

Abstract
Isolated Eustachian tube osteomata are a very rare entity indeed, with the last case being reported in 1979. We describe a case of the otoscopic finding of a blue-yellowish eardrum and successive identification by computed tomography scan of an osteoma localized in the Eustachian tube. Clinical presentation and diagnostic and therapeutic phases in comparison with the literature will be discussed.
Keywords: Osteoma, middle ear, temporal bone, hearing loss
INTRODUCTION
Osteoma of the temporal bone is a benign neoplasm composed of mature bone, usually single, unilateral, and pedunculate. It is histologically characterized by fibrovascular channels and surrounded by irregularly oriented lamellated bone[1]. The etiology is still unclear: the literature reports cases of familiar osteomata and others associated with Gartner’s syndrome, suggesting a congenital origin of the disease[2], but the inflammatory process is considered a possible cause as well[3]. Trauma, infection, hormonal and genetic factors, as well as contact by sites of distinct embryological origins have been considered possible co-factors for the onset of this clinical picture[1]. Osteomata most commonly originate from the external auditory canal; however, they can also be found at other sites such as the mastoid, the squama, the internal auditory canal, or the middle ear[4]. Their incidence in the external auditory canal is estimated at about 0.05% of the otologic procedures[5], whereas the incidence in the middle ear cannot be precisely inferred from the literature. Isolated osteoma of the Eustachian tube is extremely rare; to our knowledge since Hildyard and Compere’s first description in 1959, only one other case was reported in 1979[6,7]. We describe a case of an isolated Eustachian tube osteoma, focusing on its clinical presentation and the diagnostic and therapeutic phases in comparison with the literature.
CASE PRESENTATION
A 64-year-old female patient with a long-standing history of progressive bilateral asymmetric hearing loss was referred to our department due to an occasional otoscopic finding of a blue right eardrum. An otomicroscopic examination performed in our unit showed a blue nonpulsating eardrum in the posterior quadrants, with middle ear yellowish effusion in the anterior quadrants in the right ear (Figure 1) and myringosclerosis in the left ear. The physical evaluation of the ear, nose, and throat did not show any other alterations, and the nasal and rhinopharyngeal endoscopy was negative. A pure-tone audiogram revealed a mixed hearing loss (pure-tone average of 70 decibel Hearing Level (dB HL) with an air-bone gap of 35 dB HL in the right ear and mild sensorineural hearing loss in the left ear (Figure 2). The impedancemetry showed a type-B tympanogram on the right and a type-A tympanogram on the left. The patient underwent oral steroid therapy, without any clinical benefits. The presence of hypodense material in the middle ear and mastoid with no osteolysis affecting the ossicular chain and the mastoid trabeculae was detected by the high-resolution computed tomography (HR-CT) scan. In addition, a bony mass determining the almost complete obliteration of the tympanic opening of the right Eustachian tube was found. It was oval in shape, with maximum diameters of 11.8 × 4.5 mm, and it was identified as an osteoma (Figures 3 and 4). The therapeutic approach suggested included a right myringotomy with the insertion of a transtympanic ventilation tube or an acoustic prosthesis, but these therapies were refused. Periodical follow-up with HR-CT and audiologic examination were recommended to assess the possible growth of the osteoma.
Figure 1.

Blue-yellowish right eardrum: otoscopic view.
Figure 2.
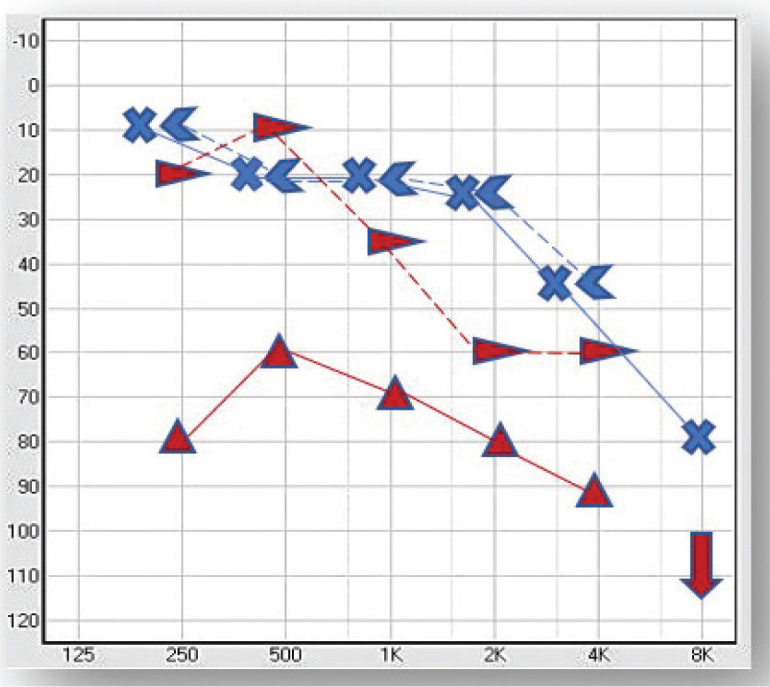
Pure tone audiometry.
Figure 3.
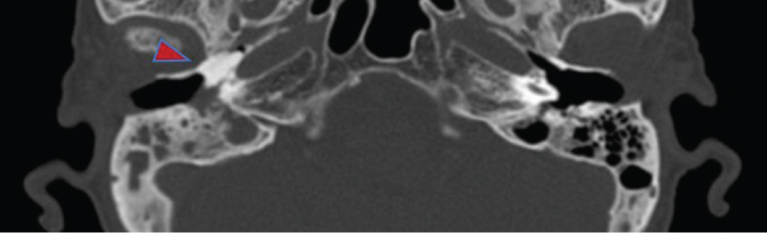
HR-CT scan: bony mass in the right Eustachian tube, axial view.
Figure 4.
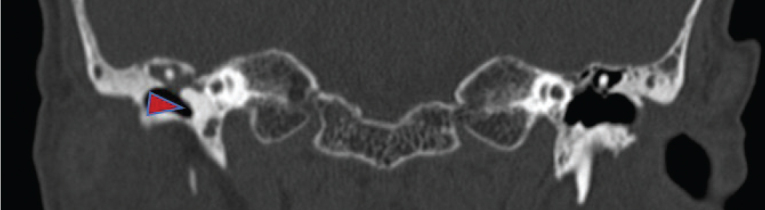
HR-CT scan: bony mass in the right Eustachian tube, coronal view.
DISCUSSION
Osteomata of the temporal bone are benign tumors of lamellar bone. An isolated Eustachian tube osteoma is an extremely rare entity: to our knowledge, only two cases were described thus far, one in 1959 and the other in 1979[6,7]. In the literature, three other osteomata, which involve Eustachian tube, have been reported: two of them were found in the context of multiple osteomata of middle ear[2, 3]; the other case was a huge osteoma of the tympanic cavity extending into the Eustachian tube[8]. The previously reported osteomata were diagnosed during radiological investigations: the first two cases were detected with an x-ray examination, and the other three were identified with a CT scan. Osteomata appear with bone CT scan as focal, well-circumscribed, pedunculated lesions with egg-shell-like density[2, 8] or bony mass density[3]. In the case we describe, the CT scan showed a bone density overgrowth. In all these cases, the patients presented with chronic or recurrent otitis media with tympanic membrane involvement: in three cases, it was perforated, and in two, eroded; the hearing loss was always the symptom of presentation (in four cases with otorrhea)[3, 6–8]. Hearing loss was attributed to dislocation[2,8] or fixation[3] of of the ossicular chain, to the tympanic membrane impingement[2, 6, 7] and to the effects of chronic otitis media[2, 3, 6–8]. On the contrary, in our case, there was no evidence of ossicular chain or tympanic membrane involvement, and the conductive component of the hearing loss was probably related only to the middle ear dysventilation. In particular, we supposed that the tubal occlusion obstructed drainage, leading to air reabsorption, negative pressure, mucosal edema, and hemorrhage. The middle ear effusion, composed of a transudate of the mucosa of the middle ear cleft, determined the yellowish coloration of the drum. The hemosiderin derived from ruptured erythrocytes deposited in the lower part of the drum and mixed with yellowish effusion, thereby giving a blue coloration to the posterior quadrants. We could speculate the absence of tympanic damage is due to favorable anatomic conformation of the middle ear responsible for maintaining gas pressure balance[9]. The causative relationship between osteoma and chronic otitis media is not univocal. Some osteomata are thought to have a genetic etiology, others an inflammatory cause[10]. To our knowledge, there are not specific criteria to distinguish congenital from acquired osteomata. Among the five cases previously reported, three were found in young girls and two in middle-aged men. In the patient described by Hildyard and Compere[6], the early age of symptoms presentation could suggest a congenital origin and the later onset of a chronic otitis media. Denia et al.[7] suggested that in their case, the Eustachian tube dysfunction caused by the osteoma could have played a role in the development of a middle ear and mastoid cholesteatoma. Cho et al.[8] and Kim et al.[2], despite the young age of their patients, speculated that the mass obliterating the Eustachian tube could have been the main reason for recurrent middle ear effusion and inflammation, and not vice versa. On the contrary, Li et al.[3] indicated as a possible origin of osteoma in their patient the chronic otitis media and long-term use of ephedrine as ear drops. Considering the apparent indolence of the osteoma we described, we could suggest that it was a slow-growing congenital osteoma. In the literature, surgical intervention is recommended for symptomatic middle ear osteomata, which include osteomata with Eustachian tube obstruction[2]. In all the five cases previously reported, the osteomata were associated with otorrhea or otalgia, and consequently, a surgical treatment was proposed to treat otitis and remove the osteoma. The surgical solution was accepted in four cases. However, some authors suggest regular clinical and radiological follow-up for these cases in which the risk–benefits assessment of the intervention seems unfavorable[10], in particular considering the risk of carotid artery injuries. Balancing the apparent indolence of the osteoma in our patient and the risks associated with surgery, we did not advise osteoma removal but suggested a periodic follow-up to evaluate its growth. To treat the hearing loss, we suggested transtympanic ventilation tube insertion or alternatively an acoustic prosthesis, but the patient refused.
CONCLUSION
To our knowledge, our case is the third of isolated Eustachian tube osteoma ever reported in the literature, with the previous one dating back to 1979. It differs from the other cases because of its apparent indolence, and it is for this reason that we suggested periodic clinical and radiological follow-ups.
MAIN POINTS.
Isolated Eustachian tube osteoma is an extremely rare entity: to our knowledge, only two cases were reported respectively in 1959 and in 1979.
We describe a case identified in a patient with a longstanding history of progressive bilateral asymmetric hearing loss, who was referred to our attention due to the occasional finding of blue eardrum.
This is the first isolated Eustachian tube osteoma detected with CT scan.
Our case differs from the others because of its apparent indolence, for this reason we did not advise osteoma removal but suggested a periodic follow-up.
Appendix. Reported osteomata involving the Eustachian tube
| Year | Authors | Age | Sex | Presentation | TM | Symptoms | Radiologic aspect | Treatment |
|---|---|---|---|---|---|---|---|---|
| 1959 | Hildyard and Compere | 22 | F | Isolated | Perforated | CHL, otorrhea | X-ray: smooth rounded | Myringoplasty, removal with a curette |
| 1979 | Denia et al. | 55 | M | Isolated | Perforated | CHL, otorrhea, associated with cholesteatoma | X-ray: oval shape | Surgical exploration advised but refused |
| 2005 | Cho et al. | 15 | F | Tympanic cavity extending into Eustachian tube | Eroded, wet | CHL, otorrhea | CT scan: Egg-shell like density | CWD mastoidectomy |
| 2006 | Kim et al. | 28 | F | Multiple | Anulus eroded, Bulge | MHL, otalgia | CT scan: Egg-shell like density | CWU mastoidectomy |
| 2012 | Li et al. | 52 | M | Multiple | Perforated | MHL, otorrhea | CT scan: Bony mass density | CWU mastoidectomy |
| Our experience | 64 | F | Isolated | Not perforated | MHL | CT scan: Bony mass density | Proposed transtympanic ventilation tube insertion or alternatively acoustic protesization | |
CHL: conductive hearing loss; MHL: mixed hearing loss.
Footnotes
Informed Consent: Written informed consent was obtained from the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – C.P., M.M., S.A.; Design - C.P., I.A., C.E.; Supervision - C.P., I.A., B.M.; Resource - C.P., P.F., S.A.; Materials - C.P., S.A., P.F.; Data Collection and/or Processing - C.P., C.E., N.M.; Analysis and/or Interpretation - C.P., S.A., M.M.; Literature Search - C.P., C.E., N.M.; Writing - C.P., I.A., C.E.; Critical Reviews - C.P., M.M., B.M.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Schutt CA, Guo JN, Bagwell KA, Bulsara KR, Malhotra A, Michaelides E. Bilateral osteomas and exostoses of the internal auditory canal. Am J Otolaryngol. 2015;36:583–6. doi: 10.1016/j.amjoto.2015.03.006. [DOI] [PubMed] [Google Scholar]
- 2.Kim CW, Oh SJ, Kang JM, Ahn HY. Multiple osteomas in the middle ear. Eur Arch Otorhinolaryngol. 2006;263:1151–4. doi: 10.1007/s00405-006-0123-x. [DOI] [PubMed] [Google Scholar]
- 3.Li Y, Li Q, Gong S, Liu H, Yu Z, Zhang L. Multiple Osteomas in Middle Ear. Case Rep Otolaryngol. 2012;2012:685932. doi: 10.1155/2012/685932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Toro PC, Castillo ÀC, Moya Martínez R, Domenech Juan I. Middle Ear Promontory Osteoma. Am J Otolaryngol. 2014;35:626–7. doi: 10.1016/j.amjoto.2014.07.005. [DOI] [PubMed] [Google Scholar]
- 5.Gheorghe DC, Stanciu AE, Ulici A, Zamfir-Chiru-Anton A. Bilateral external ear canal osteomas - discussion on a clinical case. J Med Life. 2016;9:434–6. [PMC free article] [PubMed] [Google Scholar]
- 6.Hildyard VH, Compere WEJ. Osteoma of the Eustachian tube. Laryngoscope. 1959;69:1524–7. doi: 10.1288/00005537-195912000-00005. [DOI] [PubMed] [Google Scholar]
- 7.Denia A, Perez F, Canalis RR, Graham MD. Extracanalicular Osteomas of the Temporal Bone. Arch Otolaryngol. 1979;105:706–9. doi: 10.1001/archotol.1979.00790240020005. [DOI] [PubMed] [Google Scholar]
- 8.Cho YS, Kim JH, Hong SH, Chung WH. A huge osteoma of the middle ear. Int J Pediatr Otorhinolaryngol. 2005;69:1569–74. doi: 10.1016/j.ijporl.2005.04.008. [DOI] [PubMed] [Google Scholar]
- 9.Presutti L, Anschuetz L, Rubini A, Ruberto M, Alicandri-Ciufelli M, Dematte M, et al. The Impact of the Transcanal Endoscopic Approach and Mastoid Preservation on Recurrence of Primary Acquired Attic Cholesteatoma. Otol Neurotol. 2018;39:445–50. doi: 10.1097/MAO.0000000000001712. [DOI] [PubMed] [Google Scholar]
- 10.Molher J, Pujol EMD, Zounon ADS, Darrouzet V, Bonnard D. Middle Ear Osteoma Causing Mixed Hearing Loss: A Case Report. J Int Adv Otol. 2018;14:493–6. doi: 10.5152/iao.2018.5265. [DOI] [PMC free article] [PubMed] [Google Scholar]