

Abstract
Establish outcomes following cochlear implantation (CI) in patients with Jervell and Lange-Nielsen Syndrome (JLNS). Methods Systematic review and narrative synthesis. Databases searched on Medline, Pubmed, Embase, Web of Science, Cochrane Collection and ClinicalTrials.gov. No limits placed on language or year of publication. Review conducted in accordance with the PRISMA statement. Searches identified 63 abstracts and 19 full texts. Of these, 9 studies met inclusion criteria reporting outcomes in 66 patients with at least 72 implants. Hearing outcomes were generally good. Mortality secondary to cardiac complications within the follow up period occurred in at least five cases (7.6%), though three of these were thought to be unrelated to surgery. Potentially dangerous arrhythmias without associated morbidity were also noted in at least five patients. The methodological quality of included studies was modest, predominantly consisting of case reports and non-controlled case series with small numbers of patients. All studies were OCEBM grade IV. One study contributed 41/66 patients (62%). Hearing outcomes following CI in JLNS are generally good with the majority of patients experiencing useful hearing improvement. Significant peri-operative cardiac risks exist and should be discussed with the patient and family during pre-operative counselling and prompt thorough investigation, pre-operative optimisation and peri-operative monitoring.
Keywords: Cochlear implantation, cardiac complications, Jervell and Lange-Nielsen Syndrome
INTRODUCTION
Background and Epidemiology
Jervell and Lange-Nielsen syndrome (JLNS) is an autosomal recessive disorder characterized by bilateral sensorineural hearing loss and prolonged QT interval with cardiac dysfunction. It was first described by Anton Jervell and Fred Lange-Nielsen in 1957, highlighting the features of deaf-mutism, syncope, and prolonged QT interval on electrocardiogram[1]. Both auditory and cardiac dysfunction arise from defective potassium channel function. Mutations in the KCNQ1 gene are responsible for 90% of cases, and mutations in the KCNE1 gene are responsible for the remaining 10%[2]. Among those with KCNQ1, two-thirds are homozygous with an autosomal recessive pattern and the remaining one-third are with compound heterozygous mutations[3], which describe the presence of 2 different mutant alleles, 1 on each chromosome. In some reports, approximately 4% of patients with long QT syndromes and KCNQ1 mutations presented without sensorineural hearing loss[4]. This is thought to result from a milder mutation that results in sufficient residual K+ current within the ear to allow normal hearing function but still compromises the cardiac function[4]. Dysfunction of this voltage-gated potassium channel impairs the luminal secretion of K+ from the stria vascularis into the endolymphatic space, which is essential for maintaining the endolymphatic potential[5]. The site of dysfunction within the cochlea, and likely normal auditory nerve, might be expected to predispose to good hearing outcomes in cochlear implantation (CI). The overall incidence of JLNS is estimated at between 1 in 166,000 and 1 in 625,000, with the incidence thought to be notably higher in Scandinavian countries at approximately 1 in 200,000[2]. These figures are likely to be an underestimate of the true prevalence owing to the failure of diagnosis before sudden death because, if untreated, cardiac mortality is likely to exceed 50%[6].
Diagnosis and Cardiac Complications
Jervell and Lange-Nielsen syndrome should be suspected in any child presenting with hearing loss and syncopal episodes. In some centers, electrocardiogram (ECG) recording forms a part of the routine preoperative workup of every child presenting for CI, and it has been suggested that this should form part of the routine protocol in all centers[7]. JLNS is a form of inherited long QT syndrome with a QTc interval of more than 500 ms, although between 10% and 37% of genotype positive patients have a normal QT interval at rest[8]. If untreated, this can lead to Torsade de pointes, a polymorphic ventricular tachycardia, and sudden cardiac death[9]. Other T-wave abnormalities may also be present depending on the channelopathy present[8]. The increased risk of perioperative complications, including death, should be discussed with the parents when weighing the risks and benefits of the surgery[10].
Risks During CI
Typical recommendations may include beta blockers, avoiding sympathetic stimulation, avoidance of anesthetic agents that prolong the QT interval, use of magnesium sulfate, and close access to a cardiac defibrillator with cardiac monitoring during surgery and implant switch on[11]. Some patients will require implantable cardiac defibrillation[12]. Although there are multiple reports of cardiac complications, including deaths, in the perioperative period, it is difficult to quantify the risk owing to the small number of patients in the reported studies[13]. There is widespread awareness of the potential for complications during CI; however, there is a significant variation in practice with respect to preoperative investigations and management[14].
Objectives
In this review, we aimed to look at CI outcomes from JLNS and reported the cardiac risks during implantation and the perioperative considerations.
Population: Children or adults with JLNS
Intervention: CI
Comparison: No comparison group
Outcomes: Preimplantation versus postimplantation audiometric outcomes (where preimplantation outcomes were not available, we looked at only postimplantation audiometric outcomes). Cardiac complications associated with perioperative period in patients receiving CI.
MATERIALS AND METHODS
The study protocol was registered in the PROSPERO prospective database of systematic reviews (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020190621).
Study Inclusion Criteria
Clinical studies of CI in patients with JLNS with hearing outcomes were reported at a minimum of 3 months after implantation. Diagnosis of JLNS may be clinical, because of profound sensorineural hearing loss and prolonged QTc, or genetic. Studies of any experimental or observational design in humans were included. Animal and human studies without the report of postoperative audiometric outcomes or where the abstract or full text was unavailable were excluded.
Search Strategy
In total, 2 reviewers (CM/JM) independently performed the searches and screened the abstracts. The following databases were searched: MEDLINE, PubMed, EMBASE, Web of Science, Cochrane Collection, and ClinicalTrials.gov (via Cochrane). The search terms used were:
“Cochlear Implants”
“Cochlear Implantation”
Cochlear Implant* (title)
1 OR 2 OR 3
“Jervell and Lange-Nielsen”
JLN (title)
JLNS (title)
5 OR 6 OR 7
4 and 8
No limit was placed on language or year of publication.
Selection of Studies
As mentioned, 2 reviewers (CM/JM) independently screened all the records by title and abstract, which were identified from the database searches. Studies describing CI in patients with JLNS were assessed against the inclusion and exclusion criteria, with any disagreement resolved by discussion with a third reviewer. Studies without accessible abstract or full text after the title/abstract screening were followed up by attempting to contact the respective authors. If they were unavailable, the study was excluded. Studies were excluded if they did not report postintervention audiometric outcomes at a minimum of 3 months post-procedure. Studies presenting overlapping populations were limited to the largest study sharing data if it was not possible to disambiguate them. Potentially relevant studies, identified from the initial searches and abstract screening, underwent full-text screening by the 2 independent reviewers before data extraction. Conflicts on the selection were resolved by discussion between the reviewers.
Data Extraction
Data were extracted by the first reviewer (CM) and then checked by the second reviewer (JM). The extracted data were arranged in a spreadsheet (Excel, Microsoft Corp, WA, USA).
Risk of Biased Quality Scoring
The 2 reviewers independently assessed the risk of bias using the Brazzelli risk of bias tool for nonrandomized studies[15]. The studies were also graded according to the Oxford Centre for Evidence Based Medicine (OBECM) grading system[16]. Discrepancies between the reviewers were resolved by discussion.
RESULTS
Searches were initially performed on May 18, 2020 and rechecked on June 18, 2020. A flowsheet detailing the study selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines is included in Figure 1.
Figure 1.
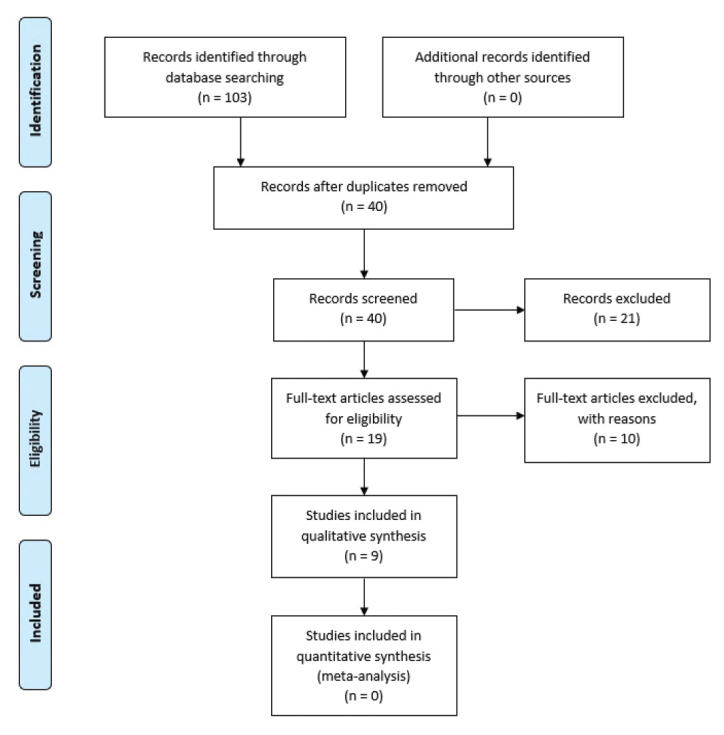
Prisma flow diagram.
Description of Studies
In total, 9 studies met the inclusion criteria with a total of 66 patients and at least 72 implants. There were 6 case series of between 2 and 41 patients and 3 single case reports. All the studies were published between 2002 and 2019. All studies included pediatric patients only, with age at the time of CI ranging from 1 to 6 years; however, the reporting of age was variable, even within the studies. Only 5 studies reported on the type of implant used[17–21]. Moreover, 4 studies reported a genetic analysis for the included patients, 3 of which identified a KCNQ1 mutation[18,20,22], with a further study reporting a homozygous QVLQT1 mutation[17]. The majority of JLNS diagnoses were based on the presence of both profound congenital sensorineural hearing loss and prolonged QTc on ECG. Preoperative radiological assessment of anatomy was only reported in 2 studies; however, it was deemed to be normal in both[17, 20]. Study characteristics are summarized in Table 1.
Table 1.
Study characteristics
| Study | Year | Country | Number of patients | Patient age at implant | Study type | OCEBM* grade |
|---|---|---|---|---|---|---|
| Anto et al. [11] | 2019 | India | 41 | <6y | Retrospective-prospective case series | IV |
| Berrettini et al. [17] | 2003 | Italy | 1 | 3 y | Retrospective case report | IV |
| Broomfield et al. [12] | 2012 | UK | 4 | 24–43 m | Retrospective case series | IV |
| Broomfield et al. [13] | 2013 | UK | 5 | 1 y 11 m–6 y 5 m | Retrospective case series | IV |
| Chorbachi et al. [18] | 2002 | UK | 2 | 2 y 6 m–3 y | Retrospective case series | IV |
| Daneshi et al. [19] | 2007 | Iran | 3 | <4 y | Retrospective case series | IV |
| Kaneshiro et al. [22] | 2018 | Japan | 1 | 2 y | Retrospective case report | IV |
| Siem et al. [20] | 2008 | Norway | 8 | 1 y 11 m–4 y (2 cases not specified) | Retrospective case series | IV |
| Yanmei et al. [21] | 2008 | China | 1 | 3 y | Retrospective case report | IV |
Oxford Centre for Evidence-Based Medicine
Y: years; m: months.
Quality of Studies
The methodological quality of the included studies was modest, predominantly consisting of case reports and non-controlled case series with a small number of patients. All studies were OCEBM grade IV (Table 1). Moreover, 1 study contributed 41/66 patients (62%). All studies were retrospective, except the one by Anto et al.,[11] who specified a retrospective-prospective observational study; however, its exact nature was unclear. Heterogeneity of the audiological outcomes precluded a meta-analysis. There were also limitations in reporting of the implant used, surgical technique, and rehabilitation protocols. Furthermore, 2 studies were included by the same author from the same cochlear implant unit[12,13]; therefore, it is assumed that there was some duplication of the included patients.
Audiological Outcomes
Hearing outcomes were generally good across all the studies; however, their reporting was heterogeneous both in terms of assessment method and follow-up duration as may be expected because all patients were children under the age of 6 years. All but one study reported on preimplantation hearing status with all cases having at least severe to profound bilateral hearing loss. In total, 3 studies used Categories of Auditory Performance (CAP) and Speech Intelligibility Ratings (SIR) to report the outcomes after implantation. The study by Anto et al.[11] was the only study to incorporate a statistical analysis comparing pre- and postimplantation CAP/SIR scores, demonstrating a significant improvement[11]. The remaining 2 studies reported high CAP/SIR scores after implantation[19,21]. In addition, 4 studies reported pure-tone thresholds after implantation, with average thresholds ranging from 26.3 dB to 45 dB[17,18,21,22]. Siem et al.[20] utilized the LittlEARS score[23] for children under 2 years (3 patients), demonstrating scores of 32–34 out of 35. For the four older patients in the study the Rikshospitalet-Radiumhospitalet Medical Center speech perception test was used, yielding comparable outcomes to the mean for the entire population of children undergoing CI at that center. Broomfield et al. [12,13] varied their reporting across the 2 studies; 1 study[12] utilized a descriptive analysis, reporting full-time implant use for all patients. Their second study[13] reported speech reception scores of 6/6 for 3 patients, noting that all were communicating using speech. As discussed, it is possible that there was an overlap between the patient populations in these 2 studies. Audiological outcomes are summarized in Table 2.
Table 2.
Audiological outcomes
| Study | Preoperative data | Postoperative data | Follow-up |
|---|---|---|---|
| Anto et al., 2019[11] | All profoundly deaf | Significant improvement in CAP (p=0.000, ANOVA F=73.928) and SIR (p=0.001 and ANOVA F=7.883) scores at 3 and 6 m | 6 m |
| Berrettini et al., 2003[17] | COR and BAEPs confirmed profound HL. Subsequent play audiometry revealed average air conduction threshold of 110 dB HL from 0.5–2 kHz (No aids). | Italian-language speech perception test for children-open-set word recognition score of 95%, an open-set phrase recognition score of 100%, and a phrase comprehension score of 100%, (no lip reading). PTA average air conduction threshold 28 dB HL (0.5–2 kHz) | 18 m |
| Broomfield et al., 2012[12] | Case 1- ABR 90 dB in the right ear and 60 dB in the left ear in the low frequencies, with no response from either side in the high frequencies. Case 2- Failure to progress with hearing and language development. Case 3- Profound HL on ABR Case 4- Failure to progress with hearing aids |
Case 1- Initial results were excellent, with full-time implant use, environmental awareness of dogs, passing cars and doors closing, and early signs of language development. Case 2- Initial results were excellent, with full-time implant use and good speech development. Case 3- Full-time implant user more than 5 years after her surgery Case 4- Good implant user with no problems |
4–5 y |
| Broomfield et al., 2013[13] | None | SRS- 6/6 (3 patients). All communicate with speech | 60–180 m |
| Chorbachi et al., 2002[18] | Case 1- Profound hearing loss. PTA >90 dB at 500 Hz–4 kHz Case 2- Profound hearing loss. PTA >90 dB at 250 Hz+ |
Case 1- PTA 35–45 dB Case 2- PTA 35–40 dB |
8–10 y |
| Daneshi et al., 2007[19] | Case 1- Profound, congenital hearing loss Case 2/3- Severe to profound hearing loss, failure to benefit from hearing aid |
All cases at 48 months- CAP 6/7, SIR 4/5 | 4 y |
| Kaneshiro et al., 2018[22] | ABR absent on both sides at 105 dB nHL | PTA average 26.3 dB HL in a free-field condition, speech discrimination score 90%. | 9 y |
| Siem et al., 2008[20] | Profound HL on ABR and TEOAE | LittlEARS score for 3 patients (out of 35)- 33, 32, and 34 Rikshospitalet-Radiumhospitalet Medical Center speech perception test for 4 patients- 8,9,5,4. Compared to mean for 213 other CI children at center (6.32 SD 2.22) | 1–4 y |
| Yanmei et al, 2008[21] | Free-sound audiometry, ABR, and auditory steady-state response revealed bilateral, severe to profound, sensorineural hearing loss. CAP 0, SIR 1 | CAP 7/7, SIR 5/5 at 36 m postoperative PTA thresholds >40 dB | 3 y |
ABR: auditory brainstem response; CAP: category of auditory performance; SIR: speech intelligibility rating; PTA: pure-tone audiogram; SRS: speech reception score; TEOAE: transient evoked otoacoustic emission; COR: conditioned orientated reflex; BAEP: brainstem auditory evoked potential; HL: hearing loss; m: months; y: years; SD: standard deviation.
Surgical Outcomes
In total, 7 studies reported no surgical complications. Siem et al.[20] reported an infection, which was successfully treated with antibiotics. Broomfield et al.[12] also reported an infection; however, this was following a minor head injury and scalp laceration 2 months after implantation. Unfortunately, this infection did not respond to antibiotics and required explantation at 6 months. They also reported a spontaneous device failure requiring reimplantation.
Cardiac Precautions and Complications
Cardiac complications leading to death within the follow-up period occurred in at least 5/66 patients (7.6%); however, only 2 of these were thought to be directly related to surgery (3%). Anto et al.[11] also noted that 5/41 (12.2%) patients exhibited a potentially fatal cardiac arrhythmia during their surgery, which required pacing; however, they reported no cardiac deaths. Preoperative cardiac optimization was common, with 7 studies reporting use of beta-blocker medication[11,12,17,19,DI]. At least 8 patients had either a pacemaker or an implantable cardioverter-defibrillator device fitted; however, it was not always clear whether this was done pre or postoperatively. Chorbachi et al.[18] reported no specific cardiac precautions perioperatively and had no cardiac complications in their 2 patients. Cardiac precautions and complications are reported in Table 3. An algorithm, specifically for the perioperative management of patients with long QT during CI, has been produced on the basis of a large series of cases from a tertiary unit, although no hearing outcomes were available from this study [24].
Table 3.
Cardiac considerations
| Study | Number of patients | Preoperative cardiac precautions | Cardiac complications |
|---|---|---|---|
| Anto et al., 2019[11] | 41 | Preoperative beta blockade, electrolyte optimization, cardiac monitoring, cardiology review | A total of 12.2% patients had potentially fatal arrhythmia requiring pacing. No deaths |
| Berrettini et al., 2003[17] | 1 | Preoperative beta blockade, cardiac monitoring | Nil |
| Broomfield et al., 2012[12] | 4 | 2 case- Preoperative beta blockade and ICD, 2 cases nil. | Nil around CI surgery; 1 death following GA for explant secondary to infection; 1 cardiac death unrelated to surgery |
| Broomfield et al., 2013[13] | 5 | Not specified | 1 death related to anesthetic. |
| Chorbachi et al., 2002[18] | 2 | Nil | Nil |
| Daneshi et al., 2007[19] | 3 | Beta blockade, cardiac monitoring | Nil |
| Kaneshiro et al., 2018[22] | 1 | Beta blockade | Nil perioperatively. Subsequent arrhythmias requiring ICD |
| Siem et al., 2008[20] | 8 | 7/8 cases treated with beta blocker, 5/8 pacemaker. Not specified whether preoperative or not in some cases |
Nil perioperatively; 2 cardiac deaths unrelated to surgery |
| Yanmei et al., 2008[21] | 1 | Beta blockade, temporary pacemaker, cardiac monitoring | Nil |
ICD: implantable cardioverter-defibrillator; CI: cochlear implantation; GA: General Anaesthetic.
DISCUSSION
Clinical and Research Consequences
This systematic review and narrative synthesis reports on the outcomes of CI in profoundly deaf children diagnosed with JLNS. To the authors’ knowledge, this is the first systematic review on this topic. There was a trend toward good audiological outcomes in all the studies, with the majority of patients receiving benefit. Although most studies focused on either pure-tone audiograms or speech perception postoperatively, favorable speech intelligibility was also reported. These findings are in line with the underlying cause of impairment being inadequacy of intracochlear K+ current flow rather than within the auditory nerve, which bypasses the dysfunctional area by direct electrical stimulation of the auditory nerve. In addition to the included studies, 2 further studies were identified which, although not reporting specific audiological outcomes or follow-up duration, did report successful implant use with JLNS in 5 patients[25,26]. Siem et al. were also able to demonstrate that speech perception outcomes in JLNS are comparable with the speech perception scores in a wider group of patients with implants. Similarly, Broomfield et al. reported comparable speech reception scores in JLNS compared with other patients with implants, with other genetic syndromes, such as Usher, Waardenburg, and Pendred. Only 2 studies reported specifically on preoperative imaging, noting normal anatomy in 9 patients with JLNS; however, nothing in the included studies suggested that surgery was any more technically demanding in patients with JLNS than other populations.
Although audiological outcomes after CI appear to be favorable in JLNS, the potential for cardiac complications is significant, both perioperatively and in general. Optimal management starts with the initial diagnosis of JLNS, which may not be made until after CI, which was the case in some of the included studies. Therefore, given the low cost, potential for discovering other abnormalities, and potentially catastrophic risks of missing a significant cardiac problem, ECG has been recommended as a part of the workup for all patients being assessed for CI (unless there is any other known genetic cause), where a prolonged QTc should prompt a diagnosis of JLNS[27,28]. This will facilitate cardiac optimization preoperatively and hopefully reduce the risk of complications. Moreover, the risk of cardiac death, if untreated, is thought to be as high as 50%[6]. An overarching theme from included studies is that a multidisciplinary approach is required to optimize the patients preoperatively. This includes a close liaison between anesthetist, cardiologist, and ear-nose-throat surgeon. Anto et al.[11] summarized a number of measures taken to minimize the cardiac risk perioperatively, including cardiac monitoring, preoperative beta blockade, and the avoidance of drugs that further prolong the QT interval. Even with these precautions, they reported a potentially fatal cardiac arrhythmia in 12.2% of their patients intraoperatively; however, there was no associated mortality. In extremely symptomatic children who fail to respond to beta-blocker therapy, an implantable cardioverter-defibrillator device or temporary pacing device may be required before CI. There are also considerations during switching the device on, which should be performed with cardiac monitoring and a defibrillator on hand to reduce the chance of death should an arrhythmia be precipitated[11]. There were no reported events of cardiac arrest during device switch on in the included studies. Kaneshiro et al.[22] reported no detrimental effects on hearing outcomes and the implanted device, even in a patient who underwent multiple defibrillations in the years after implantation.
The perioperative CI-specific cardiac mortality of 3% in the included studies may be helpful for preoperative counseling of the patients and their families. However, given the predominance of case reports and small-volume case series within published studies, there may be a significant reporting bias in the available literature. Reporting of negative outcomes may have been avoided to prevent embarrassment to the implant center. Conversely, a death, which is very rare among implant procedures and indeed among operations in Otolaryngology in general, may prompt a center to report a case and uneventful cases go unreported. Similarly, the variation in preoperative cardiac management also makes it difficult to draw conclusions as a whole. The relatively small sample of reported cases also raises questions regarding the validity of pooled results. This would best be addressed by large-scale mandatory registries of implantation recipients and results, particularly useful for such types of rare diseases. Such registries are not yet in use, but the proliferation of electronic patient records and increased interest in outcome measures is likely to drive this adoption. Although a number of challenges exist in the implementation of national registries, including oversight, funding, and legal implications, there are trends toward the development of such a database for CI[29,30]. Additionally, a more standardized approach to reporting of outcomes, including pre and postoperative audiology, would facilitate the synthesis of a wider pool of data and provide opportunities to assess the outcomes more accurately on a larger scale.
CONCLUSION
Hearing outcomes after CI in JLNS are generally good with the majority of patients experiencing a benefit, both in terms of speech perception and speech intelligibility. Significant perioperative cardiac risks exist and should be discussed with the patients and their family during preoperative counseling, and prompt and thorough investigation, preoperative optimization, and perioperative monitoring should be carried out. Profoundly deaf patients may present for cochlear implant assessment without symptoms or a formal diagnosis of JLNS; therefore, cochlear implant teams must be aware of their important diagnostic role and ensure that an ECG is included as a mandatory part of the preoperative assessment.
MAIN POINTS.
Hearing outcomes following cochlear implantation in patients with JLNS are generally good.
Significant cardiac risk may be involved and clear discussion and counselling and peri-operative workup are important.
Electrocardiography should be a mandatory part of pre-operative workup.
Footnotes
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – M.B., J.M., P.M..; Design – M.B., J.M., P.M., C.M.; Supervision – M.B., P.M.; Resource – J.M.; Materials – J.M., M.B.; Data Collection and/or Processing – C.M., J.M.; Analysis and/or Interpretation – C.M., J.M., P.M., M.B.; Literature Search – C.M., J.M.; Writing – C.M., J.M.; Critical Reviews – M.B., P.M.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Jervell A, Lange-Nielsen F. Congenital deaf-mutism, functional heart disease with prolongation of the Q-T interval and sudden death. Am Heart J. 1957;54:59–68. doi: 10.1016/0002-8703(57)90079-0. [DOI] [PubMed] [Google Scholar]
- 2.Tranebjærg L, Samson RA, Green GE. Jervell and Lange-Nielsen Syndrome. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJ, Stephens K, et al., editors. GeneReviews® [Internet] Seattle (WA): University of Washington, Seattle; 1993. [cited 2020 Jun 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1405/ [Google Scholar]
- 3.Schwartz PJ, Spazzolini C, Crotti L, Bathen J, Amlie JP, Timothy K, et al. The Jervell and Lange-Nielsen syndrome: natural history, molecular basis, and clinical outcome. Circulation. 2006;113:783–90. doi: 10.1161/CIRCULATIONAHA.105.592899. [DOI] [PubMed] [Google Scholar]
- 4.Giudicessi JR, Ackerman MJ. Prevalence and potential genetic determinants of sensorineural deafness in KCNQ1 homozygosity and compound heterozygosity. Circ Cardiovasc Genet. 2013;6:193–200. doi: 10.1161/CIRCGENETICS.112.964684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Neyroud N, Tesson F, Denjoy I, Leibovici M, Donger C, Barhanin J, et al. A novel mutation in the potassium channel gene KVLQT1 causes the Jervell and Lange-Nielsen cardioauditory syndrome. Nat Genet. 1997;15:186–9. doi: 10.1038/ng0297-186. [DOI] [PubMed] [Google Scholar]
- 6.Bitner-Glindzicz M, Tranebjaerg L. The Jervell and Lange-Nielsen syndrome. Adv Otorhinolaryngol. 2000;56:45–52. doi: 10.1159/000059080. [DOI] [PubMed] [Google Scholar]
- 7.Scott-Warren V, Bendon A, Bruce IA, Henderson L, Diacono J. Cochlear implantation in children with congenital long QT syndrome: Introduction of an evidence-based pathway of care. Cochlear Implants Int. 2018;19:350–4. doi: 10.1080/14670100.2018.1518686. [DOI] [PubMed] [Google Scholar]
- 8.Priori SG, Schwartz PJ, Napolitano C, Bloise R, Ronchetti E, Grillo M, et al. Risk stratification in the long-QT syndrome. N Engl J Med. 2003;348:1866–74. doi: 10.1056/NEJMoa022147. [DOI] [PubMed] [Google Scholar]
- 9.Pabba K, Chakraborty RK. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2020. Jervell and Lange Nielsen Syndrome. [cited 2020 Jun 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK537300/ [PubMed] [Google Scholar]
- 10.Goldenberg I, Moss AJ, Peterson DR, McNitt S, Zareba W, Andrews ML, et al. Risk factors for aborted cardiac arrest and sudden cardiac death in children with the congenital long-QT syndrome. Circulation. 2008;117:2184–91. doi: 10.1161/CIRCULATIONAHA.107.701243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Anto R, Maheswari S, Vadivu S, Kameswaran M. Cochlear Implantation in Congenital Long-QT Syndrome: A Comprehensive Study. J Int Adv Otol. 2019;15:352–7. doi: 10.5152/iao.2019.7404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Broomfield SJ, Bruce IA, Henderson L, Ramsden RT, Green KMJ. Cochlear implantation in children with Jervell and Lange-Nielsen syndrome - a cautionary tale. Cochlear Implants Int. 2012;13:168–72. doi: 10.1179/1754762810Y.0000000006. [DOI] [PubMed] [Google Scholar]
- 13.Broomfield SJ, Bruce IA, Henderson L, Ramsden RT, Green KMJ. Cochlear implantation in children with syndromic deafness. Int J Pediatr Otorhinolaryngol. 2013;77:1312–6. doi: 10.1016/j.ijporl.2013.05.022. [DOI] [PubMed] [Google Scholar]
- 14.Kang SL, Jackson C, Kelsall W. Electrocardiogram screening of deaf children for long QT syndrome: are we following UK national guidelines? J Laryngol Otol. 2011;125:354–6. doi: 10.1017/S0022215110002379. [DOI] [PubMed] [Google Scholar]
- 15.Brazzelli M, Cruickshank M, Tassie E, McNamee P, Robertson C, Elders A, et al. Collagenase clostridium histolyticum for the treatment of Dupuytren’s contracture: systematic review and economic evaluation. Appendix 4 Risk-of-bias checklist: non-randomised comparative studies. Health Technol Assess Winch Engl. 2015;19:1–202. doi: 10.3310/hta19900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2 [Internet] Oxford Centre for Evidence-Based Medicine; Available from: https://www.cebm.net/index.aspx?o=5653. [Google Scholar]
- 17.Berrettini S, Forli F, Ursino F, Franceschini SS. Cochlear implant in Jervell and Lange-Nielsen syndrome. Audiol Med. 2003;1:224–7. doi: 10.1080/16513860310001924. [DOI] [Google Scholar]
- 18.Chorbachi R, Graham JM, Ford J, Raine CH. Cochlear implantation in Jervell and Lange-Nielsen syndrome. Int J Pediatr Otorhinolaryngol. 2002;66:213–21. doi: 10.1016/S0165-5876(02)00181-7. [DOI] [PubMed] [Google Scholar]
- 19.Daneshi A, Ghassemi MM, Talee M, Hassanzadeh S. Cochlear implantation in children with Jervell, Lange-Nielsen syndrome. J Laryngol Otol. 2008;122:314–7. doi: 10.1017/S0022215107007712. [DOI] [PubMed] [Google Scholar]
- 20.Siem G, Früh A, Leren TP, Heimdal K, Teig E, Harris S. Jervell and Lange-Nielsen syndrome in Norwegian children: aspects around cochlear implantation, hearing, and balance. Ear Hear. 2008;29:261–9. doi: 10.1097/AUD.0b013e3181645393. [DOI] [PubMed] [Google Scholar]
- 21.Yanmei F, Yaqin W, Haibo S, Huiqun Z, Zhengnong C, Dongzhen Y, et al. Cochlear implantation in patients with Jervell and Lange-Nielsen syndrome, and a review of literature. Int J Pediatr Otorhinolaryngol. 2008;72:1723–9. doi: 10.1016/j.ijporl.2008.07.013. [DOI] [PubMed] [Google Scholar]
- 22.Kaneshiro S, Hiraumi H, Shimamoto K, Sasamori K, Kobayashi Y, Sato H. Cochlear implant function in a patient with Jervell and Lange-Nielsen syndrome after defibrillation by countershock. Auris Nasus Larynx. 2018;45:890–3. doi: 10.1016/j.anl.2017.11.017. [DOI] [PubMed] [Google Scholar]
- 23.Coninx F, Weichbold V, Tsiakpini L, Autrique E, Bescond G, Tamas L, et al. Validation of the LittlEARS((R)) Auditory Questionnaire in children with normal hearing. Int J Pediatr Otorhinolaryngol. 2009;73:1761–8. doi: 10.1016/j.ijporl.2009.09.036. [DOI] [PubMed] [Google Scholar]
- 24.Anto R, Maheswari S, Vadivu S, Kameswaran M. Cochlear Implantation in Congenital Long-QT Syndrome: A Comprehensive Study. J Int Adv Otol. 2019;15:352. doi: 10.5152/iao.2019.7404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Eftekharian A, Mahani MH. Jervell and Lange-Nielsen syndrome in cochlear implanted patients: our experience and a review of literature. Int J Pediatr Otorhinolaryngol. 2015;79:1544–7. doi: 10.1016/j.ijporl.2015.07.012. [DOI] [PubMed] [Google Scholar]
- 26.Green JD, Schuh MJ, Maddern BR, Haymond J, Helffrich RA. Cochlear implantation in Jervell and Lange-Nielsen syndrome. Ann Otol Rhinol Laryngol Suppl. 2000;185:27–8. doi: 10.1177/0003489400109S1211. [DOI] [PubMed] [Google Scholar]
- 27.Lin JW, Chowdhury N, Mody A, Tonini R, Emery C, Haymond J, et al. Comprehensive diagnostic battery for evaluating sensorineural hearing loss in children. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol. 2011;32:259–64. doi: 10.1097/MAO.0b013e31820160fa. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Morzaria S, Westerberg BD, Kozak FK. Evidence-based algorithm for the evaluation of a child with bilateral sensorineural hearing loss. J Otolaryngol. 2005;34:297–303. doi: 10.2310/7070.2005.34501. [DOI] [PubMed] [Google Scholar]
- 29.Mandavia R, Knight A, Phillips J, Mossialos E, Littlejohns P, Schilder A. What are the essential features of a successful surgical registry? a systematic review. BMJ Open. 2017;7:e017373. doi: 10.1136/bmjopen-2017-017373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mandavia R, Knight A, Carter AW, Toal C, Mossialos E, Littlejohns P, et al. What are the requirements for developing a successful national registry of auditory implants? A qualitative study. BMJ Open. 2018;8:e021720. doi: 10.1136/bmjopen-2018-021720. [DOI] [PMC free article] [PubMed] [Google Scholar]