

Abstract
The development of in vitro fertilization (IVF) in the UK, in 1978, proved a major breakthrough in the process of human reproduction, which had remained constant in human history. The impact of IVF and the ensuing assisted reproductive technologies (ARTs) has not been limited in revolutionizing the “natural” practice of biological reproduction, but has reached out to and affected almost every institution in society. Family and kinship, as the social expression of reproduction and the institutions which are the most transparently structured realm of human life are those most profoundly affected by ARTs. Although literature on the implications of ARTs is in general abundant, this article presents new insights on their impact on family and kinship in Iran, which remains a unique case in the Muslim world. It explores the particular way ARTs, especially third-party donation, have been endorsed and practiced in Iran, and their consequences for the family, the infertile individuals, and their position vis-à-vis their kin and social group. The conclusion points to the lack of clarity concerning the initial rulings by the Islamic jurists, who allowed the practice of ARTs, and which has led to a number of unintended consequences regarding the legal, religious, cultural, and ethical issues, affecting the family, its structure and the relationship between the kin group. These consequences range, inter alia, from the question of the anonymity of third-party donor, to the permissibility of gamete donation between blood relatives, and to the absence of enforceable legislation.
Keywords: Family, Infertility, Kinship, Third party reproduction
Introduction
The biological process of human reproduction, which had remained constant throughout the history, witnessed a major breakthrough in 1978 in the form of the development of in vitro fertilization (IVF) technology in the UK and the birth of the first IVF baby, Louise Brown. IVF technology rapidly led to the emergence of various assisted reproductive technologies (ARTs) and their spread around the globe. These technologies have revolutionized the “natural” way people have reproduced by enabling the infertile couples to conceive and the fertile couples to access a wide range of reproductive choices. At the same time, ARTs have proved a potential challenge to the traditional carved-in-stone reproductive norms and practices. IVF, a scientifically advanced technology in 1978 and now a routine medical treatment, has acted as the instigator of a process that has opened up unimaginable possibilities in the way humans reproduce now. These innovations continue to emerge and alter the biological reproductive functioning of their users at an alarming speed. In reality, ARTs have recast the way humans reproduce and as Bamford points out “It is now possible to artificially create in a clinic what was previously understood to be the province of innate biology” (1).
However, reproduction goes beyond two people reproducing biologically, or otherwise, and is a dynamic process, which interacts closely with other social institutions and is determined by a combination of biological, environmental, and social factors (2). As Ginsburg and Rapp explain, “by using reproduction as an entry point into the study of social life and placing it in the centre of social theory, we can see how cultures are produced, contested, and transformed as people imagine their collective future in the creation of the next generation” (3). Robertson also defines reproduction “[as ..] a relentless force in our lives, adding to and subtracting from the people around us, and obliging us to change our relationships with each other and with the wider world. It is a persistent strategic challenge, the outcome of which is as important for society as for the person in each household” (4). Finally, Kligman links reproduction to its broader context as follows “[reproduction is …] fundamentally linked with identity, whether of the nation, the state, the family, the lineage, or the individual” (5). Nonetheless, of all the social institutions surrounding reproduction, it is the family and kinship that more directly affect reproduction and remain at its heart. It then follows that any changes in the way humans reproduce will have a direct impact on family and kinship as confirmed by Bamford: “Technological conceptions pay attention to the way in which innovation in science and technology along with reproductive medicine have impacted how kinship is created and experienced” (5)
The possibility of conceiving through ARTs, more specifically from a third-party, has provoked different reactions in different cultures which have received and interpreted them to befit their own reproductive norms and practices. As Unnithan-Kumar points out “[Reproductive] technologies in themselves do not bring about social transformation but it is in how they are made socially meaningful that their power lies” (6). In some cultures, ARTs have weakened or even reversed the existing reproductive norms and values and restructured the family from its conventional form. For example, in some cultures, the structure of the traditional family has been dramatically transformed from the union of a married heterosexual couple and their biological children to single unmarried women or homosexual couples who reproduce by resorting to gamete from a third-party. In such cases, the new family could consist of an unmarried single mother with a child from a donor sperm, or two homosexual men having children with the help from surrogate mothers, or two lesbian women conceiving using donor sperm. The impact of these emerging forms of family extends beyond the relationship between the immediate parents and their offspring and involves and affects the generation of grandparents and the wider kin group in a variety of ways. Interestingly, in those cultures, where deviation from the traditional form of family, consisting of a married heterosexual couple and their children, is not an option, ARTs have helped reinforce the status quo. They have helped remove the stigma of infertility and strengthened the stability of the marriage and the family. These cultural variations are encapsulated in what Inhorn and Van Ballen define as “[reproduction is]….a biological phenomenon that is socially constituted and culturally variable through space and time” (7).
While conceiving through IVF between a couple can be viewed as a medical technology and does not affect the social and cultural norms and values, and taboos attached to procreation, resorting to a third-party gamete has had different social and cultural implications, wherever it has been practiced. Introducing a stranger’s gamete to conceive has the potential of disrupting the biological continuity and, inevitably, leads to a redefinition of what is “biological” and what is “social” as far as family and kinship are concerned. In such situation, the terms of relatedness and the boundaries of the interaction between wives and husbands, siblings, parents and children, relatives and strangers, and generally the wider kin group, shifts and is redefined. According to Bamford “Studies of ARTs have contributed to the field of kinship studies and have precipitated a radical requestioning of what it means to be related to other persons. These studies often deal with not only ARTs, but also with the challenges that often accompany family-making in an increasingly globalized world” (1). Hampshire and Simpson go further by emphasizing that “In their effect, ARTs are not simply grafted onto stable forms of family and kinship but are themselves part of the shifting mosaic or relationality in everyday life” (8), and “…as such, ARTs pose significant challenges to prevailing ethical, legal and religious orthodoxies. Not least of these challenges is the potential commoditisation of gametes and embryos, which threaten to dislodge these substances from their position within existing schemes of meaning and value” (8).
A substantial body of literature exists on the social and cultural implications of ARTs on family and kinship, illustrating the variations mentioned earlier (3, 7, 9–18). As these studies have shown, the application of ARTs continues to affect family forms and kinship more than any other institution in society. However, views of scholars were initially divided on the impact of ARTs on kinship. For example, Strathern (10, 11) argues that the choices the consumers of these technologies make have led to “destabilizing” nature in European kinship. On the other hand, Susan Kahn’s studies of Jewish communities shows a contrasting example to such argument (19). Finally, Parkin and Stone (17) offer a different outcome namely that “new constructions of kinship are occurring in European and American society and in this process choice is playing a larger role, there is at the same time a counter-current drawing Americans back to biogenetic conceptions of kinship”. Inhorn (18) and Clarke’s (20) more recent studies of ARTs in the Muslim Middle East throw a different light on what constitutes kinship in Islamic societies. Clarke argues that “According to the vision of the Islamic legal establishments, relations of filiation (nasab), are not mutable or fluid, but are given, paradigmatically–but not exclusively-through procreation”. Clarke’s analysis clearly distinguishes the notions of the Islamic relatedness from the Euro-American ones and its place and association in relation to the application of ARTs (21, 22).
The diversity of the cultural responses to ARTs is, therefore, a culmination of the interaction between social, political, legal, ethical and religious institutions in different cultures, determining the structure of the family and concepts of relatedness. To illustrate some of the points argued earlier, the impact of ARTs on family and its structure was explored in Iran, which provided fertile ground for such examination. An attempt was made to investigate the extent to which the structure of the family has been both potentially and actually affected, and whether and how the relationship between the family members and that of the kin group has been altered in both positive and negative ways. Iran, a Shia Muslim country, together with Lebanon’s Shiite-majority areas, presents a unique case among the Muslim countries. Both countries allow the use of ARTs in all their forms, whereas the Sunni Muslim countries have banned third-party gamete donation and only allow IVF between a married couple (18, 23). However, Iran also differs from those countries where ARTs are practiced in all their forms, by forbidding conception outside the marital union or by homosexual couples (Homosexuality is forbidden and illegal by the Islamic law).
In this article, an attempt was made to examine how the flexibility involved in the legitimization of third-party gamete donation in Iran has resulted in creating stability and happiness for many families. Also, several examples were provided which indicate such flexibility has led to unintended consequences on the structure of the family and the relationship between the kin group. Moreover, an emerging phenomenon was explored which is increasing among the infertile couples and that is their “transition” from being “infertile” to appearing to be “fertile” and thus dispelling the stigma of infertility.
The background: Infertility and sterility treatment by in vitro fertilization (IVF) and through gamete or embryo donation is one of the most phenomenal technological achievements in the second half of the twentieth century. It seems that these technological advancements provide a basis for the continuity and protection of the family. They lead into increased harmony and affection, and result in closer relationship between infertile couples (24). At the same time, they introduce new forms of relatedness between the resulting child and parents whose genetic make-up is different from one or both of the parents, being the recipients of gamete or the recipients of donated embryo. The impact of donor technologies in cultures with closely-knit kinship networks can result in intense negative effects on the relationship between the couple, the parents and the child, the siblings and relatives, and will lead to undesirable and difficult situations for all involved (25, 26). Application of new methods involved in infertility treatment such as in vitro gametes through stem cells (27, 28), embryo manipulation and preimplantation genetic diagnosis (29), uterus transplantation (30), ovarian transplantation (31) and, spermatogonial stem cell transplantation (32) have led to further complications in the relationship between the members of the kin group. Additionally, further development of ART treatments, in cases such as extending the right to adoption 1 for individuals in countries such as Iran (33) or using third-party donation for couples with genetic defects leading into abortion or birth of disabled children (34) are also conducive to additional problems (35). As a result, the use of these reproductive technologies has led to occurrence of families, where the children have one or more genetic parents which are different from the infertile couple’s genes. This has drastically changed the structure of the traditional family and promoted new forms of families (36). The reality is that ART has opened up a wide range of possibilities for the recipients of gamete and their choice of treatment. Such possibilities result in new forms of “social” kinship and relatedness which is different from “biological” one. This new form of relatedness can be influenced by different institutions in society such as religion (37).
A majority of infertile and sterile couples find the use of third-party-assisted treatments a desirable and viable alternative. Pursuing it secretly enables them to conceal the infertility and to elude from social pressure and stigmata of infertility (38). To obtain these treatments, couples overcome cultural, moral belief, or legal restrictions by using means such as receiving the treatment in a different city or country (39).
The focus of this article remained mainly on the changes brought about by the ART revolutions on the structure of the family and kinship in Iran. Iran is a country where cultural and religious beliefs jointly have played an important role in legalizing ART treatments and changing decision-making process of infertile couples (40).
The legitimization of ARTs in Iran: Third-party reproduction (Donation) is acceptable in Iran and the Lebanon’s Shiite-majority areas, but forbidden (Haram) in other Muslim countries (18, 41). Third-party reproduction has been legitimized in Iran following the jurisprudential views driven from the Shia School in Islam. Compared to other ideologies, Shia is more welcoming to new science and technology. The third-party reproduction has been allowed in Iran in most of its forms through the endorsement of the Islamist jurists (For embryo, a law has also been passed). The permissibility of third-party donation has resulted in fundamental changes in the make-up and structures of families (40).
Prior to the introduction of ART, the traditional family was an extended family, structured as a socio-economic unit of the producer and the consumer. The family was kinship-oriented, with a reproduction purpose focused on creating a large family, with no fertility control. However, the family has now evolved into a nuclear one, changing into a consumer unit and characterized by a smaller circle of relatives, controlled reproduction, and a smaller family size (42). The family consists of the formal and legal union between a man and a woman and their children, who are the biological outcome of the couple’s relationship. Any child born out of wedlock is considered illegitimate (Valad e zena or born of incest). In Islamic law, marriage is legitimate only between the two sexes (Ruum Sura, verse 21) 2, who are not religiously intimate people (Namahram) (Nissa Sura, verse 23) 3, and thus in-law relationships are formed between men and women through marriage with a new intimate circle 4 (Mahram). Such prohibition of marrying one’s mahram group of relatives effectively forbids marriage between close biological relatives (See below the list of close relatives with whom marriage is forbidden).
Within the Iranian culture and society, conception can only take place within marriage and a legally formed union. The resulting biological children then take their lineage from both their parents. Nevertheless, kinship ties are not limited to the biological family and go beyond the relatedness which is based on bloodline alone. There are a number of other social links and relationships, which also constitute kinship. For example, in Islam, breastfeeding a child can result in what is referred to as milk kinship (Rezaie) between the child and the milk mother. Such relatedness extends to the woman’s direct members of her family too and the same rules of marriage between the mahram and na’mahram also applies to them (40, 43, 44). Other forms of social connections include a wide range such as foster children, stepchildren, offspring adoption, and the children resulting from ART. In latter cases, although according to the rules that legitimized third-party donation, the donor children born from gamete or embryo donation belong to their biological parents, they start life in the infertile couples’ families from conception till birth. These children’s biological links (Nasab) are disrupted with one or both parents, which changes the interaction between the two parties and brings to the fore the question of intimacy (Mahramiat) of the relatives to each other, and creates new families, which are socially, and not biologically related to each other.
The role of evolution in the emergence of new family structures: The above alterations in the nature of relatedness in the family stem from the reproductive technologies, which have revolutionized the traditional forms of relatedness within the family. A prominent characteristic of the technological revolution is the development of science, knowledge, and technology and their employment in a growing feedback circle between innovation and its applications. The feedback circle between new technology areas takes place very swiftly (Especially in biological sciences) despite confronting cultural, social, and religious barriers (45). Iran is no exception and has provided the means to have children beyond the natural fertilization process during the past three decades and even out of the natural biologic path using third-party assisted reproductive methods (46). The diversity of these technologies, including donated gametes, surrogacy, and embryo donation, makes this therapeutic potential prevalent in the society. Due to this diversity, the recognized and accepted nuclear biological family, as the only and fundamental form of reproduction, is subjected to dramatic changes.
Global figures on third-party reproduction: People who use third party reproduction are mainly those suffering from sterility, which can be due to the late marriage and childbearing (47), the absence or defect in one or both gametes (Eggs, sperm), absence of uterine, medical prohibition for the potential mother, unknown infertility, recurrent miscarriages, and the probability of defective off-spring. According to the World Health Organization, 12–15% of the couples (48) are infertile, which is more than one quarter of married women of childbearing age. In 2013, in the United States, only 1% of all births was done by IVF/ICSI and 10% of these pregnancies resulted from donated eggs (49). Reports show increasing interest in using these methods. An official US report in 2014 indicated that 9.82% of treatment cycles used donated eggs or embryos (50). Another report from European Society of Human Reproduction and Embryology shows that in a 15-year period (1997–2011), about 6 million infertility treatment cycles were implemented in Europe and about 23% of these treatment cycles used donated sperms, oocytes or embryos. Meanwhile, Iran’s comprehensive national infertility assessment in 2013 revealed that the prevalence of the primary infertility was above the global average (20.2%) (51). There is no accurate statistical report of the number of births due to infertility treatment and donation in Iran. Based on similar report in Europe and USA, it can be predicted that 20% of the cycles, i.e., about 12000 out of 60000 pregnancies in 2015 was due to third-party treatment.
Diversity of structure and problems of ART families: The diversity and rapid development of third-party reproduction resulted in the creation of a variety of family structures, depending on how these technologies have been used and by whom. A brief mention of these technologies is as follows:
IVF/ICSI: In this method, sperm is injected into the oocyte, and the embryo resulting from this technology is transferred into the mother’s uterus (Section A, Figure 1).
Figure 1.
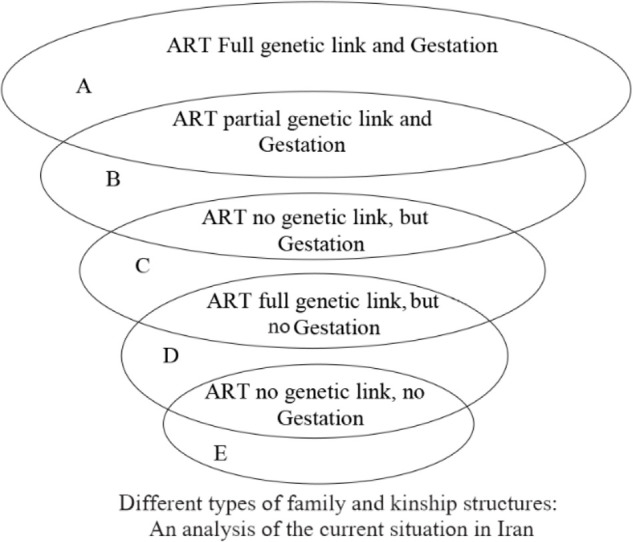
Natural fertilization (Circle A), Fertilization with the aid of ART (Circle B), Fertilization and the pregnancy occurs using a third person’s sperm/oocyte (Circle C), Pregnancy with the couple’s sperm or oocytes when a surrogate mother is used (Circle D), Pregnancy occurs when the infertile couple use third person’s embryo and uterus (Circle E)
Gamete donation
Oocyte donation: Oocyte donation is one of the methods widely used in third-party treatments in Iran. Therefore, the use of donated oocytes in infertility treatments is relatively easier and less troublesome than other third-party assisted treatments in the country. Couples who have experienced fertility problems for many years or have no hope for fertilization using their own oocytes, after early menopause, are usually aware of the possibility of utilizing donated oocyte. In this treatment, the embryo is an outcome of the father’s genes that has biologically been grown in the mother’s uterus with different genetic origins from the mother.
As mentioned earlier, the only acceptable form of conception in Iran is within the marital union. On the introduction of ARTs to the country, one of the suggested solutions to legitimize oocyte donation was through temporary marriage (Muttah) 1 of the husband with a divorced single woman (40). In some cases, temporary marriage could make the second woman, the donor of oocyte, misunderstand the situation as she could consider herself the real mother of the child or the real wife of the husband, and impose herself on the infertile family, causing a great deal of trouble for the infertile couple. The following example is one of the dozens of the writers’ experiences (52).
A woman with infertility and ovulation problem (POF) who sought treatment stated that she had a record for oocyte donation treatment in an infertility center.
The center responded that they could provide treatment on the condition that the costs were paid and the donor temporarily wedded my husband. Then, we were referred to the office of Imam of Friday prayer (Imam Jume). After donation and pregnancy, the donor started making some trouble and legal claims such as demands for renting a house or food and clothing expenses. Then, she immodestly asked for living with us. We were extremely worried about this situation and were seeking a way to get out of it. Upon screening tests to assess the health of the embryo, some genetic problems were found and we had to abort it, and fortunately, got rid of the donor. We were disappointed and stopped the treatment until we realized that there was a possibility of receiving donated oocytes in an anonymous way. That’s why we made an appointment with you for treatment (a 31-year-old woman).
In the absence of a secular body overseeing the practice of ARTs, these issues led to questions from jurisprudents about the necessity of temporary marriage. Many jurisprudents did not consider temporary marriage as a pre-requirement for the use of donated oocytes, whether or not the donor is married. The jurists reasoned that due to the fact that the fertilization of the gamete or the embryo is carried out in the laboratory and later the embryo (Similar to the donated embryo) is transferred to the woman’s uterus, the use of temporary marriage to give the conception legitimacy, is not necessary. Thus, in Iran, marriage (Temporary or permanent) was excluded from the oocyte donation process. Following this advancement, usually, the treatment took place confidentially. This enabled preserving the traditional structure of the nuclear family. But nevertheless, oocyte donation methods could still get the infertile couple into trouble. This was due to the absence of any laws in the country and overlooking other problematic consequences of donation–especially as a result of ignoring confidentiality and the anonymity of the recipients and donors of gamete. As an example, another experience of the authors is presented in the following:
An infertile couple, due to lack of evaluation and financial problems to cover the expenses of the donation, was advised by their doctor to receive oocytes from a relative (A sister-in-law). They shared this request with the sister and his husband (Who already has a healthy daughter) and they accepted it. Thus, the treatment started and the sister’s oocytes were collected in an ovulation stimulation process. Then, the embryos from the sister-in-law’s eggs and the husband’s sperm were transferred to the wife’s uterus, resulting in a baby boy. The sister-in-law became pregnant again and gave birth to her second daughter. Her concerns about not having a son turned her attention to the boy born from the donated oocytes. This incident led to arguments. First, the sister-in-law tried to take care of the son and after a while, the time they spent together increased. Eventually, she made a claim on the baby and stopped all connections with the infertile couple who moved to another city.
By the time of this report, the infertile couple did not have any contacts with the child for 8 years. Although the action taken by the donor did not have any legal and moral justification, the infertile couple decided to remain silent to avoid harming the child. Thus, they referred to us having heard about the possibility of confidential treatment (A 35-year old woman).
Sperm donation: Sperm donation is one of the easiest and less expensive treatment methods for male factor infertility. With progress in developing ART, the use of the donated sperm in IVF or ICSI has also been approved by Shi’a authorities in Iran, due to the fact that the embryo forms out of the uterus by injection of sperm into oocyte. Initially, the use of the anonymously donated sperm for treating infertility in men was controversial from a religious point of view in the country. Later, some of the leading Islamic jurists ruled on prohibition of the use of donated sperm. Other Jurists suggested that, in cases of male infertility, his wife divorces him, marries a fertile man temporarily, and then divorces him after pregnancy and remarries her first husband (40, 52). This proposal received no support from the infertile couples. For example, after waiting for many years, a woman aware of her husband’s infertility due to lack of sperm and the possibility of pregnancy with donated sperm said,
The possibility of the use of donated sperm instead of donated embryo–which carries our genes partially–is promising. However, we became a little worried knowing the problems we might face. We visited the clergyman we follow (Marja) to discuss the religious concerns of this method. He suggested that we get a divorce and I marry the sperm donor, and then I divorce him after pregnancy and re-marry my husband. Practically, we could face many problems doing this. We noticed that there was no guarantee that this process would succeed. The pregnancy, divorcing the sperm donor and more importantly the remarriage could not be taken for granted. So, we gave up and applied for adoption. Now we have noticed that our Marja has changed his opinion, we are regretful, because we lost a lot of time and we could follow another Marja and use the opportunity to have a child (A 38-year-old woman).
Due to the follow ups and questions by patients and doctors, the jurisprudents ruled that those IVF technologies that do not involve bodily contacts between the donors and recipients, during the fertility process (E.g. IVF methods and transfer of oocyte to the uterus resulting in an embryo) are allowed. Currently, receiving a third person’s sperm for fertility has been accepted and applied as one of the infertility treatments. Although, in some countries, single or homosexual women are able to resort to the use of sperm, no decision has been made on this issue in Iran. Research carried out by the authors in this article confirms that confidentiality is key to the success of all these treatments and the more this procedure remains confidential, the less undesirable social consequences will ensue.
Embryo donation: Embryo donation is far more complicated than oocyte or sperm donation. In this method, there is no genetic links between the embryo and the parenting couple. From this perspective, embryo donation can be considered similar to adoption. However, at the donation time, a biological link is established during pregnancy, delivery, and breastfeeding between the woman and the resulting child.
In this method, within five days of the initial cell division of the embryos donated by a married couple, they are fertilized and transferred into the uterus. Here, it is also possible to benefit from the embryos of infertile couples who performed IVF and then refused to use their surplus frozen embryos. The success of using frozen embryos is not less than fresh ones. The treatment centers usually welcome this treatment and obtain permission from the couple to use the surplus embryos. The rights of donated embryos differ among different countries. In Iran, the embryo donation law was passed by the Iranian Parliament in 2003 and its implementing code (The laws and regulation collection) was issued in 2004 (53). Third-party reproduction using sperm/oocyte or embryo donation, which had not had a law but was endorsed by the jurisprudence and religious edicts (fatwa), is also classified under the embryo donation law. Only about 5% of the infertile couples have medical indications for using donated embryos. In other cases, the couples tend to preserve 50% of their biological link with the child and thus use donated oocytes or sperm. On this basis, donation bypasses the law in most cases. The nuclear family structure appears to be maintained in embryo donation treatments.
Returning to the importance of anonymity, in cases of embryo donation, the disclosure of the recipient or donor’s identity can intensely damage the parent’s expectations and disturb both the infertile couple and the child. An example of an infertile couple’s problems caused by non-anonymous embryo donation is presented in the following:
A couple with a 10-year old child resulting from infertility treatment (IVF/ICSI) decided to donate their frozen surplus embryos and offered them to a treatment center so that infertile couples could use them. Unfortunately, this couple lost their child in a car accident. The couple decided to receive a second treatment, but they found that it was impossible due to the weak oocytes due to ageing. When asked if they could use their surplus embryos, they realized that a patient was already using their donated embryos. Despite the confidentiality of the recipient’s identity, they found a way to identify the recipient and learned that she was pregnant with the donated embryo. The trauma of their loss, knowing that there was a child resulting from their donated embryos, led them to act unethically and immorally. Their claim on the child resulting from their donated embryo and the shortcomings of law and its conflict with some jurisprudents’ statements (Fatwa) made the court withdraw the child and return him/her to his/her biological parents (A 48-year-old woman).
It seems that there was a possibility for a lawsuit against the treatment center for disclosing the record and objecting to the court order. The trauma caused by the disclosure and its stigma in the society damage the social reputation of couples. They chose a confidential treatment, and to them the possibility for returning the child was excluded. Therefore, the embryo donation law could not recognize and guarantee the infertile couple’s family status and structure and is lacking in such cases.
Figure 1 summarizes the variations of different types of family and kinship structures including third party reproduction methods (Sperm, oocyte, embryo and surrogacy).
Surrogacy and a variety of related therapeutic methods: In general, surrogacy is used when the couple is infertile due to uterine defects, possibility of risky pregnancy, or the absence of the uterus. Surrogacy is an agreement between a woman with a healthy uterus willing to help the infertile couple by delivering the baby and later delivering the baby to the infertile couple. The pregnant woman (surrogate) who is also a gestational mother and the infertile couple are the real or social parents of the child. This method goes back to ancient times. Traditionally, gestational carrier (The surrogate mother) becomes pregnant only in favor of the infertile couple, and later donates the child to them. Alternatively, the surrogate mother becomes pregnant using the infertile couple’s sperm with her own egg, and later delivers the child to the infertile couple. The child resulting from this method has a genetic link to the surrogate mother and the sperm provider. These traditional methods were used when IVF methods were not invented, and the first recorded case is presented in the Book of Genesis–when Sarah, Abraham’s wife, asked him to engage in a sexual relationship with Hagar, their Egyptian maid, and make her pregnant as a solution for her infertility.
The advent of ARTs provided a new opportunity for the development of surrogacy. In the new modern IVF methodology, the in vitro embryo produced by the infertile couple’s oocyte and sperm will be transferred to the surrogate mother’s uterus until delivery, then the child will be returned to the biological parents, gamete owners. In this method, the surrogate mother does not have any genetic links with the child and is not considered the genetic/biological mother of the child. In general, surrogacy, based on sperm, oocyte, and embryo donation and a third-party uterus, considering the traditional methods, can be categorized into three main groups. The most privileged methods are as follows:
First, the infertile couple suffers from lack of uterus and ovaries. In this case, the surrogate mother’s uterus and oocytes are used. The surrogate mother becomes pregnant through transferring the embryo created by her oocytes and infertile woman’s husband sperm directly in her uterus. Hence, the surrogate mother is also the biological mother of the child, similar to the infertile woman’s husband, but the child will be brought up with no genetic/biological link with the mother.
In the second group, the infertile wife does not have a uterus and the husband suffers from lack of sperm/healthy sperm. In this group, the in vitro embryo produced by the donated sperm and parent oocyte is transferred into her uterus. The infertile woman, in this method, is considered the infant’s biologic/genetic mother. Her husband does not have such a link with the child.
The third group consists of the couples who suffer from lack of sperm and oocyte. In this method, there is no biological/genetic link between the resulting infant and the infertile couple; nor is the donated embryo developed in the infertile mother’s uterus.
Figure 2 summarizes the variations of the combined forms of all methods of “surrogacy” using ART and their encounter with the new forms of family.
Figure 2.

Seven possible combined forms of pregnancy in surrogacy by ART methods. Surrogacy is possible in the forms shown above and is done based on a contract which obligates the surrogate mother to deliver the child to the recipient family after pregnancy and childbirth. The traditional family structure is transformed in all these methods
In all methods, surrogacy is conducted with a contract based on which the surrogate mother is under obligation to deliver the resulting child to the infertile couple. The absence of an efficient law and agenda in Iran provides fertile ground for abuse. The following example demonstrates this issue:
A 44-year-old woman in need for a surrogate mother due to medical reasons said, “I was prohibited from pregnancy because of my illness. Enthusiastic for having a child, my husband and I decided to hire a surrogate mother. We were looking for a trustworthy person. Since I am a gynaecologist, I had more access to such cases. Examining my patients, I had a strong desire for an opportunity to examine our child in a surrogate uterus someday. Eventually I chose a young lady with a successful pregnancy and healthy child record. After ensuring her health condition and arranging a contract, the treatment process started. I started the process of ovulation stimulation and preparing my own oocytes and her uterus for the embryo transfer. During this period, I noticed that her attitude toward my husband changed and I found myself in the middle of difficulties more severe than the ones related to infertility. Therefore, I shared this issue with the center secretly, and after being convinced that I was right, I decided to stop the process and freeze the embryos, with the instructions given by the center. Since then, we have been looking for another suitable opportunity.
In general, all of the combined surrogacy methods used in infertility treatments aim at preserving the family; however, they cause changes in the way different members of the family are related to each other.
The emerging reproductive therapeutic methods Currently, new methods of infertility and sterility treatment are discovered. Germ cell transplantation, ovarian tissue transplantation, ovarian transplantation, uterus transplantation, production of tri –parental origin embryo, in vitro gamete production from cells, sex selection, PGD for medical reasons, and gene therapy are among therapies that cause great changes in the family structure.
The non-therapeutic use of ART methods: Many single people are now seeking the legitimization of IVF methods to be used in cases of single-parent family form. In Iran, single-parent family structure is generally forbidden. But recently, single women have been given permission to take care of orphans, or those children, who are looked after by unsuitable carers. With the availability of infertility technologies (ARTs), this expectation has grown higher so that these applicants demand for their biological childbirth using donated sperm or oocytes.
Conclusion
This article has focused on the impact of Third Party Reproduction on the structure of the family and kinship in Iran. Although the impingement of ARTs on kinship has been of intense interest to social scientists, the case of Iran provides new insights on the outcome of the encounter between these technologies and cultural practices. As this article has shown, Iran has been in the forefront of receiving ARTs with open arms and allowing their use in all their forms. At the same time, Iran has also abided by the cultural and religious rules in drawing the boundaries of what is permissible in the application of these technologies. This article has broadly outlined the process by which ARTs have been legitimized in Iran and the role played by the leading Islamist jurists, who, in the absence of an independent body responsible, were asked to give their verdicts on the legitimacy of these technologies. Although not all the jurists approved of ARTs, those who endorsed third-party donation, pointed out that the child, resulting from gamete donation, will belong to his biological parent. Such a ruling has meant that the identity of the donor of the gamete is important. Essentially, the sanctity of the lineage (nasab) has remained at the heart of re-production and the rulings.
What emerges from the case studies shows myriad of predictable and unpredictable complications and miseries caused for some of the users of third-party gamete. The examples given in this article are merely the tip of the iceberg. Clearly, the role of ARTs users in aggravating these complications can not be ignored either. For example, resorting to help from siblings and other biological relatives for gamete donation has been one of the sources of such conflicts.
The analysis of the actual and potential implications of third-party gamete donation for family and kinship also confirms the persistent stigma of infertility in Iranian culture. Prior to the introduction of IVF, it was impossible for the individuals to hide their infertility, which became a matter of concern for the entire kin group. Infertility has traditionally been perceived as the overall failure of the individuals to ensure the continuity of their lineage. Barrenness reflected on every aspect of the individuals’ personal, familial, and social life, ranging from masculinity/femininity, to personhood, and generally to their identity. The introduction of ARTs, especially third-party gamete donation, therefore, has proved a double-edge sword for the following reasons: Firstly, these technologies have altered the structure of the biological family by disrupting the continuity of the lineage, a sacrosanct value in the Islamic world-view, which gives legitimacy to the family. Secondly, this form of conception has led to the emergence of new structures and relations within the family as the child does not share one or both parents’ biogenetic material. In cases of blood relatives donating gamete to their relatives, although the child shares the same blood with the rest of the kin group, this leads to the formation of an entangled network of relatives and double relatedness, at times breaching the boundaries of what is culturally and religiously considered a taboo. Thirdly, in cases that the identity of the donors and recipients of gamete has been known to each other, frequent conflicts and arguments have arisen between the two parties on the financial, legal, religious, and emotional aspects of the ownership of the resulting child. As no solution has been foreseen to overcome these conflicts, in some cases, the responsibility falls on the medical practitioners to act as the jury and solve these problems. However, in those cases whereby the donors have been anonymous, or their identity has been kept confidential, an interesting situation has emerged whereby the infertile couples use anonymous gametes, which they keep as a secret, hide their infertility and claim the child to be their own biological offspring. In such cases, to the outside world, these couples are fertile and have their own biological children. Inwardly, however, to avoid the stigma of infertility and self-preservation, the couple must resort to concealing the truth, including the offspring. Whether from an ethical perspective this is a morally principled act or a solution that resolves problems and is in the interest of all concerned, remains open to debate.
Acknowledgement
There is no financial support in this study.
Footnotes
In cases of orphans and children with irresponsible parents, protection law was approved by the Guardian Council on September 2013. The related implementation code was approved on July 2018 by the First Vice-President. Facilitating the adoption requirements and expanding it to single women are some of the clauses pertaining to the implementation and regulations of this law.
And of His signs is that He created for you from yourselves mates that you may find tranquility in them; and He placed between you affection and mercy. Indeed, in that are signs for people who give thought (Ruum Sura, verse 21).
Prohibited to you [for marriage] are your mothers, your daughters, your sisters, your father’s sisters, your mother’s sisters, your brother’s daughters, your sister’s daughters, your [milk] mothers who nursed you, your sisters through nursing, your wives’ mothers, and your step-daughters under your guardianship [born] of your wives unto whom you have gone in. But if you have not gone in unto them, there is no sin upon you. And [also prohibited are] the wives of your sons who are from your [own] loins, and that you take [in marriage] two sisters simultaneously, except for what has already occurred. Indeed, Allah is ever forgiving and merciful (Neissa-23).
The circle of intimates (Maharem) by marriage is defined as mother-in-law, daughter-in-law, step mother, sister, or brother. The circle of intimates (Maharem) through kinship includes sister, mother and aunt and marriage with them is forbidden by Islam.
Within Islam, a temporary marriage generally implies a short-term arrangement between a man and a woman that does not come with a long-term commitment and may or may not have an explicit, pre-established timeline or endpoint. As an Arab custom, temporary marriage pre-dates Islam (Badran & Turnbull, 2019: 241)
Conflict of Interest
The authors confirm that there are no known conflicts of interest associated with this research.
References
- 1.Bamford SC. The Cambridge Handbook of kinship. 1st ed Cambridge: Cambridge university press; 2019. 750 p. [Google Scholar]
- 2.Behjati-Ardakani Z, Navabakhsh M, Hosseini SH. Sociological study on the transformation of fertility and childbearing concept in Iran. J Reprod Infertil. 2017;18(1):153–61. [PMC free article] [PubMed] [Google Scholar]
- 3.Ginsburg F. Conceiving the new world order: The global politics of reproduction. 1st ed California: University of California Press; 1995. 421 p. [Google Scholar]
- 4.Robertson AF. Beyond the family: the social organization of human reproduction. 1st ed California: Univ of California Press; 1991. 199 p. [Google Scholar]
- 5.Kligman G. The politics of duplicity: Controlling reproduction in Ceausescu’s Romania. 1st ed California: Univ of California Press; 1998. 341 p. [Google Scholar]
- 6.Unnithan-Kumar M. Female selective abortion–beyond ‘culture’: family making and gender inequality in a globalising India. Cult Health Sex. 2010;12(2): 153–66. [DOI] [PubMed] [Google Scholar]
- 7.Inhorn M, Van Balen F. Infertility around the globe: new thinking on childlessness, gender, and reproductive technologies. California: University of California Press; 2002. 315 p. [Google Scholar]
- 8.Hampshire K, Simpson B. Assisted reproductive technologies in the third phase: global encounters and emerging moral worlds. 1st ed New York: Berghahn Books; 2015. 284 p. [Google Scholar]
- 9.Ginsburg F, Rapp R. The politics of reproduction. Annu Rev Anthropol. 1991;20(1):311–43. [DOI] [PubMed] [Google Scholar]
- 10.Strathern M. After nature: English kinship in the late twentieth century. 1st ed Cambridge: Cambridge University Press; 1992. 218 p. [Google Scholar]
- 11.Strathern M. Reproducing the future: essays on anthropology, kinship and the new reproductive technologies. Manchester: Manchester University Press; 1992. 183 p. [Google Scholar]
- 12.Franklin S. Embodied progress: a cultural account of assisted conception. 1st ed London: Routledge; 1997. 252 p. [Google Scholar]
- 13.Ragoné H. Surrogate motherhood: conception in the heart. 1st ed Oxford: Westview Press; 1994. 215 p. [Google Scholar]
- 14.Edwards J, Franklin S, Strathern M, Hirsch E, Price F. Technologies of procreation: Kinship in the age of assisted conception. 2nd ed London: Routledge; 1999. 256 p. [Google Scholar]
- 15.Carsten J. Cultures of relatedness: new approaches to the study of kinship. 1st ed Cambridge: Cambridge University Press; 2000. 191 p. [Google Scholar]
- 16.Carsten J. After kinship. 1st ed Cambridge: Cambridge University Press; 2004. 191 p. [Google Scholar]
- 17.Parkin R, Stone L. Kinship and family: an anthropological reader. 1st ed US: Blackwell Pub; 2004. 496 p. [Google Scholar]
- 18.Inhorn MC. Making muslim babies: IVF and gamete donation in Sunni versus Shi’a Islam. Cult Med Psychiatry. 2006;30(4):427–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kahn SM, Farquhar J, Appadurai A. Reproducing Jews: a cultural account of assisted conception in Israel. 1st ed Durham: Duke University Press; 2000. 217 p. [Google Scholar]
- 20.Clarke M. Islam and new kinship: reproductive technology and the Shariah in Lebanon. New York: Berghahn Books; 2009. 220 p. [Google Scholar]
- 21.Eich T. Constructing kinship in Sunni Islamic legal texts. Islam and assisted reproductive technologies: Sunni and Shia perspectives. New York: Berghahn Books; 2012. 285 p. [Google Scholar]
- 22.Houlot S. Islamic Jurisprudence (Figh) and assisted reproduction: establishing limits to avoid social disorders. In: Inhorn MC, Tremayne S, editors. Islam and assisted reproductive technologies: Sunni and Shia perspectives. New York: Berghahn Books; 2012. p. 53–70. [Google Scholar]
- 23.Inhorn MC, Tremayne S. Islam and assisted reproductive technologies. 1st ed New York: Berghahn Books; 2012. 285 p. [Google Scholar]
- 24.Ardekani ZB, Akhondi MM, Kamali K, Khalaf ZF, Eskandari S, Ghorbani B. Mental health status of patients attending avicenna infertility clinic. J Reprod Infertil. 2010;11(4):319–24. [Google Scholar]
- 25.Tremayne S, Akhondi MM. Conceiving IVF in Iran. Reprod Biomed Soc Online. 2016;2:62–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tremayne S. The “down side” of gamete donation: challenging “happy family” rhetoric in Iran. Islam and assisted reproductive technologies: Sunni and Shia perspectives. 1st ed New York: Berghahn; 2012. chapter 5. p. 130–56. [Google Scholar]
- 27.Hendriks S, Dondorp W, de Wert G, Hamer G, Repping S, Dancet EA. Potential consequences of clinical application of artificial gametes: a systematic review of stakeholder views. Hum Reprod Update. 2015;21(3):297–309. [DOI] [PubMed] [Google Scholar]
- 28.Hermann BP, Sukhwani M, Winkler F, Pascarella JN, Peters KA, Sheng Y, et al. Spermatogonial stem cell transplantation into rhesus testes regenerates spermatogenesis producing functional sperm. Cell Stem Cell. 2012;11(5):715–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rafati M, Akhondi MM, Sadeghi MR, Tara SZ, Ghaffari SR. Preimplantation high-resolution HLA sequencing using next generation sequencing. Biol Blood Marrow Transplant. 2018;24(8):1575–80. [DOI] [PubMed] [Google Scholar]
- 30.Brännström M, Johannesson L, Bokström H, Kvarnström N, Mölne J, Dahm-Kähler P, et al. Live-birth after uterus transplantation. Lancet. 2015;385 (9968):607–16. [DOI] [PubMed] [Google Scholar]
- 31.Donnez J, Dolmans MM, Pellicer A, Diaz-Garcia C, Serrano MS, Schmidt KT, et al. Restoration of ovarian activity and pregnancy after transplantation of cryopreserved ovarian tissue: a review of 60 cases of reimplantation. Fertil Steril. 2013;99(6): 1503–13. [DOI] [PubMed] [Google Scholar]
- 32.Sadri-Ardekani H, Akhondi MA, van der Veen F, Repping S, van Pelt AM. In vitro propagation of human prepubertal spermatogonial stem cells. JAMA. 2011;305(23):2416–8. [DOI] [PubMed] [Google Scholar]
- 33.Marina S, Marina D, Marina F, Fosas N, Galiana N, Jové I. Sharing motherhood: biological lesbian co-mothers, a new IVF indication. Hum Reprod. 2010;25(4):938–41. [DOI] [PubMed] [Google Scholar]
- 34.Franssen MT, Musters AM, van der Veen F, Repping S, Leschot NJ, Bossuyt PM, et al. Reproductive outcome after PGD in couples with recurrent miscarriage carrying a structural chromosome abnormality: a systematic review. Hum Reprod Update. 2011;17(4):467–75. [DOI] [PubMed] [Google Scholar]
- 35.Ardekani ZB, Akhondi MM, Sadeghi MR, Sadri-Ardekani H. The necessity of a comprehensive study on abortion in Iran. J Reprod Infertil. 2005;6(4):299–320. [Google Scholar]
- 36.Golombok S. Parenting in new family forms. Curr Opin Psychol. 2017;15:76–80. [DOI] [PubMed] [Google Scholar]
- 37.Purewal S, van den Akker OB. Systematic review of oocyte donation: investigating attitudes, motivations and experiences. Hum Reprod Update. 2009; 15(5):499–515. [DOI] [PubMed] [Google Scholar]
- 38.Indekeu A, Dierickx K, Schotsmans P, Daniels K, Rober P, D’Hooghe T. Factors contributing to parental decision-making in disclosing donor conception: a systematic review. Hum Reprod Update. 2013;19(6):714–33. [DOI] [PubMed] [Google Scholar]
- 39.Inhorn MC, Patrizio P. Infertility around the globe: new thinking on gender, reproductive technologies and global movements in the 21st century. Hum Reprod Update. 2015;21(4):411–26. [DOI] [PubMed] [Google Scholar]
- 40.Behjati-Ardakani Z, Karoubi MT, Milanifar A, Masrouri R, Akhondi MM. Embryo donation in Iranian legal system: a critical review. J Reprod Infertil. 2015;16(3):130–7. [PMC free article] [PubMed] [Google Scholar]
- 41.Al-Hasani S. Islamic consideration (in Suni school) regarding bioethics and ART (especially oocyte and embryo donation) and the law in Germany. Payesh. 2007;6(4):379–84. [Google Scholar]
- 42.Sadeghi Fasaei S, Erfanmanesh I. Methodological foundations of documentary research in the social sciences: a study of the impacts of modernization on the Iranian family. Strategy Culture. 2015;8(29):61–91. [Google Scholar]
- 43.Altorki S. Milk-kinship in Arab society: an unexplored problem in the ethnography of marriage. Ethnology. 1980;19(2):233–44. [Google Scholar]
- 44.Rahbari L. Milk kinship and the maternal body in Shia Islam. De Gruyter. 2020;6:4353. [Google Scholar]
- 45.Castells M. The rise of the network society. USA: John wiley & sons; 2011. 1990 p. [Google Scholar]
- 46.Behjati Ardakani Z, Akhondi MM, Milanifar AR, Modaberi Y, Chamani Tabriz L, Moeeni M, et al. Counseling, evaluation and screening of donor and recipient in third party reproduction and the matching process. Payesh. 2007;6(4):443–51. [Google Scholar]
- 47.Behjati Ardakani Z, Abbasi Shavazi MJ, Shidfar F, Moeini M, Akhondi MM. The effect of ageing on natural and artificial reproduction. Payesh. 2007;6(4):331–45. [Google Scholar]
- 48.Abma JC. Fertility, family planning, and women’s health: new data from the 1995 national survey of family growth. US: CDC; 1997. 101 p. [PubMed] [Google Scholar]
- 49.Braverman AM. Defining, understanding, and managing the complex psychological aspects of third-party reproduction. In: Saure MV, editor. Principles of oocyte and embryo donation. London: Springer; 2013. p. 185–93. [Google Scholar]
- 50.Centers for disease control and prevention Assisted reproductive technology (ART). USA: Centers for disease control and prevention; 2014 national summary report 2014 Available from: http://www.cdc.gov/art/reports. [Google Scholar]
- 51.Akhondi MM, Kamali K, Ranjbar F, Shirzad M, Shafeghati S, Ardakani ZB, et al. Prevalence of primary infertility in Iran in 2010. Iran J Public Health. 2013;42(12):1398–404. [PMC free article] [PubMed] [Google Scholar]
- 52.Tremayne S. Law, ethics and donor technologies in Shia Iran. In: Birenbaum-Carmeli D, Inhorn MC, editors. Assisting reproduction, testing genes: global encounters with new biotechnologies. New York: Bergbahn Books;2009. p. 144–64. [Google Scholar]
- 53.Safaiee S. Failures of IRI “Embryo donation act” based on a comparative study. Payesh. 2007;6(4): 323–9. [Google Scholar]