

Abstract
Objective Video recording and video recognition (VR) with computer vision have become widely used in many aspects of modern life. Hospitals have employed VR technology for security purposes, however, despite the growing number of studies showing the feasibility of VR software for physiologic monitoring or detection of patient movement, its use in the intensive care unit (ICU) in real-time is sparse and the perception of this novel technology is unknown. The objective of this study is to understand the attitudes of providers, patients, and patient's families toward using VR in the ICU.
Design A 10-question survey instrument was used and distributed into two groups of participants: clinicians (MDs, advance practice providers, registered nurses), patients and families (adult patients and patients' relatives). Questions were specifically worded and section for free text-comments created to elicit respondents' thoughts and attitudes on potential issues and barriers toward implementation of VR in the ICU.
Setting The survey was conducted at Mayo Clinic in Minnesota and Florida.
Results A total of 233 clinicians' and 50 patients' surveys were collected. Both cohorts favored VR under specific circumstances (e.g., invasive intervention and diagnostic manipulation). Acceptable reasons for VR usage according to clinicians were anticipated positive impact on patient safety (70%), and diagnostic suggestions and decision support (51%). A minority of providers was concerned that artificial intelligence (AI) would replace their job (14%) or erode professional skills (28%). The potential use of VR in lawsuits (81% clinicians) and privacy breaches (59% patients) were major areas of concern. Further identified barriers were lack of trust for AI, deterioration of the patient–clinician rapport. Patients agreed with VR unless it does not reduce nursing care or record sensitive scenarios.
Conclusion The survey provides valuable information on the acceptance of VR cameras in the critical care setting including an overview of real concerns and attitudes toward the use of VR technology in the ICU.
Keywords: artificial intelligence, video recognition, computer vision, intensive care unit, quality improvement study
Background and Significance
Video recording devices have become a ubiquitous part of today's life, as it has been witnessed by omnipresent video cameras which were installed for security purposes in many public places such as airports, parking lots, or shopping malls. Traditionally, videos are recorded by cameras to process visual and audio information in real-time or to enable a subsequent review by a human operator.
Advances in artificial intelligence (AI) and deep learning (DL) techniques allowed the recognition of actions and objects 1 on a video feed—and brought advancement to a subfield known under the term “computer vision” (CV). DL operates with artificial neural networks arranged in layers which can recognize patterns in data and create conclusions. Tireless ability to do so was greatly effective for CV. 2 CV enables computers to recognize objects and name them in the same way as humans do. Analysis of data captured by the camera can go into a deeper level than a mere detection of objects—DL applied in CV enables classification of objects and segmentation which was proven to be beneficial for medical imaging. 2 Video recognition cameras capturing both—image and sound and operating in proximity with CV have an increasing number of applications.
Computer vision has been implemented in many industries outside of health care such as retail, security, military, agriculture, and automobile industry. Navigation, controlling processes, automatic inspection, modeling objects, and environment detection are among the few target areas. Video recognition cameras made operation of self-driving cars possible, in travel industry—facial recognition is being used for person and objects identification; visual search of images in Google is also based on CV.
Video recognition (VR) as part of telehealth technologies has a huge potential for quality and patient safety improvement as well as for optimization of workflow processes in the intensive care setting. In 2016, O'Connor et al 3 published a study in which they demonstrated reduced admission rates with the help of telehealth. Telehealth might also aid in assisting chronically ill patients. Magnus et al 4 discussed that telehealth with remote biometric monitoring may support peritoneal dialysis (PD) in patients, impacting PD care positively and increasing patient's autonomy and satisfaction. Tele-ICU technologies develop and change over time 5 and VR might embody the new trend in the modern health care. Recent VR techniques using DL algorithms and convolutional neural networks carry not only opportunities for automatization of tasks but also promising strategies for noncontact physiologic monitoring. 6 7
Further, the implementation and active utilization of VR in patient rooms in the intensive care unit (ICU) might not only serve as a safety net, but also support diagnostic process improvement, workflow optimization, and help decrease information overload, and alarm fatigue in the daily routine of ICU clinicians. ICUs are overly complex and fast-paced environments and the number of alerts and notifications for health care professionals has increased over the years and is overwhelming. In 1983, there were no more than six types of clinical alarms, however, more than 35 years later, the number has increased to 40 types of alarms for critically ill patients. 8 Due to alarm desensitization, the risk of patient harm could be intensified and lead to serious events. 9 As experienced health care providers cannot be present at each patient bedside 24/7, a digital monitoring device and its VR capability driven by AI could bridge this gap. Clinicians could receive a notification when unexpected abnormalities in patient status are being detected. Recent research studies have proven the feasibility of pervasive ICU monitoring with video recording. MacMurchy et al concluded that video recording is “a highly acceptable and feasible tool to evaluate quality and safety in the hospital”. 10 Further, Davoudi et al 11 published in 2019 the first study about developing an autonomous system for monitoring patients in the ICU. The investigators showed the huge potential of this technology in administering repetitive critical care patient assessments in real-time. Patient status deteriorations and more timely interventions could be enabled. Furthermore, new approaches for identifying and describing critical care conditions could be developed and adopted in future, especially in scenarios where real-time monitoring is essential—as it is often the case in the ICU setting. 11 VR and DL techniques have been successfully piloted to facilitate diagnosis, using noninvasive vital measurements such as heart rate 12 and respiratory rate 13 14 for prediction models. Additionally, the assessment of pain can be optimized and automated because CV can now analyze facial expressions of pain. 15 16
Objectives
The aim of the study is to assess the perception of bedside CV and VR technologies by ICU providers, patients, and patients' families.
Methods
Participants
Mayo Clinic hospitals in Rochester, Minnesota and Jacksonville, Florida participated in the study. ICU physicians, advanced practice providers, nurses, respiratory therapists (RTs), pharmacists, and dieticians were contacted for clinical version of the survey. Only adult ICU patients and adult family members were approached to answer patients' version of the questionnaire. ICU clinicians working in adult ICUs and NICU (neonatal ICU) were included in the survey procedure. The study was approved by the Mayo Clinic Institutional Review Board and endorsed by Mayo Clinic Critical Care Independent Multidisciplinary Practice.
Survey Instrument
A 10-question survey was developed with the aim to access opinions, attitudes on the use of VR technology in the ICU and the questions were developed with respect to literature “pain points” information and conversations with providers. One version was administered to ICU clinicians and another version with similar questions to patients and patients' families. Each question addressed a specific issue regarding VR. There were three identical questions in both versions. Single-choice answers and free-text comments were included in the questionnaire. The questions for clinicians included scenarios in which the clinicians would be comfortable and would agree with the use of VR cameras, specific concerns about impact on patient care and the job of health care professionals, opinions about potential benefits, harms and detrimental effects of VR on health care, and the impact on the patient—clinician relationship. Respondents were given the opportunity to specify personal comments on positive and negative impacts of VR. Questions on barriers toward VR implementation were also included in the survey.
The version for patients encompassed questions about general knowledge of cameras, exposure to video cameras, as well as patient's opinions and concerns on using VR cameras in the ICU.
Lastly, in each survey, space was left so that respondents could add free text comments.
Personal identifiers were not collected to maintain subjects' anonymity. Demographics included respondent's age and clinician's years in practice.
Survey Procedure
Clinicians were emailed the survey with background and rationale of the quality improvement study in December 2019. An explanation about the anonymity of the survey responses was included in the introduction. A follow-up request was sent 3 weeks later. The electronic survey version was managed via the RedCap tool version 9.1.15 (Vanderbilt University, Nashville, Tennessee, United States). 17 18
Surveys for patients were handed out as paper version by ICU providers to the patients and family members, the first author distributed the surveys to families and patients, respectively. Each ICU was given 30 copies of questionnaires. Responses were later entered in RedCap for further computerized analysis. At the time of the survey procedure, there were no video monitoring devices in the ICU units except for the NICU in Rochester, Minnesota (MN) where the “Caring Connection” is being used—a closed-circuit television system—which enables parents to watch their baby.
Analysis (Quantitative-Statistics, Qualitative)
Surveys were included in the analysis if more than 90% of questions were filled out completely. Descriptive statistics were used for summarizing results. Summary statistics was calculated using JMP Pro for Windows v. 14.3.0. For all statistical measures, a p -value of less than 0.05 was considered as statistically significant. The mean score was reported and tabulated for determination of central tendency of answers from both cohorts as well as differences in answers from both health care roles (prescribers vs. nonprescribers). A numerical value was collocated with written verbal answers and subsequently a calculation of the mean score was performed. The numerical values of answers were as follows: disagreement (“strongly disagree,” “No”) was assigned the value of 1.0, a neutral attitude (“I am not sure,” “I don't have a strong opinion,” “Maybe”) the value of 2.5, and agreement (“Strongly agree,” “Yes”) of 5.0.
Specific free-text comments given by providers, patient families, and patients were analyzed qualitatively, and thematic analysis of their opinions was performed to provide a detailed understanding of which aspects matter regarding the use of VR in the ICU.
Results
Electronic survey request was sent to 1,290 providers. As for patients, the survey was distributed in paper copies by ICU nurses and first author (A.G.). In total, 232 surveys (one excluded) from health care personnel (response rate 17.98%) and 50 questionnaires from patients and patient families were considered as complete and included in the final analysis. 47% respondents were prescribers (physicians, advance practice providers [APP]), 53% were nonprescribers (registered nurses [RN], RTs, other). The most representative group of providers (59%) had between 5 and 20 years of clinical experience. 19% had less than 5 years of experience, 22% had more than 20 years of experience. In total, across both participating Mayo Clinic sites, 43% of respondents were RNs, 30% were physicians, 16% were APPs, 5% were RTs, and 4% had other roles in the ICU team. Regarding the patient version of the survey, six patients (three current and three past) and 44 patients' family members completed the questionnaire.
Besides the closed questions, a large number of comments from health care professionals and a limited number of comments from patients were received (see Supplementary Appendix A , available in the online version).
Demographic characteristics of providers respondents are given in Table 1 and patients in Table 2 .
Table 1. Providers demographic characteristics ( n = 232) .
| MN— n (%) | FL— n (%) | All— n (%) | |
|---|---|---|---|
| What is your role in patient care? a | |||
| Physician (resident, fellow, consultant) | 34 (14.6) | 37 (15.9) | 71 (30.5) |
| Advanced practice provider | 26 (11.1) | 12 (5.1) | 38 (16.3) |
| Nurse | 71 (30.5) | 27 (11.6) | 100 (42.9) b |
| Respiratory therapist | 6 (2.6) | 7 (3) | 13 (5.6) |
| Other | 7 (3) | 3 (1.3) | 10 (4.3) |
| Total | 144 (61.8) | 86 (36.9) | 232 (99.6) |
| Providers age b | |||
| Under 25 y old | 12 (5) | 0 (0) | 12 (5) |
| 25–40 y old | 78 (33) | 40 (17) | 120 (52) |
| 41–55 y old | 40 (17) | 31 (13) | 71 (31) |
| 56–67 y old | 14 (6) | 13 (6) | 27 (12) |
| Over 67 y old | 0 (0) | 0 (0) | 0 (0) |
| Years in practice c | |||
| <5 y | 37 (16) | 7 (3) | 44 (19) |
| 5–10 y | 36 (15) | 26 (11) | 62 (27) |
| 10–20 y | 48 (21) | 26 (11) | 75 a (32) |
| >20 y | 24 (10) | 27 (12) | 51 (22) |
2 respondents did not respond to this question.
3 respondents did not answer this question.
1 respondent did not answer to this question.
Table 2. Patients demographic characteristics ( n = 50) .
| What is your age? | MN— n (%) | FL— n (%) | All— n (%) |
|---|---|---|---|
| Under 25 y old | 7 (100) | 0 (0) | 7 (14) |
| 25–40 y old | 10 (91) | 1 (9) | 11 (22) |
| 41–55 y old | 9 (100) | 0 (0) | 9 (18) |
| 56–67 y old | 14 (93) | 1 (7) | 15 (31) |
| Over 67 y old | 7 (100) | 0 (0) | 7 (14) |
| Total | 47 (94) | 2 (4) | 49 (98) a |
1 respondent did not answer to this question.
Providers' Responses
Providers' responses were analyzed in two cohorts to emphasize distinctions and similarities between the group of prescribers (medical doctors, APPs) and nonprescribers (RNs, RTs). Differences in answers between prescribers and nonprescribers on general acceptance of VR are displayed in Fig. 1 . An overview of concerns about VR and its impact on the clinical workflow is displayed in Fig. 2 . Summary of providers answers is included in Table 3 .
Fig. 1.
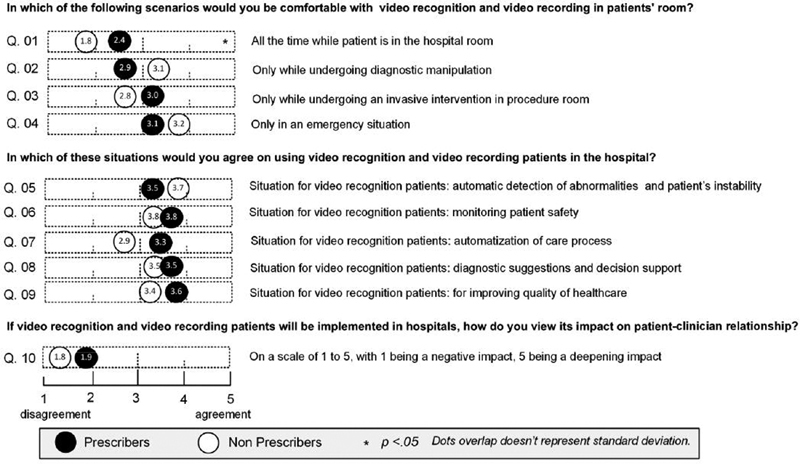
General acceptance and perception of video recognition by clinicians in Minnesota and Florida.
Fig. 2.
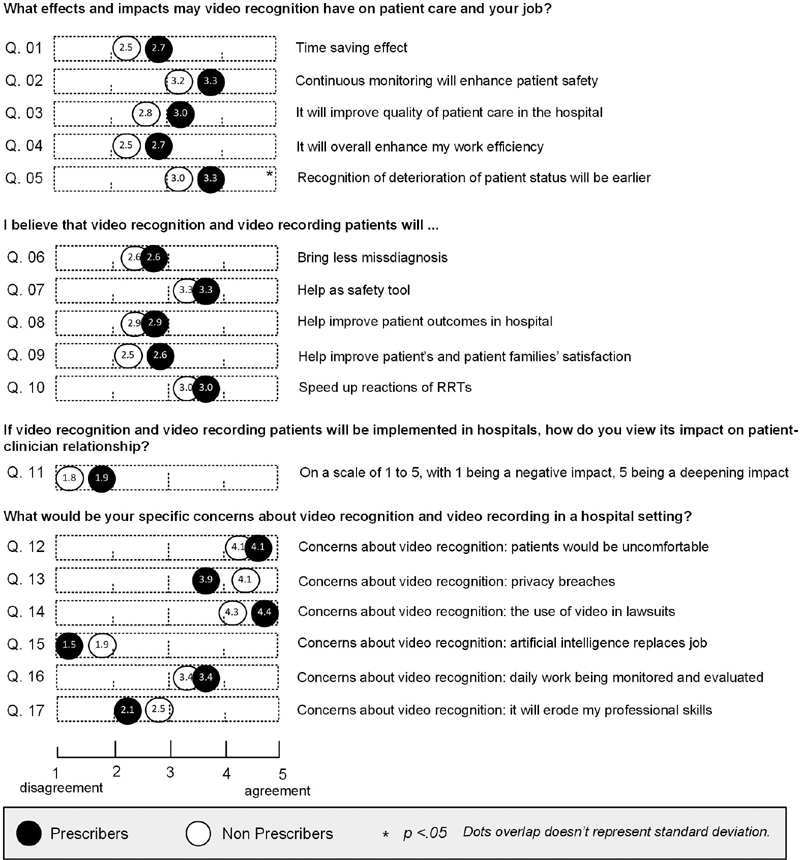
Differences in answers between subgroups of providers in Minnesota and Florida.
Table 3. Summary of answers—providers in Minnesota and Florida.
| In which of the following scenarios would you be comfortable with video recognition and video recording in patient's room? | Yes | No | No strong opinion |
|---|---|---|---|
| All the time while the patient is in the hospital room | 47 (20) | 141 (62) | 40 (18) |
| Only while undergoing diagnostic manipulation | 91 (42) | 79 (37) | 46 (21) |
| Only while undergoing an invasive intervention in procedure room | 101 (46) | 75 (34) | 43 (20) |
| Only in an emergency situation | 92 (42) | 82 (37) | 45 (21) |
| Other | 10 (10) | 43 (42) | 50 (49) |
| In which of these situations would you agree on using video recognition and video recording patients in the hospital? | |||
| Automatic detection of abnormalities and patients' instability | 125 (55) | 78 (35) | 22 (10) |
| Monitoring and enhancing patient safety | 153 (67) | 57 (25) | 19 (8) |
| Automatization of care processes | 89 (40) | 105 (46) | 31 (14) |
| Diagnostic suggestions and decision support | 113 (51) | 77 (35) | 31 (14) |
| For improving quality of health care | 128 (57) | 66 (29) | 32 (14) |
| Other | 6 (7) | 35 (40) | 47 (53) |
| What would be your specific concerns about video recognition and video recording in a hospital setting? | |||
| I am concerned that patients or family members would be uncomfortable with the video recognition and video recording patients. | 168 (73) | 25 (11) | 36 (16) |
| My concern is that there may be privacy breaches in which the video recording will be shared. | 163 (71) | 40 (17) | 27 (12) |
| I am concerned about the use of video recordings in lawsuits. | 183 (81) | 27 (12) | 17 (7) |
| I am concerned that artificial intelligence will replace my job. | 32 (14) | 172 (76) | 21 (9) |
| I am concerned about my daily work being continuously monitored and evaluated. | 132 (58) | 77 (34) | 18 (8) |
| My concern is that it will erode my professional skills | 64 (28) | 131 (58) | 32 (14) |
| What effects and impacts may video recognition have on patient care and your job? | Strongly disagree | Disagree | Neutral | Agree | Strongly agree |
|---|---|---|---|---|---|
| Time saving effect | 42 (19) | 55 (24) | 91 (40) | 31 (14) | 8 (3) |
| Continuous monitoring will enhance patient safety | 23 (10) | 32 (14) | 67 (30) | 84 (37) | 20 (9) |
| It will improve quality of patient care in hospital | 28 (12) | 43 (19) | 92 (41) | 51 (22) | 13 (6) |
| Recognition of deterioration of patient status will be earlier | 27 (12) | 33 (14) | 75 (33) | 74 (33) | 19 (8) |
| It will overall enhance my work efficiency | 39 (17) | 64 (28) | 91 (40) | 23 (10) | 10 (4) |
| I believe that video recognition and video recording patients will … | |||||
| Bring less misdiagnosis | 31 (13) | 67 (29) | 100 (44) | 27 (12) | 5 (2) |
| Help as safety tool | 20 (9) | 25 (11) | 65 (28) | 103 (45) | 15 (7) |
| Help improve patient outcomes in hospital | 28 (12) | 40 (18) | 94 (41) | 57 (25) | 9 (4) |
| Help improve patients and family's satisfaction | 39 (17) | 56 (24) | 102 (44) | 30 (13) | 4 (2) |
| Speed up reactions of RRTs | 22 (10) | 45 (20) | 83 (36) | 70 (30) | 10 (4) |
Abbreviation: RRT, renal replacement therapy.
General Acceptance and Perception of Video Recognition
Main domains identified and assessed throughout the survey were: general acceptance and perception of VR, potential concerns, and impacts on clinical practice.
The preference of choice for one out of four listed scenarios in which clinicians favored VR, showed that situations such as “for purposes of invasive intervention in procedure room” (46%), “emergency situation” (42%), and “diagnostic manipulation” (42%) gained the most acceptance. The biggest difference in mean score between prescribers and nonprescribers was preeminent in the “continuous monitoring.” Prescribers' mean score was 2.4 and thus closer to neural attitude, whereas nonprescribers' mean score of 1.8 indicated disagreement with monitoring a patient all the time. 20% of providers expressed “no strong opinion” to any of the specific scenarios.
When asked to select situations to identify acceptance of VR, “monitoring and enhancing patient safety,” “improving quality of health care” were the two most valued reasons in both cohorts, followed by “automatization of care processes,” “diagnostic suggestions and decision support.” Improving patient safety reached the same value of acceptance in prescribers and nonprescribers (both cohorts' mean score of 3.8) as well as diagnostic suggestions (mean score of 3.5). As for automatization of health care, more agreement was prevalent in prescriber's cohort (mean score of 3.3) than in the group of nonprescribers who expressed a neutral attitude (mean score of 2.9). Further, a notable equal portion of prescribers and nonprescribers agreed that VR will speed up reactions of rapid response teams (mean score of 3.0) and help as safety tool (mean score of 3.3)
Concerns about Video Recognition and VR's Impact on Clinicians and the Workflow
Participant's concerns were assessed with open multiple-choice questions. Questions assessing provider's attitudes toward the potential misuse of video recordings as well as the impact on clinical practice resulted in relatively uniform responses. A following trend in the choice of responses was observed in both provider's cohorts: concerns about the potential use of VR in lawsuits (81%) with slightly more often expressed concern in prescribers' cohort (mean score 4.4 in comparison to nonprescribers 4.3), and “patients and family members would be uncomfortable with VR” (73%, both cohorts reached the same mean score of 4.1). On the other hand, only a minority of providers had concerns such as: “it will erode my professional skills” (28%) or “AI will replace my job” (14%).
When effects and impacts of VR on clinician's job were compared a nearly homogeneous trend in answers was detected. Both prescribers and nonprescribers agreed that VR will help as safety tool. However, a certain portion of prescribers and nonprescribers doubted the time saving effect of VR technology and its capability of early recognition of deterioration of patient status with nonprescribers leading to disagreeing on this issue (mean score of 2.5). Overall, slightly more negative than positive attitudes toward VR's ability to detect deterioration of patient status and save time in the clinical workflow were noted in both cohorts. Statistically significant difference was identified in the question whether VR cameras enhance work efficiency of providers. More prescribers than nonprescribers agreed with the idea that VR will increase the work efficiency. Prescribers might possibly benefit from VR usage more than nonprescribers who will be using VR cameras less frequently than prescribers.
Patient–clinician relationship plays a crucial role in care, and the implementation of VR might change the way patients perceive clinical practice. Concerns that VR might have a negative effect on the patient–clinician relationships were raised by more than a half of prescribers and nonprescribers and their mean score was in harmony (1.9 prescribers, 1.8 nonprescribers). A part of prescribers (45%) and 23% of nonprescribers voted for a positive effect of VR. A small fraction of clinicians (6% prescribers, 10% nonprescribers) thought that VR will help deepen patient–clinician rapport.
Patients and Patients' Families' Answers
In total, six records from patients and 44 surveys from patient relatives were collected. Eight adult ICUs (cardiac, adult [extracorporeal membrane oxygenation], medical, surgical/trauma, multispecialty, neuroscience, and medical/surgical/transplant) in Mayo Clinic Rochester, MN and Jacksonville, Florida (FL) were asked for participation. The greatest portion of answers was obtained from the surgical, medical/surgical/transplant and multispecialty ICUs thanks to professional collaboration with clinical staff. The neurological ICU had the lowest response rate. Due to the seriousness of health condition of treated patients, it was challenging to obtain responses from patients and their families.
Even though the VR function of cameras is quite new, patients and patient families demonstrated great general knowledge of video cameras and were able to determine which functions cameras have (92% of patients knew that video cameras can recognize faces, 88% body movement, 69% breathing, and 55% pulse). More than a half of survey responders were persuaded that they might be exposed to cameras all the time in public places such as stores, malls, and libraries. One-third of the patients chose to get video recorded “all the time at work or school” and “all the time in the street, outdoors.” Three leading reasons for supporting VR usage among the patient cohort were: monitoring patient safety (88%) which was also the most valued reason in provider's cohort; followed by automatic detection of abnormalities and patient instability (82%) and improving quality of health care (74%).
Patients were asked to give opinion about the length of period, during which VR data will be stored and 29% of patient believed that the optimum would be 1 month after discharge. 27% of respondents from patient's cohort agreed with storage length of 1 year after discharge. 20% of respondents expressed that data should be stored only until discharge from hospital. 24 hours (20%) and permanent storage (7%) gained the least acceptance.
The current survey results showed an overall positive perception of VR technology among patients: 48% of patients were okay with the idea, 27% liked the option of using VR cameras, 17% did not like the idea, and 8% of the patient cohort had a very negative perception of VR. Nearly 70% of patients believed that this novel technology would have a positive impact on patient safety which is in congruence with echoes from providers who voted that VR would help as safety tool (46% prescribers, 55% nonprescribers), however, providers showed a noticeably decreased level of trust in VR's ability to increase patient safety based on this question.
Differences in Answers between Providers and Patients
Three out of 10 survey questions were identical for both groups of respondents (providers and patients). An overview of differences between providers' and patients' answers is displayed and reported in Fig. 3 . Patients’ and families’ responses are summarized in Table 4 .
Fig. 3.
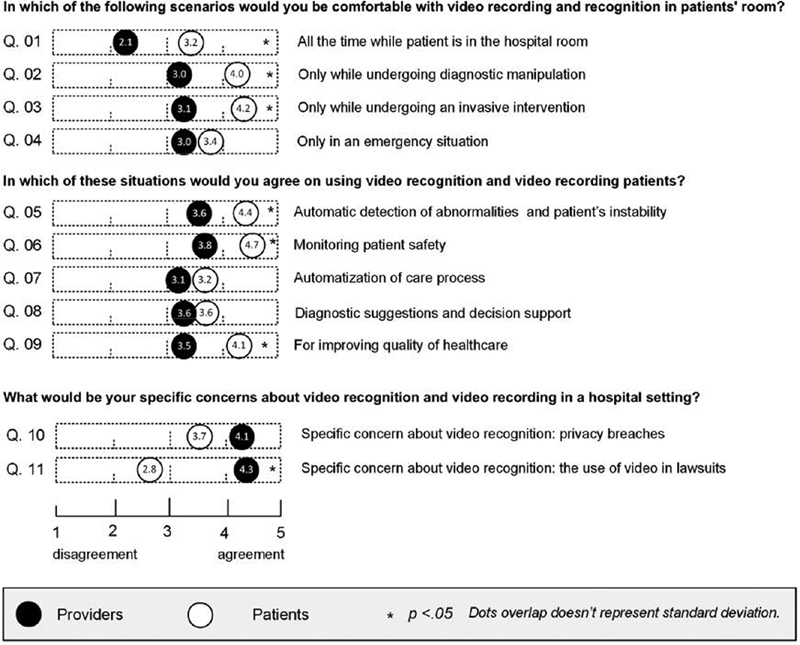
Providers–patients comparison.
Table 4. Summary of patients' and families' responses from Minnesota and Florida.
| Do you know what video cameras can recognize and analyze? | Yes | No | ||
| Faces | 46 (92) | 4 (8) | ||
| Body movement | 43 (88) | 6 (12) | ||
| Breathing | 34 (69) | 15 (31) | ||
| Pulse | 26 (55) | 21 (45) | ||
| Other objects | 34 (79) | 9 (21) | ||
| How often do you think you are exposed to video cameras at… | All the time | Sometimes | Not at all | I don't know |
| Home | 4 (8) | 22 (46) | 20 (42) | 2 (4) |
| Work or school | 17 (35) | 28 (57) | 2 (4) | 2 (4) |
| Other public places like stores, malls, libraries | 27 (54) | 23 (46) | 0 (0) | 0 (0) |
| Street, outdoors | 15 (30) | 34 (68) | 1 (2) | 0 (0) |
| In which of these situations would you agree on using video recognition and video recording patients in hospital | Yes | No | No strong opinion/maybe | |
| Automatic detection of abnormalities and patients' instability | 41 (82) | 4 (8) | 5 (10) | |
| Monitoring patient safety | 44 (88) | 2 (4) | 4 (8) | |
| Automatization of care processes | 25 (50) | 16 (32) | 9 (18) | |
| Diagnostic suggestions and decision support | 30 (60) | 13 (26) | 7 (14) | |
| For improving quality of health care | 37 (74) | 6 (12) | 7 (14) | |
| Other | 4 (50) | 1 (12) | 3 (38) | |
| In which of the following scenarios would you be comfortable with video recognition and video recording patient? | Yes | No | No strong opinion/maybe | |
| All the time while the patient is in the hospital room | 26 (52) | 20 (40) | 4 (8) | |
| Only while undergoing an invasive intervention in procedure room | 32 (71) | 7 (16) | 6 (13) | |
| Only while undergoing diagnostic manipulation | 27 (63) | 7 (16) | 9 (21) | |
| Only in an emergency situation | 23 (52) | 14 (32) | 7 (16) | |
| Other | 0 (0) | 1 (100) | 0 (0) | |
| Please, choose what best describes your viewpoint on VR and video recording patients in hospital | Yes |
I am
not sure |
No | |
| I think it will speed up clinical assessment and treatment | 19 (40) | 21 (45) | 7 (15) | |
| I believe it will have a positive impact on patient safety | 34 (69) | 11 (22) | 4 (8) | |
| I think it will be peace of mind and will have a positive impact on my satisfaction | 26 (55) | 15 (32) | 6 (13) | |
| It is okay that a video camera will monitor patient during hospital stay | 30 (64) | 11 (23) | 6 (13) | |
| What concerns do you have about video recognition and video recording patient in hospital? | Agree |
I am
not sure |
Disagree | |
| I am concerned that there may be privacy breaches and the video will be shared online | 29 (59) | 11 (22) | 9 (18) | |
| I am concerned about the use of video in lawsuits | 13 (27) | 20 (42) | 15 (31) | |
| Other | 2 (29) | 4 (57) | 1 (14) |
Patients were more comfortable with continuous monitoring (mean score of 3.20) than providers (mean score of 2.10). More than a half of providers (62%) responded “No” to continuous monitoring of patients in the ICU in comparison to 52% of patients who agreed on continuous operation of VR cameras.
Strong agreement with applying a VR camera only for situations, in which an invasive procedure takes place (46% of providers and 71% of patients), was distinctive in both cohorts—with a stronger agreement represented by patients (mean score of 4.20).
Next question regarding concerns about VR, showed that major concern of health care professionals was the use of video in lawsuits (81% of providers). 42% of patients were not sure about their opinion on this question. Privacy breaches in the VR system and sharing video online is a concern for 71% of critical care providers and 59% of patients with similar mean scores of 4.10 for providers and 3.70 for patients, respectively.
Further, evaluation of reasons which respondents found reasonable for introducing VR into the hospital setting was performed. “Monitoring patient safety” was the most important reason for using VR cameras for providers (67%, mean score 3.80) as well as for patients and their families (88%, mean score 4.64). The second most relevant reason for health care staff was “improving quality of health care” (57%, mean score 3.50). On patients' side “automatic detection of abnormalities and patient's instability” (82%, mean score 4.43) gained the most acceptance. “Diagnostic decision support” was favored by 60% of patients and 51% of providers (overlapping mean score 3.6).
Providers and Patients' Opinions
Providers' Opinions
Participants' comments which they wanted to bring to researchers' notice are displayed in Table 5 . In general, health care providers were concerned about privacy, safety, cost, security, ethical and moral issues such as data leaking, increasing cost for patients, misuse of data in lawsuits, and the distracting element of technology. They were also concerned about the limitation in patient–provider interaction, which may be caused by VR technology. Many providers desired that restrictions will be created on timing, location, and patient's health condition for the availability of VR. Several providers stated that it is inappropriate for deployment in the ICU setting. Many comments showed lack of trust in the AI technology and addressed its inaccuracy and lack of ability to act like human beings even though some clinicians sympathized with the VR technology. Detailed comments written to specific questions are listed in the table below. All “other” comments where providers expressed their own opinions about VR in general are displayed in the Supplementary Appendix A (available in the online version) section.
Table 5. Specific opinions given by providers.
| Classifier | Comments |
|---|---|
| Q1: In which of the following scenarios would you be comfortable with VR and video recording patient? | |
| Patient condition | 1. The only time I think this would be of benefit is if I had more than one confused patient that needed someone to watch them, and it did not need to be a nurse. 2. Only if patient requests for a specific reason. 3. Pt is a fall risk and is a threat to health care personnel. 4. While under any type of sedation. 5. Difficult family interaction. |
| Privacy and s ecurity | 1. Invasion of privacy/if leaked. 2. Patient mounted monitors for continuous tracking throughout the facility. |
| Timing restriction | 1. Not during personal cares. 2. During regular flow of shift and patient is not busy with other tasks. 3. I would like to turn off during sensitive procedures. 4. Communication during rounds. |
| Location restriction | 1. Never in a patient's room. 2. It all obviously depends on where the camera is trained, on the patient's bed or is entire ICU room monitored, so that a provider picking his or her nose as he leaves the room is “caught.” 3. Computer monitoring in restroom for safety as well due to risk of fall, etc. |
| Neutral | 1. I do not understand what it would be used for. |
| Q2: In which of these situations would you agree on using VR and video recording patients in the hospital? | |
| Patient condition | 1. Video on confused patient without saving feature helps protect patient when RN not in the room. |
| Alarm fatigue | 1. Alarm fatigue is a very real thing, this has the potential to make it significantly worse with false/inappropriate alarms. |
| Location restriction | 1. Never in the patient's room. 2. Computer monitoring in restroom for safety as well due to risk of fall, etc. |
| Lack of trust | 1. This is just regarding questions in the second part, I would be in favor of the computer recommending treatment/supportive measures if the AI ability is good enough to do so, not just “good enough” to make it a liability medico-legally if I do not accept the treatment and later have to defend myself in court because I used my judgment vs. the computer algorithm. 2. Code/resuscitation situations would be good to record and have the team review on how to improve processes and highlight what went well/works and what does not. 3. Many moral and ethical concerns. “Slippery slope” comes to mind immediately as does what the surveillance state in China and the arrests in Hong Kong. Also, I think it could be used for reprisals: we all make little mistakes so there would certainly be documentation a supervisor would need as grounds to threaten someone that was not staying in line even if the totality of the work was far above average. Also, people could be so focused on the video that they are not paying attention to the nuanced information that our patient's clinical presentation is giving us that AI cannot pick up. Warning fatigue is a worry.... the list goes on-and-on. 4. This is a rather biased question. How could one say “no” to improving quality of health care? How is this being interpreted? Our ICU has continuous monitoring of patients, along with 1;1, or at most 1;2 nurse staffing. Midlevel providers are present on the unit 24 hours a day along with critical care physicians. Unless there are plans to change these staffing ratios, and making an unsafe work environment, I see no need for video monitoring here. Will there be a cost to patients to have this benefit, and thus make more money for the institution? |
| Neutral | 1. I have worked in a setting where an E-ICU nurse “turned on” when there was instability in the vital signs. I did not mind this and it was helpful to have a person with a clear mind outside of the situation present to give input. It was also helpful that we could tell the E-ICU-RN, “We have everything under control—this is a planned extubation,” and the E-ICU-RN would exit the situation. |
| Q3: What would be your specific concerns about VR and video recording in a hospital setting? | |
| Safety | 1. I am concerned that staff will lean too much on technology and as a result safety issues arise. |
| Human interaction | 1. I am concerned that you are taking away the human contact and approach that these patients need during intubation and procedures. Patients want a human touch, not a machine. 2. We may depend on it too much (nurse, location unknown). 3. I am concerned that it will make communication more difficult in intense situations. I already experience many situations where there are too many people giving input in a given intense situation. |
| Cost | 1. Affordability of health care. It may add cost to the “already inflated” charges of health care. |
| Lack of trust | 1. It is a slippery slope. 2. It will modify visitor behavior/satisfaction. 3. It will be subject of a request increasing processing time on the back end. 4. I find that this can be used as a way to micromanage health care providers and decrease the limit autonomy we already have. It would be a way for an “easy financial opportunity” that some would take advantage in a lawsuit. Early recognition would only have a positive impact if the appropriate staff numbers would also improve to tend to the patients in a timely manner. 5. Algorithms cannot replace the human nature of what we do, see, and feel when working with the patient and their family. 6. We are already micromanaged. This will complicate our jobs. |
| Moral, ethical, inappropriate use | 1. Many moral and ethical concerns. “Slippery slope” comes to mind immediately as does what the surveillance state in China and the arrests in Hong Kong. Also, I think it could be used for reprisals: we all make little mistakes so there would certainly be documentation a supervisor would need as grounds to threaten someone that was not staying in line even if the totality of the work was far above average. Also, people could be so focused on the video that they are not paying attention to the nuanced information that our patient's clinical presentation is giving us that AI cannot pick up. Warning fatigue is a worry.... the list goes on-and-on. 2. I feel that patients will be taken advantage of with this video recording/recognition. How will patients be compensated for this access to their privacy? |
| Supportive comments | 1. I have worked in an ICU with remote EICU monitoring and, for the most part, it was very helpful to my practice. 2. This is a great idea that is used in various industries. |
| Q4: I believe that VR and video recording patient will… | |
| Privacy and security | 1. I think patients and family already feel like hospitals invade their privacy now. Having a continuous video recording is not something I would want as a patient. |
| Inappropriate for ICU | 1. Potential for greater benefit in general care and progressive care when patients are not under close observation. In the ICU a significant number of patients are under continuous observation by an RN who is more than capable of discerning a potentially dangerous situation. 2. In the CVS ICU, we are with our patients at all times d/t high acuity and there is a consulting physician, and NP/PAs steps away at all times. In our ICU I do not know how beneficial they will be, and it seems like a waste of resource/money. I feel like maybe it would be more beneficial in step down and med/surg units because the nurses have more patients and maybe it would help them with RRTs. |
| Human interaction | 1. Clinicians may not be as present at bedside if this technology is available. |
| Lack of trust | 1. There may be too many false alarms. 2. I am unsure how VR could assist with these things as I have never heard of it being used this way. 3. I do not believe the small safety benefit will outweigh all of the very serious negatives. |
| Supportive comments | 1. VR and video recording patients will help maintain safety to patients who are classified as very high fall risk, also to violent patients. 2. As a tool to monitor patients when needed is a great idea, which we already do. Again, for the RRTs you still have to have the appropriate staff number. 3. It all depends on how it is used. Cannot have a specific opinion unless I am given specifics. |
Abbreviations: AI, artificial intelligence; CVS, cardiovascular system; ICU, intensive care unit; RN, registered nurses; RRT, renal replacement therapy; VR, video recognition.
Opinions Given by Patients and Their Families
The opinions expressed by individual patients and families are in Table 6 . Patients and their families showed more relaxed attitude toward the use of VR in the hospital. They supported the use of this technology unless it does not substitute nursing care and expressed the request to be able to be in control such as being able to switch the camera off or being asked for consent before the VR camera is activated. The main concern of patients and their families is privacy, security issues such as leaking of data or being recorded in sensitive situations. One respondent (former worker in the image processing industry) shared his impressions on cameras and believed that a camera cannot save people.
Table 6. Specific opinions given by patients and their families.
| Classifier | Comments |
|---|---|
| Q1: In which of these situations would you agree on using VR and video recording patients in hospital? | |
| No replacement of nursing care | 1. Automatization of care processes yes—without decreased nursing care. |
| Q2: In which of the following scenarios would you agree on using VR and video recording patients in hospital? | |
| Doctor communication | 1. To record doctor communication of instructions/diagnoses |
| Education purpose | 1. For educational purposes only and with consent |
| Q3: What concerns do you have about VR and video recording patient in hospital? | |
| Privacy and security | 1. Privacy—not just online. 2. As a visitor I do not want to be filmed. 3. I believe patients are entitled to some privacy, however. 4. I have been in the image processing, machine vision, security industry for over 30 years. “Do you know what video cameras can recognize and analyze?” “Faces”: any decent resolution camera will recognize faces, it is the facial recognition software that does the work. “Body movement” biomechanics—same as above “breathing” metrology software can measure the expansion/contraction of the chest. “How often do you think you are exposed to video cameras at...” Your cell phone and laptop cameras unless you disable them, the boss is always watching, just look up, the (cameras) are everywhere—loss prevention, just look up, and in (unclear)...holy moly. Great as a security tool in hallways, elevators, stairs, medicine? unclear word? etc. The camera cannot save you. Privacy concerns. 5. Concerned about video of naked people. 6. I would not want that video of me/family out of this forever. |
| Q4: Other comments that a patient may have | |
| Controllable | 1. A person should know when they are on camera and be able to refuse being watched all the time. |
| Storing time | 1. Best: the video recording should be stored 1 to 10 years. 2. The video recording should be stored for the same amount of time as medical records are preserved. 3. How the information is used determines for me how I feel about it and for how long it is kept. |
Abbreviation: VR, video recognition.
Discussion
The main aim of this study was to thoroughly evaluate the perception of VR cameras and understand the attitudes of health care providers as well as of patients and their families toward this novel technology.
To the best of our knowledge this was the first study to evaluate background knowledge and attitudes of patients and health care personnel on the presence of video cameras in ICU patients' rooms and the machine learning's automatic VR functionality of them. All providers involved in direct ICU patient care were invited to participate in our study.
Nearly one-half of asked intensivists agreed on using VR cameras, when applied in certain listed scenarios (such as invasive intervention in procedure room, diagnostic manipulation). A continuous usage of VR cameras was not favorable for 62% of providers. Patients are exposed to certain levels of stress in ICU rooms and as McKenna et al 19 state, critical care patients suffer from circadian rhythm disruptions during the stay in the ICU. Environmental factors (monitor beeping, noise) might further influence patient's perception of stress. It could be one of the reasons why continuous usage of another monitor—the VR camera was not perceived positively, and providers suggested its use only in specified scenarios.
As with every new technological tool, its advantages and potential risks must be weighed up carefully. Providers also indicated that VR might have a negative impact on patient—physician relationship and that patients might feel uncomfortable in the presence of VR. A similar trend toward perception of technology was identified with a systematic review published in 2016 by Alkureishi et al 20 who showed evidence of negative impact of electronic medical record (EMR) use on patient–doctor communication expressed by clinicians, however, studies identified with the systematic search assessing patient perception demonstrated no change in patient satisfaction or differences in the dynamics of the patient–doctor rapport. A certain portion of studies indicated that patients felt EMR brought more clarity into communication flow.
Our survey showed that most clinicians had the opinion that their competency will not be diminished or that AI will replace their job. However, minor differences were noticeable between nurses and physicians. The nurse's cohort had increased concerns in comparison to physicians about their job being continuously monitored and 60% of participating nurses evaluated that AI might erode their professional skills.
Video recognition cameras, when appropriately applied and when all safety, socio-economic criteria are met, might be a potent tool and benefit the health care of the 21 st century. Both survey cohorts were resolute that introducing VR is reasonable for its usage as a safety tool to enable a smoother workflow process in the ICU environment. “Monitoring and enhancing patient safety” was listed by 67% of respondents as the main reason for introducing VR cameras. On the opposite side of the spectrum “diagnosis suggestions and decision support” and “automatization of health care” gained surprisingly only 51% and 40% acceptance even though the feature of VR cameras to measure vitals and produce alerts has the potential to support diagnosis decision 11 or assist in medical diagnosis 21 as previous studies found.
However, the limitation of this study is, that it was conducted only at two Mayo Clinic campuses in Rochester and Jacksonville and therefore, its results might not be generalizable for every U.S. hospital. The survey received a total of 44 responses from patient's relatives and only six responses from patients, therefore the survey results indicate the assessment of families of ICU's patients rather than patients per se as it was planned. Due to the size of patient's cohort, extrapolation of data might not be optimal to create a generalizable conclusion.
All specific concerns expressed by both sides, patients and patient's families and clinicians, must be addressed in the future and the solution for identified problems must be found before actual implementation takes place. The aim of development of VR systems is not to replace the work of health care providers. Instead, it represents a supportive tool for reduction of the workload in the monitoring of ICUs. As for severely ill patients, VR may help release concerns of both—patients and their families—due to its tireless ability to observe patients 24/7. Our hope is that all presented results will encourage researchers and engineers in this field to decide about further steps toward the accommodation of VR in health care to secure patients' satisfaction and help promote more safety for critical care staff and patients with a smoother workflow in an environment which is already incredibly complex, fast-paced, and necessitating swift action and thorough application of clinical skills to treat the most critical patients. The principles behind the functioning of VR are straightforward and their future implementation must be transparent. Patient privacy preservation is of paramount importance and use of VR must be carefully planned to benefit and serve both sides (health care staff as well as patients). Cautious application of VR systems is crucial to avoid any detrimental consequences such as misinterpretation and misuse of VR data. Use of video recordings in lawsuits and privacy issues represents relevant concerns about the VR technology.
To sum up, greater effort should be applied to enhancing patient security, privacy, and the quality of health care. VR cameras have the potential to support all these aspects and help promote automatization of health care processes in hospitals.
Conclusion
This survey study provided an initial perception of the presence of VR systems in ICUs and identified potential concerns and barriers toward implementation of this novel technological tool.
Overall acceptance of VR on clinician's side was characterized by positive perception of the VR for use in an emergency, diagnostic manipulation, and invasive intervention but concerns regarding continuous monitoring, data leaks, and using video footage in lawsuits were raised. More than a half of patients' cohort agreed with VR for safety purposes but expressed concerns on nursing care replacement. More education about benefits of the VR technology is required prior to its usage.
Clinical Relevance Statement
The study summarized authentic answers about perception of VR technology in the ICU and the survey promoted understanding of both clinicians' and patients' perspective toward application of cameras with CV in the critical care environment.
Multiple Choice Questions
-
What was the most acceptable reason for using video recognition cameras which gained the most similar agreement in both cohorts?
Emergency situation
Continuous monitoring of patient
Diagnostic procedures
Surgery
Correct Answer: The correct answer is option a, according to the results of the survey.
-
What are the major barriers toward implementation of video recognition (based on the information presented in this article)?
Concerns about using video recordings in lawsuits, safety issues, video recognition cameras will bring more confusion and information overload, worsening of the patient–clinician relationship.
Artificial intelligence replaces job of clinicians and will make health care less human, concerns about privacy breaches.
Concerns about using of video recordings in lawsuits, privacy issues, worsening of the patient–clinician relationship, and making the patient uncomfortable.
Only privacy concerns raised by health care professionals and patients.
Correct Answer: The correct answer is option c, based on survey results.
Acknowledgment
We would like to thank all the Mayo clinicians who participated in this research study. A special thank you goes to nurses who helped with the survey distribution.
Funding Statement
Funding There were no specific intramural or extramural funds for this project.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
The survey study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. The study was reviewed by Institutional Review Board and given the identifier 18–001525.
Supplementary Material
References
- 1.Yuan Y B, David G Y, Zhao S. Machine learning in intelligent video and automated monitoring. Sci World J. 2015;2015:570145. doi: 10.1155/2015/570145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Esteva A, Robicquet A, Ramsundar B. A guide to deep learning in healthcare. Nat Med. 2019;25(01):24–29. doi: 10.1038/s41591-018-0316-z. [DOI] [PubMed] [Google Scholar]
- 3.O'Connor M, Asdornwised U, Dempsey M L. Using telehealth to reduce all-cause 30-day hospital readmissions among heart failure patients receiving skilled home health services. Appl Clin Inform. 2016;7(02):238–247. doi: 10.4338/ACI-2015-11-SOA-0157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Magnus M, Sikka N, Cherian T, Lew S Q. Satisfaction and improvements in peritoneal dialysis outcomes associated with telehealth. Appl Clin Inform. 2017;8(01):214–225. doi: 10.4338/ACI-2016-09-RA-0154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Anders S H, Woods D D, Schweikhart S, Ebright P, Patterson E. The effects of health information technology change over time: a study of Tele-ICU functions. Appl Clin Inform. 2012;3(02):239–247. doi: 10.4338/ACI-2011-12-RA-0073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Liang Q, Xu L, Bao N. Research on non-contact monitoring system for human physiological signal and body movement. Biosensors (Basel) 2019;9(02):58. doi: 10.3390/bios9020058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wu H Y, Rubinstein M, Shih E. Eulerian video magnification for revealing subtle changes in the world. ACM Trans Graph. 2012;31(04):1–8. [Google Scholar]
- 8.Cho O M, Kim H, Lee Y W, Cho I. Clinical alarms in intensive care units: perceived obstacles of alarm management and alarm fatigue in nurses. Healthc Inform Res. 2016;22(01):46–53. doi: 10.4258/hir.2016.22.1.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Johnson K R, Hagadorn J I, Sink D W. Alarm safety and alarm fatigue. Clin Perinatol. 2017;44(03):713–728. doi: 10.1016/j.clp.2017.05.005. [DOI] [PubMed] [Google Scholar]
- 10.MacMurchy M, Stemler S, Zander M, Bonafide C P. Research: acceptability, feasibility, and cost of using video to evaluate alarm fatigue. Biomed Instrum Technol. 2017;51(01):25–33. doi: 10.2345/0899-8205-51.1.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Davoudi A, Malhotra K R, Shickel B. Intelligent ICU for autonomous patient monitoring using pervasive sensing and deep learning. Sci Rep. 2019;9(01):8020. doi: 10.1038/s41598-019-44004-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhu J, Shi Y, Yang M.Heart rate detection based on computer visionPaper presented at: 5th IEEE International Conference on Cloud Computing and Intelligence System; November 23–25, 2018;Nanjing, China
- 13.Jagadev P, Giri L I. Non-contact monitoring of human respiration using infrared thermography and machine learning. Infrared Phys Technol. 2020;104:103117. [Google Scholar]
- 14.Ṭarălungă D D, Mocanu B, Ṭapu R. Singapore: Springer Singapore; 2017. Automatic real time derivation of breathing rate from thermal video sequences. IFMBE Proceedings; pp. 81–84. [Google Scholar]
- 15.Lucey P, Cohn J F, Matthews I. Automatically detecting pain in video through facial action units. IEEE Trans Syst Man Cybern B Cybern. 2011;41(03):664–674. doi: 10.1109/TSMCB.2010.2082525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sikka K, Ahmed A A, Diaz D. Automated assessment of children's postoperative pain using computer vision. Pediatrics. 2015;136(01):e124–e131. doi: 10.1542/peds.2015-0029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Harris P A, Taylor R, Minor B L. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi: 10.1016/j.jbi.2019.103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Harris P A, Taylor R, Thielke R, Payne J, Gonzalez N, Conde J G. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(02):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McKenna H T, Reiss I K, Martin D S. The significance of circadian rhythms and dysrhythmias in critical illness. J Intensive Care Soc. 2017;18(02):121–129. doi: 10.1177/1751143717692603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Alkureishi M A, Lee W W, Lyons M. Impact of electronic medical record use on the patient-doctor relationship and communication: a systematic review. J Gen Intern Med. 2016;31(05):548–560. doi: 10.1007/s11606-015-3582-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thevenot J, López M B, Hadid A. A survey on computer vision for assistive medical diagnosis from faces. IEEE J Biomed Health Inform. 2018;22(05):1497–1511. doi: 10.1109/JBHI.2017.2754861. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.