized prospective clinical trial. Pak J Med Sci. 2018;34:558–63. doi: 10.12669/pjms.343.14786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Teixido M, Woods O, Kung B, Seyyedi M. A 3D benign paroxysmal positional vertigo model for study of otolith disease. World J Otorhinolaryngol Neck Surg. 2016;2:1–6. doi: 10.1016/j.wjorl.2016.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wang H, Northrop C, Burgess B, Liberman MC, Merchant SN. Three-dimensional virtual model of the human temporal bone: a stand-alone, downloadable teaching tool. Otol Neurotol. 2006;27:452–7. doi: 10.1097/01.mao.0000188353.97795.c5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Brandt T, Daroff RB. Physical Therapy for Benign Paroxysmal Positional Vertigo. Arch Otolaryngol. 1980;106:484–5. doi: 10.1001/archotol.1980.00790320036009. [DOI] [PubMed] [Google Scholar]